
Dietary Inflammatory Potential and Bone Outcomes in Midwestern Post-Menopausal Women

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
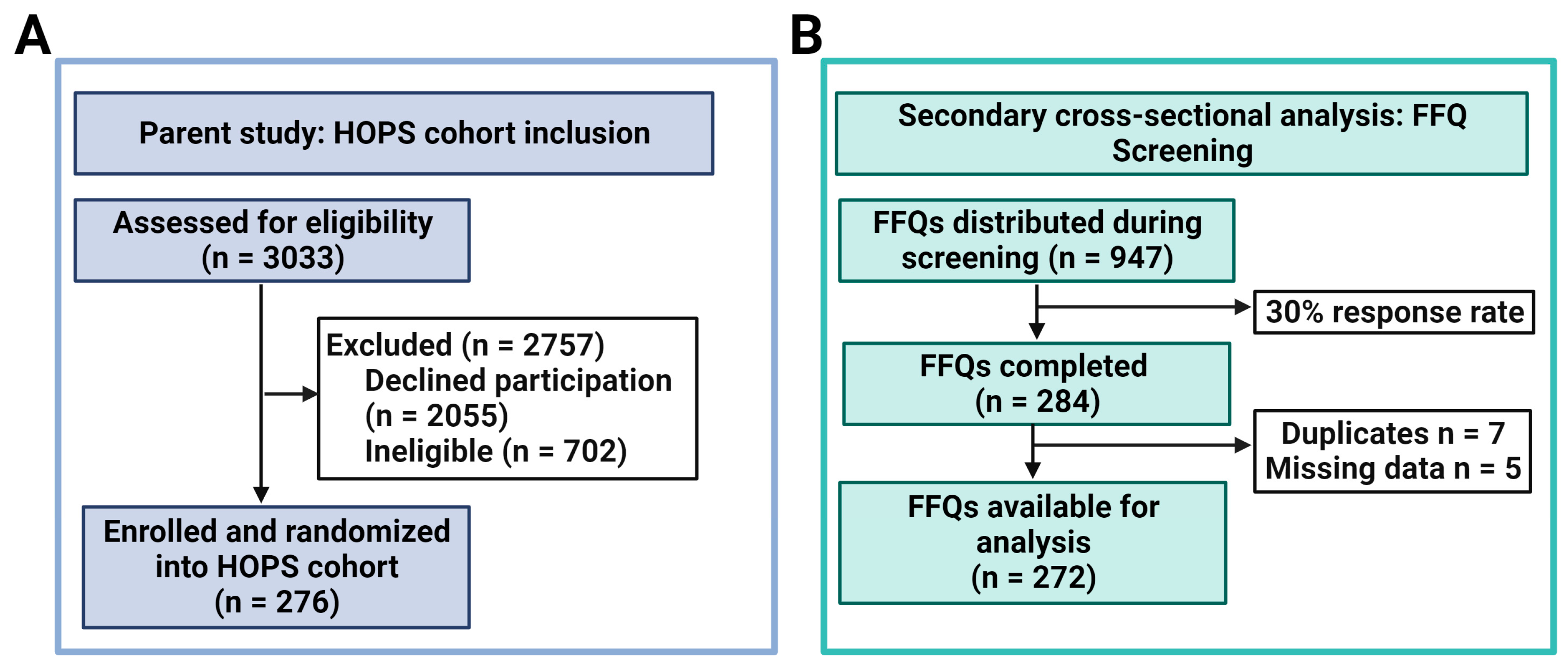
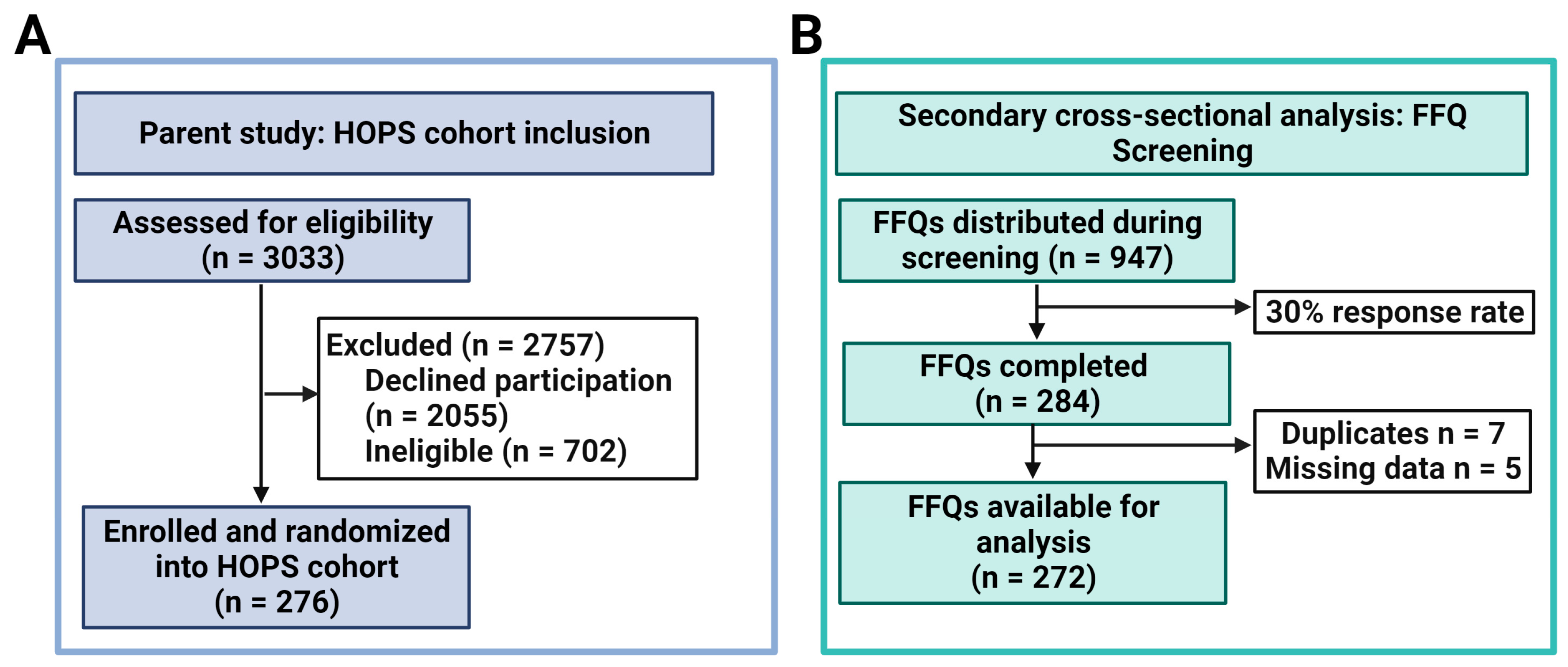
3.1. Characteristics of the Study Population
3.2. E-DII Quartiles and Bone Outcomes
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cotts, K.G.; Cifu, A.S. Treatment of Osteoporosis. JAMA 2018, 319, 1040–1041. [Google Scholar] [CrossRef]
- National Osteoporosis Foundation. What Is Osteoporosis and What Causes It? Available online: https://www.nof.org/patients/what-is-osteoporosis/ (accessed on 1 October 2022).
- Armas, L.A.; Recker, R.R. Pathophysiology of osteoporosis: New mechanistic insights. Endocrinol. Metab. Clin. N. Am. 2012, 41, 475–486. [Google Scholar] [CrossRef]
- Camacho, P.M.; Petak, S.M.; Binkley, N.; Diab, D.L.; Eldeiry, L.S.; Farooki, A.; Harris, S.T.; Hurley, D.L.; Kelly, J.; Lewiecki, E.M.; et al. American Association of Clinical Endocrinologists/american College of Endocrinology Clinical Practice Guidelines for the Diagnosis and Treatment of Postmenopausal Osteoporosis-2020 Update Executive Summary. Endocr. Pract. Off. J. Am. Coll. Endocrinol. Am. Assoc. Clin. Endocrinol. 2020, 26, 564–570. [Google Scholar] [CrossRef]
- Harvey, N.C.; Gluer, C.C.; Binkley, N.; McCloskey, E.V.; Brandi, M.L.; Cooper, C.; Kendler, D.; Lamy, O.; Laslop, A.; Camargos, B.M.; et al. Trabecular bone score (TBS) as a new complementary approach for osteoporosis evaluation in clinical practice. Bone 2015, 78, 216–224. [Google Scholar] [CrossRef]
- Movassagh, E.Z.; Vatanparast, H. Current Evidence on the Association of Dietary Patterns and Bone Health: A Scoping Review. Adv. Nutr. 2017, 8, 1–16. [Google Scholar] [CrossRef]
- Shi, Y.; Zhan, Y.; Chen, Y.; Jiang, Y. Effects of dairy products on bone mineral density in healthy postmenopausal women: A systematic review and meta-analysis of randomized controlled trials. Arch. Osteoporos. 2020, 15, 48. [Google Scholar] [CrossRef]
- Hamidi, M.; Tarasuk, V.; Corey, P.; Cheung, A.M. Association between the Healthy Eating Index and bone turnover markers in US postmenopausal women aged ≥ 45 y. Am. J. Clin. Nutr. 2011, 94, 199–208. [Google Scholar] [CrossRef]
- Zagarins, S.E.; Ronnenberg, A.G.; Gehlbach, S.H.; Lin, R.; Bertone-Johnson, E.R. Are existing measures of overall diet quality associated with peak bone mass in young premenopausal women? J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2012, 25, 172–179. [Google Scholar] [CrossRef]
- de Jonge, E.A.; Kiefte-de Jong, J.C.; de Groot, L.C.; Voortman, T.; Schoufour, J.D.; Zillikens, M.C.; Hofman, A.; Uitterlinden, A.G.; Franco, O.H.; Rivadeneira, F. Development of a Food Group-Based Diet Score and Its Association with Bone Mineral Density in the Elderly: The Rotterdam Study. Nutrients 2015, 7, 6974–6990. [Google Scholar] [CrossRef]
- Fabiani, R.; Naldini, G.; Chiavarini, M. Dietary Patterns in Relation to Low Bone Mineral Density and Fracture Risk: A Systematic Review and Meta-Analysis. Adv. Nutr. 2019, 10, 219–236. [Google Scholar] [CrossRef]
- Langsetmo, L.; Poliquin, S.; Hanley, D.A.; Prior, J.C.; Barr, S.; Anastassiades, T.; Towheed, T.; Goltzman, D.; Kreiger, N.; CaMos Research, G. Dietary patterns in Canadian men and women ages 25 and older: Relationship to demographics, body mass index, and bone mineral density. BMC Musculoskelet. Disord. 2010, 11, 20. [Google Scholar] [CrossRef]
- Ding, C.; Parameswaran, V.; Udayan, R.; Burgess, J.; Jones, G. Circulating levels of inflammatory markers predict change in bone mineral density and resorption in older adults: A longitudinal study. J. Clin. Endocrinol. Metab. 2008, 93, 1952–1958. [Google Scholar] [CrossRef]
- Tang, Y.; Peng, B.; Liu, J.; Liu, Z.; Xia, Y.; Geng, B. Systemic immune-inflammation index and bone mineral density in postmenopausal women: A cross-sectional study of the national health and nutrition examination survey (NHANES) 2007–2018. Front. Immunol. 2022, 13, 975400. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hebert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public. Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef]
- de Pablo, P.; Cooper, M.S.; Buckley, C.D. Association between bone mineral density and C-reactive protein in a large population-based sample. Arthritis Rheum. 2012, 64, 2624–2631. [Google Scholar] [CrossRef]
- Bilek, L.D.; Waltman, N.L.; Lappe, J.M.; Kupzyk, K.A.; Mack, L.R.; Cullen, D.M.; Berg, K.; Langel, M.; Meisinger, M.; Portelli-Trinidad, A.; et al. Protocol for a randomized controlled trial to compare bone-loading exercises with risedronate for preventing bone loss in osteopenic postmenopausal women. BMC Women’s Health 2016, 16, 59. [Google Scholar] [CrossRef]
- Waltman, N.; Kupzyk, K.A.; Flores, L.E.; Mack, L.R.; Lappe, J.M.; Bilek, L.D. Bone-loading exercises versus risedronate for the prevention of osteoporosis in postmenopausal women with low bone mass: A randomized controlled trial. Osteoporos. Int. 2022, 33, 475–486. [Google Scholar] [CrossRef]
- Willett, W.C.; Sampson, L.; Stampfer, M.J.; Rosner, B.; Bain, C.; Witschi, J.; Hennekens, C.H.; Speizer, F.E. Reproducibility and validity of a semiquantitative food frequency questionnaire. Am. J. Epidemiol. 1985, 122, 51–65. [Google Scholar] [CrossRef]
- Yuan, C.; Spiegelman, D.; Rimm, E.B.; Rosner, B.A.; Stampfer, M.J.; Barnett, J.B.; Chavarro, J.E.; Rood, J.C.; Harnack, L.J.; Sampson, L.K.; et al. Relative Validity of Nutrient Intakes Assessed by Questionnaire, 24-Hour Recalls, and Diet Records as Compared With Urinary Recovery and Plasma Concentration Biomarkers: Findings for Women. Am. J. Epidemiol. 2018, 187, 1051–1063. [Google Scholar] [CrossRef]
- Tabung, F.K.; Steck, S.E.; Zhang, J.; Ma, Y.; Liese, A.D.; Agalliu, I.; Hingle, M.; Hou, L.; Hurley, T.G.; Jiao, L.; et al. Construct validation of the dietary inflammatory index among postmenopausal women. Ann. Epidemiol. 2015, 25, 398–405. [Google Scholar] [CrossRef]
- Hebert, J.R.; Shivappa, N.; Wirth, M.D.; Hussey, J.R.; Hurley, T.G. Perspective: The Dietary Inflammatory Index (DII)-Lessons Learned, Improvements Made, and Future Directions. Adv. Nutr. 2019, 10, 185–195. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Ge, I.; Rudolph, A.; Shivappa, N.; Flesch-Janys, D.; Hébert, J.R.; Chang-Claude, J. Dietary inflammation potential and postmenopausal breast cancer risk in a German case-control study. Breast 2015, 24, 491–496. [Google Scholar] [CrossRef]
- Orchard, T.; Yildiz, V.; Steck, S.E.; Hebert, J.R.; Ma, Y.; Cauley, J.A.; Li, W.; Mossavar-Rahmani, Y.; Johnson, K.C.; Sattari, M.; et al. Dietary Inflammatory Index, Bone Mineral Density, and Risk of Fracture in Postmenopausal Women: Results From the Women’s Health Initiative. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2017, 32, 1136–1146. [Google Scholar] [CrossRef]
- Shivappa, N.; Blair, C.K.; Prizment, A.E.; Jacobs, D.R.; Hebert, J.R. Prospective study of the dietary inflammatory index and risk of breast cancer in postmenopausal women. Mol. Nutr. Food Res. 2017, 61, 1600592. [Google Scholar] [CrossRef]
- Shivappa, N.; Blair, C.K.; Prizment, A.E.; Jacobs, D.R., Jr.; Hebert, J.R. Dietary inflammatory index and risk of renal cancer in the Iowa Women’s Health Study. Eur. J. Nutr. 2018, 57, 1207–1213. [Google Scholar] [CrossRef]
- Tabung, F.K.; Steck, S.E.; Ma, Y.; Liese, A.D.; Zhang, J.; Lane, D.S.; Ho, G.Y.F.; Hou, L.; Snetselaar, L.; Ockene, J.K.; et al. Changes in the Inflammatory Potential of Diet Over Time and Risk of Colorectal Cancer in Postmenopausal Women. Am. J. Epidemiol. 2017, 186, 514–523. [Google Scholar] [CrossRef]
- Hebert, J.R. Social Desirability Trait: Biaser or Driver of Self-Reported Dietary Intake? J. Acad. Nutr. Diet. 2016, 116, 1895–1898. [Google Scholar] [CrossRef]
- Hebert, J.R.; Ebbeling, C.B.; Matthews, C.E.; Hurley, T.G.; Ma, Y.; Druker, S.; Clemow, L. Systematic errors in middle-aged women’s estimates of energy intake: Comparing three self-report measures to total energy expenditure from doubly labeled water. Ann. Epidemiol. 2002, 12, 577–586. [Google Scholar] [CrossRef]
- Hebert, J.R.; Ma, Y.; Clemow, L.; Ockene, I.S.; Saperia, G.; Stanek, E.J., 3rd; Merriam, P.A.; Ockene, J.K. Gender differences in social desirability and social approval bias in dietary self-report. Am. J. Epidemiol. 1997, 146, 1046–1055. [Google Scholar] [CrossRef]
- Anderson, K.B.; Holloway-Kew, K.L.; Hans, D.; Kotowicz, M.A.; Hyde, N.K.; Pasco, J.A. Physical and lifestyle factors associated with trabecular bone score values. Arch. Osteoporos. 2020, 15, 177. [Google Scholar] [CrossRef] [PubMed]
- Lanyan, A.; Marques-Vidal, P.; Gonzalez-Rodriguez, E.; Hans, D.; Lamy, O. Postmenopausal women with osteoporosis consume high amounts of vegetables but insufficient dairy products and calcium to benefit from their virtues: The CoLaus/OsteoLaus cohort. Osteoporos. Int. 2020, 31, 875–886. [Google Scholar] [CrossRef] [PubMed]
- Millar, C.L.; Kiel, D.P.; Hannan, M.T.; Sahni, S. Dairy food intake is not associated with spinal trabecular bone score in men and women: The Framingham Osteoporosis Study. Nutr. J. 2022, 21, 26. [Google Scholar] [CrossRef] [PubMed]
- Chuang, T.L.; Koo, M.; Chuang, M.H.; Lin, C.H.; Huang, C.H.; Wang, Y.F. Changes in Bone Mineral Density and Trabecular Bone Score over Time between Vegetarian and Non-Vegetarian Middle-Aged and Older Women: A Three-Year Retrospective Medical Record Review. Int. J. Environ. Res. Public. Health 2022, 19, 2445. [Google Scholar] [CrossRef] [PubMed]
- de Jonge, E.A.L.; Koromani, F.; Hofman, A.; Uitterlinden, A.G.; Franco, O.H.; Rivadeneira, F.; Kiefte-de Jong, J.C. Dietary acid load, trabecular bone integrity, and mineral density in an ageing population: The Rotterdam study. Osteoporos. Int. 2017, 28, 2357–2365. [Google Scholar] [CrossRef] [PubMed]
- Goldman, A.L.; Donlon, C.M.; Cook, N.R.; Manson, J.E.; Buring, J.E.; Copeland, T.; Yu, C.Y.; LeBoff, M.S. VITamin D and OmegA-3 TriaL (VITAL) bone health ancillary study: Clinical factors associated with trabecular bone score in women and men. Osteoporos. Int. 2018, 29, 2505–2515. [Google Scholar] [CrossRef] [PubMed]
- Leslie, W.D.; Krieg, M.A.; Hans, D.; Manitoba Bone Density, P. Clinical factors associated with trabecular bone score. J. Clin. Densitom. Off. J. Int. Soc. Clin. Densitom. 2013, 16, 374–379. [Google Scholar] [CrossRef] [PubMed]
- Coheley, L.M.; Shivappa, N.; Hebert, J.R.; Lewis, R.D. Dietary inflammatory index® and cortical bone outcomes in healthy adolescent children. Osteoporos. Int. 2019, 30, 1645–1654. [Google Scholar] [CrossRef]
- Shivappa, N.; Hebert, J.R.; Karamati, M.; Shariati-Bafghi, S.E.; Rashidkhani, B. Increased inflammatory potential of diet is associated with bone mineral density among postmenopausal women in Iran. Eur. J. Nutr. 2016, 55, 561–568. [Google Scholar] [CrossRef]
- Mazidi, M.; Shivappa, N.; Wirth, M.D.; Hebert, J.R.; Vatanparast, H.; Kengne, A.P. The association between dietary inflammatory properties and bone mineral density and risk of fracture in US adults. Eur. J. Clin. Nutr. 2017, 71, 1273–1277. [Google Scholar] [CrossRef]
- Taheri, E.; Mahdavi-Gorabi, A.; Moludi, J.; Asayesh, H.; Qorbani, M. A meta-analysis of dietary inflammatory index and bone health status. J. Diabetes Metab. Disord. 2022, 21, 109–121. [Google Scholar] [CrossRef] [PubMed]
- Biswas, S.K. Does the Interdependence between Oxidative Stress and Inflammation Explain the Antioxidant Paradox? Oxid. Med. Cell Longev. 2016, 2016, 5698931. [Google Scholar] [CrossRef] [PubMed]
- Zhao, F.; Guo, L.; Wang, X.; Zhang, Y. Correlation of oxidative stress-related biomarkers with postmenopausal osteoporosis: A systematic review and meta-analysis. Arch. Osteoporos. 2021, 16, 4. [Google Scholar] [CrossRef]
- Shivappa, N.; Hebert, J.R.; Marcos, A.; Diaz, L.E.; Gomez, S.; Nova, E.; Michels, N.; Arouca, A.; González-Gil, E.; Frederic, G.; et al. Association between dietary inflammatory index and inflammatory markers in the HELENA study. Mol. Nutr. Food Res. 2017, 61, 1600707. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.H.; Thaung Zaw, J.J.; Xian, C.J.; Howe, P.R. Regular Supplementation With Resveratrol Improves Bone Mineral Density in Postmenopausal Women: A Randomized, Placebo-Controlled Trial. J. Bone Min. Res. 2020, 35, 2121–2131. [Google Scholar] [CrossRef] [PubMed]
- Barbour, K.E.; Boudreau, R.; Danielson, M.E.; Youk, A.O.; Wactawski-Wende, J.; Greep, N.C.; LaCroix, A.Z.; Jackson, R.D.; Wallace, R.B.; Bauer, D.C.; et al. Inflammatory markers and the risk of hip fracture: The Women’s Health Initiative. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2012, 27, 1167–1176. [Google Scholar] [CrossRef] [PubMed]
- Barbour, K.E.; Lui, L.Y.; Ensrud, K.E.; Hillier, T.A.; LeBlanc, E.S.; Ing, S.W.; Hochberg, M.C.; Cauley, J.A.; Study of Osteoporotic Fractures Research Group. Inflammatory markers and risk of hip fracture in older white women: The study of osteoporotic fractures. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2014, 29, 2057–2064. [Google Scholar] [CrossRef]
- Gonzalez, A.; Simon, F.; Achiardi, O.; Vilos, C.; Cabrera, D.; Cabello-Verrugio, C. The Critical Role of Oxidative Stress in Sarcopenic Obesity. Oxid. Med. Cell Longev. 2021, 2021, 4493817. [Google Scholar] [CrossRef]
- Ishii, S.; Cauley, J.A.; Greendale, G.A.; Crandall, C.J.; Danielson, M.E.; Ouchi, Y.; Karlamangla, A.S. C-reactive protein, bone strength, and nine-year fracture risk: Data from the Study of Women’s Health Across the Nation (SWAN). J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2013, 28, 1688–1698. [Google Scholar] [CrossRef]
- Lumeng, C.N.; Saltiel, A.R. Inflammatory links between obesity and metabolic disease. J. Clin. Investig. 2011, 121, 2111–2117. [Google Scholar] [CrossRef]
- Park, S.; Na, W.; Sohn, C. Relationship between osteosarcopenic obesity and dietary inflammatory index in postmenopausal Korean women: 2009 to 2011 Korea National Health and Nutrition Examination Surveys. J. Clin. Biochem. Nutr. 2018, 63, 211–216. [Google Scholar] [CrossRef]
- National Institutes of Health. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults—The Evidence Report. Obes. Res. 1998, 6 (Suppl. S2), 51s–209s. [Google Scholar]
- Ilesanmi-Oyelere, B.L.; Coad, J.; Roy, N.; Kruger, M.C. Lean Body Mass in the Prediction of Bone Mineral Density in Postmenopausal Women. Biores. Open Access 2018, 7, 150–158. [Google Scholar] [CrossRef]

{kind=link}
| Alcohol | Energy (kcal) | Niacin | Selenium | Flavan-3-ol |
| Vitamin B12 | Total Fat | n-3 fatty acids | Thiamin | Flavones |
| Vitamin B6 | Fiber | n-6 fatty acids | Vitamin A | Flavonols |
| β-Carotene | Folic Acid | Protein | Vitamin C | Flavonones |
| Caffeine | Iron | PUFA | Vitamin D | Anthocyanidins |
| Carbohydrate | Magnesium | Riboflavin | Vitamin E | Isoflavones |
| Cholesterol | MUFA | Saturated Fat | Zinc |
| Characteristics | Overall (n = 272) | Q1 (n = 68) | Q2 (n = 68) | Q3 (n = 68) | Q4 (n = 68) | p Value * |
|---|---|---|---|---|---|---|
| Continuous Variables Mean (SD) | ||||||
| E-DII Mean (SD) | −2.0 ± (1.9) | −4.0 ± (0.5) | −2.8 ± (0.2) | −1.7 ± (0.4) | 0.6 ± (1.2) | <0.0001 |
| Age, years | 54.7 ± 3.3 | 54.7 ± 3.7 | 54.8 ± 3.1 | 54.7 ± 3.4 | 54.5 ± 3.0 | 0.74 |
| Calcium intake, mg | 1396.4 ± 604.2 | 1584.4 ± 620.2 | 1384.1 ± 572.7 | 1219.7 ± 533.0 | 1378.4 ± 640.7 | 0.01 † |
| Categorical Variables n (%) | ||||||
| BMI category ≤24.9 kg/m2 25–29.9 kg/m2 ≥30 kg/m2 | 124 (46) 71 (26) 77 (28) | 39 (57) 13 (19) 16 (24) | 34 (50) 16 (24) 18 (26) | 26 (38) 18 (26) 24 (35) | 25 (37) 24 (35) 19 (28) | 0.13 |
| Education Some college or less College degree Master’s or doctorate | 66 (22) 145 (54) 66 (24) | 14 (21) 34 (50) 20 (29) | 16 (24) 40 (60) 11 (16) | 16 (24) 37 (54) 15 (22) | 14 (21) 34 (50) 20 (29) | 0.62 |
| Race White/non-Hispanic Non-white/other | 241 (89) 31 (11) | 56 (82) 12 (18) | 63 (93) 5 (7) | 61 (90) 7 (10) | 61 (90) 7 (10) | 0.27 |
| Smoking status Ever smoker Never smoker | 56 (24) 176 (76) | 18 (30) 43 (70) | 12 (20) 49 (80) | 11 (21) 41 (79) | 15 (26) 43 (74) | 0.58 |
| Family history of osteoporosis | ||||||
| Yes No | 118 (44) 149 (56) | 36 (54) 31 (46) | 25 (37) 41 (63) | 31 (46) 36 (54) | 26 (39) 40 (61) | 0.21 |
| Physical activity Inactive Minimal HEPA | 89 (33) 92 (34) 90 (33) | 18 (27) 21 (31) 28 (42) | 14 (21) 26 (38) 28 (41) | 27 (40) 21 (31) 20 (29) | 30 (44) 24 (35) 14 (21) | 0.02 |
| Q1 | Q2 | Q3 | Q4 | p Value | |
|---|---|---|---|---|---|
| Adjusted Mean * ± SE | |||||
| Lumbar spine BMD (g/cm2) | 0.998 ± 0.022 | 1.025 ± 0.023 | 0.991 ± 0.023 | 0.995 ± 0.022 | 0.53 |
| Total hip BMD (g/cm2) | 0.913 ± 0.016 | 0.949 ± 0.017 | 0.936 ± 0.018 | 0.930 ± 0.017 | 0.29 |
| TBS-L1 | 1.338 ± 0.016 | 1.360 ± 0.017 | 1.345 ± 0.017 | 1.339 ± 0.017 | 0.65 |
| TBS-L2 | 1.374 ± 0.015 | 1.399 ± 0.016 | 1.370 ± 0.016 | 1.361 ± 0.016 | 0.19 |
| TBS-L3 | 1.374 ± 0.015 | 1.392 ± 0.016 | 1.358 ± 0.017 | 1.353 ± 0.016 | 0.13 |
| TBS-L4 | 1.336 ± 0.016 | 1.330 ± 0.017 | 1.314 ± 0.017 | 1.329 ± 0.017 | 0.69 |
| Total TBS L1-L4 | 1.000 ± 0.021 | 1.021 ± 0.022 | 0.994 ± 0.023 | 0.997 ± 0.022 | 0.69 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jackson, M.K.; Bilek, L.D.; Waltman, N.L.; Ma, J.; Hébert, J.R.; Price, S.; Graeff-Armas, L.; Poole, J.A.; Mack, L.R.; Hans, D.; et al. Dietary Inflammatory Potential and Bone Outcomes in Midwestern Post-Menopausal Women. Nutrients 2023, 15, 4277. https://doi.org/10.3390/nu15194277
Jackson MK, Bilek LD, Waltman NL, Ma J, Hébert JR, Price S, Graeff-Armas L, Poole JA, Mack LR, Hans D, et al. Dietary Inflammatory Potential and Bone Outcomes in Midwestern Post-Menopausal Women. Nutrients. 2023; 15(19):4277. https://doi.org/10.3390/nu15194277
Chicago/Turabian StyleJackson, Mariah Kay, Laura D. Bilek, Nancy L. Waltman, Jihyun Ma, James R. Hébert, Sherry Price, Laura Graeff-Armas, Jill A. Poole, Lynn R. Mack, Didier Hans, and et al. 2023. "Dietary Inflammatory Potential and Bone Outcomes in Midwestern Post-Menopausal Women" Nutrients 15, no. 19: 4277. https://doi.org/10.3390/nu15194277
APA StyleJackson, M. K., Bilek, L. D., Waltman, N. L., Ma, J., Hébert, J. R., Price, S., Graeff-Armas, L., Poole, J. A., Mack, L. R., Hans, D., Lyden, E. R., & Hanson, C. (2023). Dietary Inflammatory Potential and Bone Outcomes in Midwestern Post-Menopausal Women. Nutrients, 15(19), 4277. https://doi.org/10.3390/nu15194277