
Effect of Iso-Caloric Substitution of Animal Protein for Other Macro Nutrients on Risk of Overall, Cardiovascular and Cancer Mortality: Prospective Evaluation in EPIC-Heidelberg Cohort and Systematic Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population: The EPIC-Heidelberg Cohort
2.2. Assessment of Habitual Diet
2.3. Prospective Ascertainment of Mortality Endpoints
2.4. Statistical Analyses
2.5. Method for the Systematic Review
3. Results
3.1. Results in EPIC-Heidelberg Cohort
3.1.1. Cohort Characteristics
3.1.2. Model Selection
3.1.3. Association of Animal Protein Intake with Mortality
3.2. Systematic Review Result of Previous Prospective Cohort Studies
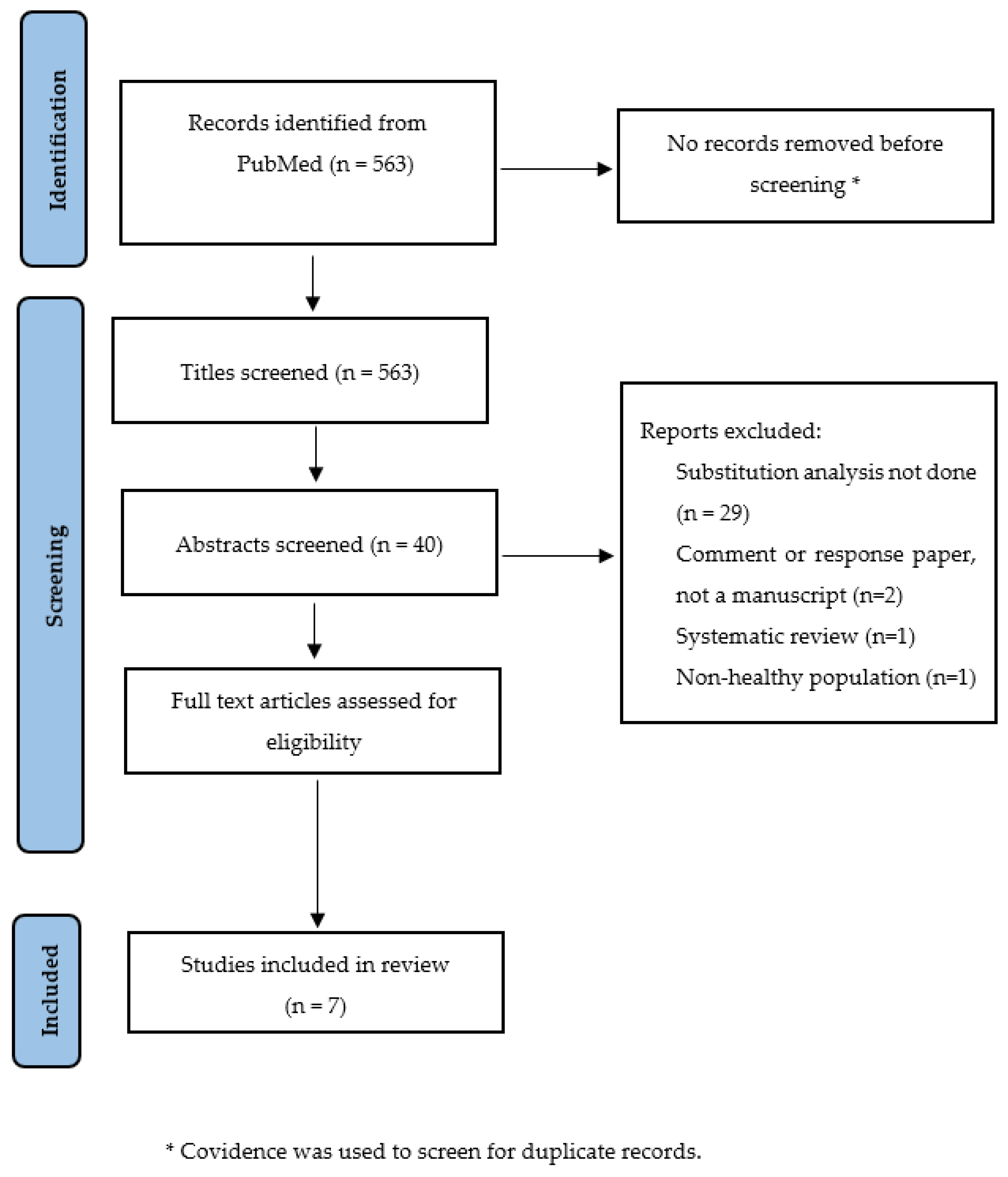
3.2.1. Literature Search and Study Characteristics
3.2.2. Association of Animal Protein Intake with Mortality
4. Discussion
Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Popkin, B.M. The nutrition transition and its health implications in lower-income countries. Public Health Nutr. 1998, 1, 5–21. [Google Scholar] [CrossRef] [PubMed]
- Dehghan, M.; Mente, A.; Zhang, X.; Swaminathan, S.; Li, W.; Mohan, V.; Iqbal, R.; Kumar, R.; Wentzel-Viljoen, E.; Rosengren, A.; et al. Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (pure): A prospective cohort study. Lancet 2017, 390, 2050–2062. [Google Scholar] [CrossRef] [PubMed]
- Grasgruber, P.; Cacek, J.; Hrazdíra, E.; Hřebíčková, S.; Sebera, M. Global correlates of cardiovascular risk: A comparison of 158 countries. Nutrients 2018, 10, 411. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, B.; Doll, R. Environmental factors and cancer incidence and mortality in different countries, with special reference to dietary practices. Int. J. Cancer 1975, 15, 617–631. [Google Scholar] [CrossRef]
- Das, A.; Cumming, R.; Naganathan, V.; Blyth, F.; Couteur, D.; Handelsman, D.J.; Waite, L.M.; Ribeiro, R.; Simpson, S.J.; Hirani, V. Associations between dietary intake of total protein and sources of protein (plant vs. Animal) and risk of all-cause and cause-specific mortality in older australian men: The concord health and ageing in men project. J. Hum. Nutr. Diet 2021, 35, 845–860. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Glisic, M.; Song, M.; Aliahmad, H.A.; Zhang, X.; Moumdjian, A.C.; Gonzalez-Jaramillo, V.; van der Schaft, N.; Bramer, W.M.; Ikram, M.A.; et al. Dietary protein intake and all-cause and cause-specific mortality: Results from the rotterdam study and a meta-analysis of prospective cohort studies. Eur. J. Epidemiol. 2020, 35, 411–429. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, H.; Voutilainen, S.; Koskinen, T.T.; Mursu, J.; Kokko, P.; Ylilauri, M.; Tuomainen, T.P.; Salonen, J.T.; Virtanen, J.K. Dietary proteins and protein sources and risk of death: The kuopio ischaemic heart disease risk factor study. Am. J. Clin. Nutr. 2019, 109, 1462–1471. [Google Scholar] [CrossRef]
- Budhathoki, S.; Sawada, N.; Iwasaki, M.; Yamaji, T.; Goto, A.; Kotemori, A.; Ishihara, J.; Takachi, R.; Charvat, H.; Mizoue, T.; et al. Association of animal and plant protein intake with all-cause and cause-specific mortality in a japanese cohort. JAMA Intern. Med. 2019, 179, 1509–1518. [Google Scholar] [CrossRef]
- Song, M.; Fung, T.T.; Hu, F.B.; Willett, W.C.; Longo, V.D.; Chan, A.T.; Giovannucci, E.L. Association of animal and plant protein intake with all-cause and cause-specific mortality. JAMA Intern. Med. 2016, 176, 1453–1463. [Google Scholar] [CrossRef]
- Huang, J.; Liao, L.M.; Weinstein, S.J.; Sinha, R.; Graubard, B.I.; Albanes, D. Association between plant and animal protein intake and overall and cause-specific mortality. JAMA Intern. Med. 2020, 180, 1173–1184. [Google Scholar]
- Sun, Y.; Liu, B.; Snetselaar, L.G.; Wallace, R.B.; Shadyab, A.H.; Kroenke, C.H.; Haring, B.; Howard, B.V.; Shikany, J.M.; Valdiviezo, C.; et al. Association of major dietary protein sources with all-cause and cause-specific mortality: Prospective cohort study. J. Am. Heart Assoc. 2021, 10, e015553. [Google Scholar] [CrossRef] [PubMed]
- Riboli, E.; Hunt, K.J.; Slimani, N.; Ferrari, P.; Norat, T.; Fahey, M.; Charrondière, U.R.; Hémon, B.; Casagrande, C.; Vignat, J.; et al. European prospective investigation into cancer and nutrition (epic): Study populations and data collection. Public Health Nutr. 2002, 5, 1113–1124. [Google Scholar] [CrossRef] [PubMed]
- Boeing, H.; Korfmann, A.; Bergmann, M.M. Recruitment procedures of epic-germany. European investigation into cancer and nutrition. Ann. Nutr. Metab. 1999, 43, 205–215. [Google Scholar] [CrossRef] [PubMed]
- Boeing, H.; Wahrendorf, J.; Becker, N. Epic-germany—A source for studies into diet and risk of chronic diseases. European investigation into cancer and nutrition. Ann. Nutr. Metab. 1999, 43, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Bohlscheid-Thomas, S.; Hoting, I.; Boeing, H.; Wahrendorf, J. Reproducibility and relative validity of energy and macronutrient intake of a food frequency questionnaire developed for the german part of the epic project. European prospective investigation into cancer and nutrition. Int. J. Epidemiol. 1997, 26, S71–S81. [Google Scholar] [CrossRef] [PubMed]
- Kaaks, R.; Slimani, N.; Riboli, E. Pilot phase studies on the accuracy of dietary intake measurements in the epic project: Overall evaluation of results. European prospective investigation into cancer and nutrition. Int. J. Epidemiol. 1997, 26, S26–S36. [Google Scholar] [CrossRef]
- Bohlscheid-Thomas, S.; Hoting, I.; Boeing, H.; Wahrendorf, J. Reproducibility and relative validity of food group intake in a food frequency questionnaire developed for the german part of the epic project. European prospective investigation into cancer and nutrition. Int. J. Epidemiol. 1997, 26, S59–S70. [Google Scholar] [CrossRef]
- Deharveng, G.; Charrondiere, U.R.; Salimani, N.; Southgate, D.A.; Riboli, E. Comparison of nutrients in the food composition tables available in the nine European countries participating in EPIC. European Prospective Investigation into Cancer and Nutrition. Eur. J. Clin. Nutr. 1999, 53, 60–79. [Google Scholar] [CrossRef]
- Jakobsen, M.U.; O’Reilly, E.J.; Heitmann, B.L.; Pereira, M.A.; Bälter, K.; Fraser, G.E.; Goldbourt, U.; Hallmans, G.; Knekt, P.; Liu, S.; et al. Major types of dietary fat and risk of coronary heart disease: A pooled analysis of 11 cohort studies. Am. J. Clin. Nutr. 2009, 89, 1425–1432. [Google Scholar] [CrossRef]
- Linseisen, J.; Welch, A.A.; Ocké, M.; Amiano, P.; Agnoli, C.; Ferrari, P.; Sonestedt, E.; Chajès, V.; Bueno-de-Mesquita, H.B.; Kaaks, R.; et al. Dietary fat intake in the european prospective investigation into cancer and nutrition: Results from the 24-h dietary recalls. Eur. J. Clin. Nutr. 2009, 63, S61–S80. [Google Scholar] [CrossRef]
- Liu, Y.; De, A. Multiple imputation by fully conditional specification for dealing with missing data in a large epidemiologic study. Int. J. Stat. Med. Res. 2015, 4, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1231S. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Giovannucci, E. Substitution analysis in nutritional epidemiology: Proceed with caution. Eur. J. Epidemiol. 2018, 33, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Abeysekera, W.; Sooriyarachchi, M. Use of schoenfeld’s global test to test the proportional hazards assumption in the cox proportional hazards model: An application to a clinical study. J. Natl. Sci. Found. Sri Lanka 2009, 37, 41–51. [Google Scholar] [CrossRef]
- Kelemen, L.E.; Kushi, L.H.; Jacobs, D.R., Jr.; Cerhan, J.R. Associations of dietary protein with disease and mortality in a prospective study of postmenopausal women. Am. J. Epidemiol. 2005, 161, 239–249. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. Prisma 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic Reviews of Etiology and Risk; The Joanna Briggs Institute: Adelaide, Australia, 2020. [Google Scholar]
- Brandt, P.A.V.D. Red meat, processed meat, and other dietary protein sources and risk of overall and cause-specific mortality in the netherlands cohort study. Eur. J. Epidemiol. 2019, 34, 351–369. [Google Scholar] [CrossRef]
- Grant, W.B. A multicountry ecological study of cancer incidence rates in 2008 with respect to various risk-modifying factors. Nutrients 2014, 6, 163–189. [Google Scholar] [CrossRef]
- Lortet-Tieulent, J.; Georges, D.; Bray, F.; Vaccarella, S. Profiling global cancer incidence and mortality by socioeconomic development. Int. J. Cancer 2020, 147, 3029–3036. [Google Scholar] [CrossRef]
- Richardson, S.; Stücker, I.; Hémon, D. Comparison of relative risks obtained in ecological and individual studies: Some methodological considerations. Int. J. Epidemiol. 1987, 16, 111–120. [Google Scholar] [CrossRef]
- Greenland, S.; Morgenstern, H. Ecological bias, confounding, and effect modification. Int. J. Epidemiol. 1989, 18, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Franco, O.H.; Lamballais, S.; Ikram, M.A.; Schoufour, J.D.; Muka, T.; Voortman, T. Associations of specific dietary protein with longitudinal insulin resistance, prediabetes and type 2 diabetes: The rotterdam study. Clin. Nutr. 2020, 39, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Lynch, C.J.; Adams, S.H. Branched-chain amino acids in metabolic signalling and insulin resistance. Nat. Rev. Endocrinol. 2014, 10, 723–736. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Bolca, S.; Vandevijvere, S.; De Vriese, S.; Mouratidou, T.; De Neve, M.; Polet, A.; Van Oyen, H.; Van Camp, J.; De Backer, G.; et al. Plant and animal protein intake and its association with overweight and obesity among the belgian population. Br. J. Nutr. 2011, 105, 1106–1116. [Google Scholar] [CrossRef]
- Kanarek, N.; Petrova, B.; Sabatini, D.M. Dietary modifications for enhanced cancer therapy. Nature 2020, 579, 507–517. [Google Scholar] [CrossRef]
- Yin, J.; Ren, W.; Huang, X.; Li, T.; Yin, Y. Protein restriction and cancer. Biochim. Biophys. Acta Rev. Cancer 2018, 1869, 256–262. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total (N = 24,106) n (%)/Mean (SD) | Alive (N = 20,077) n (%)/Mean (SD) | Dead (N = 4029) n (%)/Mean (SD) |
|---|---|---|---|
| Follow-up (years, median, inter-quartile range) | 22.7 (21.7–23.8) | 22.9 (22.1–23.9) | 16.1 (10.6–22.5) |
| Cause of death | |||
| Cancer | 1603 (39.7) | ||
| Cardiovascular | 982 (24.3) | ||
| Other causes | 1444 (35.8) | ||
| Age at recruitment (years, median, inter-quartile range) | 51.4 (43.5–57.5) | 49.1 (42.8–56.2) | 58.1 (52.6–62.1) |
| Age categories (years) | |||
| <40 | 2333 (9.6) | 2271 (11.3) | 62 (1.5) |
| 40–44 | 4685 (19.4) | 4377 (21.8) | 308 (7.6) |
| 45–49 | 4274 (17.7) | 3896 (19.4) | 378 (9.3) |
| 50–54 | 4486 (18.6) | 3824 (19.1) | 662 (16.4) |
| 55–59 | 4268 (17.7) | 3258 (16.2) | 1010 (25.1) |
| ≥60 | 4060 (16.8) | 2451 (12.1) | 1609 (39.9) |
| Sex | |||
| Female | 12,783 (53.1) | 11,373 (56.6) | 1410 (35) |
| Male | 11,323 (46.9) | 8704 (43.3) | 2619 (65) |
| BMI (kg/m2) | |||
| <18.5 | 201 (0.83) | 171 (0.8) | 30 (0.7) |
| ≥18–<25 | 10,301 (42.7) | 9183 (45.7) | 1118 (27.7) |
| ≥25–<30 | 9656 (40.1) | 7823 (38.9) | 1833 (45.5) |
| ≥30–<35 | 3107 (12.8) | 2319 (11.5) | 788 (19.5) |
| ≥35 | 841 (3.49) | 581 (2.8) | 260 (6.4) |
| Alcohol intake at recruitment (g/day) | |||
| Non-drinkers | 1300 (5.3) | 924 (4.6) | 376 (9.3) |
| 0–6 | 5798 (24.1) | 4936 (24.5) | 862 (21.3) |
| 6–12 | 6260 (25.9) | 5474 (27.2) | 786 (19.5) |
| 12–24 | 4689 (19.4) | 4007 (19.9) | 682 (16.9) |
| 24–60 | 4796 (19.9) | 3896 (19.4) | 900 (22.3) |
| 60–96 | 1044 (4.3) | 728 (3.6) | 316 (7.8) |
| >96 | 219 (0.9) | 112 (0.5) | 107 (2.6) |
| Smoking status | |||
| Never | 10,217 (42.3) | 8832 (43.9) | 1385 (34.3) |
| Long-time quitter | 5523 (22.9) | 4635 (23.1) | 888 (22.1) |
| Short-time quitter | 2676 (11.1) | 2259 (11.2) | 417 (10.3) |
| Current light | 2723 (11.3) | 2246 (11.1) | 477 (11.8) |
| Current heavy | 2523 (10.4) | 1767 (8.8) | 756 (18.7) |
| Pipe/cigar/occasional | 444 (1.84) | 338 (1.6) | 106 (2.6) |
| Total energy (kcal) | 1973.6 (634.9) | 1958.5 (621.2) | 2049.2 (694.7) |
| Animal protein (kcal) | 152.1 (69.4) | 149.8 (67.6) | 163.8 (76.9) |
| Non-animal protein (kcal) | 139.6 (48.1) | 139.1 (47.3) | 142.2 (51.2) |
| Total fat (kcal) | 687.7 (262.7) | 685.1 (258.1) | 700.5 (284.3) |
| Saturated fat (kcal) | 285.8 (118.1) | 285.5 (116.6) | 287.5 (125.4) |
| Mono-unsaturated fat (kcal) | 240.5 (96.3) | 239.4 (94.5) | 245.9 (104.6) |
| Poly-unsaturated fat (kcal) | 112.9 (47.4) | 112.1 (46.1) | 117.6 (53.5) |
| Mono- and di-saccharide (kcal) | 397.9 (200.3) | 397.7 (196.2) | 398.6 (220.1) |
| Other carbohydrate (kcal) | 470.4 (170.1) | 468.7 (168.3) | 479.2 (178.2) |
| Substitution of 3% of Energy from | Animal Protein (HR, 95% CI) | Non-Animal Protein (HR, 95% CI) | Saturated Fat (HR, 95% CI) | Mono-Unsaturated Fat (HR, 95% CI) | Poly-Unsaturated Fat (HR, 95% CI) | Mono- and Di-Saccharide (HR, 95% CI) | Other Carbohydrate (HR, 95% CI) | |
|---|---|---|---|---|---|---|---|---|
| A | Animal protein for | 1.12 (1.04–1.22) * | 1.18 (1.12–1.25) * | 1.12 (1.03–1.22) * | 1.07 (1.01–1.15) * | 1.12 (1.08–1.16) * | 1.14 (1.11–1.19) * | |
| Non-animal protein for | 0.88 (0.81–0.96) * | 1.05 (0.96–1.14) | 0.99 (0.89–1.11) | 0.95 (0.86–1.05) | 0.99 (0.91–1.08) | 1.01 (0.93–1.11) | ||
| Saturated fat for | 0.84 (0.79–0.89) * | 0.95 (0.87–1.03) | 0.94 (0.84–1.05) | 0.91 (0.85–0.96) * | 0.94 (0.90–0.99) * | 0.96 (0.91–1.01) | ||
| Mono-unsaturated for | 0.88 (0.81–0.96) * | 1.003 (0.90–1.11) | 1.05 (0.94–1.17) | 0.95 (0.85–1.07) | 0.99 (0.93–1.07) | 1.02 (0.95–1.09) | ||
| Poly-unsaturated for | 0.92 (0.86–0.99) * | 1.04 (0.94–1.15) | 1.10 (1.04–1.16) * | 1.04 (0.93–1.17) | 1.04 (0.98–1.11) | 1.06 (1.001–1.13) * | ||
| Monosaccharide for | 0.88 (0.85–0.92) * | 1.004 (0.92–1.09) | 1.05 (1.00–1.10) * | 1.001 (0.93–1.07) | 0.95 (0.90–1.01) | 1.02 (1.001–1.04) * | ||
| Other carbohydrate for | 0.87 (0.84–0.90) * | 0.98 (0.90–1.07) | 1.03 (0.98–1.08) | 0.98 (0.91–1.05) | 0.93 (0.88–0.99) * | 0.98 (0.96–0.99) * | ||
| B | Animal protein for | 1.07 (0.99–1.17) | 1.11 (1.05–1.17) * | 1.10 (1.01–1.20) * | 1.01 (0.95–1.08) | 1.07 (1.03–1.11) * | 1.07 (1.03–1.11) * | |
| Non-animal protein for | 0.92 (0.85–1.01) | 1.03 (0.94–1.11) | 1.02 (0.91–1.14) | 0.94 (0.85–1.04) | 0.99 (0.91–1.07) | 0.99 (0.91–1.08) | ||
| Saturated fat for | 0.90 (0.85–0.95) * | 0.97 (0.89–1.05) | 0.99 (0.89–1.11) | 0.91 (0.86–0.96) * | 0.96 (0.91–1.01) | 0.97 (0.92–1.02) | ||
| Mono-unsaturated for | 0.90 (0.83–0.98) * | 0.97 (0.87–1.08) | 1.01 (0.90–1.12) | 0.91 (0.82–1.02) | 0.97 (0.91–1.03) | 0.97 (0.91–1.04) | ||
| Poly-unsaturated for | 0.98 (0.92–1.05) | 1.06 (0.96–1.17) | 1.09 (1.03–1.15) * | 1.08 (0.97–1.21) | 1.05 (0.99–1.12) | 1.06 (0.99–1.12) | ||
| Monosaccharide for | 0.93 (0.90–0.96) * | 1.01 (0.92–1.09) | 1.03 (0.98–1.09) | 1.03 (0.96–1.10) | 0.94 (0.89–1.01) | 1.01 (0.98–1.02) | ||
| Other carbohydrate for | 0.92 (0.89–0.96) * | 1.001 (0.91–1.09) | 1.03 (0.98–1.08) | 1.02 (0.95–1.09) | 0.94 (0.88–1.002) | 0.99 (0.97–1.01) | ||
| C | Animal protein for | 1.02 (0.94–1.11) | 1.09 (1.03–1.15) * | 1.11 (1.02–1.21) * | 0.98 (0.92–1.05) | 1.06 (1.03–1.11) * | 1.05 (1.01–1.09) * | |
| Non-animal protein for | 0.97 (0.90–1.06) | 1.07 (0.98–1.16) | 1.09 (0.97–1.21) | 0.96 (0.87–1.06) | 1.04 (0.96–1.13) | 1.03 (0.94–1.12) | ||
| Saturated fat for | 0.91 (0.86–0.96) * | 0.93 (0.85–1.01) | 1.01 (0.91–1.13) | 0.90 (0.85–0.95) * | 0.97 (0.92–1.02) | 0.96 (0.91–1.01) | ||
| Mono-unsaturated for | 0.89 (0.82–0.97) * | 0.91 (0.82–1.02) | 0.98 (0.88–1.09) | 0.88 (0.79–0.99) | 0.95 (0.89–1.02) | 0.94 (0.88–1.01) | ||
| Poly-unsaturated for | 1.01 (0.94–1.08) | 1.03 (0.93–1.14) | 1.10 (1.04–1.17) * | 1.12 (1.01–1.26) | 1.08 (1.01–1.14) * | 1.06 (1.004–1.13) * | ||
| Monosaccharide for | 0.93 (0.90–0.97) * | 0.95 (0.88–1.03) | 1.02 (0.97–1.07) | 1.04 (0.97–1.11) | 0.92 (0.87–0.98) * | 0.98 (0.96–1.01) | ||
| Other carbohydrate for | 0.94 (0.91–0.98) * | 0.96 (0.88–1.05) | 1.03 (0.98–1.09) | 1.05 (0.98–1.13) | 0.93 (0.88–0.99) * | 1.01 (0.99–1.03) |
| Author, Year | Model | N | Duration of Follow-Up (Years) | No. of Deaths | Adjusted Covariates | Cohort, Country | Nutrient/Food Breakdown | Interpretation of Results | Adjusted for Total Energy | Result * | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Budhathoki et al., 2019 [8] | Nutrient density | 70,696 | 18 | All = 12,381 CVD = 3025 Cancer = 5055 | Age, sex, BMI, smoking status, alcohol intake, physical activity, occupational status, coffee consumption and green tea consumption, total energy | Japan Public Health Center-based Prospective Cohort, Japan | Animal protein, plant protein, saturated fat, mono-unsaturated fat, polyunsaturated fat and other fat | Quintile categories | Yes | All-cause mortality Lower quintile of plant protein intake compared to highest quintile quintile 1, reference category quintile 2, 0.89 (0.83–0.95) quintile 3, 0.88 (0.82–0.95) quintile 4, 0.84 (0.77–0.92) quintile 5, 0.87 (0.78–0.96) Cardiovascular mortality Lower quintile of plant protein intake compared to highest quintile quintile 1, reference category quintile 5, 0.73 (0.59–0.91) |
| Plant protein source, red meat, processed meat, chicken, egg, dairy, fish | 3% energy substitution | Yes | All-cause mortality Plant protein for red meat = 0.66 (0.55–0.80) Plant protein for processed meat = 0.54 (0.38–0.75) Cardiovascular mortality Plant protein for red meat = 0.58 (0.39–0.86) Cancer mortality Plant protein for red meat = 0.61 (0.45–0.82) Plant protein for processed meat = 0.50 (0.30–0.85) | ||||||||
| 2 | Chen et al., 2020 [6] | Nutrient density | 7786 | 13 | All = 3589 CVD = 877 Cancer = 896 | Age, sex, study cohort, fiber, overall diet quality score, physical activity, education level, smoking status and BMI. | The Rotterdam Study (RS-I, RS-II and RS-III combined), the Netherlands | Animal protein, plant protein, saturated fatty acid, mono-unsaturated fatty acid, poly-unsaturated fatty acid, trans fat alcohol | 5% energy substitution | Yes | All-cause mortality Animal protein for carbohydrate = 1.20 (1.05, 1.37) Cardiovascular mortality Animal protein for carbohydrate = 1.19 (1.04–1.37) |
| 3 | Huang et al., 2020 [10] | Nutrient density | 416,104 | 16 | All = 77,614 CVD = 22,228 Cancer = 28,099 | Age, BMI, alcohol, smoking, physical activity, race or ethnic group, education level, marital status, diabetes, health status, vitamin supplement use, total energy, animal protein, saturated fat, poly-unsaturated fat, mono-unsaturated fat, trans fat, fiber, vegetable and fruits. For the endpoint with cancer, mortality model was further adjusted for history of cancer in a first-degree relative. | US National Institute of Health-AARP Diet and Health Study, the United States | Plant protein, animal protein, saturated fat, poly-unsaturated fat, monounsaturated fat, trans fat | Per 1 SD increase | Yes | All-cause mortality Per 1 SD increase in plant protein intake In men, 0.95 (0.94–0.97) In women, 0.95 (0.93–0.96) Cardiovascular mortality Per 1 SD increase in plant protein intake In men, 0.95 (0.93–0.98) In women, 0.93 (0.90–0.97) |
| Red meat, white meat, dairy, egg | 5% energy substitution | Yes | All-cause mortality Plant protein for red meat In men, 0.87 (0.85–0.90) In women, 0.85 (0.81–0.88) Plant protein for dairy In men, 0.92 (0.89–0.95) In women, 0.92 (0.89–0.95) Plant protein for egg In men, 0.76 (0.72–0.80) In women, 0.79 (0.73–0.85) Cardiovascular mortality Plant protein for red meat In men, 0.88 (0.83–0.93) In women, 0.82 (0.76–0.89) Plant protein for dairy In men, 0.89 (0.84–0.94) In women, 0.88 (0.82–0.95) Plant protein for egg In men, 0.74 (0.67–0.82) In women, 0.72 (0.63–0.83) Cancer mortality Plant protein for red meat In men, 0.93 (0.88–0.98) In women, 0.89 (0.83–0.95) Plant protein for egg In men, 0.85 (0.78–0.93) In women, 0.83 (0.73–0.93) | ||||||||
| 4 | Kelemen et al., 2005 [25] | Nutrient density | 29,017 | 15 | All = 3978 CVD = 739 Cancer = 1676 | Age, total energy, saturated fat, poly-unsaturated fat, mono-unsaturated fat, trans fat, total fiber, dietary cholesterol, dietary methionine, alcohol, smoking, activity level, BMI, history of hypertension, postmenopausal hormone use, multivitamin use, vitamin E supplement use, education and history of cancer | Iowa Women’s Health Study, the United States | Animal protein, plant protein, saturated fat, poly-unsaturated fat, monounsaturated fat and trans fat | Difference in median energy intake of protein between the highest and lowest quintile | Yes | Cardiovascular mortality Vegetable protein for carbohydrate = 0.70 (0.49–0.99) Vegetable protein for animal protein = 0.70 (0.51–0.98) |
| Carbohydrate-rich food, legumes, dairy, eggs, red meats, poultry, fish | Servings per 1000 kcal | Yes | All-cause mortality Red meat for carbohydrate-rich food = 1.16 (1.02–1.32) Cardiovascular mortality Dairy for carbohydrate-rich food = 1.41 (1.07–1.87) Red meat for carbohydrate-rich food = 1.44 (1.06–1.94) Cancer mortality Legumes for carbohydrate-rich food = 1.23 (1.04–1.46) | ||||||||
| 5 | Song et al., 2016 [9] | Nutrient density model | 131,342 | 26 | 36,115 | Age, multivitamin use, smoking status, pack-years of smoking, BMI, physical activity, alcohol consumption, hypertension, glycemic index, whole grains, fiber, fruits and vegetables. | The Nurses’ Health Study (NHS) and The Health Professionals Follow-up Study (HPFS), the United States | Plant protein, saturated, mono-unsaturated, poly-unsaturated and trans fatty acid. | 10% energy substitution | Yes | Cardiovascular mortality Animal protein for carbohydrate = 1.08 (1.01–1.16) |
| 6 | Sun et al., 2021 [11] | Nutrient density model | 102,521 | 18 | All = 25,976 CVD = 6993 Cancer = 7516 | Age, race/ethnicity, education, income, observational study/clinical trial, unopposed estrogen use, estrogen + progesterone use, smoking, physical activity, alcohol intake, total energy intake, baseline diabetes mellitus, baseline high cholesterol status, family history of heart attack/stroke, dietary fiber intake, glycemic load and BMI | Women’s Health Initiative, Unites States | Animal protein, plant protein, saturated fatty acids, poly-unsaturated fatty acid, mono-unsaturated fatty acids and trans fat | 5% energy substitution | Yes | All-cause mortality plant protein for animal protein = 0.86 (0.81–0.91) Cardiovascular mortality plant protein for animal protein = 0.78 (0.70–0.87) |
| Total red meat, unprocessed red meat, processed red meat, poultry, fish/shellfish, eggs, dairy products, legumes, nuts | OZ equivalent per day for red meat, poultry, fish, eggs, legumes and nuts Cup equivalent per day for dairy products | Yes |
All-cause mortality
Red meat for nuts = 0.89 (0.81–0.98) Eggs for nuts = 0.53 (0.45–0.61) Dairy for nuts = 0.88 (0.80–0.97) Legumes for nuts = 0.86 (0.74–0.99) Cardiovascular mortality Eggs for nuts = 0.44 (0.33–0.58) Dairy for nuts = 0.81 (0.67–0.97) Legumes for nuts = 0.70 (0.53–0.92) Cancer mortality Eggs for nuts = 0.59 (0.45–0.78) | ||||||||
| 7 | Van den Brandt, 2019 [28] | Standard multivariate | 13,823 | 10 | All = 8823 CVD = 2985 Cancer = 3917 | Age; cigarette smoking; number of cigarettes smoked per day; years of smoking; history of physician-diagnosed hypertension; diabetes; BMI; non-occupational physical activity; highest level of education; intake of alcohol, vegetables, and fruits; energy; use of nutritional supplement; and, in women, post-menopausal use of hormone replacement therapy | The Netherlands Cohort Study | Poultry, eggs, fish, nuts, pulses, low-fat dairy | 50 g/day substitution | Yes |
All-cause mortality
Nuts for processed meat = 0.65 (0.49–0.85) Cardiovascular mortality Nuts for processed meat = 0.62 (0.44–0.88) Cancer mortality Nuts for processed meat = 0.73 (0.54–0.99) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bajracharya, R.; Katzke, V.; Mukama, T.; Kaaks, R. Effect of Iso-Caloric Substitution of Animal Protein for Other Macro Nutrients on Risk of Overall, Cardiovascular and Cancer Mortality: Prospective Evaluation in EPIC-Heidelberg Cohort and Systematic Review. Nutrients 2023, 15, 794. https://doi.org/10.3390/nu15030794
Bajracharya R, Katzke V, Mukama T, Kaaks R. Effect of Iso-Caloric Substitution of Animal Protein for Other Macro Nutrients on Risk of Overall, Cardiovascular and Cancer Mortality: Prospective Evaluation in EPIC-Heidelberg Cohort and Systematic Review. Nutrients. 2023; 15(3):794. https://doi.org/10.3390/nu15030794
Chicago/Turabian StyleBajracharya, Rashmita, Verena Katzke, Trasias Mukama, and Rudolf Kaaks. 2023. "Effect of Iso-Caloric Substitution of Animal Protein for Other Macro Nutrients on Risk of Overall, Cardiovascular and Cancer Mortality: Prospective Evaluation in EPIC-Heidelberg Cohort and Systematic Review" Nutrients 15, no. 3: 794. https://doi.org/10.3390/nu15030794
APA StyleBajracharya, R., Katzke, V., Mukama, T., & Kaaks, R. (2023). Effect of Iso-Caloric Substitution of Animal Protein for Other Macro Nutrients on Risk of Overall, Cardiovascular and Cancer Mortality: Prospective Evaluation in EPIC-Heidelberg Cohort and Systematic Review. Nutrients, 15(3), 794. https://doi.org/10.3390/nu15030794