
Immunomodulation of the Vaginal Ecosystem by Ligilactobacillus salivarius CECT 30632 Improves Pregnancy Rates among Women with Infertility of Unknown Origin or Habitual Abortions

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ligilactobacillus Salivarius CECT 30632
2.2. Assessment of Probiotic Properties of L. salivarius CECT 30632
2.3. L. Salivarius CECT 30632 to Increase Fertility-Related Outcomes: A Pilot Clinical Trial
2.4. Statistical Analysis
3. Results
3.1. Assessment of the Probiotic Potential of L. salivarius CECT 30632
3.2. Pilot Clinical Trial: General Description of the Recruited Women
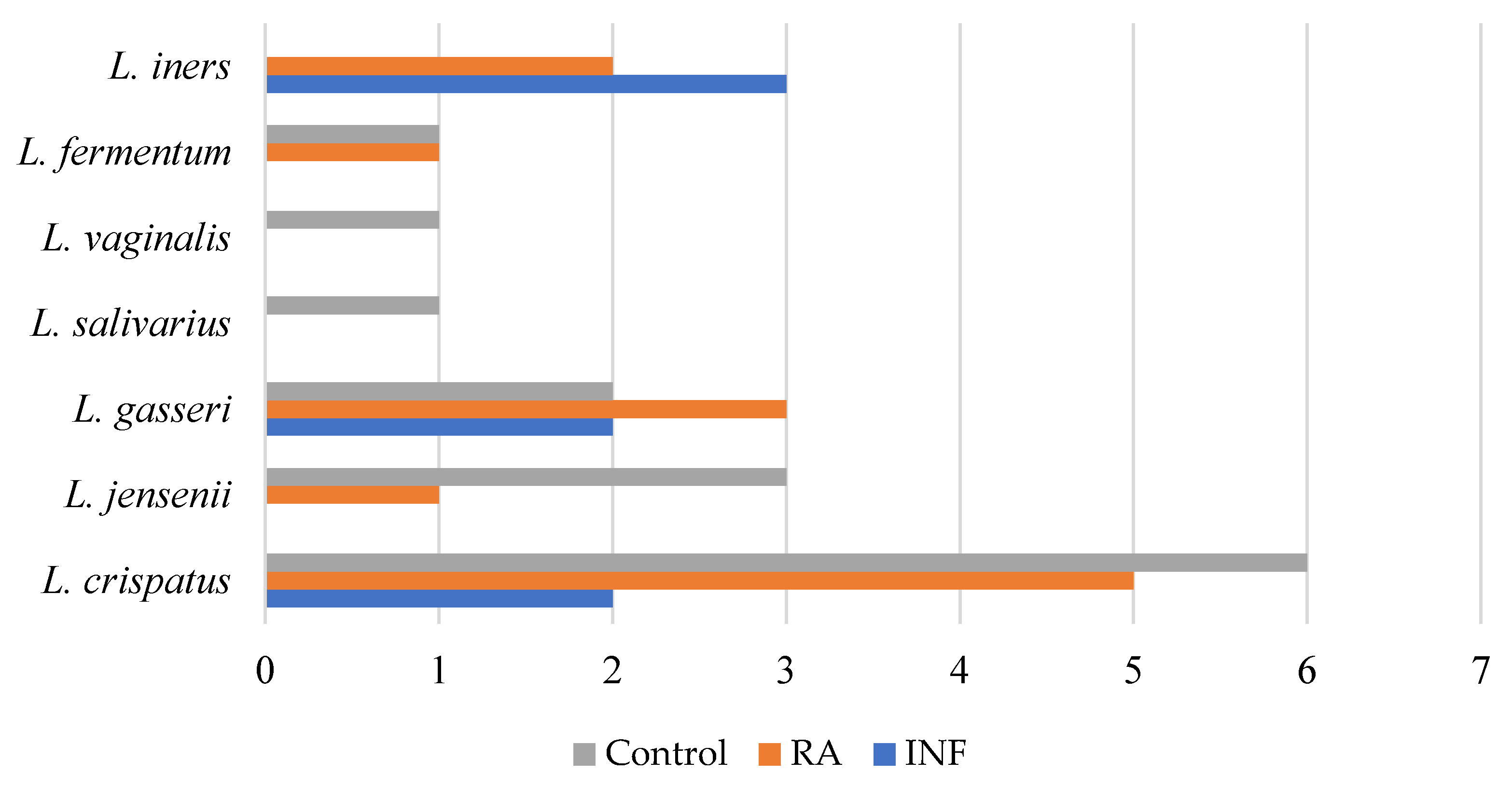
3.3. Pilot Clinical Trial: Vaginal-Related Parameters at Baseline
3.4. Pilot Clinical Trial: Pregnancy Effectiveness and Successful Pregnancy Effectiveness
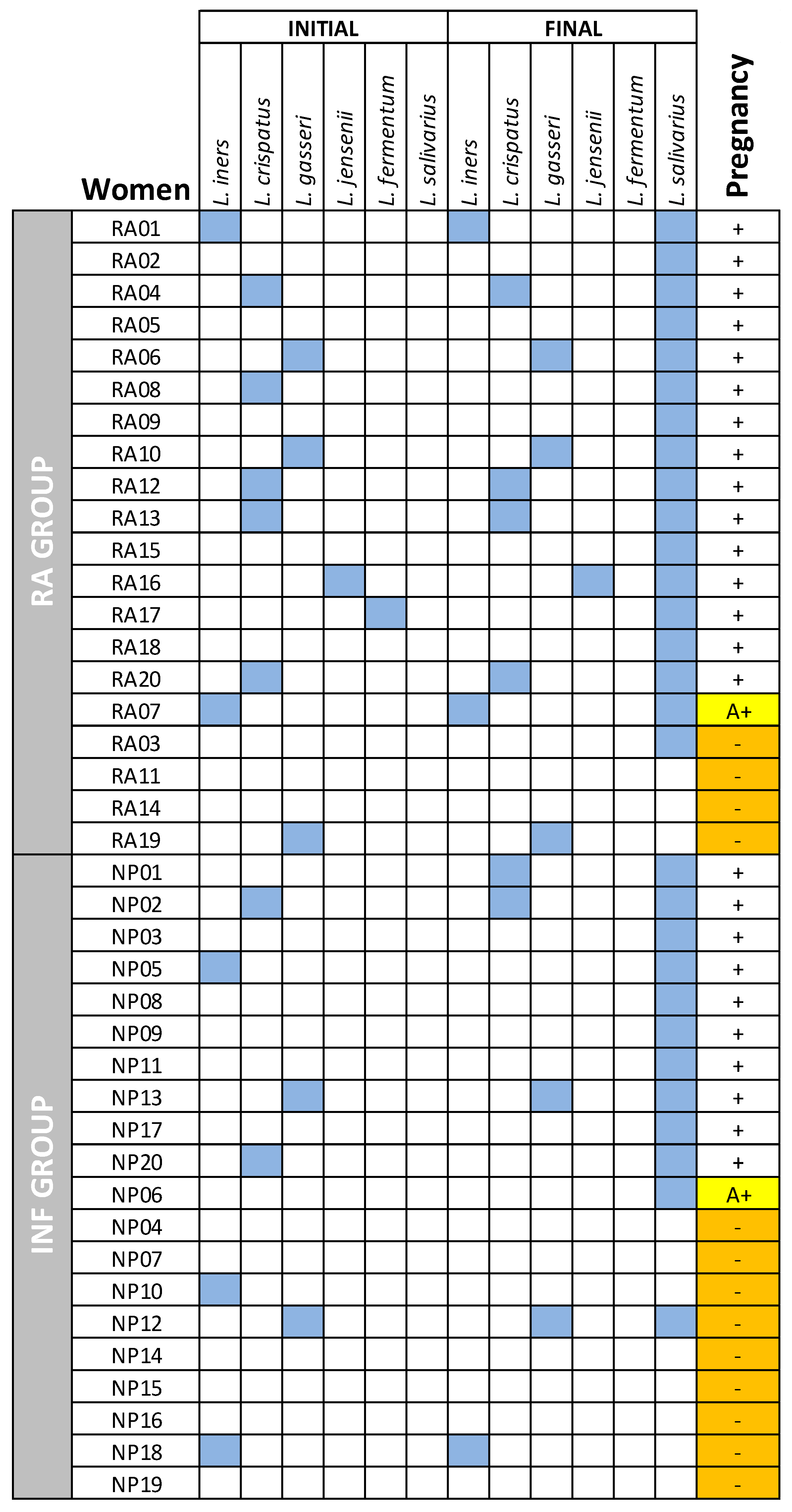
3.5. Pilot Clinical Trial: Secondary Outcomes in the RA and INF Groups
3.6. Comparison of Other Health and Safety Parameters between PC Women and Those Who Got Pregnant from the RA and INF Groups
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ravel, J.; Gajer, P.; Abdo, Z.; Schneider, G.M.; Koenig, S.S.; McCulle, S.L.; Karlebach, S.; Gorle, R.; Russell, J.; Tacket, C.O.; et al. Vaginal microbiome of reproductive-age women. Proc. Natl. Acad. Sci. USA 2011, 108 (Suppl. 1), 4680–4687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, B.; Tao, Z.; Edupuganti, L.; Serrano, M.G.; Buck, G.A. Roles of the microbiota of the female reproductive tract in gynecological and reproductive health. Microbiol. Mol. Biol. Rev. 2022, 86, e0018121. [Google Scholar] [CrossRef] [PubMed]
- Cascardi, E.; Cazzato, G.; Daniele, A.; Silvestris, E.; Cormio, G.; Di Vagno, G.; Malvasi, A.; Loizzi, V.; Scacco, S.; Pinto, V.; et al. Association between cervical microbiota and HPV: Could this be the key to complete cervical cancer eradication? Biology 2022, 11, 1114. [Google Scholar] [CrossRef]
- Kroon, S.J.; Ravel, J.; Huston, W.M. Cervicovaginal microbiota, women’s health, and reproductive outcomes. Fertil. Steril. 2018, 110, 327–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Memar, M.; Bobdiwala, S.; Fourie, H.; Mannino, R.; Lee, Y.S.; Smith, A.; Marchesi, J.R.; Timmerman, D.; Bourne, T.; Bennett, P.R.; et al. The association between vaginal bacterial composition and miscarriage: A nested case-control study. BJOG 2020, 127, 264–274. [Google Scholar] [CrossRef] [Green Version]
- Shahid, M.; Quinlivan, J.A.; Peek, M.; Castaño-Rodríguez, N.; Mendz, G.L. Is there an association between the vaginal microbiome and first trimester miscarriage? A prospective observational study. J. Obstet. Gynaecol. Res. 2022, 48, 119–128. [Google Scholar] [CrossRef]
- Moreno, I.; Codoñer, F.M.; Vilella, F.; Valbuena, D.; Martinez-Blanch, J.F.; Jimenez-Almazán, J.; Alonso, R.; Alamá, P.; Remohí, J.; Pellicer, A.; et al. Evidence that the endometrial microbiota has an effect on implantation success or failure. Am. J. Obstet. Gynecol. 2016, 215, 684–703. [Google Scholar] [CrossRef] [Green Version]
- Kyono, K.; Hashimoto, T.; Nagai, Y.; Sakuraba, Y. Analysis of endometrial microbiota by 16S ribosomal RNA gene sequencing among infertile patients: A single-center pilot study. Reprod. Med. Biol. 2018, 17, 297–306. [Google Scholar] [CrossRef]
- Reid, G.; Brigidi, P.; Burton, J.P.; Contractor, N.; Duncan, S.; Fargier, E.; Hill, C.; Lebeer, S.; Martín, R.; McBain, A.J.; et al. Microbes central to human reproduction. Am. J. Reprod. Immunol. 2015, 73, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Moreno, I.; Simon, C. Deciphering the effect of reproductive tract microbiota on human reproduction. Reprod. Med. Biol. 2019, 18, 40–50. [Google Scholar] [CrossRef]
- Reid, G.; Younes, J.A.; Van der Mei, H.C.; Gloor, G.B.; Knight, R.; Busscher, H.J. Microbiota restoration: Natural and supplemented recovery of human microbial communities. Nat. Rev. Microbiol. 2011, 9, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Fernández, L.; Castro, I.; Arroyo, R.; Alba, C.; Beltrán, D.; Rodríguez, J.M. Application of Ligilactobacillus salivarius CECT5713 to achieve term pregnancies in women with repetitive abortion or infertility of unknown origin by microbiological and immunological modulation of the vaginal ecosystem. Nutrients 2021, 13, 162. [Google Scholar] [CrossRef] [PubMed]
- Martín, V.; Cárdenas, N.; Ocaña, S.; Marín, M.; Arroyo, R.; Beltrán, D.; Badiola, C.; Fernández, L.; Rodríguez, J.M. Rectal and vaginal eradication of Streptococcus agalactiae (GBS) in pregnant women by using Lactobacillus salivarius CECT 9145, a target-specific probiotic strain. Nutrients 2019, 11, 810. [Google Scholar] [CrossRef] [Green Version]
- Magnusson, J.; Schnürer, J. Lactobacillus coryniformis subsp. coryniformis strain Si3 produces a broad-spectrum proteinaceous antifungal compound. Appl. Environ. Microbiol. 2001, 67, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martín, R.; Jiménez, E.; Olivares, M.; Marín, M.L.; Fernández, L.; Xaus, J.; Rodríguez, J.M. Lactobacillus salivarius CECT 5713, a potential probiotic strain isolated from infant feces and breast milk of a mother-child pair. Int. J. Food Microbiol. 2006, 112, 35–43. [Google Scholar] [CrossRef]
- Boris, S.; Suárez, J.E.; Vázquez, F.; Barbés, C. Adherence of human vaginal lactobacilli to vaginal epithelial cells and interaction with uropathogens. Infect. Immun. 1998, 66, 1985–1989. [Google Scholar] [CrossRef] [Green Version]
- Cohen, P.S.; Laux, D.C. Bacterial adhesion to and penetration of intestinal mucus in vitro. Methods Enzymol. 1995, 253, 309–314. [Google Scholar] [CrossRef]
- Nasioudis, D.; Beghini, J.; Bongiovanni, A.M.; Giraldo, P.C.; Linhares, I.M.; Witkin, S.S. α-Amylase in vaginal fluid: Association with conditions favorable to dominance of Lactobacillus. Reprod. Sci. 2015, 22, 1393–1398. [Google Scholar] [CrossRef]
- Padmavathi, T.; Bhargavi, R.; Priyanka, P.R.; Niranjan, N.R.; Pavitra, P.V. Screening of potential probiotic lactic acid bacteria and production of amylase and its partial purification. J. Genet. Eng. Biotechnol. 2018, 16, 357–362. [Google Scholar] [CrossRef]
- Narita, J.; Okano, K.; Kitao, T.; Ishida, S.; Sewaki, T.; Sung, M.-H.; Fukuda, H.; Kondo, A. Display of α-amylase on the surface of Lactobacillus casei cells by use of the PgsA anchor protein, and production of lactic acid from starch. Appl. Environ. Microbiol. 2006, 72, 269–275. [Google Scholar] [CrossRef]
- Marteau, P.; Minekus, M.; Havenaar, R.; Huis In’t Veld, J.H.J. Survival of lactic acid bacteria in a dynamic model of the stomach and small intestine: Validation and the effects of bile. J. Dairy Sci. 1997, 80, 1031–1037. [Google Scholar] [CrossRef]
- Martín, R.; Olivares, M.; Marín, M.L.; Fernández, L.; Xaus, J.; Rodríguez, J.M. Probiotic potential of 3 Lactobacilli strains isolated from breast milk. J. Hum. Lact. 2005, 21, 8–17. [Google Scholar] [CrossRef]
- EFSA. Guidance on the characterisation of microorganisms used as feed additives or as production organisms. EFSA J. 2018, 16, e05206. [Google Scholar] [CrossRef]
- Bover-Cid, S.; Holzapfel, W.H. Improved screening procedure for biogenic amine production by lactic acid bacteria. Int. J. Food Microbiol. 1999, 53, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.S.; Gopal, P.K.; Hill, H.S. Potential probiotic lactic acid bacteria Lactobacillus rhamnosus (HN001), Lactobacillus acidophilus (HN017) and Bifidobacterium lactis (HN019) do not degrade gastric mucin in vitro. Int. J. Food Microbiol. 2001, 63, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Anadón, A.; Martínez, M.A.; Ares, I.; Ramos, E.; Martínez-Larrañaga, M.R.; Contreras, M.M.; Ramos, M.; Recio, I. Acute and repeated dose (4 weeks) oral toxicity studies of two antihypertensive peptides, RYLGY and AYFYPEL, that correspond to fragments (90–94) and (143–149) from alpha(s1)-casein. Food Chem. Toxicol. 2010, 48, 1836–1845. [Google Scholar] [CrossRef]
- Lara-Villoslada, F.; Sierra, S.; Martín, R.; Delgado, S.; Rodríguez, J.M.; Olivares, M.; Xaus, J. Safety assessment of two probiotic strains, Lactobacillus coryniformis CECT5711 and Lactobacillus gasseri CECT5714. J. Appl. Microbiol. 2007, 103, 175–184. [Google Scholar] [CrossRef]
- Nakra, N.A.; Madan, R.P.; Buckley, N.; Huber, A.M.; Freiermuth, J.L.; Espinoza, L.; Walsh, J.; Parikh, U.M.; Penrose, K.J.; Keller, M.J.; et al. Loss of innate host defense following unprotected vaginal sex. J. Infect. Dis. 2016, 213, 840–847. [Google Scholar] [CrossRef] [Green Version]
- Mediano, P.; Fernández, L.; Jiménez, E.; Arroyo, R.; Espinosa-Martos, I.; Rodríguez, J.M.; Marín, M. Microbial diversity in milk of women with mastitis: Potential role of coagulase-negative staphylococci, viridans group streptococci, and corynebacteria. J. Hum. Lact. 2017, 33, 309–318. [Google Scholar] [CrossRef]
- Lackey, K.A.; Williams, J.E.; Meehan, C.L.; Zachek, J.A.; Benda, E.D.; Price, W.J.; Foster, J.A.; Sellen, D.W.; Kamau-Mbuthia, E.W.; Kamundia, E.W.; et al. What’s normal? Microbiomes in human milk and infant feces are related to each other but vary geographically: The INSPIRE study. Front. Nutr. 2019, 6, 45. [Google Scholar] [CrossRef]
- Harrow, S.A.; Ravindran, V.; Butler, R.C.; Marshall, J.W.; Tannock, G.W. Real-time quantitative PCR measurement of ileal Lactobacillus salivarius populations from broiler chickens to determine the influence of farming practices. Appl. Environ. Microbiol. 2007, 73, 7123–7127. [Google Scholar] [CrossRef] [Green Version]
- O’Hanlon, D.E.; Lanier, B.R.; Moench, T.R.; Cone, R.A. Cervicovaginal fluid and semen block the microbicidal activity of hydrogen peroxide produced by vaginal lactobacilli. BMC Infect. Dis. 2010, 10, 120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macklaim, J.M.; Clemente, J.C.; Knight, R.; Gloor, G.B.; Reid, G. Changes in vaginal microbiota following antimicrobial and probiotic therapy. Microb. Ecol. Health Dis. 2015, 26, 27799. [Google Scholar] [CrossRef]
- Tachedjian, G.; Aldunate, M.; Bradshaw, C.S.; Cone, R.A. The role of lactic acid production by probiotic Lactobacillus species in vaginal health. Res. Microbiol. 2017, 168, 782–792. [Google Scholar] [CrossRef] [PubMed]
- O’Hanlon, D.E.; Moench, T.R.; Cone, R.A. Vaginal pH and microbicidal lactic acid when lactobacilli dominate the microbiota. PLoS ONE 2013, 8, e80074. [Google Scholar] [CrossRef]
- O’Hanlon, D.E.; Come, R.A.; Moench, T.R. Vaginal pH measured in vivo: Lactobacilli determine pH and lactic acid concentration. BMC Microbiol. 2019, 19, 13. [Google Scholar] [CrossRef] [Green Version]
- Tachedjian, G.; O’Hanlon, D.E.; Ravel, J. The implausible “in vivo” role of hydrogen peroxide as an antimicrobial factor produced by vaginal microbiota. Microbiome 2018, 6, 29. [Google Scholar] [CrossRef] [Green Version]
- Hütt, P.; Lapp, E.; Štšepetova, J.; Smidt, I.; Taelma, H.; Borovkova, N.; Oopkaup, H.; Ahelik, A.; Rööp, T.; Hoidmets, D.; et al. Characterisation of probiotic properties in human vaginal lactobacilli strains. Microb. Ecol. Health Dis. 2016, 27, 30484. [Google Scholar] [CrossRef]
- Dellino, M.; Cascardi, E.; Laganà, A.S.; Di Vagno, G.; Malvasi, A.; Zaccaro, R.; Maggipinto, K.; Cazzato, G.; Scacco, S.; Tinelli, R.; et al. Lactobacillus crispatus M247 oral administration: Is it really an effective strategy in the management of papillomavirus-infected women. Infect. Agent. Cancer 2022, 17, 53. [Google Scholar] [CrossRef]
- Nardo, L.G. Vascular endothelial growth factor expression in the endometrium during the menstrual cycle, implantation window and early pregnancy. Curr. Opin. Obstet. Gynecol. 2005, 17, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Demir, R.; Yaba, A.; Huppertz, B. Vasculogenesis and angiogenesis in the endometrium during menstrual cycle and implantation. Acta Histochem. 2010, 112, 203–214. [Google Scholar] [CrossRef]
- Gordon, J.D.; Shifren, J.L.; Foulk, R.A.; Taylor, R.N.; Jaffe, R.B. Angiogenesis in the human female reproductive tract. Obstet. Gynecol. Surv. 1995, 50, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Licht, P.; Russu, V.; Lehmeyer, S.; Wissentheit, T.; Siebzehnrübl, E.; Wildt, L. Cycle dependency of intrauterine vascular endothelial growth factor levels is correlated with decidualization and corpus luteum function. Fertil. Steril. 2003, 80, 1228–1233. [Google Scholar] [CrossRef]
- Torry, D.S.; Leavenworth, J.; Chang, M.; Maheshwari, V.; Groesch, K.; Ball, E.R.; Torry, R.J. Angiogenesis in implantation. J. Assist. Reprod. Genet. 2007, 24, 303–315. [Google Scholar] [CrossRef] [Green Version]
- Meegdes, B.H.; Ingenhoes, R.; Peeters, L.L.; Exalto, N. Early pregnancy wastage: Relationship between chorionic vascularization and embryonic development. Fertil. Steril. 1988, 49, 216–220. [Google Scholar] [CrossRef]
- Vuorela, P.; Carpen, O.; Tulppala, M.; Halmesmaki, E. VEGF, its receptors and the tie receptors in recurrent miscarriage. Mol. Hum. Reprod. 2000, 6, 276–282. [Google Scholar] [CrossRef]
- Reynolds, L.P.; Caton, J.S.; Redmer, D.A.; Grazul-Bilska, A.T.; Vonnahme, K.A.; Borowicz, P.P.; Luther, J.S.; Wallace, J.M.; Wu, G.; Spencer, T.E. Evidence for altered placental blood flow and vascularity in compromised pregnancies. J. Physiol. 2006, 572, 51–58. [Google Scholar] [CrossRef]
- Robertson, S.A.; Ingman, W.V.; O’Leary, S.; Sharkey, D.J.; Tremellen, K.P. Transforming growth factor beta: A mediator of immune deviation in seminal plasma. J. Reprod. Immunol. 2002, 57, 109–128. [Google Scholar] [CrossRef]
- Wahl, S.M.; Wen, J.; Moutsopoulos, N. TGF-beta: A mobile purveyor of immune privilege. Immunol. Rev. 2006, 213, 213–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nocera, M.; Chu, T.M. Characterization of latent transforming growth factor-beta from human seminal plasma. Am. J. Reprod. Immunol. 1995, 33, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Loras, B.; Vételé, F.; El Malki, A.; Rollet, J.; Soufir, J.C.; Benahmed, M. Seminal transforming growth factor-beta in normal and infertile men. Hum. Reprod. 1999, 14, 1534–1539. [Google Scholar] [CrossRef] [Green Version]
- Chu, T.M.; Kawinski, E. Plasmin, substilisin-like endoproteases, tissue plasminogen activator, and urokinase plasminogen activator are involved in activation of latent TGF-beta 1 in human seminal plasma. Biochem. Biophys. Res. Commun. 1998, 253, 128–134. [Google Scholar] [CrossRef]
- Emami, N.; Diamandis, E.P. Potential role of multiple members of the kallikrein-related peptidase family of serine proteases in activating latent TGF beta 1 in semen. Biol. Chem. 2010, 391, 85–95. [Google Scholar] [CrossRef]
- Sharkey, D.J.; Macpherson, A.M.; Tremellen, K.P.; Mottershead, D.G.; Gilchrist, R.B.; Robertson, S.A. TGF-β mediates proinflammatory seminal fluid signaling in human cervical epithelial cells. J. Immunol. 2012, 189, 1024–1035. [Google Scholar] [CrossRef] [Green Version]
- Lindsay, K.L.; Kennelly, M.; Culliton, M.; Smith, T.; Maguire, O.C.; Shanahan, F.; Brennan, L.; McAuliffe, F.M. Probiotics in obese pregnancy do not reduce maternal fasting glucose: A double-blind, placebo-controlled, randomized trial (Probiotics in Pregnancy Study). Am. J. Clin. Nutr. 2014, 99, 1432–1439. [Google Scholar] [CrossRef] [Green Version]
- Fernández, L.; Cárdenas, N.; Arroyo, R.; Manzano, S.; Jiménez, E.; Martín, V.; Rodríguez, J.M. Prevention of infectious mastitis by oral administration of Lactobacillus salivarius PS2 during late pregnancy. Clin. Infect. Dis. 2016, 62, 568–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellonperä, O.; Mokkala, K.; Houttu, N.; Vahlberg, T.; Koivuniemi, E.; Tertti, K.; Rönnemaa, T.; Laitinen, K. Efficacy of fish oil and/or probiotic intervention on the incidence of gestational diabetes mellitus in an at-risk group of overweight and obese women: A randomized, placebo-controlled, double-blind clinical trial. Diabetes Care 2019, 42, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Jiménez, E.; Manzano, S.; Schlembach, D.; Arciszewski, K.; Martin, R.; Ben Amor, K.; Roelofs, M.; Knol, J.; Rodríguez, J.M.; Abou-Dakn, M.; et al. Ligilactobacillus salivarius PS2 supplementation during pregnancy and lactation prevents mastitis: A randomised controlled trial. Microorganisms 2021, 9, 1933. [Google Scholar] [CrossRef]
- Davidson, S.J.; Barrett, H.L.; Price, S.A.; Callaway, L.K.; Dekker Nitert, M. Probiotics for preventing gestational diabetes. Cochrane Database Syst. Rev. 2021, 4, CD009951. [Google Scholar] [CrossRef] [PubMed]
- Callaway, L.K.; McIntyre, H.D.; Barrett, H.L.; Foxcroft, K.; Tremellen, A.; Lingwood, B.E.; Tobin, J.M.; Wilkinson, S.; Kothari, A.; Morrison, M. Probiotics for the prevention of gestational diabetes mellitus in overweight and obese women: Findings from the SPRING double-blind randomized controlled trial. Diabetes Care 2019, 42, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Aaltonen, J.; Ojala, T.; Laitinen, K.; Piirainen, T.J.; Poussa, T.A.; Isolauri, E. Evidence of infant blood pressure programming by maternal nutrition during pregnancy: A prospective randomized controlled intervention study. J. Pediatr. 2008, 152, 79–84.e2. [Google Scholar] [CrossRef]
- Jamilian, M.; Bahmani, F.; Vahedpoor, Z.; Salmani, A.; Tajabadi-Ebrahimi, M.; Jafari, P.; Hashemi Dizaji, S.; Asemi, Z. Effects of probiotic supplementation on metabolic status in pregnant women: A randomized, double-blind, placebo-controlled trial. Arch. Iran Med. 2016, 19, 27743432. [Google Scholar] [PubMed]
- Wickens, K.L.; Barthow, C.A.; Murphy, R.; Abels, P.R.; Maude, R.M.; Stone, P.R.; Mitchell, E.A.; Stanley, T.V.; Purdie, G.L.; Kang, J.M. Early pregnancy probiotic supplementation with Lactobacillus rhamnosus HN001 may: A randomised controlled trial. Br. J. Nutr. 2017, 117, 804–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martín, R.; Soberón, N.; Vaneechoutte, M.; Flórez, A.B.; Vázquez, F.; Suárez, J.E. Characterization of indigenous vaginal lactobacilli from healthy women as probiotic candidates. Int. Microbiol. 2008, 11, 261–266. [Google Scholar] [CrossRef]
- Amabebe, E.; Anumba, D. The vaginal microenvironment: The physiologic role of lactobacilli. Front. Med. 2018, 5, 181. [Google Scholar] [CrossRef] [Green Version]
- Halper, J.; Leshin, L.S.; Lewis, S.J.; Li, W.I. Wound healing and angiogenic properties of supernatants from Lactobacillus cultures. Exp. Biol. Med. 2003, 228, 1329–1337. [Google Scholar] [CrossRef]
- Witkin, S.S.; Linhares, I.M. Why do lactobacilli dominate the human vaginal microbiota? BJOG 2017, 124, 606–611. [Google Scholar] [CrossRef] [Green Version]
- Kovachev, S. Defence factors of vaginal lactobacilli. Crit. Rev. Microbiol. 2018, 44, 31–39. [Google Scholar] [CrossRef]
- Koot, Y.E.; Teklenburg, G.; Salker, M.S.; Brosens, J.J.; Macklon, N.S. Molecular aspects of implantation failure. Biochim. Biophys. Acta. 2012, 1822, 1943–1950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ticconi, C.; Pietropolli, A.; Di Simone, N.; Piccione, E.; Fazleabas, A. Endometrial immune dysfunction in recurrent pregnancy loss. Int. J. Mol. Sci. 2019, 20, 5332. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Strain | Inhibition Zone (mm) | Co-Aggregation |
|---|---|---|
| G. vaginalis MP14 | 4.5 | ++ |
| G. vaginalis MP17 | 4.3 | ++ |
| G. vaginalis MP20 | 4.4 | ++ |
| G. vaginalis MP24 | 4.2 | ++ |
| G. vaginalis MP29 | 4.3 | ++ |
| S. agalactiae MP07 | 2.4 | + |
| S. agalactiae MP12 | 2.3 | + |
| S. agalactiae MP46 | 2.0 | + |
| C. albicans MP09 | 3.4 | ++ |
| C. albicans MP18 | 3.6 | ++ |
| C. albicans MP31 | 3.0 | ++ |
| C. glabrata MP33 | 2.8 | ++ |
| C. glabrata MP37 | 2.6 | ++ |
| C. parapsilosis MP36 | 2.9 | ++ |
| C. parapsilosis MP48 | 2.7 | ++ |
| U. urealyticum MP39 | 3.1 | + |
| U. urealyticum MP57 | 3.3 | + |
| Antibiotic a | GEN | KAN | STP | NEO | TET | ERY | CLI | CHL |
| MIC value | 2 | 128 | 32 | 4 | 2 | 0.25 | 0.5 | 2 |
| Breakpoint b | 16 | 64 (R c) | 64 | nr | 8 | 1 | 4 | 4 |
| Antibiotic | AMP | PEN | VAN | VIR | LIN | TRM | CIP | RIF |
| MIC value | 0.5 | 0.25 | >128 | 0.25 | 0.5 | 0.25 | 2 | |
| Breakpoint b | 4 | nr | nr (R c) | nr | nr | nr | nr | nr |
| NPC n = 14 | RA n = 20 | INF n = 20 | p-Value | ||
|---|---|---|---|---|---|
| Age (years) | Mean (95% CI) | 34.6 (33.5–35.8) a | 39.5 (38.51–40.49) b | 37.95 (36.92–38.98) b | <0.001 # |
| Range [min–max] | [28.0–45.0] | [35.0–43.0] | [35.0–44.1] | ||
| Weight (kg) | Mean (95% CI) | 62.4 (59.7–65.0) | 69.25 (66.05–72.45) | 67.55 (64.66–70.44) | 0.054 # |
| Range [min–max] | [46.0–87.0] | [54.0–86.0] | [55.0–82.0] | ||
| Height (cm) | Mean (95% CI) | 166 (164–168) | 166.99 (164.18–170.42) | 167.80 (165.48–170.12) | 0.624 # |
| Range [min–max] | [156–175] | [154–189] | [161–183] | ||
| Regularity of the menstrual cycle | Yes, n (%) | 10 (71) | 9 (45) | 10 (50) | 0.225 * |
| No, n (%) | 4 (29) | 11 (55) | 10 (50) | ||
| Duration menstrual cycle (days) | Mean (95% CI) | 28.0 (27.4–28.7) | 27.35 (26.73–27.97) | 27.58 (26.87–28.28) | 0.752 # |
| Range [min–max] | [25.0–32.5] | [24.0–30.0] | [24.0–30.0] | ||
| History of infections | |||||
| Vaginal | n (%) | 2 (14) | 12 (60) | 7 (35) | 0.024 * |
| Urinary tract | n (%) | 2 (14) | 12 (60) | 12 (60) | 0.013 * |
| Otorhinolaryngology | n (%) | 3 (21) | 7 (35) | 11 (55) | 0.128 * |
| Lower respiratory tract | n (%) | 2 (14) | 7 (35) | 7 (35) | 0.344 * |
| Skin | n (%) | 1 (7) | 3 (15) | 4 (20) | 0.999 * |
| Gastrointestinal | n (%) | 0 (0) | 1 (5) | 1 (5) | 1.000 |
| Antibiotic usage | |||||
| In infancy | n (%) | 4 (29) | 18 (90) | 14 (70) | <0.001 * |
| In adulthood | n (%) | 4 (29) | 15 (75) | 16 (80) | 0.016 * |
| History of other conditions | |||||
| Allergies | n (%) | 2 (14) | 5 (25) | 4 (20) | 0.995 * |
| Food intolerance | n (%) | 0 (0) | 7 (35) | 11 (55) | <0.001 * |
| Thyroid disease | n (%) | 0 (0) | 5 (25) | 3 (15) | 0.125 * |
| Control n = 14 | RA n = 20 | INF n = 20 | p-Value | ||
|---|---|---|---|---|---|
| pH | Mean (95% CI) | 4.53 (4.38–4.68) a | 5.74 (5.53–5.94) b | 6.03 (5.88–6.18) b | < 0.001 # |
| Range (min–max) | (4.20–5.00) | (4.70–6.40) | (4.90–6.30) | ||
| Nugent score | Mean (95% CI) | 1.79 (1.27–2.30) a | 6.55 (5.99–7.11) b | 6.40 (5.90–6.90) b | < 0.001 # |
| Range (min–max) | (0.00–4.00) | (4.00–8.00) | (4.00–8.00) | ||
| TGF-β1 (pg/mL) | Mean (95% CI) | 4.83 (4.65–5.01) a | 2.46 (2.19–2.72) b | 2.13 (1.98–2.27) b | < 0.001 # |
| Range (min–max) | (4.20–5.30) | (1.60–3.50) | (1.60–2.70) | ||
| TGF-β2 (pg/mL) | Mean (95% CI) | 3.22 (3.10–3.34) a | 1.50 (1.35–1.65) b | 1.35 (1.24–1.46) b | <0.001 # |
| Range (min–max) | (2.70–3.70) | (1.00–2.10) | (0.90–1.80) | ||
| VEGF (pg/mL) | Mean (95% CI) | 406.0 (322.0–490.0) a | 258.20 (203.76–312.64) a | 182.95 (136.19–229.71) b | 0.010 # |
| Range (min–max) | (1.4–929.0) | (99.0–479.0) | (69.0–433.0) | ||
| Lactobacilli | |||||
| positive women | n (%) | 14 (100) | 12 (60) | 7 (35) | <0.001 * |
| Viable counts (log10 CFU/mL) ** | Mean (95% CI) | 7.33 (7.15 -7.46) a | 4.19 (3.71–5.14) b | 3.65 (2.47–5.98) b | <0.001 # |
| Range (min–max) | (6.80–7.70) | (2.10–5.20) | (2.00–5.30) |
| Group | ||||
|---|---|---|---|---|
| Outcome | RA | INF | Total (RA+INF) | Ratio (95% CI) (RA/INF) |
| Pregnancy (no. events/total events) | 16/20 | 11/20 | 27/40 | |
| Pregnancy effectiveness (95% CI) | 80% (62.47–97.53%) | 55% (33.20–76.80%) | 67.5% (52.98–82.02%) | 1.45 (0.92–2.29) |
| Successful pregnancy * (no. events/total events) | 15/20 | 10/20 | 25/40 | |
| Reproductive success (95% CI) | 75% (56.02–93.98%) | 50% (28.09–71.91%) | 62.5% (47.50–77.50%) | 1.50 (0.90–2.49) |
| Pregnancy | |||
|---|---|---|---|
| Yes (n = 15) | No (n = 5) | ||
| Vaginal Parameter | (Mean (95% CI)) | (Mean (95% CI)) | p-Value # |
| pH | |||
| Baseline | 5.61 (5.37–5.84) | 6.16 (6.04–6.39) | 0.007 |
| Post-intervention | 4.44 (4.31–4.58) | 5.64 (5.43–6.06) | <0.001 |
| Change | −1.19 (−1.36–−0.86) | −0.52 (−0.62–−0.32) | <0.001 |
| p-value † | <0.001 | 0.025 | |
| Nugent score | |||
| Baseline | 6.31 (5.62–7.00) | 7.4 (7.12–7.95) | 0.074 |
| Post-intervention | 2.25 (1.72–2.78) | 6.2 (5.78–7.04) | 0.001 |
| Change | −4.2 (−4.68–−3.26) | −1.2 (−1.43–−0.75) | <0.001 |
| p-value † | <0.001 | 0.025 | |
| TGF-β1 (pg/mL) | |||
| Baseline | 2.64(2.36–2.91) | 1.78 (1.70–1.93) | 0.002 |
| Post-intervention | 4.18125 (3.94–4.42) | 2.18 (1.98–2.57) | 0.001 |
| Change | 1.59 (1.31–2.15) | 0.4 (0.26–0.67) | <0.001 |
| p-value † | <0.001 | 0.025 | |
| TGF-β2 (pg/mL) | |||
| Baseline | 1.59 (1.43–1.74) | 1.12 (0.98–1.39) | 0.007 |
| Post-intervention | 2.91 (2.69–3.13) | 1.34 (1.17–1.68) | 0.001 |
| Change | 1.36 (1.17–1.73) | 0.22 (0.03–0.59) | <0.001 |
| p-value † | <0.001 | 0.655 | |
| VEGF (pg/mL) | |||
| Baseline | 296.66 (239.09–354.16) | 106.60 (103.08–113.55) | 0.001 |
| Post-intervention | 586.88 (479.76–693.99) | 126.20 (113.63–151.04) | <0.001 |
| Change | 306.40 (233.76–449.93) | 19.6 (10.10–38.37) | <0.001 |
| p-value † | <0.001 | 0.025 | |
| Lactobacilli presence (n (%)) | |||
| Baseline | 10 (66.66) | 2 (40) | 0.172 * |
| Post-intervention | 15 (100) | 3 (60) | 0.052 * |
| Change | 5 (33.33) | 1 (20) | 0.613 * |
| Lactobacilli counts (log10 CFU/mL) | |||
| Baseline | 4.08 (3.58–5.08) | 4.75 (4.50–5.24) | 0.685 |
| Post-intervention | 7.34 (7.08–7.85) | 4.23 (3.42–5.84) | <0.001 |
| Change | 3.12 (2.51–4.33) | 0.4 (0.33–0.54) | <0.001 |
| p-value † | <0.001 | 0.525 | |
| L. salivarius qPCR (n (%)) | |||
| Initial | nd | nd | nd |
| Post-intervention | 15 (100) | 2 (40) | 0.035 * |
| L. salivariusqPCR (log10 copies/mL) ** | |||
| Initial | nd | nd | nd |
| Post-intervention | 7.81 (7.52–8.39) | 2.25 (1.50–3.73) | <0.001 |
| Pregnancy | |||
|---|---|---|---|
| Yes (n = 10) | No (n = 10) | ||
| Vaginal Parameter | (Mean (95% CI)) | (Mean (95% CI)) | p-Value # |
| pH | |||
| Baseline | 5.9 (5.68–6.12) | 6.16 (6.00–6.32) | 0.026 |
| Post-intervention | 4.49 (4.37–4.61) | 5.88 (5.69–6.07) | <0.001 |
| Change | −1.41 (−1.59–1.23) | −0.28 (−0.43–0.13) | <0.001 |
| p-value † | 0.001 | 0.002 | |
| Nugent score | |||
| Baseline | 6.2 (5.44–6.96) | 6.6 (5.93–7.27) | 0.571 |
| Post-intervention | 2 (1.42–2.58) | 5.7 (5.04–6.36) | <0.001 |
| Change | −4.2 (−4.90–3.50) | −0.9 (−1.44–0.36) | <0.001 |
| p-value † | 0.001 | 0.027 | |
| TGF-β1 (pg/mL) | |||
| Baseline | 2.26 (2.05–2.47) | 1.99 (1.82–2.16) | 0.070 |
| Post-intervention | 4.58 (4.39–4.77) | 2.23 (2.06–2.40) | <0.001 |
| Change | 2.32 (2.16–2.48) | 0.24 (0.09–0.39) | <0.001 |
| p-value † | 0.001 | 0.027 | |
| TGF-β2 (pg/mL) | |||
| Baseline | 1.51 (1.386–1.64) | 1.19 (1.09–1.29) | <0.001 |
| Post-intervention | 2.86 (2.72–3.00) | 1.33 (1.20–1.46) | <0.001 |
| Change | 1.35 (1.26–1.44) | 0.14 (0.06–0.22) | <0.001 |
| p-value † | 0.001 | 0.027 | |
| VEGF (pg/mL) | |||
| Baseline | 261.8 (203.52–320.08) | 104.1 (81.07–127.13) | <0.001 |
| Post-intervention | 734.1 (600.11–868.09) | 119.7 (89.24–150.16) | <0.001 |
| Change | 472.3 (379.31–565.29) | 15.6 (3.81–27.39) | <0.001 |
| p-value † | 0.001 | 0.057 | |
| Lactobacilli presence (n (%)) | |||
| Baseline | 4 (40) | 3 (30) | 1.000 * |
| Post-intervention | 10 (100) | 3 (30) | 0.003 * |
| Change | 6 (60) | 0 (0) | 0.020 * |
| Lactobacilli counts (log10 CFU/mL) | |||
| Initial | 3.26 (1.77–4.60) | 3.57 (1.81–5.12) | 0.290 |
| Post-intervention | 6.70 (6.19–7.15) | 5.4 (3.73–6.88) | 0.032 |
| Change | 3.23 (2.46–3.90) | 2.05 (0.05–3.82) | <0.001 |
| p-value † | <0.001 | 0.451 | |
| L. salivarius qPCR (n (%)) | |||
| Initial | nd | nd | - |
| Post-intervention | 10 (100) | 1 (10) | 0.002 * |
| L. salivariusqPCR (log10 copies/mL) ** | |||
| Initial | - | - | - |
| Post-intervention | 7.05 (6.39–7.63) | 4.20 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández, L.; Castro, I.; Arroyo, R.; Alba, C.; Beltrán, D.; Rodríguez, J.M. Immunomodulation of the Vaginal Ecosystem by Ligilactobacillus salivarius CECT 30632 Improves Pregnancy Rates among Women with Infertility of Unknown Origin or Habitual Abortions. Nutrients 2023, 15, 362. https://doi.org/10.3390/nu15020362
Fernández L, Castro I, Arroyo R, Alba C, Beltrán D, Rodríguez JM. Immunomodulation of the Vaginal Ecosystem by Ligilactobacillus salivarius CECT 30632 Improves Pregnancy Rates among Women with Infertility of Unknown Origin or Habitual Abortions. Nutrients. 2023; 15(2):362. https://doi.org/10.3390/nu15020362
Chicago/Turabian StyleFernández, Leónides, Irma Castro, Rebeca Arroyo, Claudio Alba, David Beltrán, and Juan M. Rodríguez. 2023. "Immunomodulation of the Vaginal Ecosystem by Ligilactobacillus salivarius CECT 30632 Improves Pregnancy Rates among Women with Infertility of Unknown Origin or Habitual Abortions" Nutrients 15, no. 2: 362. https://doi.org/10.3390/nu15020362
APA StyleFernández, L., Castro, I., Arroyo, R., Alba, C., Beltrán, D., & Rodríguez, J. M. (2023). Immunomodulation of the Vaginal Ecosystem by Ligilactobacillus salivarius CECT 30632 Improves Pregnancy Rates among Women with Infertility of Unknown Origin or Habitual Abortions. Nutrients, 15(2), 362. https://doi.org/10.3390/nu15020362