



Acute Insulin Secretory Effects of a Classic Ketogenic Meal in Healthy Subjects: A Randomized Cross-Over Study
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Experimental Protocol
2.3. Laboratory Analyses
2.4. Analysis and Modelling of Meal
2.5. Statistical Analysis
3. Results
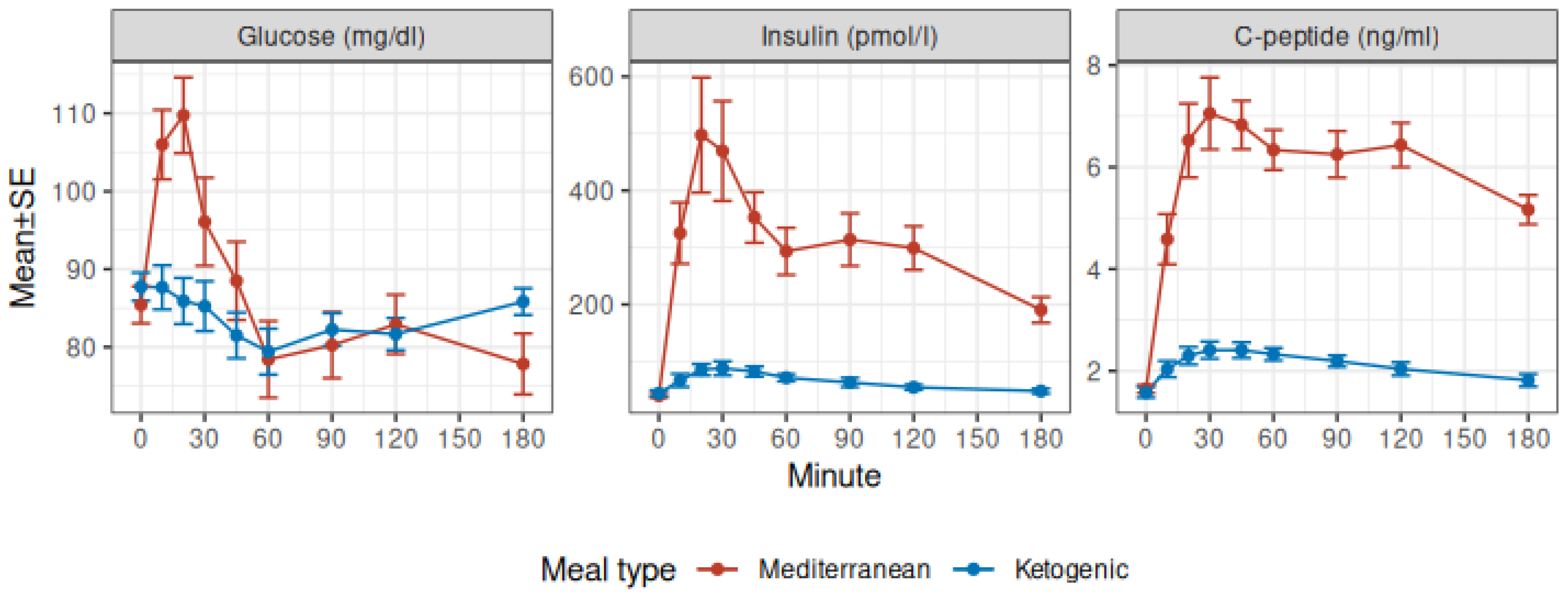
3.1. Glucose, Insulin, and C-Peptide
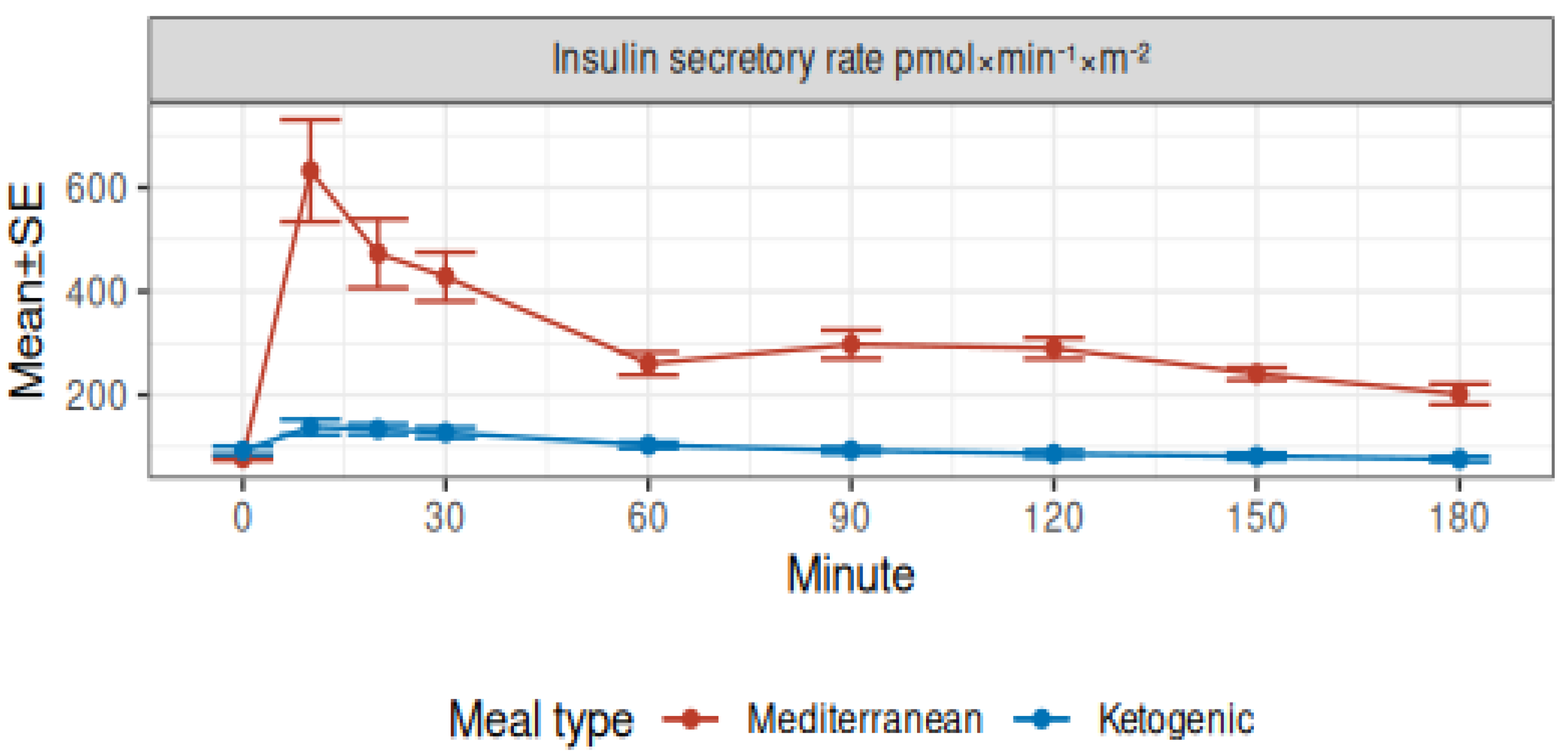
3.2. Modeled Insulin Secretion and Insulin Clearance
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Desli, E.; Spilioti, M.; Evangeliou, A.; Styllas, F.; Magkos, F.; Dalamaga, M. The efficacy and safety of ketogenic diets in drug-resistant epilepsy in children and adolescents: A systematic review of randomized controlled trials. Curr. Nutr. Rep. 2022, 11, 102–116. [Google Scholar] [CrossRef] [PubMed]
- Koch, H.; Weber, Y.G. The glucose transporter type 1 (Glut1) syndromes. Epilepsy Behav. 2019, 91, 90–93. [Google Scholar] [CrossRef] [PubMed]
- De Amicis, R.; Leone, A.; Lessa, C.; Foppiani, A.; Ravella, S.; Ravasenghi, S.; Trentani, C.; Ferraris, C.; Veggiotti, P.; De Giorgis, V.; et al. Long-term effects of a classic ketogenic diet on ghrelin and leptin concentration: A 12-month prospective study in a cohort of Italian children and adults with glut1-deficiency syndrome and drug resistant epilepsy. Nutrients 2019, 11, 1716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varesio, C.; Pasca, L.; Parravicini, S.; Zanaboni, M.P.; Ballante, E.; Masnada, S.; Ferraris, C.; Bertoli, S.; Tagliabue, A.; Veggiotti, P.; et al. Quality of life in chronic ketogenic diet treatment: The glut1ds population perspective. Nutrients 2019, 11, 1650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertoli, S.; Masnada, S.; De Amicis, R.; Sangiorgio, A.; Leone, A.; Gambino, M.; Lessa, C.; Tagliabue, A.; Ferraris, C.; De Giorgis, V.; et al. Glucose transporter 1 deficiency syndrome: Nutritional and growth pattern phenotypes at diagnosis. Eur. J. Clin. Nutr. 2020, 74, 1290–1298. [Google Scholar] [CrossRef]
- Pietrzak, D.; Kasperek, K.; Rękawek, P.; Piątkowska-Chmiel, I. The therapeutic role of ketogenic diet in neurological disorders. Nutrients 2022, 14, 1952. [Google Scholar] [CrossRef] [PubMed]
- Ferraris, C.; Guglielmetti, M.; Pasca, L.; De Giorgis, V.; Ferraro, O.E.; Brambilla, I.; Leone, A.; De Amicis, R.; Bertoli, S.; Veggiotti, P.; et al. Impact of the ketogenic diet on linear growth in children: A single-center retrospective analysis of 34 cases. Nutrients 2019, 11, 1442. [Google Scholar] [CrossRef] [Green Version]
- Wibisono, C.; Rowe, N.; Beavis, E.; Kepreotes, H.; Mackie, F.E.; Lawson, J.A.; Cardamone, M. Ten-year single-center experience of the ketogenic diet: Factors influencing efficacy, tolerability, and compliance. J. Pediatr. 2015, 166, 1030–1036.e1. [Google Scholar] [CrossRef] [PubMed]
- Heussinger, N.; Della Marina, A.; Beyerlein, A.; Leiendecker, B.; Hermann-Alves, S.; Dalla Pozza, R.; Klepper, J. 10 patients, 10 years long term follow-up of cardiovascular risk factors in Glut1 deficiency treated with ketogenic diet therapies: A prospective, multicenter case series. Clin. Nutr. 2018, 37, 2246–2251. [Google Scholar] [CrossRef] [Green Version]
- Gershuni, V.M.; Yan, S.L.; Medici, V. Nutritional Ketosis for Weight Management and Reversal of Metabolic Syndrome. Curr. Nutr. Rep. 2018, 7, 97–106. [Google Scholar] [CrossRef]
- Kosinski, C.; Jornayvaz, F.R. Effects of Ketogenic Diets on Cardiovascular Risk Factors: Evidence from Animal and Human Studies. Nutrients 2017, 9, 517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, X.; Wang, J.; Yang, S.; Gao, M.; Cao, L.; Li, X.; Hong, D.; Tian, S.; Sun, C. Effect of the ketogenic diet on glycemic control, insulin resistance, and lipid metabolism in patients with T2DM: A systematic review and meta-analysis. Nutr. Diabetes 2020, 10, 38. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, B.; Raggi, P. The ketogenic diet: Pros and cons. Atherosclerosis 2019, 292, 119–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopp, W. How western diet and lifestyle drive the pandemic of obesity and civilization diseases. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 2221–2236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehran, A.E.; Templeman, N.M.; Brigidi, G.S.; Lim, G.E.; Chu, K.-Y.; Hu, X.; Botezelli, J.D.; Asadi, A.; Hoffman, B.G.; Kieffer, T.J.; et al. Hyperinsulinemia drives diet-induced obesity independently of brain insulin production. Cell Metab. 2012, 16, 723–737. [Google Scholar] [CrossRef] [Green Version]
- Kopp, W. High-insulinogenic nutritionan etiologic factor for obesity and the metabolic syndrome? Metabolism 2003, 52, 840–844. [Google Scholar] [CrossRef] [PubMed]
- Nolan, C.; Prentki, M. Insulin resistance and insulin hypersecretion in the metabolic syndrome and type 2 diabetes: Time for a conceptual framework shift. Diabetes Vasc. Dis. Res. 2019, 16, 118–127. [Google Scholar] [CrossRef]
- Erion, K.A.; Corkey, B.E. Hyperinsulinemia: A cause of obesity? Curr. Obes. Rep. 2017, 6, 178–186. [Google Scholar] [CrossRef] [Green Version]
- Templeman, N.M.; Skovsø, S.; Page, M.M.; Lim, G.E.; Johnson, J.D. A causal role for hyperinsulinemia in obesity. J. Endocrinol. 2017, 232, R173–R183. [Google Scholar] [CrossRef] [Green Version]
- Battezzati, A.; Terruzzi, I.; Perseghin, G.; Bianchi, E.; Carlo, V.D.; Pozza, G.; Luzi, L. Defective insulin action on protein and glucose metabolism during chronic hyperinsulinemia in subjects with benign insulinoma. Diabetes 1995, 44, 837–844. [Google Scholar] [CrossRef]
- Corkey, B.E. Banting lecture 2011. Diabetes 2011, 61, 4–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shanik, M.H.; Xu, Y.; Skrha, J.; Dankner, R.; Zick, Y.; Roth, J. Insulin resistance and hyperinsulinemia. Diabetes Care 2008, 31 (Suppl. S2), S262–S268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.S.; Gerber, J.N.; You, H.J. Association between fasting insulin and high-sensitivity C reactive protein in Korean adults. BMJ Open Sport Exerc. Med. 2017, 3, e000236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pyörälä, M.; Miettinen, H.; Laakso, M.; Pyörälä, K. Hyperinsulinemia predicts coronary heart disease risk in healthy middle-aged men. Circulation 1998, 98, 398–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, G.L.; Park, K.; Li, Q. Selective insulin resistance and the development of cardiovascular diseases in diabetes: The 2015 edwin bierman award lecture. Diabetes 2016, 65, 1462–1471. [Google Scholar] [CrossRef] [Green Version]
- Charlot, A.; Zoll, J. Beneficial Effects of the Ketogenic Diet in Metabolic Syndrome: A Systematic Review. Diabetology 2022, 3, 292–309. [Google Scholar] [CrossRef]
- Hernandez, T.L.; Sutherland, J.P.; Wolfe, P.; Allian-Sauer, M.; Capell, W.H.; Talley, N.D.; Wyatt, H.R.; Foster, G.D.; Hill, J.O.; Eckel, R.H. Lack of suppression of circulating free fatty acids and hypercholesterolemia during weight loss on a high-fat, low-carbohydrate diet. Am. J. Clin. Nutr. 2010, 91, 578–585. [Google Scholar] [CrossRef] [Green Version]
- Bojsen-Møller, K.N.; Lundsgaard, A.-M.; Madsbad, S.; Kiens, B.; Holst, J.J. Hepatic insulin clearance in regulation of systemic insulin concentrations—Role of carbohydrate and energy availability. Diabetes 2018, 67, 2129–2136. [Google Scholar] [CrossRef] [Green Version]
- Mari, A.; Tura, A.; Gastaldelli, A.; Ferrannini, E. Assessing insulin secretion by modeling in multiple-meal tests: Role of potentiation. Diabetes 2002, 51 (Suppl. S1), S221–S226. [Google Scholar] [CrossRef] [Green Version]
- Harris, J.A.; Benedict, F.G. A biometric study of human basal metabolism. Proc. Natl. Acad. Sci. USA 1918, 4, 370–373. [Google Scholar] [CrossRef] [Green Version]
- Società Italiana di Nutrizione Umana. LARN: Livelli di Assunzione di Riferimento di Nutrienti ed Energia per la Popolazione Italiana; Società Italiana di Comunicazione Scientifica e Sanitaria: Milan, Italy, 2014. [Google Scholar]
- Foppiani, A.; De Amicis, R.; Lessa, C.; Leone, A.; Ravella, S.; Ciusani, E.; Silvani, A.; Zuccoli, G.; Battezzati, A.; Lamperti, E.; et al. Isocaloric ketogenic diet in adults with high-grade gliomas: A prospective metabolic study. Nutr. Cancer 2020, 73, 1004–1014. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: https://www.R-project.org/ (accessed on 8 January 2023).
- Battezzati, A.; Mari, A.; Zazzeron, L.; Alicandro, G.; Claut, L.; Battezzati, P.M.; Colombo, C. Identification of insulin secretory defects and insulin resistance during oral glucose tolerance test in a cohort of cystic fibrosis patients. Eur. J. Endocrinol. 2011, 165, 69–76. [Google Scholar] [CrossRef] [Green Version]
- Vilsbøll, T.; Krarup, T.; Sonne, J.; Madsbad, S.; Vølund, A.; Juul, A.G.; Holst, J.J. Incretin secretion in relation to meal size and body weight in healthy subjects and people with type 1 and type 2 diabetes mellitus. J. Clin. Endocrinol. Metab. 2003, 88, 2706–2713. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Behl, T.; Sachdeva, M.; Sehgal, A.; Kumari, S.; Kumar, A.; Kaur, G.; Yadav, H.N.; Bungau, S. Implicating the effect of ketogenic diet as a preventive measure to obesity and diabetes mellitus. Life Sci. 2020, 264, 118661. [Google Scholar] [CrossRef]
- Società Italiana di Diabetologia. Terapia Insulinica. 2022. Available online: https://www.siditalia.it/divulgazione/insulina (accessed on 8 January 2023).
- Diakogiannaki, E.; Gribble, F.M.; Reimann, F. Nutrient detection by incretin hormone secreting cells. Physiol. Behav. 2012, 106, 387–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Najjar, S.M.; Perdomo, G. Hepatic insulin clearance: Mechanism and physiology. Physiology 2019, 34, 198–215. [Google Scholar] [CrossRef] [PubMed]
- Bergman, R.N.; Kabir, M.; Ader, M. The physiology of insulin clearance. Int. J. Mol. Sci. 2022, 23, 1826. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Overall, n = 12 1 | Female, n = 6 1 | Male, n = 6 1 |
|---|---|---|---|
| Age (years) | 24.1 (23.1, 25.2) | 23.7 (23.3, 24.6) | 24.7 (23.2, 25.7) |
| Body mass index (kg/m2) | 21.5 (20.4, 23.4) | 21.8 (20.3, 23.0) | 21.5 (20.7, 23.7) |
| Waist circumference (cm) | 73.9 (72.7, 78.4) | 72.6 (72.4, 73.5) | 76.7 (74.3, 78.8) |
| Fat mass fraction (as %) | 20.7 (16.4, 30.0) | 30.1 (28.6, 33.9) | 15.9 (12.3, 17.4) |
| Total energy expenditure (kcal) | 2393 (2164, 2655) | 2156 (2139, 2215) | 2679 (2555, 2776) |
| OGTT Minutes | Two-Way ANOVA p-Values 2 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristic | Group | 0 1 | 10 1 | 20 1 | 30 1 | 60 1 | 90 1 | 120 1 | 180 1 | Minute | Meal | Interaction |
| Glucose (mg/dL) | <0.001 | 0.005 | <0.001 | |||||||||
| Mediterranean | 85 ± 2 | 106 ± 4 | 110 ± 5 | 96 ± 6 | 78 ± 5 | 80 ± 4 | 83 ± 4 | 78 ± 4 | ||||
| Ketogenic | 88 ± 2 | 88 ± 3 | 86 ± 3 | 85 ± 3 | 79 ± 3 | 82 ± 2 | 82 ± 2 | 86 ± 2 | ||||
| Insulin (pmol/L) | <0.001 | <0.001 | <0.001 | |||||||||
| Mediterranean | 40 ± 4 | 325 ± 54 | 497 ± 101 | 469 ± 88 | 293 ± 41 | 314 ± 46 | 299 ± 38 | 190 ± 23 | ||||
| Ketogenic | 44 ± 5 | 67 ± 11 | 86 ± 10 | 88 ± 12 | 71 ± 6 | 63 ± 8 | 55 ± 5 | 48 ± 4 | ||||
| C-peptide (ng/mL) | <0.001 | <0.001 | <0.001 | |||||||||
| Mediterranean | 1.65 ± 0.08 | 4.58 ± 0.49 | 6.52 ± 0.72 | 7.05 ± 0.71 | 6.34 ± 0.39 | 6.25 ± 0.46 | 6.43 ± 0.43 | 5.16 ± 0.29 | ||||
| Ketogenic | 1.58 ± 0.10 | 2.04 ± 0.16 | 2.30 ± 0.17 | 2.41 ± 0.17 | 2.33 ± 0.12 | 2.19 ± 0.11 | 2.04 ± 0.13 | 1.82 ± 0.12 | ||||
| Insulin secretion rate (pmol × min−1 × m−2) | <0.001 | <0.001 | <0.001 | |||||||||
| Mediterranean | 78 ± 4 | 632 ± 98 | 473 ± 66 | 428 ± 47 | 261 ± 22 | 298 ± 27 | 290 ± 20 | 202 ± 20 | ||||
| Ketogenic | 93 ± 8 | 138 ± 15 | 134 ± 10 | 128 ± 10 | 103 ± 6 | 94 ± 6 | 87 ± 7 | 77 ± 5 | ||||
| Characteristic | Mediterranean, n = 12 1 | Ketogenic, n = 12 1 | Difference 2 | 95% CI 2,3 | p-Value 2 |
|---|---|---|---|---|---|
| Basal rate of insulin secretion (pmol × min−1 × m−2) | 78 ± 4 | 93 ± 8 | −14 | −32, 2.7 | 0.091 |
| Peak rate of insulin secretion (pmol × min−1 × m−2) | 697 ± 95 | 161 ± 14 | 535 | 308, 763 | <0.001 |
| Basal insulin concentration (pmol/L) | 40 ± 4 | 44 ± 5 | −3.8 | −12, 4.1 | 0.3 |
| Incremental insulin concentration (pmol/L) | 7929 ± 999 | 668 ± 110 | 7261 | 5040, 9482 | <0.001 |
| Total insulin concentration (pmol/L) | 54,764 ± 6378 | 9821 ± 1103 | 44,943 | 30,706, 59,181 | <0.001 |
| Basal insulin clearance (l × min−1 × m−2) | 2.12 ± 0.18 | 2.48 ± 0.39 | −0.36 | −0.95, 0.22 | 0.2 |
| Insulin clearance during the test (l × min−1 × m−2) | 1.10 ± 0.08 | 1.39 ± 0.18 | −0.30 | −0.74, 0.15 | 0.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Battezzati, A.; Foppiani, A.; Leone, A.; De Amicis, R.; Spadafranca, A.; Mari, A.; Bertoli, S. Acute Insulin Secretory Effects of a Classic Ketogenic Meal in Healthy Subjects: A Randomized Cross-Over Study. Nutrients 2023, 15, 1119. https://doi.org/10.3390/nu15051119
Battezzati A, Foppiani A, Leone A, De Amicis R, Spadafranca A, Mari A, Bertoli S. Acute Insulin Secretory Effects of a Classic Ketogenic Meal in Healthy Subjects: A Randomized Cross-Over Study. Nutrients. 2023; 15(5):1119. https://doi.org/10.3390/nu15051119
Chicago/Turabian StyleBattezzati, Alberto, Andrea Foppiani, Alessandro Leone, Ramona De Amicis, Angela Spadafranca, Andrea Mari, and Simona Bertoli. 2023. "Acute Insulin Secretory Effects of a Classic Ketogenic Meal in Healthy Subjects: A Randomized Cross-Over Study" Nutrients 15, no. 5: 1119. https://doi.org/10.3390/nu15051119