

Dietary Flavonoid Intake and Cancer Mortality: A Population-Based Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Dietary Flavonoid Intake Assessment
2.2. Mortality Ascertainment
2.3. Covariate Assessment
2.4. Flavonoid Supplement Identification
2.5. Urinary Isoflavone Metabolite Assessment
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Flavonoid Intake
3.2. Baseline Characteristics of the Cohort
3.3. Dietary Flavonoid Intake
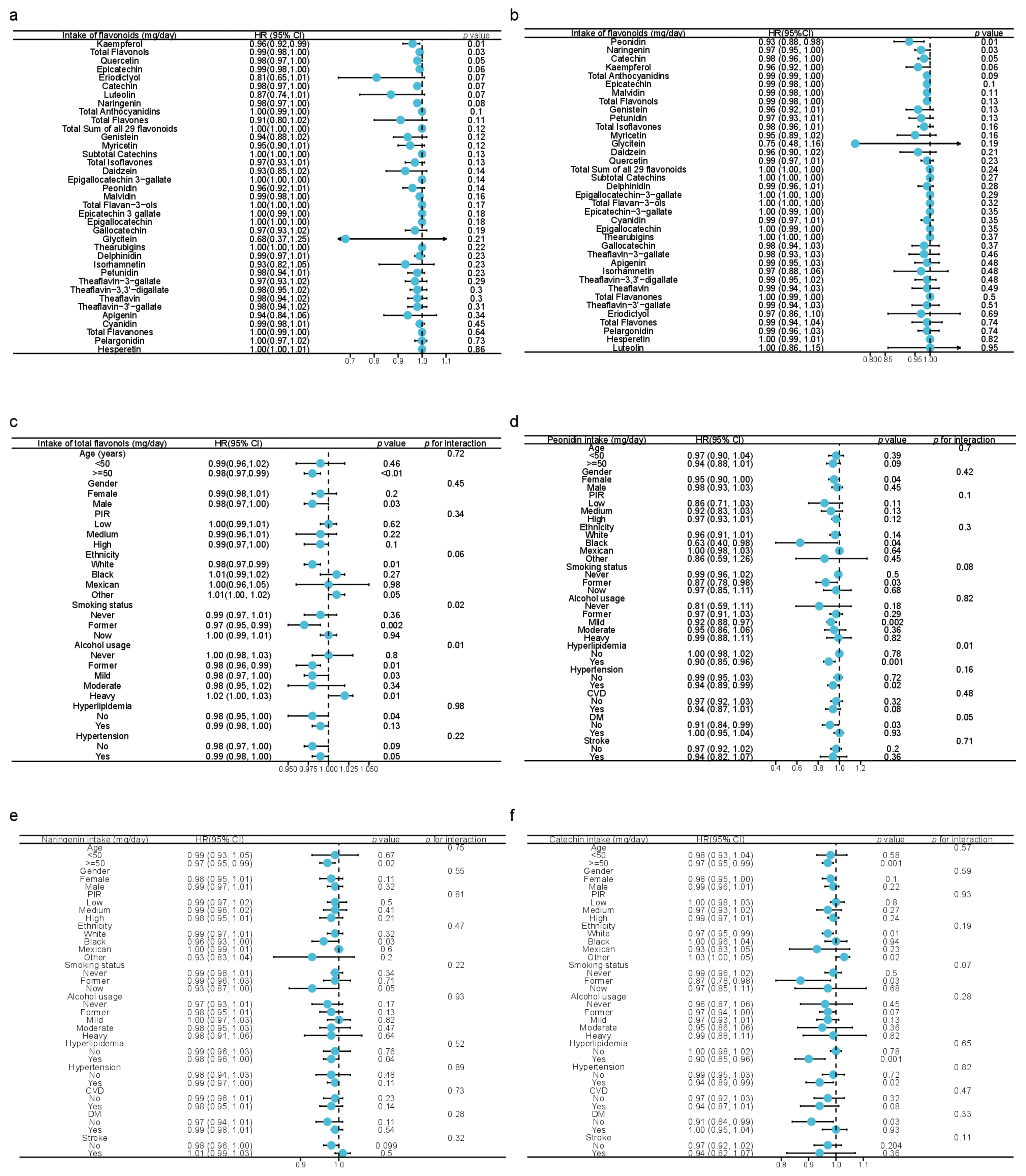
3.4. Associations between Dietary Flavonoid Intake and Cancer-Related Mortality
3.5. Establishment of Nomogram with Total Dietary Flavonol Intake
3.6. Associations between Isoflavone Metabolites in Urine and Cancer-Related Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Hosseinzadeh, E.; Hassanzadeh, A.; Marofi, F.; Alivand, M.R.; Solali, S. Flavonoid-Based Cancer Therapy: An Updated Review. Anticancer Agents Med. Chem. 2020, 20, 1398–1414. [Google Scholar] [CrossRef] [PubMed]
- Rothwell, J.A.; Knaze, V.; Zamora-Ros, R. Polyphenols: Dietary assessment and role in the prevention of cancers. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 512–521. [Google Scholar] [CrossRef] [PubMed]
- Le Marchand, L. Cancer preventive effects of flavonoids—A review. BioMed. Pharmacother. 2002, 56, 296–301. [Google Scholar] [CrossRef]
- Kuo, S.M. Dietary flavonoid and cancer prevention: Evidence and potential mechanism. Crit. Rev. Oncog. 1997, 8, 47–69. [Google Scholar] [CrossRef]
- Davatgaran-Taghipour, Y.; Masoomzadeh, S.; Farzaei, M.H.; Bahramsoltani, R.; Karimi-Soureh, Z.; Rahimi, R.; Abdollahi, M. Polyphenol nanoformulations for cancer therapy: Experimental evidence and clinical perspective. Int. J. Nanomed. 2017, 12, 2689–2702. [Google Scholar] [CrossRef] [Green Version]
- Abotaleb, M.; Samuel, S.M.; Varghese, E.; Varghese, S.; Kubatka, P.; Liskova, A.; Busselberg, D. Flavonoids in Cancer and Apoptosis. Cancers 2018, 11, 28. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.W.; Hu, J.J.; Fu, R.Q.; Liu, X.; Zhang, Y.H.; Li, J.; Liu, L.; Li, Y.N.; Deng, Q.; Luo, Q.S.; et al. Flavonoids inhibit cell proliferation and induce apoptosis and autophagy through downregulation of PI3Kgamma mediated PI3K/AKT/mTOR/p70S6K/ULK signaling pathway in human breast cancer cells. Sci. Rep. 2018, 8, 11255. [Google Scholar] [CrossRef] [Green Version]
- Masuelli, L.; Benvenuto, M.; Mattera, R.; Di Stefano, E.; Zago, E.; Taffera, G.; Tresoldi, I.; Giganti, M.G.; Frajese, G.V.; Berardi, G.; et al. In Vitro and In Vivo Anti-tumoral Effects of the Flavonoid Apigenin in Malignant Mesothelioma. Front. Pharmacol. 2017, 8, 373. [Google Scholar] [CrossRef] [Green Version]
- Hertog, M.G.; Feskens, E.J.; Hollman, P.C.; Katan, M.B.; Kromhout, D. Dietary flavonoids and cancer risk in the Zutphen Elderly Study. Nutr. Cancer 1994, 22, 175–184. [Google Scholar] [CrossRef] [Green Version]
- Hertog, M.G.; Kromhout, D.; Aravanis, C.; Blackburn, H.; Buzina, R.; Fidanza, F.; Giampaoli, S.; Jansen, A.; Menotti, A.; Nedeljkovic, S.; et al. Flavonoid intake and long-term risk of coronary heart disease and cancer in the seven countries study. Arch. Intern. Med. 1995, 155, 381–386. [Google Scholar] [CrossRef]
- Ivey, K.L.; Hodgson, J.M.; Croft, K.D.; Lewis, J.R.; Prince, R.L. Flavonoid intake and all-cause mortality. Am. J. Clin. Nutr. 2015, 101, 1012–1020. [Google Scholar] [CrossRef] [Green Version]
- Bondonno, N.P.; Dalgaard, F.; Kyro, C.; Murray, K.; Bondonno, C.P.; Lewis, J.R.; Croft, K.D.; Gislason, G.; Scalbert, A.; Cassidy, A.; et al. Flavonoid intake is associated with lower mortality in the Danish Diet Cancer and Health Cohort. Nat. Commun. 2019, 10, 3651. [Google Scholar] [CrossRef] [Green Version]
- Flavonoid Values for USDA Survey Foods and Beverages. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/fndds-flavonoid-database/ (accessed on 16 December 2022).
- About the National Health and Nutrition Examination Survey. Available online: https://www.cdc.gov/nchs/nhanes/about_nhanes.htm (accessed on 23 November 2022).
- NHANES Directors. Available online: https://www.cdc.gov/nchs/nhanes/directors.htm (accessed on 23 November 2022).
- NCHS Ethics Review Board (ERB) Approval. Available online: https://www.cdc.gov/nchs/nhanes/irba98.htm (accessed on 23 November 2022).
- NHANES Tutorials. Available online: https://wwwn.cdc.gov/nchs/nhanes/tutorials/default.aspx (accessed on 23 November 2022).
- USDA Special Interest Databases on Flavonoids. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/methods-and-application-of-food-composition-laboratory/mafcl-site-pages/flavonoids/ (accessed on 23 November 2022).
- FNDDS Documentation and Databases. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/fndds-download-databases/ (accessed on 23 November 2022).
- WWEIA Documentation and Data Sets. Available online: https://www.ars.usda.gov/northeast-area/beltsville-md-bhnrc/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/wweia-documentation-and-data-sets/ (accessed on 23 November 2022).
- Harnly, J.M.; Doherty, R.F.; Beecher, G.R.; Holden, J.M.; Haytowitz, D.B.; Bhagwat, S.; Gebhardt, S. Flavonoid content of U.S. fruits, vegetables, and nuts. J. Agric. Food Chem. 2006, 54, 9966–9977. [Google Scholar] [CrossRef]
- Rattan, P.; Penrice, D.D.; Ahn, J.C.; Ferrer, A.; Patnaik, M.; Shah, V.H.; Kamath, P.S.; Mangaonkar, A.A.; Simonetto, D.A. Inverse Association of Telomere Length With Liver Disease and Mortality in the US Population. Hepatol. Commun. 2022, 6, 399–410. [Google Scholar] [CrossRef]
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef] [Green Version]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hebert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [Green Version]
- National Health and Nutrition Examination Survey 2007–2008 Data Documentation, Codebook, and Frequencies Blood Pressure (BPX_E). Available online: https://wwwn.cdc.gov/Nchs/Nhanes/2007-2008/BPX_E.htm (accessed on 23 November 2022).
- Zhang, Z.; Kattan, M.W. Drawing Nomograms with R: Applications to categorical outcome and survival data. Ann. Transl. Med. 2017, 5, 211. [Google Scholar] [CrossRef] [Green Version]
- Fang, J. Classification of fruits based on anthocyanin types and relevance to their health effects. Nutrition 2015, 31, 1301–1306. [Google Scholar] [CrossRef]
- Wiseman, M. The second World Cancer Research Fund/American Institute for Cancer Research expert report. Food, nutrition, physical activity, and the prevention of cancer: A global perspective. Proc. Nutr. Soc. 2008, 67, 253–256. [Google Scholar] [CrossRef] [Green Version]
- Hirvonen, T.; Virtamo, J.; Korhonen, P.; Albanes, D.; Pietinen, P. Flavonol and flavone intake and the risk of cancer in male smokers (Finland). Cancer Causes Control. 2001, 12, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Imran, M.; Salehi, B.; Sharifi-Rad, J.; Aslam Gondal, T.; Saeed, F.; Imran, A.; Shahbaz, M.; Tsouh Fokou, P.V.; Umair Arshad, M.; Khan, H.; et al. Kaempferol: A Key Emphasis to Its Anticancer Potential. Molecules 2019, 24, 2277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, J.H.; An, J.Y.; Kwon, Y.T.; Rhee, J.G.; Lee, Y.J. Effects of low dose quercetin: Cancer cell-specific inhibition of cell cycle progression. J. Cell BioChem. 2009, 106, 73–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reyes-Farias, M.; Carrasco-Pozo, C. The Anti-Cancer Effect of Quercetin: Molecular Implications in Cancer Metabolism. Int. J. Mol. Sci. 2019, 20, 3177. [Google Scholar] [CrossRef] [Green Version]
- Ren, M.X.; Deng, X.H.; Ai, F.; Yuan, G.Y.; Song, H.Y. Effect of quercetin on the proliferation of the human ovarian cancer cell line SKOV-3 in vitro. Exp. Ther. Med. 2015, 10, 579–583. [Google Scholar] [CrossRef] [Green Version]
- Deng, X.H.; Song, H.Y.; Zhou, Y.F.; Yuan, G.Y.; Zheng, F.J. Effects of quercetin on the proliferation of breast cancer cells and expression of survivin in vitro. Exp. Ther. Med. 2013, 6, 1155–1158. [Google Scholar] [CrossRef] [Green Version]
- Afroze, N.; Pramodh, S.; Hussain, A.; Waleed, M.; Vakharia, K. A review on myricetin as a potential therapeutic candidate for cancer prevention. 3 Biotech 2020, 10, 211. [Google Scholar] [CrossRef]
- Barzegar, A. Antioxidant activity of polyphenolic myricetin in vitro cell- free and cell-based systems. Mol. Biol. Res. Commun. 2016, 5, 87–95. [Google Scholar]
- Zhang, C.; Zhang, G.; Liao, Y.; Gong, D. Myricetin inhibits the generation of superoxide anion by reduced form of xanthine oxidase. Food Chem. 2017, 221, 1569–1577. [Google Scholar] [CrossRef]
- Chen, H.; Lin, H.; Xie, S.; Huang, B.; Qian, Y.; Chen, K.; Niu, Y.; Shen, H.M.; Cai, J.; Li, P.; et al. Myricetin inhibits NLRP3 inflammasome activation via reduction of ROS-dependent ubiquitination of ASC and promotion of ROS-independent NLRP3 ubiquitination. Toxicol. Appl. Pharmacol. 2019, 365, 19–29. [Google Scholar] [CrossRef]
- Galati, G.; O’Brien, P.J. Potential toxicity of flavonoids and other dietary phenolics: Significance for their chemopreventive and anticancer properties. Free Radic. Biol. Med. 2004, 37, 287–303. [Google Scholar] [CrossRef]
- Skibola, C.F.; Smith, M.T. Potential health impacts of excessive flavonoid intake. Free Radic. Biol. Med. 2000, 29, 375–383. [Google Scholar] [CrossRef]
- Engen, A.; Maeda, J.; Wozniak, D.E.; Brents, C.A.; Bell, J.J.; Uesaka, M.; Aizawa, Y.; Kato, T.A. Induction of cytotoxic and genotoxic responses by natural and novel quercetin glycosides. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2015, 784–785, 15–22. [Google Scholar] [CrossRef]
- Gliszczynska-Swiglo, A.; van der Woude, H.; de Haan, L.; Tyrakowska, B.; Aarts, J.M.; Rietjens, I.M. The role of quinone reductase (NQO1) and quinone chemistry in quercetin cytotoxicity. Toxicol. Vitr. 2003, 17, 423–431. [Google Scholar] [CrossRef]
- Di Lorenzo, C.; Colombo, F.; Biella, S.; Stockley, C.; Restani, P. Polyphenols and Human Health: The Role of Bioavailability. Nutrients 2021, 13, 273. [Google Scholar] [CrossRef]
- Murota, K.; Nakamura, Y.; Uehara, M. Flavonoid metabolism: The interaction of metabolites and gut microbiota. BioSci. Biotechnol. BioChem. 2018, 82, 600–610. [Google Scholar] [CrossRef] [Green Version]
- Shabbir, U.; Rubab, M.; Daliri, E.B.; Chelliah, R.; Javed, A.; Oh, D.H. Curcumin, Quercetin, Catechins and Metabolic Diseases: The Role of Gut Microbiota. Nutrients 2021, 13, 206. [Google Scholar] [CrossRef]
- Couch, C.A.; Gray, M.S.; Shikany, J.M.; Howard, V.J.; Howard, G.; Long, D.L.; McClure, L.A.; Manly, J.J.; Cushman, M.; Zakai, N.A.; et al. Correlates of a southern diet pattern in a national cohort study of blacks and whites: The REasons for Geographic And Racial Differences in Stroke (REGARDS) study. Br. J. Nutr. 2021, 126, 1904–1910. [Google Scholar] [CrossRef]
- Li, B.; Robinson, D.H.; Birt, D.F. Evaluation of properties of apigenin and [G-3H] apigenin and analytic method development. J. Pharm. Sci. 1997, 86, 721–725. [Google Scholar] [CrossRef]
- Tang, D.; Chen, K.; Huang, L.; Li, J. Pharmacokinetic properties and drug interactions of apigenin, a natural flavone. Expert Opin. Drug Metab. Toxicol. 2017, 13, 323–330. [Google Scholar] [CrossRef]
- Heinonen, S.; Wahala, K.; Adlercreutz, H. Identification of isoflavone metabolites dihydrodaidzein, dihydrogenistein, 6′-OH-O-dma, and cis-4-OH-equol in human urine by gas chromatography-mass spectroscopy using authentic reference compounds. Anal. BioChem. 1999, 274, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Setchell, K.D.; Brown, N.M.; Lydeking-Olsen, E. The clinical importance of the metabolite equol-a clue to the effectiveness of soy and its isoflavones. J. Nutr. 2002, 132, 3577–3584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkinson, C.; Frankenfeld, C.L.; Lampe, J.W. Gut bacterial metabolism of the soy isoflavone daidzein: Exploring the relevance to human health. Exp. Biol. Med. 2005, 230, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.L.; Chen, P.N.; Chu, S.C.; Kuo, D.Y.; Kuo, W.H.; Chen, J.Y.; Hsieh, Y.S. Peonidin 3-glucoside inhibits lung cancer metastasis by downregulation of proteinases activities and MAPK pathway. Nutr. Cancer 2010, 62, 505–516. [Google Scholar] [CrossRef]
- Zeng, W.; Jin, L.; Zhang, F.; Zhang, C.; Liang, W. Naringenin as a potential immunomodulator in therapeutics. Pharmacol. Res. 2018, 135, 122–126. [Google Scholar] [CrossRef]
- Shirakami, Y.; Shimizu, M. Possible Mechanisms of Green Tea and Its Constituents against Cancer. Molecules 2018, 23, 2284. [Google Scholar] [CrossRef] [Green Version]
- Kent, K.; Charlton, K.E.; Lee, S.; Mond, J.; Russell, J.; Mitchell, P.; Flood, V.M. Dietary flavonoid intake in older adults: How many days of dietary assessment are required and what is the impact of seasonality? Nutr. J. 2018, 17, 7. [Google Scholar] [CrossRef] [Green Version]
- Jiang, C.K.; Ni, D.J.; Yao, M.Z. Metabolic and transcriptome analysis reveals metabolite variation and flavonoid regulatory networks in fresh shoots of tea (Camellia sinensis) over three seasons. Front. Agr. Sci. Eng. 2021, 8, 215–230. [Google Scholar] [CrossRef]
- National Health and Nutrition Examination Survey 1999–2020 Data Documentation, Codebook, and Frequencies Dietary Supplement Database - Product Information (DSPI). Available online: https://wwwn.cdc.gov/Nchs/Nhanes/1999-2000/DSPI.htm#Appendix_1:_Rules_for_Classifying_Ingredients (accessed on 17 December 2022).




{kind=link}
{kind=link}
{kind=link}
| Intake of Flavonoids (mg/day) | Minimum | 25th Percentile | Median | Mean | 75th Percentile | Maximum |
|---|---|---|---|---|---|---|
| Daidzein | 0 | 0 | 0 | 0.6919 | 0.025 | 151 |
| Genistein | 0 | 0 | 0.01 | 0.9426 | 0.045 | 204.32 |
| Glycitein | 0 | 0 | 0 | 0.1341 | 0 | 35.28 |
| Cyanidin | 0 | 0.045 | 0.515 | 2.447 | 1.885 | 639.96 |
| Petunidin | 0 | 0 | 0 | 0.9845 | 0.37 | 144.4 |
| Delphinidin | 0 | 0 | 0.01 | 1.4 | 0.66 | 187.14 |
| Malvidin | 0 | 0 | 0 | 4.258 | 1.81 | 309.485 |
| Pelargonidin | 0 | 0 | 0.01 | 1.427 | 0.35 | 91.135 |
| Peonidin | 0 | 0 | 0.095 | 1.705 | 0.66 | 636.765 |
| Catechin | 0 | 1.825 | 5.025 | 7.224 | 9.8 | 166.845 |
| Epigallocatechin | 0 | 0.105 | 0.485 | 14.408 | 13.825 | 1083.675 |
| Epicatechin | 0 | 1.375 | 5.68 | 9.232 | 12.71 | 316.94 |
| Epicatechin 3-gallate | 0 | 0 | 0.02 | 9.294 | 8.895 | 666.03 |
| Epigallocatechin 3-gallate | 0 | 0 | 0.14 | 24.98 | 21.93 | 2606.33 |
| Theaflavin | 0 | 0 | 0 | 1.354 | 0.845 | 75.87 |
| Thearubigins | 0 | 0 | 0 | 78.11 | 73.62 | 3891 |
| Eriodictyol | 0 | 0 | 0 | 0.196 | 0.095 | 47 |
| Hesperetin | 0 | 0 | 0.135 | 9.818 | 12.695 | 509.42 |
| Naringenin | 0 | 0.035 | 0.305 | 3.708 | 3.49 | 224.35 |
| Apigenin | 0 | 0.015 | 0.065 | 0.1953 | 0.21 | 70.01 |
| Luteolin | 0 | 0.115 | 0.355 | 0.6633 | 0.85 | 43.305 |
| Isorhamnetin | 0 | 0.13 | 0.46 | 0.8339 | 1.045 | 75.155 |
| Kaempferol | 0 | 0.895 | 2.325 | 4.207 | 5.485 | 152.885 |
| Myricetin | 0 | 0.245 | 0.6 | 1.373 | 1.625 | 39.645 |
| Quercetin | 0 | 4.32 | 8.09 | 10.65 | 13.9 | 202.75 |
| Theaflavin-3,3’-digallate | 0 | 0 | 0 | 1.493 | 0.94 | 83.66 |
| Theaflavin-3’-gallate | 0 | 0 | 0 | 1.264 | 0.605 | 72.18 |
| Theaflavin-3-gallate | 0 | 0 | 0 | 1.074 | 0.74 | 59.67 |
| Gallocatechin | 0 | 0 | 0.02 | 1.466 | 1.42 | 73.66 |
| Subtotal Catechins | 0 | 4.78 | 14.49 | 66.6 | 63.83 | 4897.1 |
| Total Isoflavones | 0 | 0 | 0.01 | 1.768 | 0.08 | 390.6 |
| Total Anthocyanidins | 0 | 0.11 | 2.02 | 12.22 | 10.78 | 756.1 |
| Total Flavan-3-ols | 0 | 4.915 | 15.425 | 149.891 | 154.295 | 6724.88 |
| Total Flavanones | 0 | 0.055 | 0.61 | 13.722 | 18.925 | 590.625 |
| Total Flavones | 0 | 0.18 | 0.505 | 0.8586 | 1.085 | 87.245 |
| Total Flavonols | 0 | 6.815 | 12.555 | 17.064 | 22.105 | 332.035 |
| Total Sum of all 29 flavonoids | 0 | 24.31 | 64.05 | 195.53 | 217.38 | 6974.47 |
| Variable | Alive (n = 13,624) | Death Caused by Cancer (n = 405) | p Value |
|---|---|---|---|
| Baseline sociodemographic, lifestyle, and health-related variables | |||
| Age, years | 46.67 ± 0.32 | 65.93 ± 0.89 | <0.0001 |
| Gender, % | 0.01 | ||
| Female | 52.86% (51.76%, 53.96%) | 42.70% (36.11%, 49.29%) | |
| Male | 47.14% (46.04%, 48.24%) | 57.30% (50.71%, 63.89%) | |
| Ethnicity, % | 0.002 | ||
| Black | 11.41% (9.61%, 13.21%) | 12.15% (8.61%, 15.69%) | |
| Mexican | 8.74% (6.73%, 10.74%) | 3.32% (1.03%, 5.60%) | |
| Other | 13.14% (11.21%, 15.08%) | 6.82% (2.37%, 11.27%) | |
| White | 66.71% (63.01%, 70.40%) | 77.71% (70.94%, 84.48%) | |
| Education, % | <0.0001 | ||
| <9 years | 4.89% (4.16%, 5.61%) | 10.18% (6.45%, 13.92%) | |
| 9−12 years | 35.37% (33.30%, 37.44%) | 45.38% (39.66%, 51.10%) | |
| >12 years | 59.74% (57.48%, 62.00%) | 44.44% (37.76%, 51.11%) | |
| Marital status, % | 0.67 | ||
| Without partner | 37.08% (35.23%, 38.93%) | 38.69% (31.22%, 46.15%) | |
| With partner | 62.92% (61.07%, 64.77%) | 61.31% (53.85%, 68.78%) | |
| PIR | 3.02 ± 0.04 | 2.65 ± 0.15 | 0.02 |
| BMI (kg/m2) | 29.14 ± 0.13 | 29.04 ± 0.52 | 0.84 |
| Daily energy intake (kcal) | 4161.93 ± 27.93 | 3828.29 ± 112.64 | 0.01 |
| Total score of HEI | 53.25 ± 0.36 | 54.40 ± 0.97 | 0.23 |
| DII | 1.47 ± 0.05 | 1.77 ± 0.12 | 0.02 |
| Total time of PA (mins/week) | 1288.52 ± 29.66 | 1244.04 ± 166.92 | 0.79 |
| Total MET of PA (/week) | 5124.83 ± 137.52 | 4375.36 ± 681.03 | 0.28 |
| Smoking status, % | <0.0001 | ||
| Never | 56.97% (54.88%, 59.05%) | 35.95% (27.82%, 44.09%) | |
| Former | 24.20% (22.87%, 25.53%) | 36.55% (28.37%, 44.73%) | |
| Now | 18.8%3 (17.43%, 20.23%) | 27.50% (19.33%, 35.66%) | |
| Alcohol consumption, % | <0.0001 | ||
| Never | 10.72% (9.76%, 11.68%) | 9.02% (4.87%, 13.17%) | |
| Former | 10.65% (9.35%, 11.94%) | 36.13% (28.06%, 44.20%) | |
| Mild | 38.38% (36.43%, 40.33%) | 31.86% (23.67%, 40.06%) | |
| Moderate | 18.17% (17.08%, 19.26%) | 12.68% (8.19%, 17.17%) | |
| Heavy | 22.08% (20.72%, 23.44%) | 10.31% (4.79%, 15.84%) | |
| Dietary intake of flavonoids (mg/day) | |||
| Daidzein | 0.80 ± 0.06 | 0.37 ± 0.12 | <0.001 |
| Genistein | 1.13 ± 0.08 | 0.46 ± 0.15 | <0.001 |
| Glycitein | 0.16 ± 0.01 | 0.06 ± 0.02 | <0.001 |
| Cyanidin | 2.69 ± 0.19 | 2.17 ± 0.32 | 0.2 |
| Petunidin | 1.20 ± 0.09 | 0.83 ± 0.16 | 0.03 |
| Delphinidin | 1.72 ± 0.14 | 1.22 ± 0.21 | 0.03 |
| Malvidin | 4.92 ± 0.31 | 3.59 ± 0.60 | 0.04 |
| Pelargonidin | 1.64 ± 0.12 | 1.53 ± 0.36 | 0.72 |
| Peonidin | 2.12 ± 0.16 | 0.87 ± 0.21 | <0.0001 |
| Catechin | 7.83 ± 0.18 | 6.95 ± 0.50 | 0.07 |
| Epigallocatechin | 16.76 ± 0.81 | 13.72 ± 1.89 | 0.13 |
| Epicatechin | 10.13 ± 0.24 | 8.73 ± 0.66 | 0.04 |
| Epicatechin 3-gallate | 10.81 ± 0.53 | 8.88 ± 1.28 | 0.15 |
| Epigallocatechin 3-gallate | 28.90 ± 1.65 | 23.03 ± 3.19 | 0.09 |
| Theaflavin | 1.59 ± 0.08 | 1.39 ± 0.22 | 0.39 |
| Thearubigins | 90.86 ± 4.36 | 79.31 ± 11.27 | 0.32 |
| Eriodictyol | 0.17 ± 0.01 | 0.14 ± 0.02 | 0.12 |
| Hesperetin | 8.86 ± 0.26 | 9.77 ± 1.08 | 0.42 |
| Naringenin | 3.40 ± 0.16 | 2.62 ± 0.36 | 0.04 |
| Apigenin | 0.24 ± 0.03 | 0.21 ± 0.02 | 0.34 |
| Luteolin | 0.71 ± 0.02 | 0.59 ± 0.05 | 0.02 |
| Isorhamnetin | 0.86 ± 0.02 | 0.77 ± 0.07 | 0.17 |
| Kaempferol | 4.67 ± 0.10 | 3.59 ± 0.33 | 0.002 |
| Myricetin | 1.54 ± 0.04 | 1.31 ± 0.11 | 0.04 |
| Quercetin | 11.38 ± 0.19 | 10.31 ± 0.65 | 0.09 |
| Theaflavin-3,3′-digallate | 1.75 ± 0.09 | 1.54 ± 0.24 | 0.39 |
| Theaflavin-3′-gallate | 1.48 ± 0.08 | 1.30 ± 0.21 | 0.4 |
| Theaflavin-3-gallate | 1.26 ± 0.06 | 1.11 ± 0.17 | 0.41 |
| Gallocatechin | 1.71 ± 0.07 | 1.43 ± 0.22 | 0.21 |
| Subtotal Catechins | 76.14 ± 3.36 | 62.75 ± 7.34 | 0.09 |
| Total Isoflavones | 2.09 ± 0.15 | 0.89 ± 0.29 | <0.001 |
| Total Anthocyanidins | 14.30 ± 0.74 | 10.21 ± 1.40 | 0.01 |
| Total Flavan-3-ols | 173.08 ± 7.19 | 147.41 ± 19.38 | 0.2 |
| Total Flavanones | 12.43 ± 0.39 | 12.53 ± 1.34 | 0.95 |
| Total Flavones | 0.95 ± 0.04 | 0.80 ± 0.06 | 0.03 |
| Total Flavonols | 18.45 ± 0.32 | 15.97 ± 1.07 | 0.02 |
| Total Sum of all 29 flavonoids | 221.30 ± 7.48 | 187.80 ± 20.34 | 0.11 |
| Disease history at interview | |||
| DM, % | <0.0001 | ||
| No | 79.30% (77.90%, 80.70%) | 61.21% (54.12%, 68.31%) | |
| Yes | 20.70% (19.30%, 22.10%) | 38.79% (31.69%, 45.88%) | |
| Hyperlipidemia, % | 0.12 | ||
| No | 31.43% (29.70%, 33.17%) | 25.08% (17.66%, 32.50%) | |
| Yes | 68.57% (66.83%, 70.30%) | 74.92% (67.50%, 82.34%) | |
| CVD, % | <0.0001 | ||
| No | 91.48% (90.62%, 92.34%) | 65.84% (59.01%, 72.66%) | |
| Yes | 8.52% (7.66%, 9.38%) | 34.16% (27.34%, 40.99%) | |
| Respiratory system disease, % | <0.0001 | ||
| ACO | 2.06% (1.70%, 2.42%) | 8.06% (1.88%, 14.23%) | |
| Asthma | 11.70% (10.75%, 12.64%) | 7.62% (4.20%, 11.03%) | |
| COPD | 2.83% (2.33%, 3.32%) | 15.46% (9.30%, 21.63%) | |
| No | 83.42% (82.16%, 84.68%) | 68.86% (61.16%, 76.56%) | |
| Stroke, % | <0.0001 | ||
| No | 96.86% (96.50%, 97.21%) | 84.35% (78.74%, 89.97%) | |
| Yes | 3.14% (2.79%, 3.50%) | 15.65% (10.03%, 21.26%) | |
| Cancer, % | <0.001 | ||
| No | 90.33% (89.67%, 90.98%) | 80.53% (74.37%, 86.68%) | |
| Yes | 9.67% (9.02%, 10.33%) | 19.47% (13.32%, 25.63%) | |
| Hypertension, % | <0.0001 | ||
| No | 63.80% (62.09%, 65.51%) | 26.20% (19.40%, 32.99%) | |
| Yes | 36.20% (34.49%, 37.91%) | 73.80% (67.01%, 80.60%) | |
| 2007–2008 | 2009–2010 | 2017–2018 | p-Value | |
|---|---|---|---|---|
| Dietary intake of flavonoids (mg/day) | ||||
| Daidzein | 0.62 ± 0.08 | 0.79 ± 0.05 | 0.93 ± 0.13 | 0.09 |
| Genistein | 0.84 ± 0.10 | 1.12 ± 0.07 | 1.36 ± 0.19 | 0.02 |
| Glycitein | 0.11 ± 0.01 | 0.16 ± 0.01 | 0.21 ± 0.03 | 0.01 |
| Cyanidin | 2.22 ± 0.19 | 2.99 ± 0.25 | 2.82 ± 0.42 | 0.04 |
| Petunidin | 0.77 ± 0.10 | 1.38 ± 0.18 | 1.40 ± 0.17 | 0.001 |
| Delphinidin | 1.04 ± 0.13 | 2.10 ± 0.29 | 1.96 ± 0.24 | <0.001 |
| Malvidin | 4.05 ± 0.46 | 5.23 ± 0.47 | 5.36 ± 0.56 | 0.11 |
| Pelargonidin | 1.44 ± 0.21 | 1.88 ± 0.25 | 1.60 ± 0.16 | 0.36 |
| Peonidin | 1.23 ± 0.12 | 2.11 ± 0.30 | 2.85 ± 0.32 | <0.0001 |
| Catechin | 7.71 ± 0.32 | 8.18 ± 0.24 | 7.58 ± 0.33 | 0.26 |
| Epigallocatechin | 17.41 ± 1.11 | 15.93 ± 1.30 | 16.76 ± 1.57 | 0.66 |
| Epicatechin | 10.24 ± 0.41 | 10.13 ± 0.37 | 9.97 ± 0.41 | 0.9 |
| Epicatechin 3-gallate | 11.50 ± 0.74 | 10.44 ± 0.88 | 10.41 ± 0.98 | 0.53 |
| Epigallocatechin 3-gallate | 30.12 ± 1.90 | 27.50 ± 2.25 | 28.75 ± 3.60 | 0.64 |
| Theaflavin | 1.77 ± 0.12 | 1.59 ± 0.14 | 1.41 ± 0.15 | 0.22 |
| Thearubigins | 101.89 ± 6.79 | 91.63 ± 8.00 | 79.87 ± 7.67 | 0.14 |
| Eriodictyol | 0.19 ± 0.01 | 0.20 ± 0.01 | 0.14 ± 0.01 | 0.004 |
| Hesperetin | 9.55 ± 0.61 | 10.05 ± 0.35 | 7.24 ± 0.35 | <0.0001 |
| Naringenin | 3.52 ± 0.29 | 3.40 ± 0.20 | 3.26 ± 0.30 | 0.82 |
| Apigenin | 0.23 ± 0.03 | 0.31 ± 0.07 | 0.17 ± 0.01 | 0.03 |
| Luteolin | 0.64 ± 0.04 | 0.74 ± 0.03 | 0.74 ± 0.04 | 0.11 |
| Isorhamnetin | 0.80 ± 0.04 | 0.90 ± 0.03 | 0.87 ± 0.03 | 0.08 |
| Kaempferol | 4.55 ± 0.19 | 4.64 ± 0.16 | 4.74 ± 0.12 | 0.7 |
| Myricetin | 1.51 ± 0.07 | 1.46 ± 0.08 | 1.64 ± 0.07 | 0.23 |
| Quercetin | 11.70 ± 0.41 | 11.91 ± 0.30 | 10.58 ± 0.24 | 0.004 |
| Theaflavin-3,3′-digallate | 1.96 ± 0.14 | 1.76 ± 0.16 | 1.55 ± 0.17 | 0.2 |
| Theaflavin-3′-gallate | 1.66 ± 0.12 | 1.49 ± 0.13 | 1.32 ± 0.14 | 0.23 |
| Theaflavin-3-gallate | 1.42 ± 0.10 | 1.27 ± 0.12 | 1.10 ± 0.12 | 0.17 |
| Gallocatechin | 1.87 ± 0.12 | 1.71 ± 0.14 | 1.55 ± 0.12 | 0.23 |
| Subtotal Catechins | 78.85 ± 4.38 | 73.90 ± 5.11 | 75.03 ± 6.76 | 0.72 |
| Total Isoflavones | 1.58 ± 0.19 | 2.06 ± 0.13 | 2.50 ± 0.34 | 0.04 |
| Total Anthocyanidins | 10.74 ± 0.91 | 15.68 ± 1.09 | 15.99 ± 1.48 | <0.001 |
| Total Flavan-3-ols | 187.55 ± 11.60 | 171.63 ± 13.66 | 160.28 ± 11.43 | 0.27 |
| Total Flavanones | 13.26 ± 0.87 | 13.65 ± 0.52 | 10.64 ± 0.58 | 0.001 |
| Total Flavones | 0.87 ± 0.05 | 1.05 ± 0.08 | 0.91 ± 0.04 | 0.18 |
| Total Flavonols | 18.56 ± 0.68 | 18.92 ± 0.52 | 17.82 ± 0.40 | 0.26 |
| Total Sum of all 29 flavonoids | 232.55 ± 12.43 | 222.98 ± 14.09 | 208.13 ± 11.66 | 0.39 |
| Baseline sociodemographic, lifestyle, and health-related variables | ||||
| Age, years | 46.85 ± 0.47 | 46.96 ± 0.51 | 47.29 ± 0.55 | 0.82 |
| Gender, % | 0.41 | |||
| Female | 53.69% (51.99%, 55.40%) | 52.22% (51.03%, 53.40%) | 52.15% (49.83%, 54.47%) | |
| Male | 46.31% (44.60%, 48.01%) | 47.78% (46.60%, 48.97%) | 47.85% (45.53%, 50.17%) | |
| Ethnicity, % | 0.16 | |||
| Black | 11.15% (7.55%, 14.75%) | 11.49% (9.76%, 13.23%) | 11.61% (8.35%, 14.87%) | |
| Mexican | 8.39% (5.63%, 11.16%) | 8.32% (4.51%, 12.13%) | 9.12% (5.80%, 12.44%) | |
| Other | 9.91% (6.71%, 13.10%) | 11.56% (8.05%, 15.08%) | 17.06% (14.12%, 19.99%) | |
| White | 70.55% (64.29%, 76.80%) | 68.62% (62.27%, 74.97%) | 62.22% (56.62%, 67.82%) | |
| Education, % | 0.002 | |||
| <9 years | 6.29% (4.87%, 7.71%) | 5.84% (4.53%, 7.15%) | 3.03% (2.14%, 3.92%) | |
| 9–12 years | 38.37% (34.35%, 42.38%) | 34.87% (32.08%, 37.67%) | 33.65% (30.25%, 37.04%) | |
| >12 years | 55.34% (50.57%, 60.11%) | 59.29% (56.52%, 62.05%) | 63.32% (59.82%, 66.83%) | |
| Marital status, % | 0.81 | |||
| Without partner | 37.71% (33.75%, 41.68%) | 36.42% (34.30%, 38.54%) | 37.20% (34.42%, 39.98%) | |
| With partner | 62.29% (58.32%, 66.25%) | 63.58% (61.46%, 65.70%) | 62.80% (60.02%, 65.58%) | |
| PIR | 3.01 ± 0.09 | 2.96 ± 0.05 | 3.06 ± 0.06 | 0.47 |
| BMI (kg/m2) | 28.74 ± 0.20 | 28.83 ± 0.13 | 29.77 ± 0.28 | 0.01 |
| Daily energy intake (kcal) | 4120.26 ± 52.88 | 4207.67 ± 44.41 | 4140.31 ± 43.02 | 0.36 |
| Total Score of HEI | 53.09 ± 0.65 | 54.30 ± 0.36 | 52.52 ± 0.71 | 0.04 |
| DII | 1.65 ± 0.10 | 1.33 ± 0.04 | 1.45 ± 0.09 | 0.004 |
| Total time of PA (mins/week) | 1274.92 ± 50.84 | 1102.61 ± 33.04 | 1463.02 ± 60.66 | <0.0001 |
| Total MET of PA (/week) | 5094.71 ± 230.20 | 4243.83 ± 171.63 | 5870.06 ± 274.40 | <0.0001 |
| Smoking status, % | 0.01 | |||
| Never | 53.62% (50.24%, 57.00%) | 55.61% (51.57%, 59.66%) | 59.99% (56.97%, 63.01%) | |
| Former | 24.11% (22.33%, 25.89%) | 25.11% (22.18%, 28.04%) | 24.13% (22.21%, 26.05%) | |
| Now | 22.27% (19.75%, 24.79%) | 19.27% (17.31%, 21.24%) | 15.88% (13.51%, 18.25%) | |
| Alcohol usage, % | <0.0001 | |||
| Never | 11.56% (9.94%, 13.17%) | 10.87% (9.09%, 12.65%) | 9.62% (8.28%, 10.96%) | |
| Former | 17.53% (14.56, 20.50) | 15.21% (13.27%, 17.15%) | 0.65% (0.33%, 0.98%) | |
| Mild | 34.23% (30.60, 37.85) | 35.69% (32.90%, 38.47%) | 44.89% (41.47%, 48.31%) | |
| Moderate | 15.60% (13.66, 17.54) | 16.65% (14.58%, 18.72%) | 21.97% (20.55%, 23.39%) | |
| Heavy | 21.09% (19.46, 22.71) | 21.59% (19.12%, 24.05%) | 22.87% (20.11%, 25.63%) | |
| Disease history at interview | ||||
| DM, % | 0.45 | |||
| No | 78.14% (75.37%, 80.90%) | 80.15% (78.17%, 82.13%) | 78.61% (76.44%, 80.79%) | |
| Yes | 21.86% (19.10%, 24.63%) | 19.85% (17.87%, 21.83%) | 21.39% (19.21%, 23.56%) | |
| Hyperlipidemia, % | 0.002 | |||
| No | 28.37% (25.98%, 30.76%) | 29.88% (28.12%, 31.64%) | 35.17% (31.50%, 38.83%) | |
| Yes | 71.63% (69.24%, 74.02%) | 70.12% (68.36%, 71.88%) | 64.83% (61.17%, 68.50%) | |
| CVD, % | 0.96 | |||
| No | 91.06% (90.00%, 92.12%) | 91.06% (89.71%, 92.41%) | 90.84% (89.16%, 92.53%) | |
| Yes | 8.94% (7.88%, 10.00%) | 8.94% (7.59%, 10.29%) | 9.16% (7.47%, 10.84%) | |
| Respiratory system disease, % | <0.0001 | |||
| ACO | 2.58% (2.05%, 3.11%) | 2.11% (1.57%, 2.65%) | 1.87% (1.07%, 2.66%) | |
| Asthma | 11.83% (9.90%, 13.75%) | 10.14% (9.25%, 11.04%) | 12.78% (11.05%, 14.51%) | |
| COPD | 4.39% (3.46%, 5.33%) | 3.81% (2.65%, 4.98%) | 1.19% (0.80%, 1.58%) | |
| No | 81.20% (78.58%, 83.82%) | 83.94% (82.45%, 85.42%) | 84.16% (81.87%, 86.44%) | |
| Stroke, % | 0.49 | |||
| No | 96.30% (95.59%, 97.00%) | 96.83% (96.33%, 97.34%) | 96.70% (95.99%, 97.40%) | |
| Yes | 3.70% (3.00%, 4.41%) | 3.17% (2.66%, 3.67%) | 3.30% (2.60%, 4.01%) | |
| Cancer, % | 0.46 | |||
| No | 90.69% (89.63%, 91.75%) | 90.06% (88.86%, 91.26%) | 89.70% (88.56%, 90.83%) | |
| Yes | 9.31% (8.25%, 10.37%) | 9.94% (8.74%, 11.14%) | 10.30% (9.17%, 11.44%) | |
| Hypertension, % | 0.18 | |||
| No | 63.63% (61.50%, 65.76%) | 64.67% (61.79%, 67.55%) | 61.19% (58.00%, 64.38%) | |
| Yes | 36.37% (34.24%, 38.50%) | 35.33% (32.45%, 38.21%) | 38.81% (35.62%, 42.00%) | |
| Age and Gender Group | Case, n | Subtotal Catechins (mg/day) | Total Isoflavones(mg/day) | Total Anthocyanidins (mg/day) | Total Flavan-3-ols (mg/day) | Total Flavanones (mg/day) | Total Flavones (mg/day) | Total Flavonols (mg/day) | Total Sum of All 29 Flavonoids (mg/day) |
|---|---|---|---|---|---|---|---|---|---|
| White | |||||||||
| All | 6361 | 84.12 (74.74, 93.50) | 2.05 (1.66, 2.45) | 16.12 (13.98, 18.25) | 195.74 (176.20, 215.28) | 11.21 (10.38, 12.04) | 0.99 (0.89, 1.09) | 19.45 (18.51, 20.39) | 245.56 (225.09, 266.04) |
| male < 50 | 1299 | 82.42 (66.25, 98.60) | 2.56 (1.94, 3.19) | 11.28 (8.22, 14.34) | 186.79 (154.01, 219.57) | 11.03 (9.01, 13.06) | 1.02 (0.78, 1.26) | 20.55 (18.87, 22.23) | 233.23 (199.48, 266.98) |
| female < 50 | 1458 | 76.74 (63.04, 90.44) | 1.91 (1.13, 2.68) | 14.93 (12.46, 17.40) | 179.59 (151.12, 208.05) | 7.68 (6.53, 8.83) | 0.82 (0.72, 0.91) | 17.06 (15.66, 18.45) | 221.98 (191.88, 252.07) |
| male ≧ 50 | 1825 | 82.98 (71.91, 94.04) | 1.77 (0.97, 2.56) | 18.09 (14.71, 21.47) | 200.97 (171.61, 230.34) | 14.05 (12.33, 15.77) | 1.10 (0.95, 1.25) | 20.89 (19.63, 22.15) | 256.88 (226.01, 287.74) |
| female ≧ 50 | 1779 | 94.01 (71.62, 116.40) | 1.98 (1.42, 2.53) | 20.05 (17.08, 23.01) | 215.48 (184.48, 246.49) | 12.41 (10.83, 13.99) | 1.05 (0.82, 1.27) | 19.54 (18.15, 20.94) | 270.51 (238.49, 302.52) |
| Black | |||||||||
| All | 2904 | 51.92 (46.67, 57.17) | 1.43 (1.00, 1.86) | 8.27 (7.07, 9.48) | 118.85 (105.57, 132.13) | 14.17 (12.79, 15.54) | 0.60 (0.56, 0.64) | 14.53 (13.83, 15.23) | 157.85 (144.43, 171.26) |
| male < 50 | 618 | 52.30 (44.65, 59.94) *** | 2.24 (0.79, 3.69) | 8.16 (6.15, 10.17) *** | 118.94 (100.24, 137.64) *** | 15.47 (12.65, 18.30) *** | 0.54 (0.49, 0.60) *** | 15.78 (14.40, 17.17) *** | 161.14 (140.57, 181.70) *** |
| female < 50 | 767 | 46.39 (38.01, 54.77) *** | 1.14 (0.52, 1.76) * | 7.40 (6.21, 8.58) *** | 102.25 (80.69, 123.82) *** | 14.12 (11.87, 16.37) *** | 0.61 (0.52, 0.69) *** | 12.78 (11.78, 13.78) *** | 138.30 (115.47, 161.12) *** |
| male ≧ 50 | 745 | 56.95 (44.95, 68.96) *** | 0.98 (0.51, 1.44) | 8.19 (6.37, 10.00) *** | 140.29 (107.30, 173.28) *** | 14.44 (12.08, 16.80) | 0.63 (0.54, 0.71) *** | 16.81 (15.31, 18.32) *** | 181.34 (147.20, 215.48) *** |
| female ≧ 50 | 774 | 56.46 (47.39, 65.54) *** | 1.19 (0.53, 1.85) *** | 9.92 (6.79, 13.05) *** | 128.77 (112.63, 144.91) *** | 12.30 (10.07, 14.53) * | 0.64 (0.57, 0.72) *** | 13.91 (12.84, 14.99) *** | 166.74 (148.28, 185.20) *** |
| Mexican | |||||||||
| All | 2222 | 45.48 (38.26, 52.70) | 2.23 (0.83, 3.63) | 8.60 (6.74, 10.47) | 89.90 (72.66, 107.13) | 16.16 (14.43, 17.89) | 0.97 (0.88, 1.06) | 15.41 (14.55, 16.27) | 133.27 (115.85, 150.69) |
| male < 50 | 596 | 48.62 (40.34, 56.90) *** | 1.97 (0.30, 3.64) | 7.18 (4.50, 9.87) *** | 85.23 (67.11, 103.35) *** | 17.85 (15.02, 20.68) *** | 0.98 (0.86, 1.11) | 16.94 (15.57, 18.32) *** | 130.16 (110.49, 149.84) *** |
| female < 50 | 681 | 41.91 (31.21, 52.61) *** | 3.47 (−0.12, 7.06) | 8.01 (6.01, 10.02) *** | 89.48 (65.06, 113.89) *** | 14.05 (11.88, 16.23) *** | 0.90 (0.76, 1.05) | 13.93 (12.63, 15.24) *** | 129.85 (104.53, 155.16) ** |
| male ≧ 50 | 442 | 48.55 (30.97, 66.12) *** | 0.96 (0.37, 1.54) | 10.73 (5.95, 15.52) *** | 102.11 (57.99, 146.24) *** | 18.10 (14.21, 22.00) *** | 1.18 (0.62, 1.74) | 16.92 (14.44, 19.41) *** | 150.01 (104.08, 195.94) *** |
| female ≧ 50 | 503 | 43.60 (35.53, 51.67) *** | 0.83 (0.45, 1.22) | 12.13 (5.69, 18.56) *** | 92.77 (71.66, 113.88) *** | 15.39 (12.96, 17.81) *** | 0.92 (0.81, 1.03) | 13.74 (12.32, 15.16) *** | 135.78 (114.28, 157.28) *** |
| Other | |||||||||
| All | 2542 | 74.72 (61.57, 87.88) | 2.58 (2.02, 3.13) | 13.42 (10.99, 15.84) | 155.55 (133.35, 177.75) | 14.73 (12.86, 16.60) | 0.97 (0.90, 1.05) | 18.45 (17.40, 19.50) | 205.69 (182.44, 228.95) |
| male < 50 | 617 | 65.64 (35.89, 95.39) | 2.64 (1.80, 3.48) | 11.23 (7.18, 15.27) | 129.79 (90.52, 169.05) ** | 16.52 (13.11, 19.93) *** | 0.96 (0.84, 1.08) | 19.01 (17.12, 20.89) | 180.14 (138.41, 221.88) ** |
| female < 50 | 744 | 55.10 (45.61, 64.59) | 2.53 (1.55, 3.51) | 13.05 (10.26, 15.84) | 121.23 (97.05, 145.41) ** | 13.90 (11.47, 16.33) *** | 0.90 (0.77, 1.03) | 16.11 (14.66, 17.56) | 167.73 (141.56, 193.89) ** |
| male ≧ 50 | 555 | 99.23 (73.52, 124.94) | 2.48 (1.43, 3.52) | 16.35 (10.81, 21.89) | 213.04 (160.48, 265.60) | 14.26 (11.18, 17.33) * | 1.15 (0.98, 1.32) | 21.66 (19.33, 23.99) | 268.93 (215.27, 322.59) |
| female ≧ 50 | 626 | 104.70 (76.67, 132.72) | 2.62 (1.68, 3.56) | 15.43 (11.42, 19.45) | 213.06 (167.17, 258.95) * | 13.51 (11.05, 15.97) * | 0.99 (0.82, 1.15) | 18.98 (16.79, 21.18) | 264.59 (216.78, 312.40) * |
| Flavonoid Intake Quartiles | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 1Q | 2Q | p for 1Q vs. 2Q | 3Q | p for 1Q vs. 3Q | 4Q | p for 1Q vs. 4Q | HR (95%CI) | p for Trend | |
| Total flavonoid (mg/day) | ≦24.31 | 24.31–64.05 | 64.05–217.38 | >217.38 | |||||
| Model 1 (unadjusted) | 1 | 1.15 (0.71, 1.88) | 0.57 | 0.76 (0.47, 1.22) | 0.26 | 0.74 (0.49, 1.11) | 0.14 | 0.88 (0.78, 0.99) | 0.03 |
| Model 2 (adjusted for age, ethnicity, and gender) | 1 | 0.97 (0.61, 1.55) | 0.91 | 0.54 (0.33, 0.89) | 0.02 | 0.60 (0.40, 0.91) | 0.03 | 0.81 (0.71, 0.92) | <0.01 |
| Model 3 (multivariate) | 1 | 1.16 (0.74, 1.81) | 0.52 | 0.73 (0.45, 1.17) | 0.19 | 0.76 (0.48, 1.20) | 0.24 | 0.88 (0.76, 1.02) | 0.10 |
| Total flavones (mg/day) | ≦0.18 | 0.18–0.51 | 0.51–1.09 | >1.09 | |||||
| Model 1 (unadjusted) | 1 | 0.52 (0.33, 0.82) | 0.01 | 0.67 (0.45, 0.97) | 0.04 | 0.79 (0.52, 1.21) | 0.28 | 0.95 (0.81, 1.11) | 0.52 |
| Model 2 (adjusted for age, ethnicity, and gender) | 1 | 0.46 (0.28, 0.74) | 0.001 | 0.58 (0.39, 0.86) | 0.01 | 0.69 (0.46, 1.05) | 0.08 | 0.91 (0.78, 1.07) | 0.26 |
| Model 3 (multivariate) | 1 | 0.48 (0.26, 0.87) | 0.02 | 0.72 (0.47, 1.10) | 0.12 | 1.02 (0.62, 1.67) | 0.94 | 1.04 (0.88, 1.24) | 0.63 |
| Total anthocyanidins (mg/day) | ≦0.11 | 0.11–2.02 | 2.02–10.78 | >10.78 | |||||
| Model 1 (unadjusted) | 1 | 0.89 (0.57, 1.39) | 0.60 | 0.91 (0.60, 1.37) | 0.64 | 0.72 (0.44, 1.19) | 0.20 | 0.91 (0.78, 1.06) | 0.22 |
| Model 2 (adjusted for age, ethnicity, and gender) | 1 | 0.74 (0.47, 1.18) | 0.21 | 0.65 (0.42, 1.02) | 0.06 | 0.46 (0.27, 0.79) | <0.01 | 0.78 (0.66, 0.92) | <0.01 |
| Model 3 (multivariate) | 1 | 0.86 (0.49, 1.50) | 0.60 | 0.82 (0.48, 1.39) | 0.46 | 0.63 (0.32, 1.23) | 0.18 | 0.87 (0.71, 1.06) | 0.17 |
| Total flavanones (mg/day) | ≦0.06 | 0.06–0.61 | 0.61–18.93 | >18.93 | |||||
| Model 1 (unadjusted) | 1 | 0.90 (0.59, 1.36) | 0.61 | 0.79 (0.50, 1.25) | 0.319 | 1.01 (0.68, 1.50) | 0.97 | 0.99 (0.86, 1.14) | 0.90 |
| Model 2 (adjusted for age, ethnicity, and gender) | 1 | 0.89 (0.58, 1.36) | 0.58 | 0.72 (0.46, 1.14) | 0.16 | 0.74 (0.48, 1.12) | 0.16 | 0.89 (0.78, 1.03) | 0.13 |
| Model 3 (multivariate) | 1 | 1.23 (0.73, 2.07) | 0.44 | 1.06 (0.66, 1.73) | 0.80 | 1.02 (0.65, 1.59) | 0.93 | 0.99 (0.86, 1.13) | 0.88 |
| Total flavonol (mg/day) | ≦6.82 | 6.82–12.56 | 12.56–22.11 | >22.11 | |||||
| Model 1 (unadjusted) | 1 | 0.60 (0.41, 0.88) | 0.01 | 0.63 (0.39, 1.05) | 0.08 | 0.53 (0.34, 0.83) | 0.01 | 0.83 (0.70, 0.97) | 0.02 |
| Model 2 (adjusted for age, ethnicity, and gender) | 1 | 0.56 (0.39, 0.79) | 0.001 | 0.59 (0.37, 0.93) | 0.03 | 0.51 (0.33, 0.81) | <0.01 | 0.82 (0.69, 0.96) | 0.02 |
| Model 3 (multivariate) | 1 | 0.58 (0.36, 0.91) | 0.02 | 0.55 (0.31, 0.96) | 0.04 | 0.54 (0.30, 0.99) | 0.05 | 0.82 (0.67, 1.02) | 0.08 |
| Total Flavan–3–ols (mg/day) | ≦4.92 | 4.92–15.43 | 15.43–154.30 | >154.30 | |||||
| Model 1 (unadjusted) | 1 | 0.88 (0.60, 1.30) | 0.53 | 0.90 (0.56, 1.46) | 0.68 | 0.71 (0.47, 1.08) | 0.11 | 0.90 (0.79, 1.03) | 0.13 |
| Model 2 (adjusted for age, ethnicity, and gender) | 1 | 0.71 (0.48, 1.05) | 0.09 | 0.66 (0.42, 1.03) | 0.07 | 0.57 (0.38, 0.86) | 0.01 | 0.84 (0.73, 0.96) | 0.01 |
| Model 3 (multivariate) | 1 | 0.82 (0.53, 1.27) | 0.38 | 0.79 (0.48, 1.31) | 0.36 | 0.68 (0.42, 1.12) | 0.13 | 0.89 (0.76, 1.04) | 0.15 |
| Subtotal Catechins (mg/day) | ≦4.78 | 4.78–14.49 | 14.49–63.83 | >63.83 | |||||
| Model 1 (unadjusted) | 1 | 0.89 (0.60, 1.32) | 0.55 | 0.83 (0.51, 1.36) | 0.46 | 0.74 (0.49, 1.11) | 0.14 | 0.91 (0.80, 1.03) | 0.14 |
| Model 2 (adjusted for age, ethnicity, and gender) | 1 | 0.71 (0.47, 1.07) | 0.10 | 0.61 (0.39, 0.97) | 0.04 | 0.59 (0.39, 0.88) | 0.011 | 0.84 (0.74, 0.96) | 0.01 |
| Model 3 (multivariate) | 1 | 0.81 (0.51, 1.28) | 0.36 | 0.72 (0.43, 1.21) | 0.21 | 0.71 (0.44, 1.16) | 0.18 | 0.90 (0.76, 1.06) | 0.19 |
| Total isoflavones (mg/day) | ≦0.01 | >0.01 | |||||||
| Model 1 (unadjusted) | 1 | 0.74 (0.57, 0.97) | 0.03 | ||||||
| Model 2 (adjusted for age, ethnicity, and gender) | 1 | 0.81 (0.61, 1.09) | 0.16 | ||||||
| Model 3 (multivariate) | 1 | 0.93 (0.64, 1.35) | 0.70 | ||||||
| Quartile of Isoflavone Metabolites | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| HR (95%CI) | 1Q | 2Q | 3Q | 4Q | HR (95%CI) | p for Trend | |||
| Daidzein (ng/mL) | <16.6 | 16.6–48.8 | 48.8–195.0 | ≧195.0 | |||||
| model 1 (unadjusted) | 1 | 1.31 (0.72, 2.37) | 0.38 | 0.99 (0.53, 1.85) | 0.97 | 1.22 (0.58, 2.55) | 0.60 | 1.03 (0.82, 1.30) | 0.56 |
| model 2 (adjusted for age, race, and sex) | 1 | 1.27 (0.69, 2.31) | 0.44 | 0.88 (0.48, 1.61) | 0.68 | 1.22 (0.60, 2.49) | 0.59 | 1.02 (0.81, 1.29) | 0.84 |
| model 3 (multivariate) | 1 | 1.41 (0.91, 2.19) | 0.12 | 0.96 (0.53, 1.72) | 0.89 | 1.38 (0.73, 2.62) | 0.32 | 1.06 (0.87, 1.29) | 0.78 |
| ODMA (ng/mL) | <0.60 | 0.60–2.70 | 2.70–19.15 | ≧19.15 | |||||
| model 1 (unadjusted) | 1 | 1.21 (0.68, 2.14) | 0.51 | 0.90 (0.53, 1.52) | 0.70 | 0.78 (0.46, 1.33) | 0.36 | 0.90 (0.77, 1.06) | 0.20 |
| model 2 (adjusted for age, race, and sex) | 1 | 0.93 (0.55, 1.58) | 0.79 | 0.62 (0.38, 1.02) | 0.06 | 0.63 (0.38, 1.05) | 0.08 | 0.83 (0.71, 0.98) | 0.03 |
| model 3 (multivariate) | 1 | 0.97 (0.49, 1.94) | 0.94 | 0.63 (0.32, 1.22) | 0.17 | 0.66 (0.31, 1.40) | 0.27 | 0.84 (0.66, 1.06) | 0.14 |
| Equol (ng/mL) | <2.70 | 2.70–6.18 | 6.18–13.70 | ≧13.70 | |||||
| model 1 (unadjusted) | 1 | 0.87 (0.47, 1.62) | 0.67 | 1.04 (0.62, 1.76) | 0.88 | 0.95 (0.54, 1.68) | 0.87 | 1.00 (0.83, 1.22) | 0.97 |
| model 2 (adjusted for age, race, and sex) | 1 | 0.85 (0.47, 1.54) | 0.59 | 0.81 (0.50, 1.32) | 0.40 | 0.83 (0.49, 1.40) | 0.48 | 0.94 (0.79, 1.13) | 0.53 |
| model 3 (multivariate) | 1 | 0.99 (0.54, 1.82) | 0.97 | 0.88 (0.56, 1.38) | 0.57 | 0.95 (0.60, 1.50) | 0.82 | 0.97 (0.84, 1.13) | 0.71 |
| Genistein (ng/mL) | <8.35 | 8.35–24.90 | 24.90–88.60 | ≧88.60 | |||||
| model 1 (unadjusted) | 1 | 1.12 (0.66, 1.90) | 0.69 | 1.23 (0.75, 2.03) | 0.41 | 1.14 (0.57, 2.29) | 0.72 | 1.05 (0.86, 1.28) | 0.65 |
| model 2 (adjusted for age, race, and sex) | 1 | 1.15 (0.68, 1.96) | 0.60 | 1.13 (0.69, 1.86) | 0.62 | 1.09 (0.53, 2.24) | 0.82 | 1.02 (0.83, 1.26) | 0.84 |
| model 3 (multivariate) | 1 | 1.20 (0.59, 2.40) | 0.62 | 1.20 (0.65, 2.23) | 0.55 | 1.18 (0.61, 2.30) | 0.63 | 1.05 (0.87, 1.27) | 0.63 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, Y.; Gu, K.; Zhou, F. Dietary Flavonoid Intake and Cancer Mortality: A Population-Based Cohort Study. Nutrients 2023, 15, 976. https://doi.org/10.3390/nu15040976
Zhou Y, Gu K, Zhou F. Dietary Flavonoid Intake and Cancer Mortality: A Population-Based Cohort Study. Nutrients. 2023; 15(4):976. https://doi.org/10.3390/nu15040976
Chicago/Turabian StyleZhou, Yanjun, Ke Gu, and Fengying Zhou. 2023. "Dietary Flavonoid Intake and Cancer Mortality: A Population-Based Cohort Study" Nutrients 15, no. 4: 976. https://doi.org/10.3390/nu15040976
APA StyleZhou, Y., Gu, K., & Zhou, F. (2023). Dietary Flavonoid Intake and Cancer Mortality: A Population-Based Cohort Study. Nutrients, 15(4), 976. https://doi.org/10.3390/nu15040976