
Preparing Patients for Cosmetic Surgery and Aesthetic Procedures: Ensuring an Optimal Nutritional Status for Successful Results
 , ,
, ,
Abstract
:1. Introduction
2. Major Complications of Reconstructive Surgery, Aesthetic Surgery, and Aesthetic Medicine
Link between Nutritional Status and Complications
3. Key Nutrients for Individuals Undergoing Aesthetic Procedures
4. Dietary Pattern for Individuals Undergoing Aesthetic Procedures
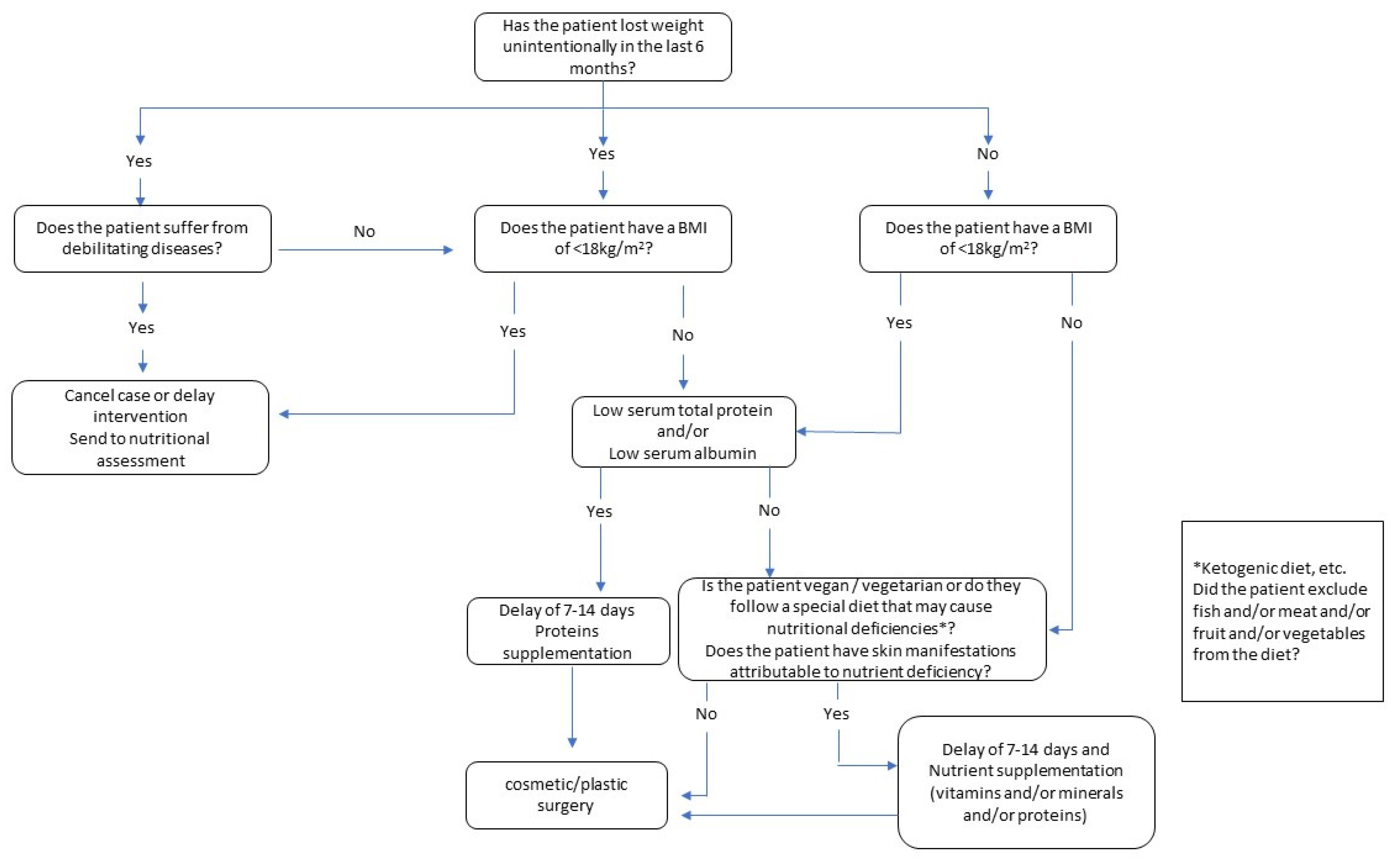
5. Reduction in the Risk of Complications through the Bundle Approach
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Furnham, A.; Levitas, J. Factors that Motivate People to Undergo Cosmetic Surgery. Can. J. Plast. Surg. 2012, 20, 47. [Google Scholar] [CrossRef] [Green Version]
- American Society of Plastic Surgeons. Plastic Surgery Procedural Statistics. 2022. Available online: https://www.globenewswire.com/news-release/2022/07/06/2474716/0/en/Cosmetic-Surgery-Global-Market-Report-2022.html (accessed on 26 July 2021).
- Levy, L.L.; Emer, J.J. Complications of Minimally Invasive Cosmetic Procedures: Prevention and Management. J. Cutan. Aesthet. Surg. 2012, 5, 121–132. [Google Scholar] [PubMed]
- Shermak, M.A. Body Contouring. Plast. Reconstr. Surg. 2012, 129, 963e–978e. [Google Scholar] [CrossRef] [PubMed]
- Khunger, N. Complications in Cosmetic Surgery: A Time to Reflect and Review and Not Sweep them Under the Carpet. J. Cutan. Aesthet. Surg. 2015, 8, 189–190. [Google Scholar] [CrossRef]
- Harrison, B.; Khansa, I.; Janis, J.E. Evidence-Based Strategies to Reduce Postoperative Complications in Plastic Surgery. Plast. Reconstr. Surg. 2016, 138, 51S–60S. [Google Scholar] [CrossRef]
- Pakize Özçiftci Yilmaz, C.D. The Effect of Malnutrition on Prognosis in Surgical Inpatients in the Intensive Care Unit. J. Clin. Med. Kazakhstan 2020, 4, 57–61. [Google Scholar] [CrossRef]
- Bozzetti, F.; Gianotti, L.; Braga, M.; Di Carlo, V.; Mariani, L. Postoperative Complications in Gastrointestinal Cancer Patients: The Joint Role of the Nutritional Status and the Nutritional Support. Clin. Nutr. 2007, 26, 698–709. [Google Scholar] [CrossRef]
- Correia, M.I.T.D.; Waitzberg, D.L. The Impact of Malnutrition on Morbidity, Mortality, Length of Hospital Stay and Costs Evaluated through a Multivariate Model Analysis. Clin. Nutr. 2003, 22, 235–239. [Google Scholar] [CrossRef]
- Cardinale, F.; Chinellato, I.; Caimmi, S.; Peroni, D.G.; Franceschini, F.; Miraglia Del Giudice, M.; Bernardini, R. Perioperative Period: Immunological Modifications. Int. J. Immunopathol. Pharmacol. 2011, 24, 3. [Google Scholar] [CrossRef]
- Sungurtekin, H.; Sungurtekin, U.; Balci, C.; Zencir, M.; Erdem, E. The Influence of Nutritional Status on Complications After Major Intraabdominal Surgery. J. Am. Coll. Nutr. 2004, 23, 227–232. [Google Scholar] [CrossRef]
- Shepherd, A.A. Nutrition for Optimum Wound Healing. Nurs. Stand. 2003, 18, 55–58. [Google Scholar]
- Yu, J.; Hunter, P.J.; Perry, J.A.; Cross, K.M. Plastic Surgery Patients are Malnourished: Utilizing the Canadian Malnutrition Screening Tool. Plast. Reconstr. Surg. Glob. Open 2016, 4, e1058. [Google Scholar] [CrossRef] [PubMed]
- Christensen, L. Normal and Pathologic Tissue Reactions to Soft Tissue Gel Fillers. Dermatol. Surg. 2007, 33 (Suppl. 2), 168. [Google Scholar]
- Vidal, P.; Berner, J.E.; Will, P.A. Managing Complications in Abdominoplasty: A Literature Review. Arch. Plast. Surg. 2017, 44, 457–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neaman, K.C.; Armstrong, S.D.; Baca, M.E.; Albert, M.; Vander Woude, D.L.; Renucci, J.D. Outcomes of Traditional Cosmetic Abdominoplasty in a Community Setting: A Retrospective Analysis of 1008 Patients. Plast. Reconstr. Surg. 2013, 131, 403e–410e. [Google Scholar] [CrossRef] [Green Version]
- Hurvitz, K.A.; Olaya, W.A.; Nguyen, A.; Wells, J.H. Evidence-Based Medicine: Abdominoplasty. Plast. Reconstr. Surg. 2014, 133, 1214–1221. [Google Scholar] [CrossRef] [PubMed]
- Washer, L.L.; Gutowski, K. Breast Implant Infections. Infect. Dis. Clin. North Am. 2012, 26, 111–125. [Google Scholar] [CrossRef]
- Alijotas-Reig, J.; Fernandez-Figueras, M.T.; Puig, L. Inflammatory, Immune-Mediated Adverse Reactions Related to Soft Tissue Dermal Fillers. Semin. Arthritis Rheum. 2013, 43, 241–258. [Google Scholar] [CrossRef]
- Najera, O.; Gonzalez, C.; Toledo, G.; Lopez, L.; Ortiz, R. Flow Cytometry Study of Lymphocyte Subsets in Malnourished and Well-Nourished Children with Bacterial Infections. Clin. Diagn. Lab. Immunol. 2004, 11, 577–580. [Google Scholar] [CrossRef] [Green Version]
- Savino, W.; Dardenne, M.; Velloso, L.A.; Dayse Silva-Barbosa, S. The Thymus is a Common Target in Malnutrition and Infection. Br. J. Nutr. 2007, 98 (Suppl. 1), 11. [Google Scholar] [CrossRef] [Green Version]
- Cunningham-Rundles, S.; McNeeley, D.F.; Moon, A. Mechanisms of Nutrient Modulation of the Immune Response. J. Allergy Clin. Immunol. 2005, 115, 1119–1128. [Google Scholar] [CrossRef]
- Lourenco, S.V.; Hussein, T.P.; Bologna, S.B.; Sipahi, A.M.; Nico, M.M.S. Oral Manifestations of Inflammatory Bowel Disease: A Review Based on the Observation of Six Cases. J. Eur. Acad. Dermatol. Venereol. 2010, 24, 204–207. [Google Scholar] [CrossRef]
- Kim, H.; Hwang, S.; Lim, K.; Jung, Y.; Ahnng-Min; Kim Song, J. Recurrent Auricular Keloids during Pregnancy. Arch. Plast. Surg. 2013, 40, 70–72. [Google Scholar] [CrossRef] [Green Version]
- Noishiki, C.; Hayasaka, Y.; Ogawa, R. Sex Differences in Keloidogenesis: An Analysis of 1659 Keloid Patients in Japan. Dermatol. Ther. 2019, 9, 747–754. [Google Scholar] [CrossRef] [Green Version]
- Katta, R.; Kramer, M.J. Skin and Diet: An Update on the Role of Dietary Change as a Treatment Strategy for Skin Disease. Skin Therapy Lett. 2018, 23, 1–5. [Google Scholar]
- Smith, K.E.; Fenske, N.A. Cutaneous Manifestations of Alcohol Abuse. J. Am. Acad. Dermatol. 2000, 43, 1–18. [Google Scholar] [CrossRef]
- Prendiville, J.S.; Manfredi, L.N. Skin Signs of Nutritional Disorders. Semin. Dermatol. 1992, 11, 88–97. [Google Scholar]
- Lawrence, A.C.; Schwartz, S.J. Isomerization and Losses of Trans $-Carotene in Sweet Potatoes as Affected by Processing Treatments. J. Agric. Food Chem. 1988, 36, 129–133. [Google Scholar]
- Araco, A.; Gravante, G.; Araco, F.; Sorge, R.; Cervelli, V. Postoperative Seromas After Abdominoplasty: A Retrospective Analysis of 494 Patients and Possible Risk Factors. Plast. Reconstr. Surg. 2009, 123, 158e–159e. [Google Scholar] [CrossRef]
- Matarasso, A. Liposuction as an Adjunct to a Full Abdominoplasty Revisited. Plast. Reconstr. Surg. 2000, 106, 1197–1205. [Google Scholar] [CrossRef]
- Klink, C.D.; Binnebosel, M.; Lucas, A.H.; Schachtrupp, A.; Grommes, J.; Conze, J.; Klinge, U.; Neumann, U.; Junge, K. Serum Analyses for Protein, Albumin and IL-1-RA Serve as Reliable Predictors for Seroma Formation After Incisional Hernia Repair. Hernia 2011, 15, 69–73. [Google Scholar] [CrossRef]
- Stoffels, K.; Overbergh, L.; Giulietti, A.; Kasran, A.; Bouillon, R.; Gysemans, C.; Mathieu, C. NOD Macrophages Produce High Levels of Inflammatory Cytokines upon Encounter of Apoptotic or Necrotic Cells. J. Autoimmun. 2004, 23, 9–15. [Google Scholar] [CrossRef]
- Veterans Affairs Total Parenteral Nutrition Cooperative Study Group. Perioperative Total Parenteral Nutrition in Surgical Patients. N. Engl. J. Med. 1991, 325, 525–532. [Google Scholar] [CrossRef]
- Dobner, J.; Kaser, S. Body Mass Index and the Risk of Infection—From Underweight to Obesity. Clin. Microbiol. Infect. 2018, 24, 24–28. [Google Scholar] [CrossRef] [Green Version]
- Strumia, R. Eating Disorders and the Skin. Clin. Dermatol. 2013, 31, 80–85. [Google Scholar] [CrossRef]
- Denner, A.M.; Townley, S.A. Preventing Extravasation from Central Venous Catheters. Anaesthesia 2006, 61, 614–615. [Google Scholar] [CrossRef]
- Bamgbade, O.A.; Rutter, T.W.; Nafiu, O.O.; Dorje, P. Postoperative Complications in Obese and Nonobese Patients. World J. Surg. 2007, 31, 556–560; discussion 561. [Google Scholar] [CrossRef]
- Strumia, R. Dermatologic Signs in Patients with Eating Disorders. Am. J. Clin. Dermatol. 2005, 6, 165–173. [Google Scholar] [CrossRef]
- Englesbe, M.J.; Lee, J.S.; He, K.; Fan, L.; Schaubel, D.E.; Sheetz, K.H.; Harbaugh, C.M.; Holcombe, S.A.; Campbell, D.A.J.; Sonnenday, C.J.; et al. Analytic Morphomics, Core Muscle Size, and Surgical Outcomes. Ann. Surg. 2012, 256, 255–261. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.S.; Terjimanian, M.N.; Tishberg, L.M.; Alawieh, A.Z.; Harbaugh, C.M.; Sheetz, K.H.; Holcombe, S.A.; Wang, S.C.; Sonnenday, C.J.; Englesbe, M.J. Surgical Site Infection and Analytic Morphometric Assessment of Body Composition in Patients Undergoing Midline Laparotomy. J. Am. Coll. Surg. 2011, 213, 236–244. [Google Scholar] [CrossRef] [Green Version]
- Tan, B.H.L.; Birdsell, L.A.; Martin, L.; Baracos, V.E.; Fearon, K.C.H. Sarcopenia in an Overweight or Obese Patient is an Adverse Prognostic Factor in Pancreatic Cancer. Clin. Cancer Res. 2009, 15, 6973–6979. [Google Scholar] [CrossRef] [Green Version]
- Gillis, C.; Hasil, L.; Kasvis, P.; Bibby, N.; Davies, S.J.; Prado, C.M.; West, M.A.; Shaw, C. Nutrition Care Process Model Approach to Surgical Prehabilitation in Oncology. Front. Nutr. 2021, 8, 644706. [Google Scholar] [CrossRef]
- Mazza, E.; Ferro, Y.; Pujia, R.; Mare, R.; Maurotti, S.; Montalcini, T.; Pujia, A. Mediterranean Diet in Healthy Aging. J. Nutr. Health Aging 2021, 25, 1076–1083. [Google Scholar] [CrossRef]
- Gillis, C.; Wischmeyer, P.E. Pre-Operative Nutrition and the Elective Surgical Patient: Why, how and what? Anaesthesia 2019, 74 (Suppl. 1), 27–35. [Google Scholar] [CrossRef] [Green Version]
- Gillis, C.; Davies, S.J.; Carli, F.; Wischmeyer, P.E.; Wootton, S.A.; Jackson, A.A.; Riedel, B.; Marino, L.V.; Levett, D.Z.H.; West, M.A. Current Landscape of Nutrition Within Prehabilitation Oncology Research: A Scoping Review. Front. Nutr 2021, 8, 644723. [Google Scholar] [CrossRef]
- Mechanick, J.I.; Kushner, R.F.; Sugerman, H.J.; Gonzalez-Campoy, J.M.; Collazo-Clavell, M.L.; Guven, S.; Spitz, A.F.; Apovian, C.M.; Livingston, E.H.; Brolin, R.; et al. American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic & Bariatric Surgery Medical Guidelines for Clinical Practice for the Perioperative Nutritional, Metabolic, and Nonsurgical Support of the Bariatric Surgery Patient. Surg. Obes. Relat. Dis. 2008, 4, 109. [Google Scholar]
- Solano, F. Metabolism and Functions of Amino Acids in the Skin. Adv. Exp. Med. Biol. 2020, 1265, 187–199. [Google Scholar]
- Agha-Mohammadi, S.; Hurwitz, D.J. Nutritional Deficiency of Post-Bariatric Surgery Body Contouring Patients: What Every Plastic Surgeon should Know. Plast. Reconstr. Surg. 2008, 122, 604–613. [Google Scholar] [CrossRef] [Green Version]
- Debats, I.B.J.G.; Wolfs, T.G.A.M.; Gotoh, T.; Cleutjens, J.P.M.; Peutz-Kootstra, C.J.; van der Hulst, R.R.W.J. Role of Arginine in Superficial Wound Healing in Man. Nitric Oxide 2009, 21, 175–183. [Google Scholar] [CrossRef]
- Molnar, J.A.; Underdown, M.J.; Clark, W.A. Nutrition and Chronic Wounds. Adv. Wound. Care 2014, 3, 663–681. [Google Scholar] [CrossRef]
- Wischmeyer, P.E. Glutamine and Heat Shock Protein Expression. Nutrition 2002, 18, 225–228. [Google Scholar] [CrossRef]
- Wang, W.; Wu, Z.; Dai, Z.; Yang, Y.; Wang, J.; Wu, G. Glycine Metabolism in Animals and Humans: Implications for Nutrition and Health. Amino Acids 2013, 45, 463–477. [Google Scholar] [CrossRef]
- Harris, C.L.; Fraser, C. Malnutrition in the Institutionalized Elderly: The Effects on Wound Healing. Ostomy Wound. Manage 2004, 50, 54–63. [Google Scholar]
- Russell, L. The Importance of Patients’ Nutritional Status in Wound Healing. Br. J. Nurs. 2001, 10, S42, S44–S49. [Google Scholar] [CrossRef]
- Busetto, L.; Dicker, D.; Azran, C.; Batterham, R.L.; Farpour-Lambert, N.; Fried, M.; Hjelmesæth, J.; Kinzl, J.; Leitner, D.R.; Makaronidis, J.M.; et al. Practical Recommendations of the Obesity Management Task Force of the European Association for the Study of Obesity for the Post-Bariatric Surgery Medical Management. Obes. Facts 2017, 10, 597–632. [Google Scholar] [CrossRef]
- Soleimani, Z.; Hashemdokht, F.; Bahmani, F.; Taghizadeh, M.; Memarzadeh, M.R.; Asemi, Z. Clinical and Metabolic Response to Flaxseed Oil Omega-3 Fatty Acids Supplementation in Patients with Diabetic Foot Ulcer: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Diabetes Complicat. 2017, 31, 1394–1400. [Google Scholar] [CrossRef] [PubMed]
- McDougle, D.R.; Watson, J.E.; Abdeen, A.A.; Adili, R.; Caputo, M.P.; Krapf, J.E.; Johnson, R.W.; Kilian, K.A.; Holinstat, M.; Das, A. Anti-Inflammatory Ω-3 Endocannabinoid Epoxides. Proc. Natl. Acad. Sci. USA 2017, 114, E6034–E6043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hackam, D.J.; Ford, H.R. Cellular, Biochemical, and Clinical Aspects of Wound Healing. Surg. Infect. 2002, 3 (Suppl. 1), 23. [Google Scholar] [CrossRef]
- Scholl, D.; Langkamp-Henken, B. Nutrient Recommendations for Wound Healing. J. Intraven. Nurs. 2001, 24, 124–132. [Google Scholar]
- Helming, L.; Böse, J.; Ehrchen, J.; Schiebe, S.; Frahm, T.; Geffers, R.; Probst-Kepper, M.; Balling, R.; Lengeling, A. 1alpha,25-Dihydroxyvitamin D3 is a Potent Suppressor of Interferon Gamma-Mediated Macrophage Activation. Blood 2005, 106, 4351–4358. [Google Scholar] [CrossRef] [Green Version]
- Pittas, A.G.; Lau, J.; Hu, F.B.; Dawson-Hughes, B. The Role of Vitamin D and Calcium in Type 2 Diabetes. A Systematic Review and Meta-Analysis. J. Clin. Endocrinol. Metab. 2007, 92, 2017–2029. [Google Scholar] [CrossRef]
- van Etten, E.; Decallonne, B.; Bouillon, R.; Mathieu, C. NOD Bone Marrow-Derived Dendritic Cells are Modulated by Analogs of 1,25-Dihydroxyvitamin D3. J. Steroid Biochem. Mol. Biol. 2004, 89–90, 457–459. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, B.M.; Fisher, B.J.; Kraskauskas, D.; Ward, S.; Wayne, J.S.; Brophy, D.F.; Fowler, A.A., III; Yager, D.R.; Natarajan, R. Vitamin C Promotes Wound Healing through Novel Pleiotropic Mechanisms. Int. Wound. J. 2016, 13, 572–584. [Google Scholar] [CrossRef]
- Chokesuwattanaskul, S.; Sukpat, S.; Duangpatra, J.; Buppajarntham, S.; Decharatanachart, P.; Mutirangura, A.; Patumraj, S. High Dose Oral Vitamin C and Mesenchymal Stem Cells Aid Wound Healing in a Diabetic Mouse Model. J. Wound Care 2018, 27, 334–339. [Google Scholar] [CrossRef]
- Chawla, J.; Kvarnberg, D. Hydrosoluble Vitamins. Handb. Clin. Neurol. 2014, 120, 891–914. [Google Scholar] [PubMed]
- Darling, A.M.; Chavarro, J.E.; Malspeis, S.; Harris, H.R.; Missmer, S.A. A Prospective Cohort Study of Vitamins B, C, E, and Multivitamin Intake and Endometriosis. J. Endometr. 2013, 5, 17–26. [Google Scholar] [CrossRef] [Green Version]
- Burns, J.L.; Mancoll, J.S.; Phillips, L.G. Impairments to Wound Healing. Clin. Plast. Surg. 2003, 30, 47–56. [Google Scholar] [CrossRef]
- Demling, R.H. Nutrition, Anabolism, and the Wound Healing Process: An Overview. Eplasty 2009, 9, e9. [Google Scholar]
- Todorovic, V. Food and Wounds: Nutritional Factors in Wound Formation and Healing. Br. J. Community Nurs. 2002, 7, 43–44, 46, 48 passim. [Google Scholar] [CrossRef]
- Ayello, E.A.; Thomas, D.R.; Litchford, M.A. Nutritional aspects of wound healing. Home Healthcare Nurse. 1999, 17, 719–730. [Google Scholar] [PubMed]
- Agren, M.S.; Franzén, L. Influence of Zinc Deficiency on Breaking Strength of 3-Week-Old Skin Incisions in the Rat. Acta Chir. Scand. 1990, 156, 667–670. [Google Scholar] [PubMed]
- Vargas-Ruiz, A.G.; Hernández-Rivera, G.; Herrera, M.F. Prevalence of Iron, Folate, and Vitamin B12 Deficiency Anemia After Laparoscopic Roux-En-Y Gastric Bypass. Obes. Surg. 2008, 18, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Sen, C.K.; Khanna, S.; Venojarvi, M.; Trikha, P.; Ellison, E.C.; Hunt, T.K.; Roy, S. Copper-Induced Vascular Endothelial Growth Factor Expression and Wound Healing. Am. J. Physiol. Heart Circ. Physiol. 2002, 282, 1821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tenaud, I.; Sainte-Marie, I.; Jumbou, O.; Litoux, P.; Dreno, B. In Vitro Modulation of Keratinocyte Wound Healing Integrins by Zinc, Copper and Manganese. Br. J. Dermatol. 1999, 140, 26–34. [Google Scholar] [CrossRef]
- Vaxman, F.; Olender, S.; Lambert, A.; Nisand, G.; Grenier, J.F. Can the Wound Healing Process be Improved by Vitamin Supplementation? Experimental Study on Humans. Eur. Surg. Res. 1996, 28, 306–314. [Google Scholar] [CrossRef]
- Talaei, M.; Koh, W.; Yuan, J.; van Dam, R.M. DASH Dietary Pattern, Mediation by Mineral Intakes, and the Risk of Coronary Artery Disease and Stroke Mortality. J. Am. Heart Assoc. 2019, 8, e011054. [Google Scholar] [CrossRef] [Green Version]
- Castro-Quezada, I.; Román-Viñas, B.; Serra-Majem, L. The Mediterranean Diet and Nutritional Adequacy: A Review. Nutrients 2014, 6, 231–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roy, M.; Hunter, P.; Perry, J.A.; Cross, K.M. Development of a Universal Nutritional Screening Platform for Plastic Surgery Patients. Plast. Reconstr. Surg. Glob. Open 2017, 5, e1342. [Google Scholar] [CrossRef] [PubMed]
- Detsky, A.S.; McLaughlin, J.R.; Baker, J.P.; Johnston, N.; Whittaker, S.; Mendelson, R.A.; Jeejeebhoy, K.N. What is Subjective Global Assessment of Nutritional Status? JPEN J. Parenter. Enteral Nutr. 1987, 11, 8–13. [Google Scholar] [CrossRef] [Green Version]
- Kondrup, J.; Rasmussen, H.H.; Hamberg, O.; Stanga, Z.; Ad Hoc ESPEN Working Group. Nutritional Risk Screening (NRS 2002): A New Method Based on an Analysis of Controlled Clinical Trials. Clin. Nutr. 2003, 22, 321–336. [Google Scholar] [CrossRef]
- Bakaloudi, D.R.; Halloran, A.; Rippin, H.L.; Oikonomidou, A.C.; Dardavesis, T.I.; Williams, J.; Wickramasinghe, K.; Breda, J.; Chourdakis, M. Intake and Adequacy of the Vegan Diet. A Systematic Review of the Evidence. Clin. Nutr. 2021, 40, 3503–3521. [Google Scholar] [CrossRef]
- Vitiello, V.; Germani, A.; Capuzzo Dolcetta, E.; Donini, L.M.; Del Balzo, V. The New Modern Mediterranean Diet Italian Pyramid. Ann. Ig. 2016, 28, 179–186. [Google Scholar] [PubMed]
- Wong, C.J. Involuntary Weight Loss. Med. Clin. North Am. 2014, 98, 625–643. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.M.; et al. Diagnostic Criteria for Malnutrition—An ESPEN Consensus Statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Matory, W.E.J.; O’Sullivan, J.; Fudem, G.; Dunn, R. Abdominal Surgery in Patients with Severe Morbid Obesity. Plast. Reconstr. Surg. 1994, 94, 976–987. [Google Scholar] [CrossRef] [PubMed]
- Gounden, V.; Vashisht, R.; Jialal, I. Hypoalbuminemia. In StatPearls; Anonymous; StatPearls Publishing LLC: Treasure Island, FL, USA, 2022. [Google Scholar]
- Muscaritoli, M.; Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Hutterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN Practical Guideline: Clinical Nutrition in Cancer. Clin. Nutr. 2021, 40, 2898–2913. [Google Scholar] [CrossRef]
- Tuck, C.J.; Biesiekierski, J.R.; Schmid-Grendelmeier, P.; Pohl, D. Food Intolerances. Nutrients 2019, 11, 1684. [Google Scholar] [CrossRef] [Green Version]
- Wilder-Smith, C.H.; Materna, A.; Wermelinger, C.; Schuler, J. Fructose and Lactose Intolerance and Malabsorption Testing: The Relationship with Symptoms in Functional Gastrointestinal Disorders. Aliment. Pharmacol. Ther. 2013, 37, 1074–1083. [Google Scholar] [CrossRef] [Green Version]
- Heath, M.L.; Sidbury, R. Cutaneous Manifestations of Nutritional Deficiency. Curr. Opin. Pediatr. 2006, 18, 417–422. [Google Scholar] [CrossRef]
- Wong, C.Y.; Chu, D.H. Cutaneous Signs of Nutritional Disorders. Int. J. Womens Dermatol. 2021, 7, 647–652. [Google Scholar] [CrossRef]

{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vitagliano, T.; Garieri, P.; Lascala, L.; Ferro, Y.; Doldo, P.; Pujia, R.; Pujia, A.; Montalcini, T.; Greco, M.; Mazza, E. Preparing Patients for Cosmetic Surgery and Aesthetic Procedures: Ensuring an Optimal Nutritional Status for Successful Results. Nutrients 2023, 15, 352. https://doi.org/10.3390/nu15020352
Vitagliano T, Garieri P, Lascala L, Ferro Y, Doldo P, Pujia R, Pujia A, Montalcini T, Greco M, Mazza E. Preparing Patients for Cosmetic Surgery and Aesthetic Procedures: Ensuring an Optimal Nutritional Status for Successful Results. Nutrients. 2023; 15(2):352. https://doi.org/10.3390/nu15020352
Chicago/Turabian StyleVitagliano, Tiziana, Pietro Garieri, Lidia Lascala, Yvelise Ferro, Patrizia Doldo, Roberta Pujia, Arturo Pujia, Tiziana Montalcini, Manfredi Greco, and Elisa Mazza. 2023. "Preparing Patients for Cosmetic Surgery and Aesthetic Procedures: Ensuring an Optimal Nutritional Status for Successful Results" Nutrients 15, no. 2: 352. https://doi.org/10.3390/nu15020352