
Relationship between Hydration Status and Muscle Catabolism in the Aged Population: A Cross-Sectional Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Study Sample
3.2. Hydration and Catabolic Indicators
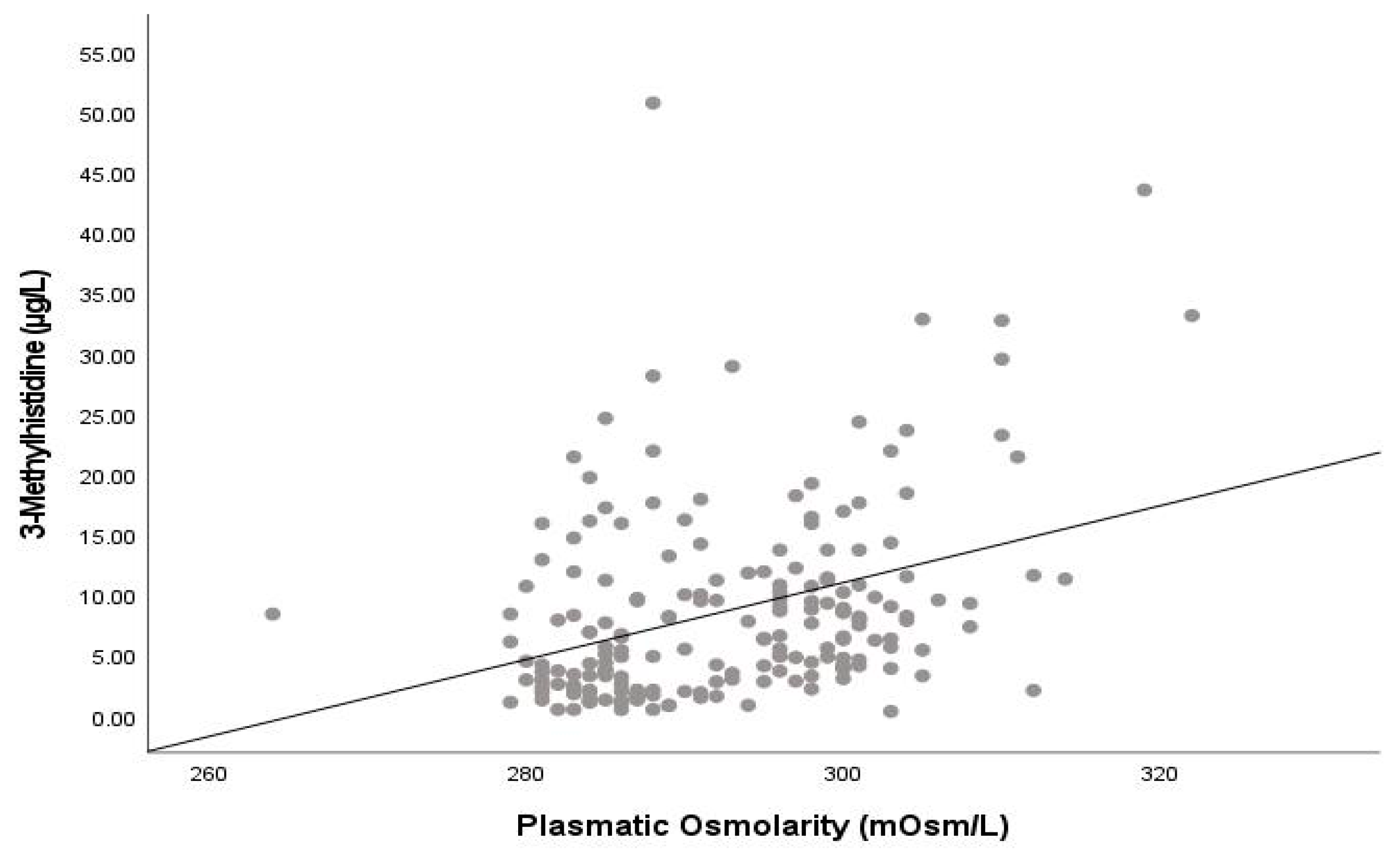
3.3. Relationship between Hydration Indicators and Muscle Catabolism
3.4. Relationship of Hydration and Water Content Indicators with MM and Sarcopenia
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Cesari, M.; Landi, F.; Vellas, B.; Bernabei, R.; Marzetti, E. Sarcopenia and physical frailty: Two sides of the same coin. Front. Aging Neurosci. 2014, 28, 192. [Google Scholar] [CrossRef]
- Yeung, S.S.Y.; Reijnierse, E.M.; Pham, V.K.; Trappenburg, M.C.; Lim, W.K.; Meskers, C.G.M.; Maier, A.B. Sarcopenia and its association with falls and fractures in older adults: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2019, 10, 485–500. [Google Scholar] [CrossRef] [PubMed]
- Hirani, V.; Blyth, F.; Naganathan, V.; Le Couteur, D.G.; Seibel, M.J.; Waite, L.M.; Handelsman, D.J.; Cumming, R.G. Sarcopenia Is Associated with Incident Disability, Institutionalization, and Mortality in Community-Dwelling Older Men: The Concord Health and Ageing in Men Project. J. Am. Med. Dir. Assoc. 2015, 16, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Hughes, V.A.; Frontera, W.R.; Roubenoff, R.; Evans, W.J.; Fiatarone-Singh, M.A. Longitudinal changes in body composition in older men and women: Role of body weight change and physical activity. Am. J. Clin. Nutr. 2002, 76, 473–481. [Google Scholar] [CrossRef]
- Ziaaldini, M.M.; Marzetti, E.; Picca, A.; Murlasits, Z. Biochemical Pathways of Sarcopenia and Their Modulation by Physical Exercise: A Narrative Review. Front. Med. 2017, 4, 167. [Google Scholar] [CrossRef]
- Ferri, E.; Marzetti, E.; Calvani, R.; Picca, A.; Cesari, M.; Arosio, B. Role of age-related mitochondrial dysfunction in sarcopenia. Int. J. Mol. Sci. 2020, 21, 5236. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.; Xie, W.; Fu, X.; Lu, W.; Jin, H.; Lai, J.; Zhang, A.; Yu, Y.; Li, Y.; Xiao, W. Inflammation and sarcopenia: A focus on circulating inflammatory cytokines. Exp. Gerontol. 2021, 154, 111544. [Google Scholar] [CrossRef]
- St-Onge, M.P.; Gallagher, D. Body composition changes with aging: The cause or the result of alterations in metabolic rate and macronutrient oxidation? Nutrition 2010, 26, 152–155. [Google Scholar] [CrossRef]
- Serra-Prat, M.; Lorenzo, I.; Palomera, E.; Yébenes, J.C.; Campins, L.; Cabré, M. Intracellular water content in lean mass is associated with muscle strength, functional capacity and frailty in community-dwelling elderly individuals. A cross-sectional study. Nutrients 2019, 11, 661. [Google Scholar] [CrossRef]
- Hooper, L.; Bunn, D.; Jimoh, F.O.; Fairweather-Tait, S.J. Water-loss dehydration and aging. Mech Ageing Dev. 2014, 136–137, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Maughan, R.J. Hydration, morbidity, and mortality in vulnerable populations. Nutr. Rev. 2012, 70 (Suppl. S2), S152–S155. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.I.; Choi, H.; Song, S.Y.; Park, K.S.; Lee, D.H.; Ha, Y.C. Relationship between water intake and skeletal muscle mass in elderly Koreans: A nationwide population-based study. Nutrition 2018, 53, 38–42. [Google Scholar] [CrossRef]
- Serra-Prat, M.; Lorenzo, I.; Cabré, M.; Martínez, J.; Palomera, E.; Ferrer, P.; Burdoy, E.; Pleguezuelos, E. Relationship between lower-limb bioelectrical impedance indicators of hydration status and muscle function in aged population. A cross-sectional study. J. Fam. Med. 2023, 10, 1327. [Google Scholar]
- Yamada, Y.; Yoshida, T.; Yokoyama, K.; Watanabe, Y.; Miyake, M.; Yamagata, E.; Yamada, M.; Kimura, M.; Study, K.-K. The extracellulat to intracelular water ratio in upper legs is negatively associated with skeletal muscle strength and gait speed in older people. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 293–298. [Google Scholar]
- Taniguchi, M.; Yamada, Y.; Fukumoto, Y.; Sawano, S.; Minami, S.; Ikezoe, T.; Watanabe, Y.; Kimura, M.; Ichihashi, N. Increase in echo intensity and extracellular-to-intracellular water ratio is independently associated with muscle weakness in elderly women. Eur. J. Appl. Physiol. 2017, 117, 2001–2007. [Google Scholar] [CrossRef] [PubMed]
- Hioka, A.; Akazawa, N.; Okawa, N.; Nagahiro, S. Increased total body extracellular-to-intracellular water ratio in community-dwelling elderly women is associated with decreased handgrip strength and gait speed. Nutrition 2021, 86, 111175. [Google Scholar] [CrossRef]
- Serra-Prat, M.; Lorenzo, I.; Palomera, E.; Ramírez, S.; Yébenes, J.C. Total Body Water and Intracellular Water Relationships with Muscle Strength, Frailty and Functional Performance in an Elderly Population. J. Nutr. Health Aging 2019, 23, 96–101. [Google Scholar] [CrossRef]
- Yoshida, T.; Yamada, Y.; Tanaka, F.; Yamagishi, T.; Shibata, S.; Kawakami, Y. Intracellular-to-total water ratio explains the variability of muscle strength dependence on the size of lower leg in the elderly. Exp. Gerontol. 2018, 113, 120–127. [Google Scholar] [CrossRef]
- Neuhäuser, M.; Bässler, K.H. Endogenous 3-methylhistidine excretion in healthy women and men with reference to muscle protein metabolism. Z. Ernährungswiss 1984, 23, 171–180. [Google Scholar] [CrossRef]
- Johnson, P.; Perry, S.V. Biological activity and the 3-methylhistidine content of actin and myosin. Biochem. J. 1970, 119, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Laurens, C.; Grundler, F.; Damiot, A.; Chery, I.; Le Maho, A.; Zahariev, A.; Le Maho, Y.; Bergouignan, A.; Gauquelin-Koch, G.; Simon, C.; et al. Is muscle and protein loss relevant in long-term fasting in healthy men? A prospective trial on physiological adaptations. J. Cachexia Sarcopenia Muscle 2021, 12, 1690–1703. [Google Scholar] [CrossRef] [PubMed]
- Bres, E.; Pagan, C.; Bouchara, A.; Pastural, M.; Granjon, S.; Laville, M.; Fouque, D.; O Soulage, C.; Koppe, L. 3-methylhistidine and clinical outcomes in maintenance haemodialysis patients. Nephrol. Dial. Transpl. 2022, 37, 1951–1961. [Google Scholar] [CrossRef] [PubMed]
- McKeran, R.O.; Halliday, D.; Purkiss, P.; Royston, P. 3-Methylhistidine excretion as an index of myofibrillarprotein catabolism in neuromuscular disease. J. Neurol. Neurosurg. Psychiatry 1979, 42, 536–541. [Google Scholar] [CrossRef] [PubMed]
- Kochlik, B.; Stuetz, W.; Pérès, K.; Féart, C.; Tegner, J.; Rodriguez-Mañas, L.; Grune, T.; Weber, D. Associations of Plasma 3-Methylhistidine with Frailty Status in French Cohorts of the FRAILOMIC Initiative. J. Clin. Med. 2019, 8, 1010. [Google Scholar] [CrossRef] [PubMed]
- Parkinson, E.; Hooper, L.; Fynn, J.; Wilsher, S.H.; Oladosu, T.; Poland, F.; Roberts, S.; Van Hout, E.; Bunn, D. Low-intake dehydration prevalence in non-hospitalised older adults: Systematic review and meta-analysis. Clin. Nutr. 2023, 42, 1510–1520. [Google Scholar] [CrossRef]
- El-Sharkawy, A.M.; Watson, P.; Neal, K.R.; Ljungqvist, O.; Maughan, R.J.; Sahota, O.; Lobo, D.N. Hydration and outcome in older patients admitted to hospital (The HOOP prospective cohort study). Age Ageing 2015, 44, 943–947. [Google Scholar] [CrossRef]
- Mentes, J. Oral hydration in older adults: Greater awareness is needed in preventing, recognizing, and treating dehydration. Am. J. Nurs. 2006, 106, 40–49. [Google Scholar] [CrossRef]
- Cowen, L.E.; Hodak, S.P.; Verbalis, J.G. Age-associated abnormalities of water homeostasis. Endocrinol. Metab. Clin. N. Am. 2013, 42, 349–370. [Google Scholar] [CrossRef]
- Fernández-Elías, V.E.; Ortega, J.F.; Nelson, R.K.; Mora-Rodriguez, R. Relationship between muscle water and glycogen recovery after prolonged exercise in the heat in humans. Eur. J. Appl. Physiol. 2015, 115, 1919–1926. [Google Scholar] [CrossRef]
- Lorenzo, I.; Serra-Prat, M.; Yébenes, J.C. The role of water homeostasis in the muscle function and frailty: A review. Nutrients 2019, 11, 1857. [Google Scholar] [CrossRef] [PubMed]
- Paik, I.-Y.; Jeong, M.-H.; Jin, H.-E.; Kim, Y.-I.; Suh, A.-R.; Cho, S.-Y.; Roh, H.-T.; Jin, C.-H.; Suh, S.-H. Fluid replacement following dehydration reduces oxidative stress during recovery. Biochem. Biophys. Res. Commun. 2009, 383, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Hooper, L.; Abdelhamid, A.; Attreed, N.J.; Campbell, W.W.; Channell, A.M.; Chassagne, P.; Culp, K.R.; Fletcher, S.J.; Fortes, M.B.; Fuller, N.; et al. Clinical symptoms, signs and tests for identification of impending and current water-loss dehydration in older people. Cochrane Database Syst. Rev. 2015, 2015, CD009647. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Sample N = 190 | Women N = 98 | Men N = 92 | p | <80 Years N = 142 | ≥80 Years N = 48 | p | |
|---|---|---|---|---|---|---|---|
| Hydration indicators | |||||||
| Plasma osmolarity (mOsm/L) | 292.9 (9.1) | 292.0 (9.0) | 293.8 (9.0) | 0.197 | 291.8 (8.6) | 296.0 (9.7) | 0.002 |
| Osmolarity (mOsm/L): | |||||||
| ≤290 | 86 (45.3%) | 49 (50.0%) | 37 (40.2%) | 0.323 | 74 (52.1%) | 12 (25.0%) | 0.002 |
| 291–295 | 22 (11.6%) | 9 (9.2%) | 13 (14.1%) | 17 (12.0%) | 5 (10.4%) | ||
| >295 | 82 (43.2%) | 40 (40.8%) | 42 (45.7%) | 51 (35.9%) | 31 (64.6%) | ||
| BIA water content indicators | |||||||
| %TBW | 46.4 (5.5) | 43.9 (5.4) | 49.0 (4.4) | <0.001 | 46.9 (5.6) | 44.6 (5.0) | 0.016 |
| %ICW | 61.0 (0.8) | 60.8 (0.8) | 61.2 (0.7) | 0.003 | 61.1 (0.7) | 60.6 (0.9) | 0.002 |
| TBW/FFM | 73.6 (0.3) | 73.5 (0.3) | 73.8 (0.3) | <0.001 | 73.6 (0.3) | 73.6 (0.3) | 0.726 |
| ICW/FFM | 44.9 (0.6) | 44.7 (0.6) | 45.1 (0.5) | <0.001 | 45.2 (0.52) | 44.6 (0.7) | 0.003 |
| Catabolic indicators | |||||||
| 3MH (µmol/L) | 8.7 (8.0) | 8.2 (8.2) | 9.3 (7.8) | 0.165 | 8.4 (8.2) | 9.7 (7.6) | 0.069 |
| 3MH/MM (µmol/L/kg) | 0.36 (0.4) | 0.39 (0.4) | 0.34 (0.3) | 0.464 | 0.34 (0.3) | 0.44 (0.4) | 0.018 |
| 3MH/Cr (µmol/L/g) | 10.0 (9.1) | 11.0 (10.7) | 8.9 (6.9) | 0.376 | 9.8 (9.6) | 10.5 (7.3) | 0.148 |
| Plasma Osmolarity (mOsm/L) | |||||
|---|---|---|---|---|---|
| ≤290 Hydrated | 290–295 Dehydration Risk | 295–300 Incipient Dehydration | >300 Severe Dehydration | p | |
| N (%) | 86 (45.3%) | 22 (11.6%) | 43 (22.6%) | 39 (20.5%) | --- |
| 3MH | 6.9 (7.8) | 7.8 (6.6) | 8.5 (4.4) | 13.6 (10.2) | <0.001 |
| 3MH/MM | 0.27 (0.3) | 0.33 (0.3) | 0.37 (0.2) | 0.58 (0.5) | <0.001 |
| 3MH/Cr | 9.0 (10.9) | 9.1 (7.6) | 10.1 (5.5) | 12.7 (8.3) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serra-Prat, M.; Lorenzo, I.; Martínez, J.; Palomera, E.; Pleguezuelos, E.; Ferrer, P. Relationship between Hydration Status and Muscle Catabolism in the Aged Population: A Cross-Sectional Study. Nutrients 2023, 15, 4718. https://doi.org/10.3390/nu15224718
Serra-Prat M, Lorenzo I, Martínez J, Palomera E, Pleguezuelos E, Ferrer P. Relationship between Hydration Status and Muscle Catabolism in the Aged Population: A Cross-Sectional Study. Nutrients. 2023; 15(22):4718. https://doi.org/10.3390/nu15224718
Chicago/Turabian StyleSerra-Prat, Mateu, Isabel Lorenzo, Jessica Martínez, Elisabet Palomera, Eulogio Pleguezuelos, and Pau Ferrer. 2023. "Relationship between Hydration Status and Muscle Catabolism in the Aged Population: A Cross-Sectional Study" Nutrients 15, no. 22: 4718. https://doi.org/10.3390/nu15224718
APA StyleSerra-Prat, M., Lorenzo, I., Martínez, J., Palomera, E., Pleguezuelos, E., & Ferrer, P. (2023). Relationship between Hydration Status and Muscle Catabolism in the Aged Population: A Cross-Sectional Study. Nutrients, 15(22), 4718. https://doi.org/10.3390/nu15224718