

Association between Mineral Intake and Cognition Evaluated by Montreal Cognitive Assessment (MoCA): A Cross-Sectional Study

 ,
,  , , , , , , , , and
, , , , , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
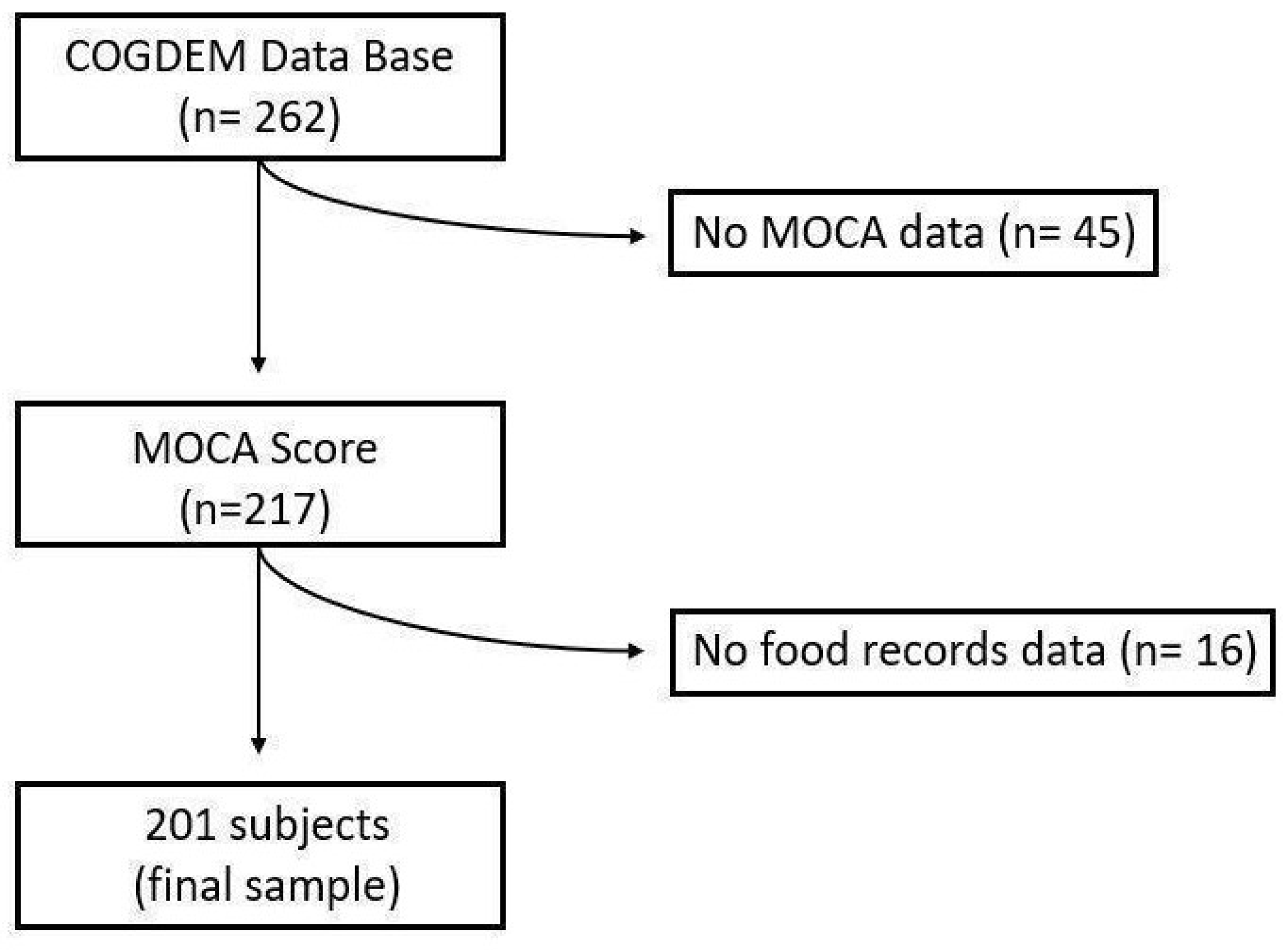
2.1. Participants
2.2. Health and Socio-Demographic Data
2.3. Food Record Data
2.4. Anthropometric Data
2.5. Physical Activity
2.6. APOE Genotyping
2.7. Neuropsychological Test
2.7.1. Geriatric Depression Scale (GDS)
2.7.2. Mini-Mental State Examination (MMSE)
2.7.3. Montreal Cognitive Assessment (MoCA)
2.8. Statistical Analysis
3. Results
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hou, Y.; Dan, X.; Babbar, M.; Wei, Y.; Hasselbalch, S.G.; Croteau, D.L.; Bohr, V.A. Aging as a Risk Factor for Neurodegenerative Disease. Nat. Rev. Neurol. 2019, 15, 565–581. [Google Scholar] [CrossRef]
- Sasitharan, P.K. Aging and Osteoarthritis. Subcell. Biochem. 2019, 91, 123–159. [Google Scholar] [CrossRef]
- Costantino, S.; Paneni, F.; Cosentino, F. Ageing, Metabolism and Cardiovascular Disease. J. Physiol. 2016, 594, 2061–2073. [Google Scholar] [CrossRef]
- OMS|Demencia: Una Prioridad de Salud Pública. Available online: https://iris.who.int/bitstream/handle/10665/98377/9789275318256_spa.pdf?sequence=1&isAllowed=y (accessed on 20 May 2020).
- Gale, S.A.; Acar, D.; Daffner, K.R. Dementia. Am. J. Med. 2018, 131, 1161–1169. [Google Scholar] [CrossRef]
- Deterioro Cognitivo Leve (DCL). Available online: https://www.alz.org/demencia-alzheimer/que-es-demencia/condiciones_relacionados/deterioro-cognitivo-leve?lang=en-US (accessed on 28 June 2022).
- Sanford, A.M. Mild Cognitive Impairment. Clin. Geriatr. Med. 2017, 33, 325–337. [Google Scholar] [CrossRef]
- Anderson, N.D. State of the Science on Mild Cognitive Impairment (MCI). CNS Spectr. 2019, 24, 78–87. [Google Scholar] [CrossRef]
- Morley, J.E. An Overview of Cognitive Impairment. Clin. Geriatr. Med. 2018, 34, 505–513. [Google Scholar] [CrossRef]
- Dembitsky, V.M.; Dzhemilev, L.; Gloriozova, T.; D’yakonov, V. Natural and Synthetic Drugs Used for the Treatment of Dementia. Biochem. Biophys. Res. Commun. 2020, 524, 772–783. [Google Scholar] [CrossRef]
- Panza, F.; Lozupone, M.; Solfrizzi, V.; Sardone, R.; Dibello, V.; Di Lena, L.; D’Urso, F.; Stallone, R.; Petruzzi, M.; Giannelli, G.; et al. Different Cognitive Frailty Models and Health-and Cognitive-Related Outcomes in Older Age: From Epidemiology to Prevention. J. Alzheimer’s Dis. 2018, 62, 993–1012. [Google Scholar] [CrossRef]
- Gatz, M.; Mack, W.J.; Chui, H.C.; Law, E.M.; Barisano, G.; Sutherland, M.L.; Sutherland, J.D.; Eid Rodriguez, D.; Quispe Gutierrez, R.; Copajira Adrian, J.; et al. Prevalence of Dementia and Mild Cognitive Impairment in Indigenous Bolivian Forager-Horticulturalists. Alzheimer’s Dement. 2023, 19, 44–55. [Google Scholar] [CrossRef]
- Au, B.; Dale-McGrath, S.; Tierney, M.C. Sex Differences in the Prevalence and Incidence of Mild Cognitive Impairment: A Meta-Analysis. Ageing Res. Rev. 2017, 35, 176–199. [Google Scholar] [CrossRef] [PubMed]
- Reitz, C. Genetic Diagnosis and Prognosis of Alzheimer’s Disease: Challenges and Opportunities. Expert Rev. Mol. Diagn. 2015, 15, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Sun, W.; Zhang, D. Association of Zinc, Iron, Copper, and Selenium Intakes with Low Cognitive Performance in Older Adults: A Cross-Sectional Study from National Health and Nutrition Examination Survey (NHANES). J. Alzheimer’s Dis. 2019, 72, 1145–1157. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, L.J.; Veronese, N.; Vernuccio, L.; Catanese, G.; Inzerillo, F.; Salemi, G.; Barbagallo, M. Nutrition, Physical Activity, and Other Lifestyle Factors in the Prevention of Cognitive Decline and Dementia. Nutrients 2021, 13, 4080. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Barbagallo, M. Nutritional Prevention of Cognitive Decline and Dementia. Acta Bio. Medica Atenei Parm. 2018, 89, 276. [Google Scholar] [CrossRef]
- Abbatecola, A.M.; Russo, M.; Barbieri, M. Dietary Patterns and Cognition in Older Persons. Curr. Opin. Clin. Nutr. Metab. Care 2018, 21, 10–13. [Google Scholar] [CrossRef]
- Scarmeas, N.; Anastasiou, C.A.; Yannakoulia, M. Nutrition and Prevention of Cognitive Impairment. Lancet Neurol. 2018, 17, 1006–1015. [Google Scholar] [CrossRef]
- Román, G.C.; Jackson, R.E.; Gadhia, R.; Román, A.N.; Reis, J. Mediterranean Diet: The Role of Long-Chain ω-3 Fatty Acids in Fish; Polyphenols in Fruits, Vegetables, Cereals, Coffee, Tea, Cacao and Wine; Probiotics and Vitamins in Prevention of Stroke, Age-Related Cognitive Decline, and Alzheimer Disease. Rev. Neurol. 2019, 175, 724–741. [Google Scholar] [CrossRef]
- Berendsen, A.M.; Kang, J.H.; Feskens, E.J.M.; de Groot, C.P.G.M.; Grodstein, F.; van de Rest, O. Association of Long-Term Adherence to the Mind Diet with Cognitive Function and Cognitive Decline in American Women. J. Nutr. Health Aging 2018, 22, 222–229. [Google Scholar] [CrossRef]
- Wang, Z.; Zhu, W.; Xing, Y.; Jia, J.; Tang, Y. B Vitamins and Prevention of Cognitive Decline and Incident Dementia: A Systematic Review and Meta-Analysis. Nutr. Rev. 2022, 80, 931–949. [Google Scholar] [CrossRef]
- Zhang, C.; Luo, J.; Yuan, C.; Ding, D. Vitamin B12, B6, or Folate and Cognitive Function in Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis. J. Alzheimer’s Dis. 2020, 77, 781–794. [Google Scholar] [CrossRef]
- Solfrizzi, V.; Colacicco, A.M.; D’Introno, A.; Capurso, C.; Torres, F.; Rizzo, C.; Capurso, A.; Panza, F. Dietary Intake of Unsaturated Fatty Acids and Age-Related Cognitive Decline: A 8.5-Year Follow-up of the Italian Longitudinal Study on Aging. Neurobiol. Aging 2006, 27, 1694–1704. [Google Scholar] [CrossRef]
- Martí, A.; Fortique, F. Omega-3 Fatty Acids and Cognitive Decline: A Systematic Review. Nutr. Hosp. 2019, 36, 939–949. [Google Scholar] [CrossRef]
- Araki, A.; Yoshimura, Y.; Sakurai, T.; Umegaki, H.; Kamada, C.; Iimuro, S.; Ohashi, Y.; Ito, H. Low Intakes of Carotene, Vitamin B2, Pantothenate and Calcium Predict Cognitive Decline among Elderly Patients with Diabetes Mellitus: The Japanese Elderly Diabetes Intervention Trial. Geriatr. Gerontol. Int. 2017, 17, 1168–1175. [Google Scholar] [CrossRef] [PubMed]
- Janka, Z. Tracing Trace Elements in Mental Functions. Clin. Neurosci. 2019, 72, 367–379. [Google Scholar] [CrossRef]
- Cardoso, B.R.; Szymlek-Gay, E.A.; Roberts, B.R.; Formica, M.; Gianoudis, J.; O’connell, S.; Nowson, C.A.; Daly, R.M. Selenium Status Is Not Associated with Cognitive Performance: A Cross-Sectional Study in 154 Older Australian Adults. Nutrients 2018, 10, 1847. [Google Scholar] [CrossRef]
- Lo, K.; Liu, Q.; Madsen, T.; Rapp, S.; Chen, J.C.; Neuhouser, M.; Shadyab, A.; Pal, L.; Lin, X.; Shumaker, S.; et al. Relations of Magnesium Intake to Cognitive Impairment and Dementia among Participants in the Women’s Health Initiative Memory Study: A Prospective Cohort Study. BMJ Open 2019, 9, e030052. [Google Scholar] [CrossRef]
- Tao, M.; Liu, J.; Cervantes, D. Association between Magnesium Intake and Cognition in US Older Adults: National Health and Nutrition Examination Survey (NHANES) 2011 to 2014. Alzheimer’s Dement. Transl. 2022, 8, e12250. [Google Scholar] [CrossRef]
- Wei, J.; Gianattasio, K.Z.; Bennett, E.E.; Stewart, J.D.; Xu, X.; Park, E.S.; Smith, R.L.; Ying, Q.; Whitsel, E.A.; Power, M.C. The Associations of Dietary Copper With Cognitive Outcomes. Am. J. Epidemiol. 2022, 191, 1202–1211. [Google Scholar] [CrossRef] [PubMed]
- Deficiencia y Sobrecarga de Hierro: Implicaciones en el Estado Oxidativo y la Salud Cardiovascular. Available online: https://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0212-16112010000300003 (accessed on 25 June 2023).
- Vilaplana, M. Antioxidantes Presentes En Los Alimentos. Vitaminas, Minerales y Suplementos. Offarm 2007, 26, 79–86. [Google Scholar]
- Meramat, A.; Rajab, N.F.; Shahar, S.; Sharif, R. Cognitive Impairment, Genomic Instability and Trace Elements. J. Nutr. Health Aging 2015, 19, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Klevay, L.M. Alzheimer’s Disease as Copper Deficiency. Med. Hypotheses 2008, 70, 802–807. [Google Scholar] [CrossRef] [PubMed]
- Nooyens, A.C.J.; Milder, I.E.J.; Van Gelder, B.M.; Bueno-De-Mesquita, H.B.; Van Boxtel, M.P.J.; Verschuren, W.M.M. Diet and Cognitive Decline at Middle Age: The Role of Antioxidants. Br. J. Nutr. 2015, 113, 1410–1417. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Tsoi, K.K.F.; Chan, J.Y.C.; Hirai, H.W.; Wong, A.; Mok, V.C.T.; Lam, L.C.W.; Kwok, T.C.Y.; Wong, S.Y.S. Recall Tests Are Effective to Detect Mild Cognitive Impairment: A Systematic Review and Meta-Analysis of 108 Diagnostic Studies. J. Am. Med. Dir. Assoc. 2017, 18, 807.e17–807.e29. [Google Scholar] [CrossRef]
- De Frutos-Lucas, J.; Cuesta, P.; Ramírez-Toraño, F.; Nebreda, A.; Cuadrado-Soto, E.; Peral-Suárez, Á.; Lopez-Sanz, D.; Bruña, R.; Marcos-De Pedro, S.; Delgado-Losada, M.L.; et al. Age and APOE Genotype Affect the Relationship between Objectively Measured Physical Activity and Power in the Alpha Band, a Marker of Brain Disease. Alzheimer’s Res. Ther. 2020, 12, 113. [Google Scholar] [CrossRef]
- de Frutos-Lucas, J.; López-Sanz, D.; Zuluaga, P.; Rodríguez-Rojo, I.C.; Luna, R.; López, M.E.; Delgado-Losada, M.L.; Marcos, A.; Barabash, A.; López-Higes, R.; et al. Physical Activity Effects on the Individual Alpha Peak Frequency of Older Adults with and without Genetic Risk Factors for Alzheimer’s Disease: A MEG Study. Clin. Neurophysiol. 2018, 129, 1981–1989. [Google Scholar] [CrossRef]
- Rosen, W.G.; Terry, R.D.; Fuld, P.A.; Katzman, R.; Peck, A. Pathological Verification of Ischemic Score in Differentiation of Dementias. Ann. Neurol. 1980, 7, 486–488. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and Validation of a Geriatric Depression Screening Scale: A Preliminary Report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Ortega, R.M.; Requejo, A.M. Registro de consumo de alimentos y bebidas. In Nutriguía. Manual de Nutrición Clínica; Editorial Panamericana: Madrid, Spain, 2015. [Google Scholar]
- Ortega, R.M.; López-Sobaler, A.M.; Andrés, P.; Requejo, A.M.; Aparicio, A.; Molinero, L.M. Programa DIAL Para Valoración de Dietas y Cálculos de Alimentación (Para Windows, Versión 3.0.0.5); Departamento de Nutrición (UCM) y Alceingeniería, S.A.: Madrid, Spain, 2013. [Google Scholar]
- Ortega, R.M.; López-Sobaler, A.M.; Andrés, P.; Aparicio, A. Composición nutricional de los alimentos. In Herramienta Para El Diseño y Valoración de Alimentos y Dietas; Departamento de Nutrición y Ciencia de Los Alimentos, Universidad Complutense de Madrid: Madrid, Spain, 2021; Available online: https://www.ucm.es/idinutricion/file/tca-2021?ver (accessed on 21 July 2022).
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for Total Energy Intake in Epidemiologic Studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1228S. [Google Scholar] [CrossRef]
- Institute of Medicine. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; The National Academies Press: Washington, DC, USA, 2001. [Google Scholar] [CrossRef]
- Institute of Medicine. Standing Committee on the Scientific Evaluation of Dietary Reference Intakes and Its Panel on Folate, Other B Vitamins, and Choline; The National Academy Press: Washintong, DC, USA, 1998. [Google Scholar]
- Institute of Medicine. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids; The National Academies Press: Washington, DC, USA, 2000. [Google Scholar] [CrossRef]
- Marfell-Jones, M.J.; Stewart, A.D.; de Ridder, J.H. International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Wellington, New Zealand, 2012. [Google Scholar]
- Durnin, J.V.; Fidanza, F. Evaluation of Nutritional Status. Bibl. Nutr. Dieta 1985, 35, 20–30. [Google Scholar]
- Barbany, M.; Remesar, X.; Carrillo, M.; Aranceta, J.; García-Luna, P.; Alemany, M.; Vázquez, C.; Palou, A.; Picó, C.; Soriguer, F.; et al. Obesidad; Sobrepeso; Epidemiología; Tratamiento; Prevención; Documento de Consenso. Med. Clin. 2000, 115, 587–597. [Google Scholar]
- WHO. Physical Status: The Use of and Interpretation of Anthropometry; Report of a WHO Expert Committee; WHO: Geneva, Switzerland, 1995. [Google Scholar]
- Pulakka, A.; Cheung, Y.B.; Ashorn, U.; Penpraze, V.; Maleta, K.; Phuka, J.C.; Ashorn, P. Feasibility and Validity of the ActiGraph GT3X Accelerometer in Measuring Physical Activity of Malawian Toddlers. Acta Paediatr. 2013, 102, 1192–1198. [Google Scholar] [CrossRef] [PubMed]
- Jefferis, B.J.; Sartini, C.; Shiroma, E.; Whincup, P.H.; Wannamethee, S.G.; Lee, I.M. Duration and Breaks in Sedentary Behaviour: Accelerometer Data from 1566 Community-Dwelling Older Men (British Regional Heart Study). Br. J. Sport. Med. 2015, 49, 1591–1594. [Google Scholar] [CrossRef] [PubMed]
- Ishii, K.; Shibata, A.; Adachi, M.; Nonoue, K.; Oka, K. Gender and Grade Differences in Objectively Measured Physical Activity and Sedentary Behavior Patterns among Japanese Children and Adolescents: A Cross-Sectional Study. BMC Public Health 2015, 15, 1254. [Google Scholar] [CrossRef] [PubMed]
- de Frutos Lucas, J.; Sewell, K.R.; García-Colomo, A.; Markovic, S.; Erickson, K.I.; Brown, B.M. How Does Apolipoprotein E Genotype Influence the Relationship between Physical Activity and Alzheimer’s Disease Risk? A Novel Integrative Model. Alzheimer’s Res. Ther. 2023, 15, 22. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br. J. Sport. Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”: A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Gallego, M.L.; Ferrándiz, M.H.; Garriga, O.T.; Nierga, I.P.; López-pousa, S.; Vilalta, J. Validación Del Montreal Cognitive Assessment ( MoCA): Test de Cribado Para El Deterioro Cognitivo Leve. Datos Preliminares. Alzheimer. Real Investig. Demenc. 2009, 43, 4–11. [Google Scholar]
- Klevay, L.M. Copper and Cognition. Clin. Neurophysiol. 2010, 121, 2177. [Google Scholar] [CrossRef]
- Meng, Q.; Liu, C.; Zu, C.; Wei, Y.; Su, X.; Gan, X.; Zhang, Y.; He, P.; Zhou, C.; Liu, M.; et al. Association Between Dietary Copper Intake and Cognitive Decline: A Perspective Cohort Study in Chinese Elderly. Am. J. Geriatr. Psychiatry 2023, 31, 753–763. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Huang, Y.; Wang, B.; Chen, H.; Pan, W.; Yang, M.; Xia, Z.; Zhang, R.; Yuan, C. Dietary Intake Levels of Iron, Copper, Zinc, and Manganese in Relation to Cognitive Function: A Cross-Sectional Study. Nutrients 2023, 15, 704. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.C.; Evans, D.A.; Tangney, C.C.; Bienias, J.L.; Schneider, J.A.; Wilson, R.S.; Scherr, P.A. Dietary Copper and High Saturated and Trans Fat Intakes Associated with Cognitive Decline. Arch. Neurol. 2006, 63, 1085–1088. [Google Scholar] [CrossRef] [PubMed]
- Loef, M.; Walach, H. Copper and Iron in Alzheimer’s Disease: A Systematic Review and Its Dietary Implications. Br. J. Nutr. 2012, 107, 7–19. [Google Scholar] [CrossRef] [PubMed]
- Cherbuin, N.; Kumar, R.; Sachdev, P.S.; Anstey, K.J. Dietary Mineral Intake and Risk of Mild Cognitive Impairment: The PATH through Life Project. Front. Aging Neurosci. 2014, 6, 4. [Google Scholar] [CrossRef]
- Vercambre, M.N.; Boutron-Ruault, M.C.; Ritchie, K.; Clavel-Chapelon, F.; Berr, C. Long-Term Association of Food and Nutrient Intakes with Cognitive and Functional Decline: A 13-Year Follow-up Study of Elderly French Women. Br. J. Nutr. 2009, 102, 419–427. [Google Scholar] [CrossRef]
- Pivina, L.; Semenova, Y.; Doşa, M.D.; Dauletyarova, M.; Bjørklund, G. Iron Deficiency, Cognitive Functions, and Neurobehavioral Disorders in Children. J. Mol. Neurosci. 2019, 68, 1–10. [Google Scholar] [CrossRef]
- Gómez Ramírez, S.; Remacha Sevilla, Á.F.; Muñoz Gómez, M. Anaemia in the Elderly. Med. Clin. 2017, 149, 496–503. [Google Scholar] [CrossRef]
- Agrawal, S.; Berggren, K.L.; Marks, E.; Fox, J.H. Impact of High Iron Intake on Cognition and Neurodegeneration in Humans and in Animal Models: A Systematic Review. Nutr. Rev. 2017, 75, 456–470. [Google Scholar] [CrossRef]
- Sparks, D.L.; Schreurs, B.G. Trace Amounts of Copper in Water Induce β-Amyloid Plaques and Learning Deficits in a Rabbit Model of Alzheimer’s Disease. Proc. Natl. Acad. Sci. USA 2003, 100, 11065–11069. [Google Scholar] [CrossRef]
- Erikson, K.M.; Aschner, M. Manganese: Its Role in Disease and Health. Met. Ions Life Sci. 2019, 19, 253–266. [Google Scholar] [CrossRef]
- Aschner, M.; Erikson, K. Manganese. Adv. Nutr. 2017, 8, 520–521. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Bornhorst, J.; Aschner, M. Manganese Metabolism in Humans. Front. Biosci. 2018, 23, 1655–1679. [Google Scholar] [CrossRef] [PubMed]
- Soares, A.T.G.; Silva, A.d.C.; Tinkov, A.A.; Khan, H.; Santamaría, A.; Skalnaya, M.G.; Skalny, A.V.; Tsatsakis, A.; Bowman, A.B.; Aschner, M.; et al. The Impact of Manganese on Neurotransmitter Systems. J. Trace Elem. Med. Biol. 2020, 61, 126554. [Google Scholar] [CrossRef] [PubMed]
- Velho, S.; Marques-Vidal, P.; Baptista, F.; Camilo, M.E. Dietary Intake Adequacy and Cognitive Function in Free-Living Active Elderly: A Cross-Sectional and Short-Term Prospective Study. Clin. Nutr. 2008, 27, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Aschner, J.L.; Aschner, M. Nutritional Aspects of Manganese Homeostasis. Mol. Aspects Med. 2005, 26, 353–362. [Google Scholar] [CrossRef]
- Gibbons, R.A.; Dixon, S.N.; Hallis, K.; Russell, A.M.; Sansom, B.F.; Symonds, H.W. Manganese Metabolism in Cows and Goats. BBA-Gen. Subj. 1976, 444, 1–10. [Google Scholar] [CrossRef]
- Reaney, S.H.; Bench, G.; Smith, D.R. Brain Accumulation and Toxicity of Mn(II) and Mn(III) Exposures. Toxicol. Sci. 2006, 93, 114–124. [Google Scholar] [CrossRef]
- Maier, J.A.M.; Locatelli, L.; Fedele, G.; Cazzaniga, A.; Mazur, A. Magnesium and the Brain: A Focus on Neuroinflammation and Neurodegeneration. Int. J. Mol. Sci. 2023, 24, 223. [Google Scholar] [CrossRef]
- Ozawa, M.; Ninomiya, T.; Ohara, T.; Hirakawa, Y.; Doi, Y.; Hata, J.; Uchida, K.; Shirota, T.; Kitazono, T.; Kiyohara, Y. Self-Reported Dietary Intake of Potassium, Calcium, and Magnesium and Risk of Dementia in the Japanese: The Hisayama Study. J. Am. Geriatr. Soc. 2012, 60, 1515–1520. [Google Scholar] [CrossRef]
- Bojar, I.; Wierzbińska-Stępniak, A.; Witczak, M.; Raczkiewicz, D.; Owoc, A. Are Cognitive Functions in Post-Menopausal Women Related with the Contents of Macro- and Micro-Components in the Diet? Ann. Agric. Environ. Med. 2015, 22, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Rayman, M.P. Selenium and Human Health. Lancet 2012, 379, 1256–1268. [Google Scholar] [CrossRef]
- Steinbrenner, H.; Klotz, L.O. Selenium and Zinc: “Antioxidants” for Healthy Aging? Z. Gerontol. Geriatr. 2020, 53, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Solovyev, N.D. Importance of Selenium and Selenoprotein for Brain Function: From Antioxidant Protection to Neuronal Signalling. J. Inorg. Biochem. 2015, 153, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wang, H.; Zhang, F.; Cui, Y.; Zhang, D.; Shen, X. Threshold Effects and Interactive Effects of Total Zinc and Selenium Intake on Cognitive Function in Older Adults. Clin. Nutr. ESPEN 2022, 47, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Berti, V.; Murray, J.; Davies, M.; Spector, N.; Tsui, W.H.; Li, Y.; Williams, S.; Pirraglia, E.; Vallabhajosula, S.; McHugh, P.; et al. Nutrient Patterns and Brain Biomarkers of Alzheimer’s Disease in Cognitively Normal Individuals. J. Nutr. Health Aging 2015, 19, 413–423. [Google Scholar] [CrossRef]
- Wang, Y.; Sun, X.; Ma, H.; Qu, X.; Wang, H. Iron, Zinc and Copper from Cereal Food Sources and Cognitive Performance in Older Adults in China. Iran. J. Public Health 2021, 50, 2546–2554. [Google Scholar] [CrossRef]
- Bush, A.I.; Pettingell, W.H.; Multhaup, G.; Paradis, M.D.; Vonsattel, J.P.; Gusella, J.F.; Beyreuther, K.; Masters, C.L.; Tanzi, R.E. Rapid Induction of Alzheimer A Beta Amyloid Formation by Zinc. Science 1994, 265, 1464–1467. [Google Scholar] [CrossRef]
- Pinto, T.C.C.; Machado, L.; Bulgacov, T.M.; Rodrigues-Júnior, A.L.; Costa, M.L.G.; Ximenes, R.C.C.; Sougey, E.B. Is the Montreal Cognitive Assessment (MoCA) Screening Superior to the Mini-Mental State Examination (MMSE) in the Detection of Mild Cognitive Impairment (MCI) and Alzheimer’s Disease (AD) in the Elderly? Int. Psychogeriatr. 2019, 31, 491–504. [Google Scholar] [CrossRef]
- Pendlebury, S.T.; Markwick, A.; De Jager, C.A.; Zamboni, G.; Wilcock, G.K.; Rothwell, P.M. Differences in Cognitive Profile between TIA, Stroke and Elderly Memory Research Subjects: A Comparison of the MMSE and MoCA. Cerebrovasc. Dis. 2012, 34, 48–54. [Google Scholar] [CrossRef]
- Ortega, R.M.; Perez-Rodrigo, C.; Lopez-Sobaler, A.M. Métodos de Evaluación de La Ingesta Actual: Registro o Diario Dietético. Nutr. Hosp. 2015, 31, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Food and Agricultural Organization. Dietary Assessment: A Resource Guide to Method Selection and Application in Low Resource Settings; Food and Agricultural Organization: Rome, Italy, 2018. [Google Scholar]
- Larouche, E.; Tremblay, M.P.; Potvin, O.; Laforest, S.; Bergeron, D.; Laforce, R.; Monetta, L.; Boucher, L.; Tremblay, P.; Belleville, S.; et al. Normative Data for the Montreal Cognitive Assessment in Middle-Aged and Elderly Quebec-French People. Arch. Clin. Neuropsychol. 2016, 31, 819–826. [Google Scholar] [CrossRef] [PubMed]
- Borland, E.; Nägga, K.; Nilsson, P.M.; Minthon, L.; Nilsson, E.D.; Palmqvist, S. The Montreal Cognitive Assessment: Normative Data from a Large Swedish Population-Based Cohort. J. Alzheimer’s Dis. 2017, 59, 893. [Google Scholar] [CrossRef] [PubMed]
- Thomann, A.E.; Goettel, N.; Monsch, R.J.; Berres, M.; Jahn, T.; Steiner, L.A.; Monsch, A.U. The Montreal Cognitive Assessment: Normative Data from a German-Speaking Cohort and Comparison with International Normative Samples. J. Alzheimer’s Dis. 2018, 64, 643–655. [Google Scholar] [CrossRef] [PubMed]
- Xiao, J.; Katsumata, N.; Bernier, F.; Ohno, K.; Yamauchi, Y.; Odamaki, T.; Yoshikawa, K.; Ito, K.; Kaneko, T. Probiotic Bifidobacterium Breve in Improving Cognitive Functions of Older Adults with Suspected Mild Cognitive Impairment: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Alzheimer’s Dis. 2020, 77, 139–147. [Google Scholar] [CrossRef]
- Handajani, Y.S.; Turana, Y.; Yogiara, Y.; Widjaja, N.T.; Sani, T.P.; Christianto, G.A.M.; Suwanto, A. Tempeh Consumption and Cognitive Improvement in Mild Cognitive Impairment. Dement. Geriatr. Cogn. Disord. 2021, 49, 497–502. [Google Scholar] [CrossRef]
- Ismail, Z.; Elbayoumi, H.; Fischer, C.E.; Hogan, D.B.; Millikin, C.P.; Schweizer, T.; Mortby, M.E.; Smith, E.E.; Patten, S.B.; Fiest, K.M. Prevalence of Depression in Patients with Mild Cognitive Impairment. JAMA Psychiatry 2017, 74, 58–67. [Google Scholar] [CrossRef]
- Johnson, L.A.; Mauer, C.; Jahn, D.; Song, M.; Wyshywaniuk, L.; Hall, J.R.; Balldin, V.H.; O’Bryant, S.E. Cognitive Differences among Depressed and Non-Depressed MCI Participants: A Project FRONTIER Study. Int. J. Geriatr. Psychiatry 2013, 28, 377–382. [Google Scholar] [CrossRef]
- Chow, Y.Y.; Verdonschot, M.; McEvoy, C.T.; Peeters, G. Associations between Depression and Cognition, Mild Cognitive Impairment and Dementia in Persons with Diabetes Mellitus: A Systematic Review and Meta-Analysis. Diabetes Res. Clin. Pract. 2022, 185, 109227. [Google Scholar] [CrossRef]


{kind=link}
| Total | Women | Men | ||||
|---|---|---|---|---|---|---|
| Non-CI | CI | Non-CI | CI | Non-CI | CI | |
| n | 92 | 109 | 58 | 69 | 34 | 40 |
| Age (X ± SD) | 58.6 ± 7.9 | 60.7 ± 7.8 | 58.5 ± 7.3 | 60.1 ± 7.7 | 58.9 ± 8.8 | 61.7 ± 7.9 |
| Family history of Alzheimer’s disease (%) | 70.7 | 66.9 | 72.4 | 69.5 | 67.6 | 62.0 |
| Employment status (%) | ||||||
| Employed | 64.1 | 50.9 | 62.1 | 54.4 | 67.6 | 45.0 |
| Unemployed | 9.7 | 13.9 | 13.8 | 20.6 | 2.9 | 2.50 |
| Retired | 26.0 | 35.1 | 24.1 | 25.0 | 29.4 | 52.5 |
| Level of education (%) | ||||||
| Primary education or lower | 17.4 | 31.2 * | 15.5 | 33.3 * | 20.6 | 27.5 |
| Secondary education | 10.9 | 20.9 | 12.1 | 14.5 | 8.8 | 30.0 * |
| University education | 71.7 | 48.6 * | 72.4 | 52.2 * | 70.6 | 42.5 * |
| Drug intake (%) | ||||||
| Antihypertensives | 16.3 | 14.7 | 13.8 | 14.5 | 20.6 | 15.0 |
| Antidepressants | 3.3 | 8.3 | 3.4 | 7.2 | 2.9 | 10.0 |
| Antidiabetics | 3.2 | 3.7 | 5.1 | 2.9 | 0.0 | 5.0 |
| Anthropometric data (X ± SD) | ||||||
| Weight (kg) S | 70.5 ± 13.5 | 70.7 ± 14.7 | 64.1 ± 10.2 | 64.3 ± 11.1 | 81.4 ± 11.5 | 81.8 ± 13.7 |
| Height (cm) S | 164.9 ± 8.8 | 163.1 ± 9.0 | 160.5 ± 6.7 | 158.0 ± 5.9 | 172.6 ± 6.2 | 171.9 ± 6.1 |
| BMI (kg/m2) S | 25.8 ± 4.2 | 26.5 ± 4.4 | 24.9 ± 4.5 | 25.8 ± 4.3 | 27.3 ± 3.4 | 27.6 ± 4.2 |
| Waist circumference (cm) S | 86.2 ± 12.7 | 87.8 ± 13.1 | 80.2 ± 10.6 | 82.2 ± 10.8 | 96.4 ± 8.8 | 97.5 ± 10.8 |
| Hip circumference (cm) | 101.12 ±6.8 | 100.8 ± 8.3 | 100.54 ± 7.6 | 100.4 ± 9.0 | 102.1 ± 4.9 | 101.6 ± 7.0 |
| Calf circumference (cm) S | 36.7 ± 2.7 | 36.5 ± 3.3 | 35.8 ± 2.6 | 35.4 ± 2.8 | 38.3 ± 2.2 | 38.3 ± 3.3 |
| Physical activity (%) | ||||||
| Moderate intensity | ||||||
| <150 min/week | 36.8 | 30.0 | 35.2 | 30.2 | 39.4 | 29.7 |
| 150–300 min/week | 40.2 | 37.0 | 44.4 | 42.9 | 33.3 | 27.0 |
| >300 min/week | 22.9 | 33.0 | 20.4 | 26.9 | 27.3 | 43.2 |
| Vigorous intensity | ||||||
| <75 min/week | 97.7 | 99.0 | 98.1 | 98.4 | 96.9 | 100.0 |
| 75–150 min/week | 2.3 | 0.0 | 1.8 | 0.0 | 3.0 | 0.0 |
| >300 min/week | 0.0 | 1.0 | 0.0 | 1.6 | 0.0 | 0.0 |
| APOE genotype (%) | ||||||
| APOE ε4− | 64.1 | 76.1 | 62.1 | 71.0 | 67.6 | 85.0 |
| APOE ε4+ | 35.9 | 23.8 | 37.9 | 28.9 | 32;3 | 15.0 |
| Neuropsychological tests (X ± SD) | ||||||
| GDS (score) | 1.2 ± 1.8 | 1.3 ± 1.7 | 1.2 ± 1.5 | 1.2 ± 1.5 | 1.3 ± 2.1 | 1.4 ± 1.9 |
| MMSE (score) | 29.0 ± 1.3 | 28.8 ± 1.2 | 28.9 ± 1.5 | 28.8 ± 1.2 | 29.1 ± 1.1 | 28.9 ± 1.3 |
| MoCA (score) M | 28.5 ± 1.1 | 23.9 ± 2.1 * | 28.6 ± 1.2 | 23.9 ± 2.2 * | 28.3 ± 1.1 | 23.8 ± 1.9 * |
| Total | Women | Men | ||||
|---|---|---|---|---|---|---|
| Non-CI | CI | Non-CI | CI | Non-CI | CI | |
| n | 92 | 109 | 58 | 69 | 34 | 40 |
| Intake | ||||||
| Energy (kcal/day) S | 2089 ± 449 | 2067 ± 539 | 1999 ± 423 | 1928 ± 465 | 2243 ± 457 | 2308 ± 577 |
| Iron (mg/day) S | 15.5 ± 3.3 | 15.39 ± 6.22 | 15.1 ± 3.0 | 14.5 ± 2.8 | 16.3 ± 3.6 | 16.9 ± 9.4 |
| Magnesium (mg/day) | 332.3 ± 65.5 | 334.8 ± 88.7 | 340.0 ± 66.1 | 333.0 ± 73.6 | 319.22 ± 63.3 | 337.93 ± 111.1 |
| Copper (µg/day) | 2476.1 ± 765.8 | 2393.0 ± 681.3 | 2493.9 ± 608.8 | 2341.2 ± 521.2 | 2445.6± 987.7 | 2481.5 ± 893.9 |
| Zinc (mg/day) | 10.6 ± 3.1 | 10.6 ± 3.4 | 10.2 ± 2.1 | 10.6 ± 3.4 | 11.3 ± 4.3 | 10.7 ± 3.5 |
| Selenium (µg/day) | 112.8 ± 39.0 | 109.3 ± 32.7 | 110.0 ± 32.8 | 108.1 ± 26.9 | 117.7 ± 48.0 | 111.4 ± 41.1 |
| Manganese (mg/day) | 2.7 ± 1.8 | 2.7 ± 2.0 | 2.9 ± 1.7 | 2.6 ± 1.8 | 2.5 ± 1.9 | 2.89 ± 2.4 |
| Contribution | ||||||
| Energy (% EAR) S | 99.9 ± 21.3 | 99.4 ± 23.8 | 103.3 ± 22.1 | 100.9 ± 23.3 | 94.0 ± 18.5 | 96.7 ± 24.8 |
| Iron (% EAR) | 287.01 ± 72.9 | 277.1 ± 120.6 * | 285.9 ± 72.8 | 261.5 ± 74.7 * | 289.0 ± 74.0 | 303.9 ± 171.4 |
| Magnesium (% EAR) S | 114.4 ± 31.4 | 113.3 ± 35.4 | 124.6 ± 29.9 | 119.1 ± 34.4 | 96.9 ± 25.8 | 103.3 ± 35.2 |
| Copper (% EAR) | 255.1 ± 85.1 | 265.9 ± 75.7 | 277.1 ± 67.6 | 260.2 ± 57.9 | 271.7 ± 109.7 | 275.7 ± 99.3 |
| Zinc (% EAR) S | 132.01 ± 41.8 | 131.5 ± 53.3 | 138.0 ± 37.7 | 140.1 ± 56.5 | 121.8 ± 46.7 | 116.7 ± 44.1 |
| Selenium (% EAR) S | 252.5 ± 95.8 | 242.6 ± 87.3 | 237.56 ± 77.73 | 226.5 ± 73.6 | 277.9 ± 117.4 | 270.3 ± 101.9 |
| Manganese (% AI) | 199.0 ± 185.2 | 153.6 ± 69.8 * | 216.4 ± 196.1 | 152.7 ± 63.2 * | 169.4 ± 163.6 | 155.3 ± 81.1 |
| Total | Women | Men | |||||||
| T1 | T2 | T3 | T1 | T2 | T3 | T1 | T2 | T3 | |
| Iron (median mg/day) | 12.5 | 14.7 | 18.0 | 12.4 | 14.5 | 17.5 | 12.4 | 15.7 | 20.0 |
| MoCA (score) I | 25.6 ± 3.1 | 25.7 ± 2.7 | 26.6 ± 2.5 | 25.8 ± 3.1 | 25.1 ± 2.8 | 27.1 ± 2.7 b | 25.2 ± 3.2 | 26.5 ± 2.4 | 25.8 ± 2.4 |
| Magnesium (median mg/day) | 268.7 | 321.7 | 395.8 | 276.6 | 325.3 | 400.0 | 256.58 | 314.9 | 318.8 |
| MoCA (score) | 25.3 ± 3.3 | 26.5 ± 2.5 a | 26.2 ± 2.5 | 25.1 ± 3.3 | 26.9 ± 2.5 a | 26.2 ± 2.6 | 25.7 ± 3.3 | 25.8 ± 2.4 | 26.1 ± 2.4 |
| Copper (median µg/day) | 1950.1 | 2270.9 | 2790.8 | 1980.7 | 2295.9 | 2795.0 | 1880.2 | 2250.4 | 2780.5 |
| MoCA (score) T | 24.9 ± 3.2 | 26.5 ± 2.6 a | 26.6 ± 2.4 a | 24.8 ± 3.3 | 26.4 ± 2.6 a | 26.9 ± 2.4 a | 25.1 ± 3.1 | 26.5 ± 2.7 | 25.6 ± 2.1 |
| Zinc (median mg/day) ‡ | 8.5 | 10.2 | 12.2 | 8.6 | 10.1 | 11.74 | 8.4 | 10.3 | 12.8 |
| MoCA (score) | 25.6 ± 3.1 | 26.0 ± 2.8 | 26.3 ± 2.7 | 25.9 ± 3.2 | 26.0 ± 2.6 | 26.3 ± 2.9 | 25.2 ± 2.8 | 26.0 ± 3.1 | 26.4 ± 2.2 |
| Selenium (median µg/day) | 80.7 | 108.9 | 135.1 | 82.0 | 109.8 | 129.3 | 75.1 | 107.3 | 152.2 |
| MoCA (score) | 25.9 ± 3.1 | 26.2 ± 2.7 | 25.9 ± 2.8 | 25.93 ± 3.32 | 26.55 ± 2.62 | 25.74 ± 2.79 | 25.80 ± 2.68 | 25.64 ± 2.78 | 26.21 ± 2.86 |
| Manganese (median mg/day) ‡ | 0.9 | 2.5 | 4.3 | 1.0 | 2.5 | 4.2 | 0.6 | 2.4 | 4.6 |
| MoCA (score) T | 25.1 ± 3.3 | 26.7 ± 2.3 a | 26.2 ± 2.7 | 25.0 ± 3.3 | 26.5 ± 2.6 a | 26.7 ± 2.6 a | 25.3 ± 3.3 | 26.9 ± 1.9 | 25.5 ± 2.6 |
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Iron | ||||||
| Tertile 1 | 1 | 1 | 1 | |||
| Tertile 2 | 1.606 (0.66–3.92) | 0.298 | 1.514 (0.61–3.74) | 0.368 | 2.437 (0.79–7.50) | 0.120 |
| Tertile 3 | 0.400 (0.17–0.96) | 0.040 | 0.334 (0.13–0.85) | 0.021 | 0.326 (0.11–0.94) | 0.037 |
| Magnesium | ||||||
| Tertile 1 | 1 | 1 | 1 | |||
| Tertile 2 | 0.594 (0.25–1.41) | 0.236 | 0.606 (0.25–1.45) | 0.260 | 0.570 (0.21–1.56) | 0.549 |
| Tertile 3 | 0.791 (0.33–1.87) | 0.595 | 0.739 (0.30–1.82) | 0.511 | 0.767 (0.26–2.22) | 0.625 |
| Copper | ||||||
| Tertile 1 | 1 | 1 | 1 | |||
| Tertile 2 | 0.711 (0.30–1.68) | 0.436 | 0.711 (0.30–1.69) | 0.439 | 0.580 (0.21–1.60) | 0.293 |
| Tertile 3 | 0.485 (0.20–1.17) | 0.106 | 0.499 (0.21–1.21) | 0.124 | 0.569 (0.20–1.59) | 0.282 |
| Zinc | ||||||
| Tertile 1 | 1 | 1 | 1 | |||
| Tertile 2 | 0.720 (0.31–1.69) | 0.452 | 0.688 (0.29–1.64) | 0.399 | 0.619 (0.22–1.79) | 0.375 |
| Tertile 3 | 0.872 (0.37–2.06) | 0.754 | 0.861 (0.36–2.05) | 0.736 | 0.754 (0.28–2.05) | 0.580 |
| Selenium | ||||||
| Tertile 1 | 1 | 1 | 1 | |||
| Tertile 2 | 0.655 (0.28–1.54) | 0.332 | 0.596 (0.24–1.45) | 0.255 | 0.531 (0.19–1.53) | 0.240 |
| Tertile 3 | 0.960 (0.41–2.27) | 0.926 | 0.917 (0.38–2.19) | 0.845 | 0.832 (0.30–2.29) | 0.722 |
| Manganese | ||||||
| Tertile 1 | 1 | 1 | 1 | |||
| Tertile 2 | 0.439 (0.18–1.06) | 0.066 | 0.450 (0.19–1.09) | 0.077 | 0.477 (0.17–1.32) | 0.156 |
| Tertile 3 | 0.439 (0.18–1.06) | 0.066 | 0.415 (0.17–1.02) | 0.057 | 0.334 (0.12–0.93) | 0.037 |
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Iron | ||||||
| Tertile 1 | 1 | 1 | 1 | |||
| Tertile 2 | 0.851 (0.28–2.59) | 0.777 | 0.966 (0.31–3.03) | 0.952 | 1.075 (0.27–4.36) | 0.919 |
| Tertile 3 | 0.929 (0.30–2.86) | 0.897 | 0.917 (0.29–2.89) | 0.883 | 0.929 (0.22–3.90) | 0.920 |
| Magnesium | ||||||
| Tertile 1 | 1 | 1 | 1 | |||
| Tertile 2 | 1.385 (0.45–4.25) | 0.569 | 1.333 (0.41–4.30) | 0.630 | 1.549 (0.38–6.21) | 0.537 |
| Tertile 3 | 0.923 (0.30–2.83) | 0.889 | 0.982 (0.31–3.14) | 0.975 | 1.189 (0.28–4.92) | 0.811 |
| Copper | ||||||
| Tertile 1 | 1 | 1 | 1 | |||
| Tertile 2 | 0.413 (0.13–1.27) | 0.124 | 0.338 (0.10–1.14) | 0.080 | 0.261 (0.06–1.13) | 0.070 |
| Tertile 3 | 0.731 (0.23–2.33) | 0.597 | 0.846 (0.25–2.84) | 0.786 | 0.654 (0.14–2.91) | 0.577 |
| Zinc | ||||||
| Tertile 1 | 1 | 1 | 1 | |||
| Tertile 2 | 0.609 (0.20–1.89) | 0.391 | 0.593 (0.19–1.87) | 0.373 | 0.351 (0.08–1.49) | 0.157 |
| Tertile 3 | 0.476 (0.15–1.50) | 0.204 | 0.462 (0.14–1.50) | 0.199 | 0.496 (0.13–1.93) | 0.311 |
| Selenium | ||||||
| Tertile 1 | 1 | 1 | 1 | |||
| Tertile 2 | 1.385 (0.45–4.25) | 0.569 | 1.634 (0.51–5.23) | 0.409 | 1.195 (0.28–5.14) | 0.811 |
| Tertile 3 | 0.923 (0.30–2.83) | 0.889 | 0.946 (0.30–2.98) | 0.924 | 0.394 (0.09–1.68) | 0.208 |
| Manganese | ||||||
| Tertile 1 | 1 | 1 | 1 | |||
| Tertile 2 | 0.617 (0.20–1.89) | 0.397 | 0.656 (0.21–2.10) | 0.478 | 0.448 (0.10–1.94) | 0.283 |
| Tertile 3 | 1.310 (0.42–4.11) | 0.644 | 1.310 (0.40–4.33) | 0.658 | 1.615 (0.35–7.29) | 0.533 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorenzo-Mora, A.M.; López-Sobaler, A.M.; Bermejo, L.M.; González-Rodríguez, L.G.; Cuadrado-Soto, E.; Peral-Suárez, Á.; Salas-González, M.D.; Delgado-Losada, M.L.; Rodríguez-Rojo, I.C.; Barabash, A.; et al. Association between Mineral Intake and Cognition Evaluated by Montreal Cognitive Assessment (MoCA): A Cross-Sectional Study. Nutrients 2023, 15, 4505. https://doi.org/10.3390/nu15214505
Lorenzo-Mora AM, López-Sobaler AM, Bermejo LM, González-Rodríguez LG, Cuadrado-Soto E, Peral-Suárez Á, Salas-González MD, Delgado-Losada ML, Rodríguez-Rojo IC, Barabash A, et al. Association between Mineral Intake and Cognition Evaluated by Montreal Cognitive Assessment (MoCA): A Cross-Sectional Study. Nutrients. 2023; 15(21):4505. https://doi.org/10.3390/nu15214505
Chicago/Turabian StyleLorenzo-Mora, Ana M., Ana M. López-Sobaler, Laura M. Bermejo, Liliana G. González-Rodríguez, Esther Cuadrado-Soto, África Peral-Suárez, María Dolores Salas-González, María Luisa Delgado-Losada, Inmaculada C. Rodríguez-Rojo, Ana Barabash, and et al. 2023. "Association between Mineral Intake and Cognition Evaluated by Montreal Cognitive Assessment (MoCA): A Cross-Sectional Study" Nutrients 15, no. 21: 4505. https://doi.org/10.3390/nu15214505
APA StyleLorenzo-Mora, A. M., López-Sobaler, A. M., Bermejo, L. M., González-Rodríguez, L. G., Cuadrado-Soto, E., Peral-Suárez, Á., Salas-González, M. D., Delgado-Losada, M. L., Rodríguez-Rojo, I. C., Barabash, A., Maestú-Unturbe, F., & Aparicio, A. (2023). Association between Mineral Intake and Cognition Evaluated by Montreal Cognitive Assessment (MoCA): A Cross-Sectional Study. Nutrients, 15(21), 4505. https://doi.org/10.3390/nu15214505