
Does Better Diet Quality Offset the Association between Depression and Metabolic Syndrome?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Data Collection
2.2. Methods and Variables
2.2.1. Socio-Demographic Factors
2.2.2. Assessment of Depressive Symptoms
2.2.3. Assessment of MetS
2.2.4. Assessment of Diet Intake and Diet Quality
2.3. Statistical Analysis
3. Results
3.1. Socio-Demographic Factors According to Depression Severity
3.2. Diet Quality Measured by KHEI According to Depression Severity Groups
3.3. KHEI Scores and Nutrient Intakes According to Tertiles of KHEI scores
3.4. MetS Parameters According to Depression Severity Groups
3.5. Adjusted OR (95% CI) for MeSe According to Depression Severity Groups
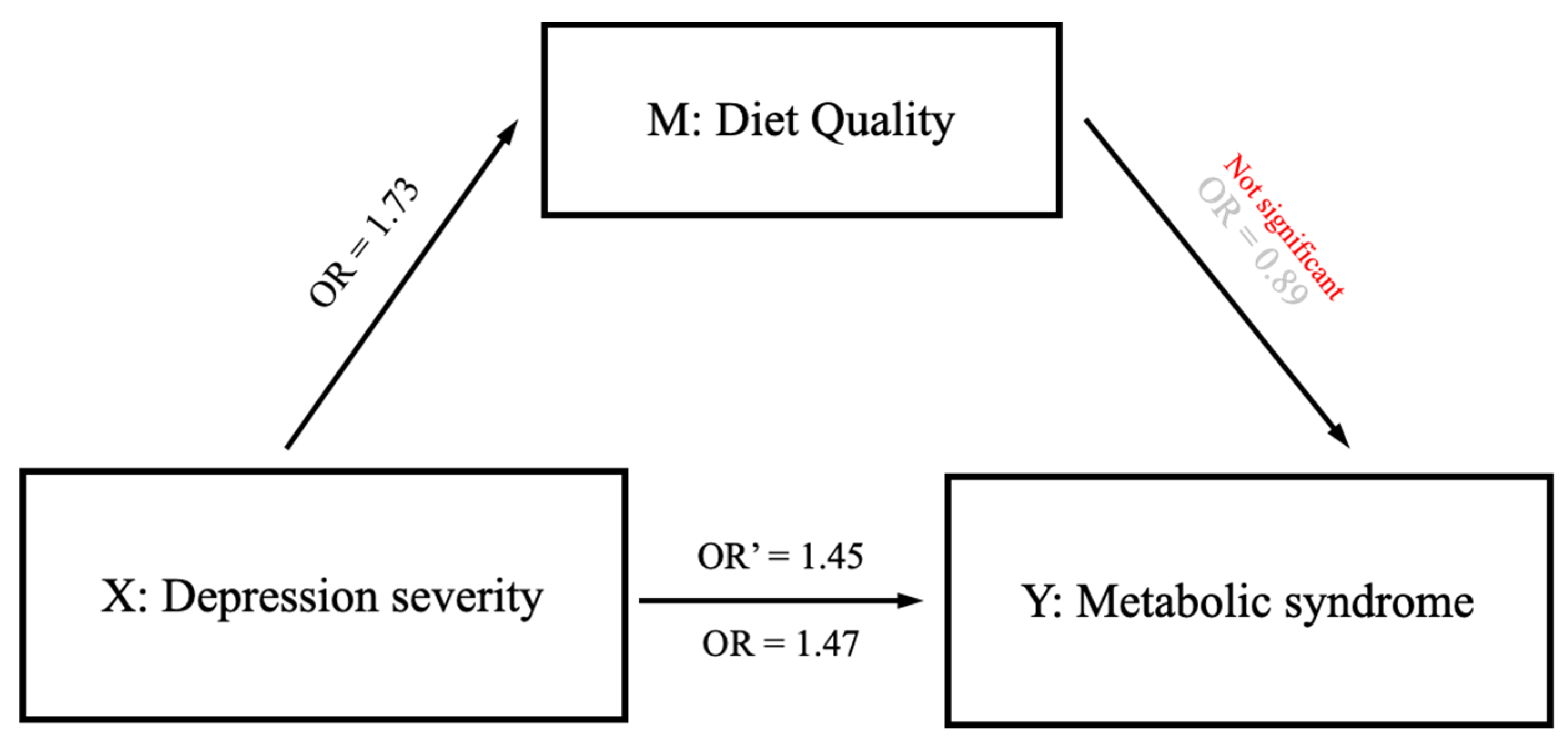
3.6. Effect Modification of Diet Quality on Association between Depression and MetS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Institute of Health Metrics and Evaluation. Global Health Data Exchange (GHDx). Available online: http://ghdx.healthdata.org/gbd-results-tool?params=gbd-api-2019-permalink/d780dffbe8a381b25e1416884959e88b (accessed on 23 March 2022).
- Murray, C.J.; Aravkin, A.Y.; Zheng, P.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Borzouei, S. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, T.; Nakao, M.; Nomura, K.; Yano, E. Association of Metabolic Syndrome with Depression and Anxiety in Japanese Men. Diabetes Metab. 2009, 35, 32–36. [Google Scholar] [CrossRef] [PubMed]
- van Leijden, M.J.; Penninx, B.W.; Agyemang, C.; Olff, M.; Adriaanse, M.C.; Snijder, M.B. The Association of Depression and Posttraumatic Stress Disorder with the Metabolic Syndrome in a Multi-Ethnic Cohort: The HELIUS Study. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 921–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vargas, H.O.; Nunes, S.O.V.; Barbosa, D.S.; Vargas, M.M.; Cestari, A.; Dodd, S.; Venugopal, K.; Maes, M.; Berk, M. Castelli Risk Indexes 1 and 2 are Higher in Major Depression but Other Characteristics of the Metabolic Syndrome are Not Specific to Mood Disorders. Life Sci. 2014, 102, 65–71. [Google Scholar] [CrossRef]
- Moradi, Y.; Albatineh, A.N.; Mahmoodi, H.; Gheshlagh, R.G. The Relationship between Depression and Risk of Metabolic Syndrome: A meta-analysis of Observational Studies. Clin. Diabetes Endocrinol. 2021, 7, 1–12. [Google Scholar] [CrossRef]
- Marazziti, D.; Rutigliano, G.; Baroni, S.; Landi, P.; Dell’Osso, L. Metabolic Syndrome and Major Depression. CNS Spectr. 2014, 19, 293–304. [Google Scholar] [CrossRef]
- Bjorntorp, P. Do Stress Reactions Cause Abdominal Obesity and Comorbidities? Obes. Rev. 2001, 2, 73–86. [Google Scholar] [CrossRef]
- McIntyre, R.S.; Soczynska, J.K.; Konarski, J.Z.; Woldeyohannes, H.O.; Law, C.W.; Miranda, A.; Fulgosi, D.; Kennedy, S.H. Should Depressive Syndromes be Reclassified as “metabolic Syndrome Type II”? Ann. Clin. Psychiatry 2007, 19, 257–264. [Google Scholar] [CrossRef]
- Valtonen, M.K.; Laaksonen, D.E.; Laukkanen, J.A.; Tolmunen, T.; Viinamäki, H.; Lakka, H.; Lakka, T.A.; Niskanen, L.; Kauhanen, J. Low-Grade Inflammation and Depressive Symptoms as Predictors of Abdominal Obesity. Scand. J. Public Health 2012, 40, 674–680. [Google Scholar] [CrossRef]
- Liu, Y.; Ozodiegwu, I.D.; Yu, Y.; Hess, R.; Bie, R. An Association of Health Behaviors with Depression and Metabolic Risks: Data from 2007 to 2014 US National Health and Nutrition Examination Survey. J. Affect. Disord. 2017, 217, 190–196. [Google Scholar] [CrossRef]
- Beydoun, M.A.; Kuczmarski, M.T.F.; Mason, M.A.; Ling, S.M.; Evans, M.K.; Zonderman, A.B. Role of Depressive Symptoms in Explaining Socioeconomic Status Disparities in Dietary Quality and Central Adiposity among US Adults: A Structural Equation Modeling Approach. Am. J. Clin. Nutr. 2009, 90, 1084–1095. [Google Scholar] [CrossRef] [Green Version]
- Morris, L.; Bhatnagar, D. The Mediterranean diet. Curr. Opin. Lipidol. 2016, 27, 89–91. [Google Scholar] [CrossRef]
- Ventriglio, A.; Sancassiani, F.; Contu, M.P.; Latorre, M.; Di Slavatore, M.; Fornaro, M.; Bhugra, D. Mediterranean Diet and its Benefits on Health and Mental Health: A Literature Review. Clin. Pract. Epidemiol. Ment. Health 2020, 16, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Giugliano, D.; Esposito, K. Mediterranean Diet and Metabolic Diseases. Curr. Opin. Lipidol. 2008, 19, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Buckland, G.; Bach, A.; Serra-Majem, L. Obesity and the Mediterranean Diet: A Systematic Review of Observational and Intervention Studies. Obes. Rev. 2008, 9, 582–593. [Google Scholar] [CrossRef]
- Peltzer, K.; Pengpid, S. High Prevalence of Depressive Symptoms in a National Sample of Adults in Indonesia: Childhood Adversity, Sociodemographic Factors and Health Risk Behaviour. Asian J. Psychiatry 2018, 33, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Kuk, J.L.; Ardern, C.I. Age and Sex Differences in the Clustering of Metabolic Syndrome Factors: Association with Mortality Risk. Diabetes Care 2010, 33, 2457–2461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brug, J.; van der Ploeg, H.P.; Loyen, A.; Ahrens, W.; Allais, O.; Andersen, L.F.; Cardon, G.; Capranica, L.; Chastin, S.; De Bourdeaudhuij, I. Determinants of Diet and Physical Activity (DEDIPAC): A Summary of Findings. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Data. Korean National Health and Nutrition Examination Survey (KNHANES). Ministry of Health and Welfare (KR). Available online: https://knhanes.kdca.go.kr/knhanes/main.do (accessed on 1 March 2021).
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Patient Health Questionnaire Primary Care Study Group. Validation and Utility of a Self-Report Version of PRIME-MD: The PHQ Primary Care Study. JAMA 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [Green Version]
- Choi, H.S.; Choi, J.H.; Park, K.H.; Joo, K.J.; Ga, H.; Ko, H.J.; Kim, S.R. Standardization of the Korean Version of Patient Health Questionnaire-9 as a Screening Instrument for Major Depressive Disorder. J. Korean Acad. Fam. Med. 2007, 28, 114–119. [Google Scholar]
- Park, S.; Choi, H.; Choi, J.; Kim, K.; Hong, J. Reliability and Validity of the Korean Version of the Patient Health Questionnaire-9 (PHQ-9). Anxiety Mood 2010, 6, 119–124. [Google Scholar]
- Lee, S.; Huh, Y.; Kim, J. Finding Optimal Cut Off Points of the Korean Version of the Patient Health Questionnaire-9 (PHQ-9) for Screening Depressive Disorders. Mood Emot 2014, 12, 32–36. [Google Scholar]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith Jr, S.C. Diagnosis and Management of the Metabolic Syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yook, S.; Park, S.; Moon, H.; Kim, K.; Shim, J.E.; Hwang, J. Development of Korean Healthy Eating Index for Adults using the Korea National Health and Nutrition Examination Survey Data. J. Nutr. Health 2015, 48, 419–428. [Google Scholar] [CrossRef] [Green Version]
- Yun, S.; Oh, K. Development and status of Korean Healthy Eating Index for adults based on the Korea National Health and Nutrition Examination Survey. Public Health Wkly Rep. 2018, 11, 1764–1772. [Google Scholar]
- Yun, S.; Park, S.; Yook, S.; Kim, K.; Shim, J.E.; Hwang, J.; Oh, K. Development of the Korean Healthy Eating Index for Adults, Based on the Korea National Health and Nutrition Examination Survey. Nutr. Res. Pract. 2022, 16, 233–247. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare, The Korean Nutrition Society. Dietary Reference Intakes for Koreans 2015; Ministry of Health and Welfare: Sejong, Republic of Korea, 2015.
- East, C.; Willis, B.L.; Barlow, C.E.; Grannemann, B.D.; FitzGerald, S.J.; DeFina, L.F.; Trivedi, M.H. Depressive Symptoms and Metabolic Syndrome in Preventive Healthcare: The Cooper Center Longitudinal Study. Metab. Syndr. Relat. Disord. 2010, 8, 451–457. [Google Scholar] [CrossRef]
- Vanderweele, T.J.; Vansteelandt, S. Odds ratios for mediation analysis for a dichotomous outcome. Am. J. Epidemiol. 2010, 172, 1339–1348. [Google Scholar] [CrossRef]
- Goldstein, P.; Leshem, M. Dietary Sodium, Added Salt, and Serum Sodium Associations with Growth and Depression in the US General Population. Appetite 2014, 79, 83–90. [Google Scholar] [CrossRef]
- Thi Thu Nguyen, T.; Miyagi, S.; Tsujiguchi, H.; Kambayashi, Y.; Hara, A.; Nakamura, H.; Suzuki, K.; Yamada, Y.; Shimizu, Y.; Nakamura, H. Association between Lower Intake of Minerals and Depressive Symptoms among Elderly Japanese Women but Not Men: Findings from Shika Study. Nutrients 2019, 11, 389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newson, R.; Elmadfa, I.; Biro, G.; Cheng, Y.; Prakash, V.; Rust, P.; Barna, M.; Lion, R.; Meijer, G.; Neufingerl, N. Barriers for Progress in Salt Reduction in the General Population. Int. Study Appet. 2013, 71, 22–31. [Google Scholar]
- Ghanei Gheshlagh, R.; Parizad, N.; Sayehmiri, K. The Relationship between Depression and Metabolic Syndrome: Systematic Review and Meta-Analysis Study. Iran. Red Crescent Med. J. 2016, 18, e26523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, A.; Keum, N.; Okereke, O.I.; Sun, Q.; Kivimaki, M.; Rubin, R.R.; Hu, F.B. Bidirectional Association between Depression and Metabolic Syndrome: A Systematic Review and Meta-Analysis of Epidemiological Studies. Diabetes Care 2012, 35, 1171–1180. [Google Scholar] [CrossRef] [Green Version]
- Vancampfort, D.; Correll, C.U.; Wampers, M.; Sienaert, P.; Mitchell, A.; De Herdt, A.; Probst, M.; Scheewe, T.W.; De Hert, M. Metabolic Syndrome and Metabolic Abnormalities in Patients with Major Depressive Disorder: A Meta-Analysis of Prevalences and Moderating Variables. Psychol. Med. 2014, 44, 2017–2028. [Google Scholar] [CrossRef] [Green Version]
- Park, S.J.; Roh, S.; Hwang, J.; Kim, H.A.; Kim, S.; Lee, T.K.; Kang, S.H.; Ha, Y.J.; Jang, J.W.; Park, S. Association between Depression and Metabolic Syndrome in Korean Women: Results from the Korean National Health and Nutrition Examination Survey (2007–2013). J. Affect. Disord. 2016, 205, 393–399. [Google Scholar] [CrossRef]
- Ma, M.; Liu, H.; Yu, J.; He, S.; Li, P.; Ma, C.; Zhang, H.; Xu, L.; Ping, F.; Li, W. Triglyceride is Independently Correlated with Insulin Resistance and Islet Beta Cell Function: A Study in Population with Different Glucose and Lipid Metabolism States. Lipids Health Dis. 2020, 19, 121. [Google Scholar] [CrossRef]
- Acierno, C.; Caturano, A.; Pafundi, P.C.; Nevola, R.; Adinolfi, L.E.; Sasso, F.C. Nonalcoholic fatty liver disease and type 2 diabetes: Pathophysiological mechanisms shared between the two faces of the same coin. Explor Med. 2020, 1, 287–306. [Google Scholar] [CrossRef]
- Garfinkel, A.S.; Nilsson-Ehle, P.; Schotz, M.C. Regulation of Lipoprotein Lipase: Induction by Insulin. Biochim. Biophys. Acta-Lipids Lipid Metab. 1976, 424, 264–273. [Google Scholar] [CrossRef]
- Tilg, H.; Moschen, A.R.; Roden, M. NAFLD and Diabetes Mellitus. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 32–42. [Google Scholar] [CrossRef]
- Stefan, N.; Häring, H.; Cusi, K. Non-Alcoholic Fatty Liver Disease: Causes, Diagnosis, Cardiometabolic Consequences, and Treatment Strategies. Lancet Diabetes Endocrinol. 2019, 7, 313–324. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Chen, J.; Yin, Z.; Wang, L.; Peng, L. The Association between Depression and Metabolic Syndrome and its Components: A Bidirectional Two-Sample Mendelian Randomization Study. Transl. Psychiatry 2021, 11, 633. [Google Scholar] [CrossRef]
- Bakhtiari, A.; Hashemi, M.; Hosseini, S.R.; Omidvar, S.; Bijani, A.; Khairkhah, F. The Relationship between Depression and Metabolic Syndrome in the Elderly Population: The Cohort Aging Study. Iran. J. Psychiatry. 2018, 13, 230–238. [Google Scholar] [PubMed]
- Licht, C.M.; De Geus, E.J.; Seldenrijk, A.; Van Hout, H.P.; Zitman, F.G.; Van Dyck, R.; Penninx, B.W. Depression is Associated with Decreased Blood Pressure, but Antidepressant use Increases the Risk for Hypertension. Hypertension 2009, 53, 631–638. [Google Scholar] [CrossRef] [Green Version]
- Marijnissen, R.M.; Smits, J.E.; Schoevers, R.A.; van den Brink, R.H.; Holewijn, S.; Franke, B.; de Graaf, J.; Voshaar, R.C.O. Association between Metabolic Syndrome and Depressive Symptom profiles—Sex-Specific? J. Affect. Disord. 2013, 151, 1138–1142. [Google Scholar] [CrossRef] [PubMed]
- Michalkiewicz, M.; Knestaut, K.M.; Bytchkova, E.Y.; Michalkiewicz, T. Hypotension and Reduced Catecholamines in Neuropeptide Y Transgenic Rats. Hypertension 2003, 41, 1056–1062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karl, T.; Herzog, H. Behavioral Profiling of NPY in Aggression and Neuropsychiatric Diseases. Peptides 2007, 28, 326–333. [Google Scholar] [CrossRef]
- Matta, J.; Hoertel, N.; Kesse-Guyot, E.; Plesz, M.; Wiernik, E.; Carette, C.; Czernichow, S.; Limosin, F.; Goldberg, M.; Zins, M. Diet and Physical Activity in the Association between Depression and Metabolic Syndrome: Constances Study. J. Affect. Disord. 2019, 244, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Gimeno, D.; Kivimäki, M.; Brunner, E.J.; Elovainio, M.; De Vogli, R.; Steptoe, A.; Kumari, M.; Lowe, G.D.; Rumley, A.; Marmot, M.G. Associations of C-Reactive Protein and Interleukin-6 with Cognitive Symptoms of Depression: 12-Year Follow-Up of the Whitehall II Study. Psychol. Med. 2009, 39, 413–423. [Google Scholar] [CrossRef]
- Almeida, O.P.; McCaul, K.; Hankey, G.J.; Norman, P.; Jamrozik, K.; Flicker, L. Homocysteine and Depression in Later Life. Arch. Gen. Psychiatry 2008, 65, 1286–1294. [Google Scholar] [CrossRef]
- Hotamisligil, G.S.; Shargill, N.S.; Spiegelman, B.M. Adipose Expression of Tumor Necrosis Factor-Alpha: Direct Role in Obesity-Linked Insulin Resistance. Science 1993, 259, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Grigoleit, J.; Kullmann, J.S.; Wolf, O.T.; Hammes, F.; Wegner, A.; Jablonowski, S.; Engler, H.; Gizewski, E.; Oberbeck, R.; Schedlowski, M. Dose-Dependent Effects of Endotoxin on Neurobehavioral Functions in Humans. PLoS ONE 2011, 6, e28330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dutheil, S.; Ota, K.T.; Wohleb, E.S.; Rasmussen, K.; Duman, R.S. High-fat diet induced anxiety and anhedonia: Impact on brain homeostasis and inflammation. Neuropsychopharmacology 2016, 41, 1874–1887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, S.; Kim, W.J.; Lok, J.; Lee, S.R.; Besancon, E.; Luo, B.H.; Stins, M.F.; Wang, X.; Dedhar, S.; Lo, E.H. Neuroprotection via matrix-trophic coupling between cerebral endothelial cells and neurons. Proc. Natl. Acad. Sci. USA 2008, 105, 7582–7587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kityo, A.; Kaggwa, A. Fruit and Vegetable Intake, and Metabolic Syndrome Components: A Population-Based Study. In Biology and Life Sciences Forum; MDPI: Basel, Switzerland, 2022; p. 18. [Google Scholar]
- Zhang, Y.; Zhang, D. Associations of Vegetable and Fruit Consumption with Metabolic Syndrome. A Meta-Analysis of Observational Studies. Public Health Nutr. 2018, 21, 1693–1703. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Yan, Y.; Li, F.; Zhang, D. Fruit and Vegetable Consumption and the Risk of Depression: A Meta-Analysis. Nutrition 2016, 32, 296–302. [Google Scholar] [CrossRef]
- Saghafian, F.; Malmir, H.; Saneei, P.; Milajerdi, A.; Larijani, B.; Esmaillzadeh, A. Fruit and Vegetable Consumption and Risk of Depression: Accumulative Evidence from an Updated Systematic Review and Meta-Analysis of Epidemiological Studies. Br. J. Nutr. 2018, 119, 1087–1101. [Google Scholar] [CrossRef] [Green Version]
- Narita, Z.; Nozaki, S.; Shikimoto, R.; Hori, H.; Kim, Y.; Mimura, M.; Tsugane, S.; Sawada, N. Association between Vegetable, Fruit, and Flavonoid-Rich Fruit Consumption in Midlife and Major Depressive Disorder in Later Life: The JPHC Saku Mental Health Study. Transl. Psychiatry 2022, 12, 412. [Google Scholar] [CrossRef]
- Melo de Carvalho, G.; Soares, J.D.S.; Freitas, E.P.S.; Lima, J.G.; Cunha Lima, S.C.V.; Sena-Evangelista, K.C.M. Sodium Intake in Individuals with Metabolic Syndrome: A Study Based on Sodium Content of Diet and Source Foods. Demetra Food Nutr. Health/Aliment. Nutr. Saúde 2018, 13, 975–992. [Google Scholar]
- Sanchez-Villegas, A.; Martínez-González, M.A. Diet, a new target to prevent depression? BMC Med. 2013, 11, 3. [Google Scholar] [CrossRef] [Green Version]
- Perez-Cornago, A.; de la Iglesia, R.; Lopez-Legarrea, P.; Abete, I.; Navas-Carretero, S.; Lacunza, C.I.; Zulet, M. A decline in inflammation is associated with less depressive symptoms after a dietary intervention in metabolic syndrome patients: A longitudinal study. Nutr. J. 2014, 13, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-Villegas, A.; Ruíz-Canela, M.; de la Fuente-Arrillaga, C.; Gea, A.; Shivappa, N.; Hébert, J.R.; Martínez-González, M.A. Dietary inflammatory index, cardiometabolic conditions and depression in the Seguimiento Universidad de Navarra cohort study. Br. J. Nutr. 2015, 114, 1471–1479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Mental Health Survey 2021. Ministry of Health and Welfare, National Center for Mental Health. 2021. Available online: https://mhs.ncmh.go.kr/front/reference/referenceDetail.do (accessed on 11 January 2023).
- Hamal, C.; Velugoti, L.S.D.R.; Tabowei, G.; Gaddipati, G.N.; Mukhtar, M.; Alzubaidee, M.J.; Dwarampudi, R.S.; Mathew, S.; Bichenapally, S.; Khachatryan, V. Metformin for the Improvement of Comorbid Depression Symptoms in Diabetic Patients: A Systematic Review. Cureus 2022, 14, e28609. [Google Scholar] [CrossRef]
- Laimer, M.; Kramer-Reinstadler, K.; Rauchenzauner, M.; Lechner-Schoner, T.; Strauss, R.; Engl, J.; Deisenhammer, E.A.; Hinterhuber, H.; Patsch, J.R.; Ebenbichler, C.F. Effect of Mirtazapine Treatment on Body Composition and Metabolism. J. Clin. Psychiatry 2006, 67, 421–424. [Google Scholar] [CrossRef]
- Berken, G.H.; Weinstein, D.O.; Stern, W.C. Weight Gain: A Side-Effect of Tricyclic Antidepressants. J. Affect. Disord. 1984, 7, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, A.; Jethani, S.L.; Rohatgi, R.K.; Kalra, J. Selective Serotonin Re-Uptake Inhibitors (SSRIs) Induced Weight Changes: A Dose and Duration Dependent Study on Albino Rats. J. Clin. Diagn. Res. 2016, 10, AF01–AF03. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Paz-Filho, G.; Mastronardi, C.; Licinio, J.; Wong, M. Is Increased Antidepressant Exposure a Contributory Factor to the Obesity Pandemic? Transl. Psychiatry 2016, 6, e759. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| PHQ-9 Depression Severity | |||||
|---|---|---|---|---|---|
| Variables | Normal (n = 10,888) | Mild (n = 1905) | Moderate to Severe (n = 746) | p-Value | |
| Age, years | 47.09 ± 0.26 a | 44.36 ± 0.47 b | 47.34 ± 0.79 a | <0.001 | |
| Male | 4879 (51.57) | 596 (37.10) | 204 (31.54) | <0.001 | |
| Urban residents | 8892 (85.37) | 1540 (83.95) | 583 (83.14) | 0.225 | |
| Education level | ≤Elementary school | 2103 (13.62) | 432 (16.40) | 266 (26.54) | <0.001 |
| Middle school | 1137 (8.73) | 199 (9.04) | 84 (9.31) | ||
| High school | 3603 (36.87) | 634 (36.88) | 209 (33.04) | ||
| ≥College graduate | 4045 (40.78) | 640 (37.68) | 187 (31.12) | ||
| Household Income | Low | 1769 (13.16) | 420 (18.00) | 287 (33.63) | <0.001 |
| Low-middle | 2629 (23.40) | 496 (27.24) | 195 (24.84) | ||
| Middle-high | 3142 (30.76) | 502 (27.94) | 158 (22.23) | ||
| High | 3348 (32.69) | 487 (26.82) | 106 (19.30) | ||
| Current smokers | 1787 (19.74) | 364 (23.10) | 177 (27.71) | <0.001 | |
| Alcohol drinking | Never | 2936 (22.68) | 521 (22.91) | 271 (30.49) | <0.001 |
| <1 time/month | 3140 (28.81) | 554 (29.46) | 190 (27.60) | ||
| 2–4 times/month | 2447 (25.00) | 424 (25.06) | 117 (17.86) | ||
| 2–3 times/week | 1653 (16.87) | 275 (15.49) | 91 (13.36) | ||
| ≥4 times/week | 712 (6.65) | 131 (7.07) | 77 (10.69) | ||
| Body mass index, kg/m | 23.95 ± 0.04 a | 23.53 ± 0.11 b | 23.91 ± 0.19 ab | 0.002 | |
| Physical inactivity | 5123 (50.62) | 869 (49.59) | 310 (46.57) | 0.190 | |
| Energy intake, kcal | 2087.06 ± 12.48 a | 1990.87 ± 25.92 b | 1869.10 ± 48.84 c | <0.001 | |
| No disease history | 6516 (54.79) | 1283 (60.96) | 574 (73.43) | <0.001 | |
| PHQ-9 Depression Severity | |||||
|---|---|---|---|---|---|
| Normal (n = 10,888) | Mild (n = 1905) | Moderate to Severe (n = 746) | p-Value | p Trend | |
| Total score | 63.46 ± 0.19 a | 61.11 ± 0.35 b | 58.46 ± 0.62 c | <0.001 | <0.001 |
| Adequacy item | |||||
| Having breakfast | 7.27 ± 0.06 a | 6.42 ± 0.11 b | 6.20 ± 0.19 c | <0.001 | <0.001 |
| Mixed grain intake | 2.08 ± 0.03 a | 1.86 ± 0.06 b | 1.86 ± 0.10 b | 0.021 | 0.007 |
| Total fruit intake | 2.22 ± 0.03 a | 2.14 ± 0.06 a | 1.87 ± 0.10 b | <0.001 | <0.001 |
| Fresh fruit intake | 2.41 ± 0.03 a | 2.32 ± 0.06 a | 2.05 ± 0.10 b | 0.002 | 0.001 |
| Total vegetable intake | 3.55 ± 0.02 a | 3.33 ± 0.04 a | 3.10 ± 0.07 b | <0.001 | <0.001 |
| Vegetable intake excluding kimchi and pickled vegetables | 3.28 ± 0.02 a | 3.06 ± 0.04 b | 2.90 ± 0.07 b | 0.001 | <0.001 |
| Meats/fishes/eggs/beans intake | 7.25 ± 0.04 a | 7.05 ± 0.09 a | 6.16 ± 0.17 b | <0.001 | <0.001 |
| Milk/dairy product intake | 3.36 ± 0.06 | 3.26 ± 0.12 | 2.91 ± 0.19 | 0.132 | 0.045 |
| Moderation item | |||||
| Energy from saturated fatty acid | 7.45 ± 0.04 | 7.34 ± 0.11 | 7.48 ± 0.18 | 0.913 | 0.934 |
| Sodium intake | 6.39 ± 0.05 a | 6.73 ± 0.09 ab | 7.26 ± 0.16 b | 0.038 | 0.015 |
| Energy from sweets/beverages | 9.18 ± 0.03 a | 8.90 ± 0.07 b | 8.80 ± 0.13 b | <0.001 | <0.001 |
| Balance item | |||||
| Energy from carbohydrate | 2.53 ± 0.03 | 2.48 ± 0.06 | 2.22 ± 0.09 | 0.152 | 0.054 |
| Energy from fat | 3.38 ± 0.02 a | 3.23 ± 0.06 b | 3.07 ± 0.09 b | 0.048 | 0.019 |
| Total energy intake | 3.11 ± 0.03 a | 2.99 ± 0.06 a | 2.58 ± 0.10 b | <0.001 | <0.001 |
| PHQ-9 Depression Severity | |||||
|---|---|---|---|---|---|
| Normal (N = 10,888) | Mild (n = 1905) | Moderate to Severe (n = 746) | p-Value | p Trend | |
| Protein, g | 75.20 ± 0.53 | 71.39 ± 1.11 | 64.99 ± 2.28 | 0.083 | 0.040 |
| Fat, g | 48.05 ± 0.48 | 47.17 ± 1.07 | 41.13 ± 1.55 | 0.147 | 0.967 |
| Saturated fatty acid, g | 14.98 ± 0.17 | 14.55 ± 0.36 | 12.85 ± 0.51 | 0.174 | 0.508 |
| Monounsaturated fatty acid, g | 15.47 ± 0.17 | 14.99 ± 0.39 | 12.92 ± 0.57 | 0.088 | 0.506 |
| Polyunsaturated fatty acid, g | 12.26 ± 0.13 a | 12.33 ± 0.30 a | 10.36 ± 0.45 b | 0.035 | 0.544 |
| n-3 fatty acid, g | 1.85 ± 0.02 | 1.77 ± 0.0.04 | 1.61 ± 0.09 | 0.550 | 0.981 |
| n-6 fatty acid, g | 10.41 ± 0.11 a | 10.57 ± 0.27 a | 8.75 ± 0.37 b | 0.018 | 0.497 |
| Cholesterol, mg | 260.92 ± 2.94 | 256.80 ± 7.31 | 218.73 ± 12.69 | 0.337 | 0.947 |
| Carbohydrate, g | 309.02 ± 1.62 | 295.15 ± 3.59 | 284.30 ± 7.11 | 0.476 | 0.327 |
| Dietary fiber, g | 25.55 ± 0.19 a | 23.39 ± 0.35 b | 21.48 ± 0.59 c | <0.001 | <0.001 |
| Calcium, mg | 523.96 ± 4.30 a | 496.57 ± 8.73 ab | 449.91 ± 14.38 b | 0.027 | 0.058 |
| Phosphate, mg | 1118.68 ± 6.51 | 1056.07 ± 13.52 | 974.63 ± 30.62 | 0.057 | 0.015 |
| Iron, mg | 14.20 ± 0.18 | 13.42 ± 0.26 | 12.82 ± 0.50 | 0.675 | 0.774 |
| Sodium, mg | 3725.85 ± 31.75 a | 3450.53 ± 58.66 ab | 3174.20 ± 112.84 b | 0.026 | 0.012 |
| Potassium, mg | 3004.27 ± 19.72 a | 2809.08 ± 37.49 a | 2581.21 ± 68.39 b | 0.001 | 0.003 |
| Carotene, μg | 3200.00 ± 66.52 | 2916.37 ± 86.37 | 2881.59 ± 198.19 | 0.407 | 0.640 |
| Retinol, μg | 152.80 ± 6.41 | 137.92 ± 6.79 | 118.50 ± 13.09 | 0.183 | 0.245 |
| Thiamin, mg | 1.61 ± 0.01 | 1.52 ± 0.03 | 1.45 ± 0.05 | 0.363 | 0.288 |
| Riboflavin, mg | 1.60 ± 0.01 a | 1.52 ± 0.03 ab | 1.36 ± 0.04 b | 0.035 | 0.124 |
| Niacin, mg | 15.10 ± 0.11 | 14.31 ± 0.24 | 13.48 ± 0.52 | 0.498 | 0.656 |
| Vitamin C, mg | 76.16 ± 1.27 | 72.00 ± 2.41 | 65.55 ± 4.21 | 0.301 | 0.615 |
| Diet Quality Level | |||||
|---|---|---|---|---|---|
| T1 (<58) (n = 4008) | T2 (58–69) (n = 4547) | T3 (≥70) (n = 4984) | p-Value | p Trend | |
| Total score | 48.20 ± 0.14 a | 63.46 ± 0.06 b | 76.91 ± 0.11 c | <0.001 | <0.001 |
| Adequacy item | |||||
| Have breakfast | 5.18 ± 0.08 a | 7.52 ± 0.06 b | 8.77 ± 0.05 c | <0.001 | <0.001 |
| Mixed grain intake | 1.22 ± 0.04 a | 2.02 ± 0.04 b | 2.92 ± 0.14 c | <0.001 | <0.001 |
| Total fruits intake | 1.06 ± 0.03 a | 2.11 ± 0.04 b | 3.40 ± 0.04 c | <0.001 | <0.001 |
| Fresh fruits intake | 1.16 ± 0.04 a | 2.33 ± 0.04 b | 3.66 ± 0.04 c | <0.001 | <0.001 |
| Total vegetables intake | 2.91 ± 3.56 a | 3.56 ± 0.02 b | 3.96 ± 0.02 c | <0.001 | <0.001 |
| Vegetable intake excluding kimchi and pickled vegetables | 2.52 ± 0.03 a | 3.28 ± 0.03 b | 3.82 ± 0.03 c | <0.001 | <0.001 |
| Meats/fishes/eggs/beans intake | 5.78 ± 0.07 a | 7.08 ± 0.05 b | 8.44 ± 0.04 c | <0.001 | <0.001 |
| Milk and dairy product intake | 1.80 ± 0.07 a | 2.88 ± 0.08 b | 5.23 ± 0.09 c | <0.001 | <0.001 |
| Moderation item | |||||
| Energy from saturated fatty acid | 5.78 ± 0.09 a | 7.97 ± 0.06 b | 8.74 ± 0.05 c | <0.001 | <0.001 |
| Sodium intake | 6.66 ± 0.07 a | 6.37 ± 0.06 b | 6.61 ± 0.06 a | <0.001 | <0.001 |
| Energy from sweets/beverages | 8.23 ± 0.06 a | 9.33 ± 0.03 b | 9.75 ± 0.02 c | <0.001 | <0.001 |
| Balance item | |||||
| Energy from carbohydrate | 1.52 ± 0.04 a | 2.49 ± 0.03 b | 3.41 ± 0.03 c | <0.001 | <0.001 |
| Energy from fat | 2.23 ± 0.04 a | 3.37 ± 0.03 b | 4.28 ± 0.03 c | <0.001 | <0.001 |
| Total energy intake | 2.13 ± 0.04 a | 3.15 ± 0.04 b | 3.93 ± 0.03 c | <0.001 | <0.001 |
| Diet Quality Level | |||||
|---|---|---|---|---|---|
| T1 (<58) (n = 4008) | T2 (58–69) (n = 4547) | T3 (≥70) (n = 4984) | p-Value | p Trend | |
| Protein, g | 70.53 ± 0.55 a | 73.93 ± 0.48 b | 77.85 ± 0.39 c | <0.001 | <0.001 |
| Fat, g | 54.83 ± 0.59 a | 43.82 ± 0.38 b | 44.04 ± 0.29 b | <0.001 | <0.001 |
| Saturated fatty acid, g | 18.03 ± 0.24 a | 13.35 ± 0.15 b | 13.03 ± 0.11 b | <0.001 | <0.001 |
| Monounsaturated fatty acid, g | 18.28 ± 0.25 a | 13.76 ± 0.15 b | 13.77 ± 0.12 b | <0.001 | <0.001 |
| Polyunsaturated fatty acid, g | 12.39 ± 0.18 a | 11.82 ± 0.13 b | 12.31 ± 0.12 a | 0.002 | 0.932 |
| n-3 fatty acid, g | 1.67 ± 0.03 a | 1.78 ± 0.03 b | 2.04 ± 0.03 c | <0.001 | <0.001 |
| n-6 fatty acid, g | 10.73 ± 0.16 a | 10.04 ± 0.11 b | 10.28 ± 0.10 b | 0.002 | 0.044 |
| Cholesterol, mg | 247.74 ± 4.38 a | 250.50 ± 3.41 a | 274.94 ± 3.71 b | <0.001 | <0.001 |
| Carbohydrate, g | 277.23 ± 1.90 a | 315.29 ± 1.27 b | 326.04 ± 1.11 c | <0.001 | <0.001 |
| Dietary fiber, g | 20.60 ± 0.20 a | 25.06 ± 0.21 b | 29.61 ± 0.22 c | <0.001 | <0.001 |
| Calcium, mg | 441.32 ± 5.01 a | 509.74 ± 4.91 b | 598.01 ± 5.57 c | <0.001 | <0.001 |
| Phosphate, mg | 991.31 ± 6.12 a | 1093.09 ± 5.45 b | 1222.82 ± 5.38 c | <0.001 | <0.001 |
| Iron, mg | 12.23 ± 0.15 a | 14.52 ± 0.34 b | 15.33 ± 0.17 b | <0.001 | <0.001 |
| Sodium, mg | 3789.46 ± 40.45 a | 3745.11 ± 35.71 a | 3438.90 ± 29.66 b | <0.001 | <0.001 |
| Potassium, mg | 2554.59 ± 18.78 a | 2977.19 ± 21.22 b | 3341.89 ± 18.65 c | <0.001 | <0.001 |
| Carotene, μg | 2636.90 ± 95.42 a | 3188.43 ± 87.47 b | 3628.35 ± 71.26 c | <0.001 | <0.001 |
| Retinol, μg | 147.38 ± 11.86 | 139.72 ± 11.06 | 159.36 ± 5.50 | 0.120 | 0.497 |
| Thiamin, mg | 1.48 ± 0.02 a | 1.60 ± 0.01 b | 1.70 ± 0.01 c | <0.001 | <0.001 |
| Riboflavin, mg | 1.50 ± 0.01 a | 1.53 ± 0.01 a | 1.69 ± 0.01 b | <0.001 | <0.001 |
| Niacin, mg | 14.15 ± 0.14 a | 14.83 ± 0.12 b | 15.70 ± 0.11 c | <0.001 | <0.001 |
| Vitamin C, mg | 55.67 ± 1.13 a | 75.12 ± 1.88 b | 94.70 ± 1.96 c | <0.001 | <0.001 |
| PHQ-9 Depression Severity | |||||
|---|---|---|---|---|---|
| Normal (n = 10,888) | Mild (n = 1905) | Moderate to Severe (n = 746) | p-Value | p Trend | |
| Waist circumference, cm | 82.30 ± 0.13 | 80.60 ± 0.30 | 81.89 ± 0.53 | 0.188 | 0.086 |
| Triglyceride, mg/dL | 136.27 ± 1.42 a | 138.08 ± 3.46 b | 148.44 ± 5.81 b | <0.001 | <0.001 |
| HDL-cholesterol, mg/dL | 50.92 ± 0.17 a | 51.59 ± 0.33 b | 51.51 ± 0.58 ab | 0.015 | 0.020 |
| Systolic blood pressure, mmHg | 117.52 ± 0.22 | 115.12 ± 0.47 | 117.23 ± 0.70 | 0.085 | 0.061 |
| Diastolic blood pressure, mmHg | 76.13 ± 0.14 a | 74.55 ± 0.30 b | 74.33 ± 0.47 b | 0.008 | 0.003 |
| Fasting blood glucose, mg/dL | 99.52 ± 0.26 | 98.15 ± 0.57 | 102.24 ± 1.35 | 0.066 | 0.026 |
| PHQ-9 Depression Severity | ||||
|---|---|---|---|---|
| Normal (n = 10,888) | Mild (n = 1905) | Moderate to Severe (n = 746) | p Trend | |
| Metabolic syndrome | 1 (Reference) | 1.01 (0.87–1.18) | 1.47 (1.17–1.86) ** | 0.006 |
| Abdominal obesity 1 | 1.13 (0.91–1.41) | 1.15 (0.84–1.16) | 0.201 | |
| Hypertriglyceridemia 2 | 1.14 (1.00–1.30) * | 1.30 (1.05–1.60) * | 0.003 | |
| Low HDL cholesterol 3 | 1.23 (1.08–1.39) ** | 1.22 (0.99–1.50) | 0.001 | |
| High blood pressure 4 | 0.84 (0.73–0.97) * | 0.89 (0.72–1.11) | 0.034 | |
| Hyperglycemia 5 | 0.95 (0.84–1.08) | 1.23 (1.00–1.50) * | 0.205 | |
| Diet Quality Levels | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 (<58) (n = 4008) | T2 (58–69) (n = 4547) | T3 (≥70) (n = 4984) | ||||||||||
| PHQ-9 Depression Severity | PHQ-9 Depression Severity | PHQ-9 Depression Severity | ||||||||||
| Normal (n = 3035) | Mild (n = 636) | Moderate to severe (n = 337) | p trend | Normal (n = 3655) | Mild (n = 670) | Moderate to severe (n = 222) | p trend | Normal (n = 4198) | Mild (n = 599) | Moderate to Severe (n = 187) | p trend | |
| Metabolic syndrome | 1 (Reference) | 0.98 (0.75–1.29) | 1.72 (1.24–2.40) ** | 0.009 | 1 (Reference) | 1.01 (0.79–1.31) | 1.18 (0.78–1.77) | 0.510 | 1 (Reference) | 1.08 (0.82–1.42) | 1.42 (0.90–2.25) | 0.145 |
| Abdominal obesity 1 | 1.16 (0.77–1.74) | 1.699 (1.04–2.81) * | 0.040 | 1.15 (0.80–1.64) | 0.78 (0.45–1.38) | 0.857 | 1.00 (0.68–1.47) | 0.93 (0.55–1.56) | 0.827 | |||
| Hypertriglyceridemia 2 | 1.04 (0.83–1.31) | 1.31 (0.96–1.78) | 0.123 | 1.16 (0.96–1.41) | 1.05 (0.74–1.48) | 0.310 | 1.28 (1.00–1.64) | 1.50 (1.00–2.26) | 0.010 | |||
| Low HDL cholesterol 3 | 1.35 (1.06–1.71) * | 1.51 (1.11–2.03) ** | <0.001 | 1.24 (1.01–1.52) * | 1.03 (0.71–1.49) | 0.219 | 1.10 (0.89–1.36) | 1.10 (0.76–1.61) | 0.361 | |||
| High blood pressure 4 | 0.80 (0.65–1.06) | 0.94 (0.67–1.30) | 0.328 | 0.89 (0.70–1.12) | 0.57 (0.41–0.80) * | 0.003 | 0.84 (0.66–1.07) | 1.35 (0.87–2.11) | 0.889 | |||
| Hyperglycemia 5 | 0.99 (0.79–1.25) | 1.05 (0.78–1.42) | 0.807 | 0.82 (0.66–1.02) | 1.46 (1.02–2.10) * | 0.513 | 0.80 (0.63–1.02) | 1.27 (0.81–1.99) | 0.264 | |||
| Metabolic Syndrome (Dependent Variable, Y) | |||
|---|---|---|---|
| Model 1 X -> Y | Model 2 X + M -> Y | Proportion of Mediation | |
| Depression severity (Independent Variable, X) | 1.47 (1.17–1.86) ** | 1.45 (1.15–1.84) ** | Fail to meet the conditions |
| Diet quality (Mediator, M) | 0.89 (0.77–1.02) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, I.S.; Hwang, J.-Y. Does Better Diet Quality Offset the Association between Depression and Metabolic Syndrome? Nutrients 2023, 15, 1060. https://doi.org/10.3390/nu15041060
Kim IS, Hwang J-Y. Does Better Diet Quality Offset the Association between Depression and Metabolic Syndrome? Nutrients. 2023; 15(4):1060. https://doi.org/10.3390/nu15041060
Chicago/Turabian StyleKim, In Seon, and Ji-Yun Hwang. 2023. "Does Better Diet Quality Offset the Association between Depression and Metabolic Syndrome?" Nutrients 15, no. 4: 1060. https://doi.org/10.3390/nu15041060
APA StyleKim, I. S., & Hwang, J.-Y. (2023). Does Better Diet Quality Offset the Association between Depression and Metabolic Syndrome? Nutrients, 15(4), 1060. https://doi.org/10.3390/nu15041060