

Intermittent Fasting in Breast Cancer: A Systematic Review and Critical Update of Available Studies



Abstract
:1. Introduction
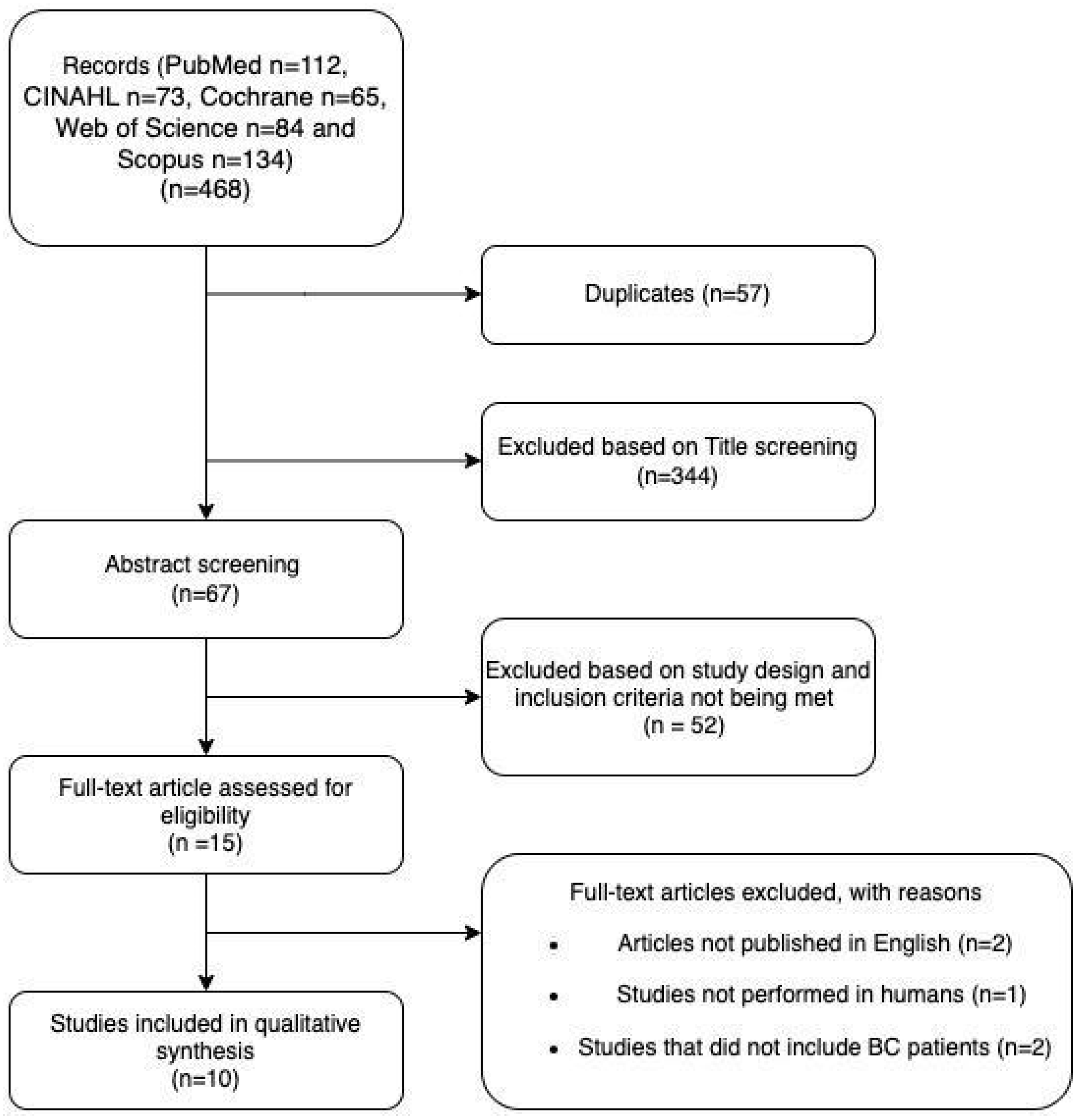
2. Methods
2.1. Data Sources and Search Strategy
2.2. Eligibility Criteria
2.3. Quality Assessment
2.4. Data Extraction
3. Results
3.1. Health Outcomes
3.1.1. Quality of Life: Chemotherapy-Induced Side Effects
3.1.2. Chemotherapy-Induced Toxicity
3.1.3. Chemotherapeutic or Radiological Response/Tumor Recurrence
3.1.4. Endocrine-Related Outcomes
3.1.5. Adverse Effects of IF
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Canadian Cancer Statistics Advisory Committee. Canadian Cancer Society. 2021. Available online: https://cancer.ca/en/cancer-information/cancer-types/breast/statistics (accessed on 14 February 2022).
- Dossus, L.; Jimenez-Corona, A.; Romieu, I.; Boutron-Ruault, M.C.; Boutten, A.; Dupré, T.; Fagherazzi, G.; Clavel-Chapelon, F.; Mesrine, S. C-reactive protein and postmenopausal breast cancer risk: Results from the E3N cohort study. Cancer Causes Control 2014, 25, 533–539. [Google Scholar] [CrossRef]
- Longo, V.D.; Fontana, L. Calorie restriction and cancer prevention: Metabolic and molecular mechanisms. Trends Pharmacol. Sci. 2010, 31, 89–98. [Google Scholar] [CrossRef] [Green Version]
- Rynders, C.A.; Thomas, E.A.; Zaman, A.; Pan, Z.; Catenacci, V.A.; Melanson, E.L. Effectiveness of Intermittent Fasting and Time-Restricted Feeding Compared to Continuous Energy Restriction for Weight Loss. Nutrients 2019, 11, 2442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donaldson, M.S. Nutrition and cancer: A review of the evidence for an anti-cancer diet. Nutr. J. 2004, 3, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donnelly, L.S.; Shaw, R.L.; Pegington, M.; Armitage, C.J.; Evans, D.G.; Howell, A.; Harvie, M.N. ‘For me it’s about not feeling like I’m on a diet’: A thematic analysis of women’s experiences of an intermittent energy restricted diet to reduce breast cancer risk. J. Hum. Nutr. Diet 2018, 31, 773–780. [Google Scholar] [CrossRef]
- Malinowski, B.; Zalewska, K.; Węsierska, A.; Sokołowska, M.M.; Socha, M.; Liczner, G.; Pawlak-Osińska, K.; Wiciński, M. Intermittent Fasting in Cardiovascular Disorders-An Overview. Nutrients 2019, 11, 673. [Google Scholar] [CrossRef] [Green Version]
- Clifton, K.K.; Ma, C.X.; Fontana, L.; Peterson, L.L. Intermittent fasting in the prevention and treatment of cancer. CA Cancer J. Clin. 2021, 71, 527–546. [Google Scholar] [CrossRef] [PubMed]
- Lv, M.; Zhu, X.; Wang, H.; Wang, F.; Guan, W. Roles of caloric restriction, ketogenic diet and intermittent fasting during initiation, progression and metastasis of cancer in animal models: A systematic review and meta-analysis. PLoS ONE 2014, 9, e115147. [Google Scholar] [CrossRef] [PubMed]
- Levine, M.E.; Suarez, J.A.; Brandhorst, S.; Balasubramanian, P.; Cheng, C.-W.; Madia, F.; Fontana, L.; Mirisola, M.G.; Guevara-Aguirre, J.; Wan, J.; et al. Low protein intake is associated with a major reduction in IGF-1, cancer, and overall mortality in the 65 and younger but not older population. Cell Metab. 2014, 19, 407–417. [Google Scholar] [CrossRef] [Green Version]
- Kim, E.J.; Choi, M.-R.; Park, H.; Kim, M.; Hong, J.E.; Lee, J.-Y.; Chun, H.S.; Lee, K.W.; Park, J.H.Y. Dietary fat increases solid tumor growth and metastasis of 4T1 murine mammary carcinoma cells and mortality in obesity resistant BALB/c mice. Breast Cancer Res. 2011, 13, R78. [Google Scholar] [CrossRef]
- Lamming, D.W.; Cummings, N.E.; Rastelli, A.L.; Gao, F.; Cava, E.; Bertozzi, B.; Spelta, F.; Pili, R.; Fontana, L. Restriction of dietary protein decreases mTORC1 in tumors and somatic tissues of a tumor-bearing mouse xenograft model. Oncotarget 2015, 6, 31233–31240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundaram, S.; Yan, L. Time-restricted feeding mitigates high-fat dietenhanced mammary tumorigenesis in MMTV-PyMT mice. Nutr. Res. 2018, 59, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Safdie, F.M.; Raffaghello, L.; Wei, M.; Madia, F.; Parrella, E.; Hwang, D.; Cohen, P.; Bianchi, G.; Longo, V.D. Reduced levels of IGF-I mediate differential protection of normal and cancer cells in response to fasting and improve chemotherapeutic index. Cancer Res. 2010, 70, 1564–1572. [Google Scholar] [CrossRef] [Green Version]
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; et al. Mixed Methods Appraisal Tool (MMAT), version 2018; Registration of Copyright (#1148552); Canadian Intellectual Property Office: Gatineau, QC, Canada, 2018. [Google Scholar]
- Cella, D. The Functional Assessment of Cancer Therapy-Anemia (FACT-An) Scale: A new tool for the assessment of outcomes in cancer anemia and fatigue. Semin. Hematol. 1997, 34, 13–19. [Google Scholar] [PubMed]
- Kleckner, A.; Reschke, J.E.; Altman, B.J.; Belcher, E.; Dunne, R.F.; Fleming, F.J.; Gilmore, N.; Jensen-Battaglia, M.; Kleckner, I.; Lin, P.; et al. A 10-hour time-restricted eating intervention to address cancer-related fatigue among cancer survivors. J. Clin. Oncol. 2021, 39, 12109. [Google Scholar] [CrossRef]
- Mendoza, T.R.; Wang, X.S.; Cleeland, C.S.; Morrissey, M.; Johnson, B.A.; Wendt, J.K.; Huber, S.L. The rapid assessment of fatigue severity in cancer patients: Use of the Brief Fatigue Inventory. Cancer 1999, 85, 1186–1196. [Google Scholar] [CrossRef]
- Bauersfeld, S.P.; Kessler, C.S.; Wischnewsky, M.; Jaensch, A.; Steckhan, N.; Stange, R.; Kunz, B.; Brückner, B.; Sehouli, J.; Michalsen, A. The effects of short-term fasting on quality of life and tolerance to chemotherapy in patients with breast and ovarian cancer: A randomised cross-over pilot study. BMC Cancer 2018, 18, 476. [Google Scholar] [CrossRef]
- Badar, T.; Ismail, A.; AlShanqeeti, A. Safety and feasability of Muslim fasting while receiving chemotherapy. IOSR J. Pharm. 2014, 4, 15–20. [Google Scholar] [CrossRef]
- Mas, S.; Le Bonniec, A.; Cousson-Gélie, F. Why do women fast during breast cancer chemotherapy? A qualitative study of the patient experience. Br. J. Health Psychol. 2019, 24, 381–395. [Google Scholar] [CrossRef]
- Safdie, F.M.; Dorff, T.; Quinn, D.; Fontana, L.; Wei, M.; Lee, C.; Cohen, P.; Longo, V.D. Fasting and cancer treatment in humans: A case series report. Aging 2009, 1, 988–1007. [Google Scholar] [CrossRef]
- Marinac, C.R.; Nelson, S.H.; Breen, C.I.; Hartman, S.J.; Natarajan, L.; Pierce, J.P.; Flatt, S.W.; Sears, D.D.; Patterson, R.E. Prolonged Nightly Fasting and Breast Cancer Prognosis. JAMA Oncol. 2016, 2, 1049–1055. [Google Scholar] [CrossRef]
- Mah, L.J.; El-Osta, A.; Karagiannis, T. γH2AX: A sensitive molecular marker of DNA damage and repair. Leukemia 2010, 24, 679–686. [Google Scholar] [CrossRef] [Green Version]
- Zorn, S.; Ehret, J.; Schäuble, R.; Rautenberg, B.; Ihorst, G.; Bertz, H.; Urbain, P.; Raynor, A. Impact of modified short-term fasting and its combination with a fasting supportive diet during chemotherapy on the incidence and severity of chemotherapy-induced toxicities in cancer patients—A controlled cross-over pilot study. BMC Cancer 2020, 20, 578. [Google Scholar] [CrossRef]
- De Groot, S.; Lugtenberg, R.T.; Cohen, D.; Welters, M.J.P.; Ehsan, I.; Vreeswijk, M.P.G.; Smit, V.T.H.B.M.; de Graaf, H.; Heijns, J.B.; Portielje, J.E.A.; et al. Dutch Breast Cancer Research Group (BOOG). Fasting mimicking diet as an adjunct to neoadjuvant chemotherapy for breast cancer in the multicentre randomized phase 2 DIRECT trial. Nat. Commun. 2020, 11, 3083. [Google Scholar] [CrossRef] [PubMed]
- De Groot, S.; Vreeswijk, M.P.; Welters, M.J.; Gravesteijn, G.; Boei, J.J.; Jochems, A.; Houtsma, D.; Putter, H.; van der Hoeven, J.J.; Nortier, J.W.; et al. The effects of short-term fasting on tolerance to (neo) adjuvant chemotherapy in HER2-negative breast cancer patients: A randomized pilot study. BMC Cancer 2015, 15, 652. [Google Scholar] [CrossRef] [Green Version]
- Dorff, T.B.; Groshen, S.; Garcia, A.; Shah, M.; Tsao-Wei, D.; Pham, H.; Cheng, C.W.; Brandhorst, S.; Cohen, P.; Wei, M.; et al. Safety and feasibility of fasting in combination with platinum-based chemotherapy. BMC Cancer 2016, 16, 360. [Google Scholar] [CrossRef] [Green Version]
- Vernieri, C.; Ligorio, F.; Zattarin, E.; Rivoltini, L.; de Braud, F. Fasting-mimicking diet plus chemotherapy in breast cancer treatment. Nat. Commun. 2020, 11, 4274. [Google Scholar] [CrossRef]
- Tiwari, S.; Sapkota, N.; Han, Z. Effect of fasting on cancer: A narrative review of scientific evidence. Cancer Sci. 2022, 113, 3291–3302. [Google Scholar] [CrossRef] [PubMed]
- Christensen, R.A.; Haykowksy, M.J.; Nadler, M.; Prado, C.M.; Small, S.D.; Rickard, J.N.; Pituskin, E.; Paterson, D.I.; Mackey, J.R.; Thompson, R.B.; et al. Rationale and Design of IMPACT-women: A randomized controlled trial of the effect of time-restricted eating, healthy eating, and reduced sedentary behavior on metabolic health during chemotherapy for early-stage breast cancer. Br. J. Nutr. 2022, 1–20, ahead-of-print. [Google Scholar] [CrossRef]


{kind=link}
| Author | Year | Population | Fasting Regimen | Results | Type of Study |
|---|---|---|---|---|---|
| Kleckner et al. [17] | 2021 | 21 (20 breast cancer survivors) | Women followed a 2-week 14: 10 h TRF dietary regimen (this dietary pattern included 14 h of fasting within the same day) with no inclusion of a control group in the study. | Fatigue scores improved in 2 weeks 5.3 ± 8.1 points on the FACIT-F fatigue subscale (p < 0.001, effect size (ES) = 0.55), 30.6 ± 35.9 points for the FACIT-F total score (p < 0.001, ES = 0.50), and 1.0 ± 1.7 points on the BFI (p < 0.001, ES =−0.58). | Clinical trial |
| De Groot et al. [26] | 2020 | 131 (HER-2 negative stage II/III breast cancer) | Fasting mimicking diet 3 days before and during neoadjuvant chemotherapy. |
| Randomized, controlled, observer-blind study |
| Zorn et al. [25] | 2020 | 30 (cancer patients) | 96 h fasting for half of scheduled chemotherapy cycles, followed by a regular diet for the remaining cycles. |
| Controlled cross-over pilot study |
| Mas et al. [21] | 2019 | 16 (breast cancer) | Participants were not instructed according to a specific dietary regimen, but rather, followed nutrition advice from healthcare practitioners. | Patients fasted in order to alleviate chemotherapeutic adverse effects and treatment-induced anxiety. The authors reported that fasting improved nausea and vomiting, as well as appetite, satiation, and fatigue between chemotherapy sessions. | Qualitative study |
| Bauersfeld et al. [19] | 2018 | 34 (breast and ovarian cancer) | Patients were randomly assigned to either a short-term fasting diet followed by a normal caloric diet or a normal caloric diet followed by a short-term fasting diet in the first half of chemotherapy. | Within 8 h after treatment, patients on the fasting diet reported improved quality of life and tiredness. | Randomized cross-over pilot study |
| Dorff et al. [28] | 2016 | 5 (BC female) | Fasting for 24 h, 48 h, or 72 h before chemotherapy. |
| Cohort |
| Marinac et al. [23] | 2015 | 2413 (BC female) | Dietary recalls were utilized to calculate the length of time spent fasting at night. | Fasting for less than 13 h per night is connected with a 36% greater risk of the recurrence of breast cancer when compared to individuals fasting for ≥13 h per night. | Cohort |
| De Groot et al. [27] | 2015 | 13 (HER2-negative, Stages II/III) | Before and after chemotherapy, patients were randomly assigned to either a 24 h fast or a diet that followed appropriate dietary standards. |
| Randomized pilot study |
| Badar et al. [20] | 2014 | 4 (BC patients at Stages IIB/IIIB/IV) | Ramadan-fasting patients previously received chemotherapy (20 min after sunset) and, then, continued their fasting routine (daily from dawn to sunset and ate from sunset to dawn) for the rest of the month. |
| Non-randomized, cross-over, pilot study |
| Safdie et al. [22] | 2009 | 4 (breast cancer) | Fasting before 48–140 h or fasting after 5–56 h of treatment. |
| Case series |
| Clinical Trial | Study Title | Trial Phase | Total Participants | Status | Primary Outcomes | Details |
|---|---|---|---|---|---|---|
| NCT05023967 | Metformin and Nightly Fasting in Women with Early Breast Cancer | 2 | 120 | Not yet recruiting |
| Age: 18 years and older Gender: female Study start: 1 April 2022 Study completion: 30 November 2024 |
| NCT05432856 [31] | A randomized controlled trial of the effect of time restricted eating, healthy eating, and reduced sedentary behavior on metabolic health during chemotherapy for early-stage breast cancer | NA | 130 | Not yet recruiting |
| Age: 18 years and older Gender: female Study start: January 2023 Study completion: December 2024 |
| NCT04560439 | Diabetes Prevention Program (METFIT) in Reducing Insulin Resistance in Stage I-III Breast Cancer Survivors | NA | 25 | Recruiting |
| Age: 18–75 years Gender: female Study start: 15 June 2022 Study completion: 15 June 2023 |
| NCT04691999 | The Effect of Intermittent Fasting on Body Composition in Women With Breast Cancer | NA | 0 | Withdrawn |
| Age: 20–70 years Gender: female Study start: 2 December 2021 Study completion: August 2023 |
| NCT04330339 | Prolonged Nightly Fasting in Breast Cancer Survivors | NA | 40 | Active, not recruiting | Baseline assessment (measurements of weight, height, quality of life, fatigue, mood, levels of physical activity, and blood markers) prior to the intervention and after completion of 12-week intervention. | Age: 18 years and older Gender: female Study start: 24 July 2020 Study completion: 31 August 2021 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anemoulis, M.; Vlastos, A.; Kachtsidis, V.; Karras, S.N. Intermittent Fasting in Breast Cancer: A Systematic Review and Critical Update of Available Studies. Nutrients 2023, 15, 532. https://doi.org/10.3390/nu15030532
Anemoulis M, Vlastos A, Kachtsidis V, Karras SN. Intermittent Fasting in Breast Cancer: A Systematic Review and Critical Update of Available Studies. Nutrients. 2023; 15(3):532. https://doi.org/10.3390/nu15030532
Chicago/Turabian StyleAnemoulis, Marios, Antonios Vlastos, Vasileios Kachtsidis, and Spyridon N. Karras. 2023. "Intermittent Fasting in Breast Cancer: A Systematic Review and Critical Update of Available Studies" Nutrients 15, no. 3: 532. https://doi.org/10.3390/nu15030532