
Maternal Pre-Pregnancy Nutritional Status and Infant Birth Weight in Relation to 0–2 Year-Growth Trajectory and Adiposity in Term Chinese Newborns with Appropriate Birth Weight-for-Gestational Age
 , , ,
, , ,
Abstract
:
1. Introduction
2. Methods
2.1. Study Population
2.2. Maternal Prenatal Nutritional Factors
2.3. AGA Definition and Sex- and Gestational Age-Specific Birthweight Tertiles among AGA
2.4. Child Anthropometric Measures
2.5. Postnatal Covariates
2.6. Data Analysis and Statistics
3. Results
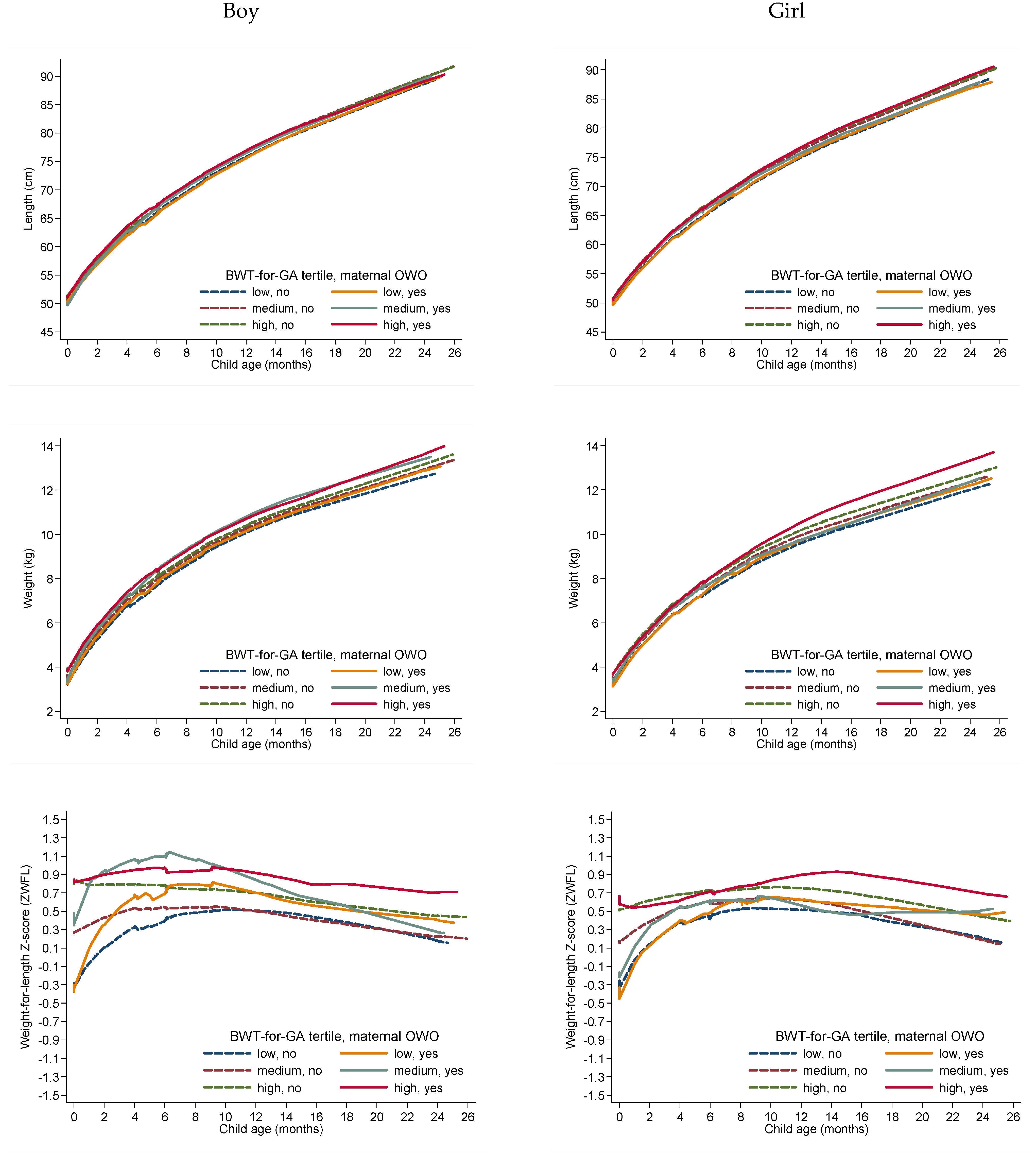
3.1. Longitudinal Data Analysis of Birthweight-for-Gestational Age Tertiles, Prenatal Factors and Adiposity Measures among AGA Infants at Age 0–2 Years
3.2. Prenatal Factors, Birthweight-for-Gestational Age Tertiles, and Body Composition among AGA Infants at 2 Years of Age
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Blake-Lamb, T.L.; Locks, L.M.; Perkins, M.E.; Baidal, J.A.W.; Cheng, E.R.; Taveras, E.M. Interventions for Childhood Obesity in the First 1000 Days a Systematic Review. Am. J. Prev. Med. 2016, 50, 780–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osmond, C.; Barker, D.J.; Winter, P.D.; Fall, C.H.; Simmonds, S.J. Early growth and death from cardiovascular disease in women. BMJ 1993, 307, 1519–1524. [Google Scholar] [CrossRef] [Green Version]
- Boney, C.M.; Verma, A.; Tucker, R.; Vohr, B.R. Metabolic syndrome in childhood: Association with birth weight, maternal obesity, and gestational diabetes mellitus. Pediatrics 2005, 115, e290–e296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleming, T.P.; Watkins, A.J.; Velazquez, M.A.; Mathers, J.C.; Prentice, A.M.; Stephenson, J.; Barker, M.; Saffery, R.; Yajnik, C.S.; Eckert, J.J.; et al. Origins of lifetime health around the time of conception: Causes and consequences. Lancet 2018, 391, 1842–1852. [Google Scholar] [CrossRef] [PubMed]
- Barker, D.J.; Gluckman, P.D.; Godfrey, K.M.; Harding, J.E.; Owens, J.A.; Robinson, J.S. Fetal nutrition and cardiovascular disease in adult life. Lancet 1993, 341, 938–941. [Google Scholar] [CrossRef]
- Meas, T.; Deghmoun, S.; Armoogum, P.; Alberti, C.; Levy-Marchal, C. Consequences of being born small for gestational age on body composition: An 8-year follow-up study. J. Clin. Endocrinol. Metab. 2008, 93, 3804–3809. [Google Scholar] [CrossRef]
- Liao, X.P.; Yu, Y.; Marc, I.; Dubois, L.; Abdelouahab, N.; Bouchard, L.; Wu, Y.T.; Ouyang, F.; Huang, H.F.; Fraser, W.D. Prenatal determinants of childhood obesity: A review of risk factors (1). Can. J. Physiol. Pharmacol. 2019, 97, 147–154. [Google Scholar] [CrossRef]
- Ouyang, F.; Parker, M.G.; Luo, Z.C.; Wang, X.; Zhang, H.J.; Jiang, F.; Wang, X.; Gillman, M.W.; Zhang, J. Maternal BMI, gestational diabetes, and weight gain in relation to childhood obesity: The mediation effect of placental weight. Obes. Silver Spring Md. 2016, 24, 938–946. [Google Scholar] [CrossRef] [Green Version]
- Ouyang, F.; Parker, M.; Cerda, S.; Pearson, C.; Fu, L.; Gillman, M.W.; Zuckerman, B.; Wang, X. Placental weight mediates the effects of prenatal factors on fetal growth: The extent differs by preterm status. Obes. Silver Spring Md. 2013, 21, 609–620. [Google Scholar] [CrossRef] [Green Version]
- He, S.; Allen, J.C.; Razali, N.S.; Chern, B.S.M.; Tan, K.H. Association between gestational weight gain and pregnancy outcomes in a Singaporean population: A prospective cohort study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 272, 160–165. [Google Scholar] [CrossRef]
- Craemer, K.A.; Sampene, E.; Safdar, N.; Antony, K.M.; Wautlet, C.K. Nutrition and Exercise Strategies to Prevent Excessive Pregnancy Weight Gain: A Meta-analysis. AJP Rep. 2019, 9, e92–e120. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; Marc, I.; Bouchard, L.; Ouyang, F.; Luo, Z.C.; Fan, J.; Dubois, L.; Mâsse, B.; Zhang, J.; Leung, P.C.K.; et al. Study protocol for the Sino-Canadian Healthy Life Trajectories Initiative (SCHeLTI): A multicentre, cluster-randomised, parallel-group, superiority trial of a multifaceted community-family-mother-child intervention to prevent childhood overweight and obesity. BMJ Open 2021, 11, e045192. [Google Scholar] [CrossRef] [PubMed]
- Griffin, I.J.; Cooke, R.J. Development of whole body adiposity in preterm infants. Early Hum. Dev. 2012, 88 (Suppl. 1), S19–S24. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Lu, F.C. The guidelines for prevention and control of overweight and obesity in Chinese adults. Biomed. Environ. Sci 2004, 17, 1–36. [Google Scholar] [PubMed]
- Goldstein, R.F.; Abell, S.K.; Ranasinha, S.; Misso, M.; Boyle, J.A.; Black, M.H.; Li, N.; Hu, G.; Corrado, F.; Rode, L.; et al. Association of Gestational Weight Gain with Maternal and Infant Outcomes: A Systematic Review and Meta-analysis. JAMA 2017, 317, 2207–2225. [Google Scholar] [CrossRef]
- Institute of Medicine. Weight Gain During Pregnancy: Reexamining the Guidelines; National Academies Press: Washington, DC, USA, 2009; NBK32813. [Google Scholar]
- ADA. Diagnosis and classification of diabetes mellitus. Diabetes Care 2013, 36 (Suppl. 1), S67–S74. [Google Scholar] [CrossRef] [Green Version]
- Ouyang, F.; Tang, N.; Zhang, H.J.; Wang, X.; Zhao, S.; Wang, W.; Zhang, J.; Cheng, W. Maternal urinary triclosan level, gestational diabetes mellitus and birth weight in Chinese women. Sci. Total Environ. 2018, 626, 451–457. [Google Scholar] [CrossRef]
- Zhu, L.; Zhang, R.; Zhang, S.L.; Shi, W.J.; Yan, W.L.; Wang, X.L.; Lyu, Q.; Liu, L.; Zhou, Q.; Qiu, Q.F. Chinese neonatal birth weight curve for different gestational age. Chin. J. Pediatr. 2015, 53, 97–103. [Google Scholar]
- Ouyang, F.; Zhang, G.H.; Du, K.; Shen, L.; Ma, R.; Wang, X.; Wang, X.; Zhang, J. Maternal prenatal urinary bisphenol A level and child cardio-metabolic risk factors: A prospective cohort study. Environ. Pollut. Barking Essex 1987 2020, 265, 115008. [Google Scholar] [CrossRef]
- Wickramasinghe, V.P.; Lamabadusuriya, S.P.; Cleghorn, G.J.; Davies, P.S. Assessment of body composition in Sri Lankan children: Validation of a skin fold thickness equation. Ceylon. Med. J. 2008, 53, 83–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Onis, M.; Onyango, A.; Borghi, E.; Siyam, A.; Blossner, M.; Lutter, C.; WHO Multicentre Growth Reference Study Group. Worldwide implementation of the WHO Child Growth Standards. Public Health Nutr. 2012, 15, 1603–1610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hendrix, M.L.E.; van Kuijk, S.M.J.; El Bahaey, S.E.; Gerver, W.J.M.; Feron, F.J.M.; Kuin, M.E.; Spaanderman, M.E.A.; Bons, J.A.P.; Al-Nasiry, S. Postnatal growth during the first five years of life in SGA and AGA neonates with reduced fetal growth. Early Hum. Dev. 2020, 151, 105199. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Mi, J.; Shan, X.Y.; Wang, Q.J.; Ge, K.Y. Is China facing an obesity epidemic and the consequences? The trends in obesity and chronic disease in China. Int. J. Obes. 2005 2007, 31, 177–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, B.F. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults—Study on optimal cut-off points of body mass index and waist circumference in Chinese adults. Biomed. Env. Sci. 2002, 15, 83–96. [Google Scholar]
- Aris, I.M.; Bernard, J.Y.; Chen, L.W.; Tint, M.T.; Pang, W.W.; Soh, S.E.; Saw, S.M.; Shek, L.P.; Godfrey, K.M.; Gluckman, P.D.; et al. Modifiable risk factors in the first 1000 days for subsequent risk of childhood overweight in an Asian cohort: Significance of parental overweight status. Int. J. Obes. Lond. 2018, 42, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Heslehurst, N.; Vieira, R.; Akhter, Z.; Bailey, H.; Slack, E.; Ngongalah, L.; Pemu, A.; Rankin, J. The association between maternal body mass index and child obesity: A systematic review and meta-analysis. PLoS Med. 2019, 16, e1002817. [Google Scholar] [CrossRef] [Green Version]
- Voerman, E.; Santos, S.; Inskip, H.; Amiano, P.; Barros, H.; Charles, M.A.; Chatzi, L.; Chrousos, G.P.; Corpeleijn, E.; Crozier, S.; et al. Association of Gestational Weight Gain with Adverse Maternal and Infant Outcomes. JAMA 2019, 321, 1702–1715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, R.C.W.; Schmidt, M.I.; Tam, W.H.; McIntyre, H.D.; Catalano, P.M. Clinical management of pregnancy in the obese mother: Before conception, during pregnancy, and post partum. Lancet Diabetes Endocrinol. 2016, 4, 1037–1049. [Google Scholar] [CrossRef] [Green Version]
- Tyrrell, J.; Richmond, R.C.; Palmer, T.M.; Feenstra, B.; Rangarajan, J.; Metrustry, S.; Cavadino, A.; Paternoster, L.; Armstrong, L.L.; De Silva, N.M.; et al. Genetic Evidence for Causal Relationships between Maternal Obesity-Related Traits and Birth Weight. JAMA 2016, 315, 1129–1140. [Google Scholar] [CrossRef] [Green Version]
- Brandkvist, M.; Bjørngaard, J.H.; Ødegård, R.A.; Åsvold, B.O.; Sund, E.R.; Vie, G.Å. Quantifying the impact of genes on body mass index during the obesity epidemic: Longitudinal findings from the HUNT Study. BMJ 2019, 366, l4067. [Google Scholar] [CrossRef] [Green Version]
- Silventoinen, K.; Rokholm, B.; Kaprio, J.; Sørensen, T.I. The genetic and environmental influences on childhood obesity: A systematic review of twin and adoption studies. Int. J. Obes. 2005 2010, 34, 29–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golab, B.P.; Santos, S.; Voerman, E.; Lawlor, D.A.; Jaddoe, V.W.V.; Gaillard, R. Influence of maternal obesity on the association between common pregnancy complications and risk of childhood obesity: An individual participant data meta-analysis. Lancet Child Adolesc. Health 2018, 2, 812–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Maternal Characteristics | Mean ± SD, or n (%) | Infant Characteristics | Mean ± SD, or n (%) |
|---|---|---|---|
| Maternal age at childbirth (years) | 29.4 ± 3.5 | Gestational age (weeks) | 39.0 ± 1.0 |
| Prepregnancy BMI (kg/m2) | 21.2 ± 3.0 | Birthweight (g) | 3359.8 ± 281.5 |
| Mother Education | Infant sex | ||
| High school or lower | 85 (12.6) | Boy | 354 (52.5) |
| College or above | 589 (87.4) | Girl | 320 (47.5) |
| Mother passive smoke during pregnancy | Feeding Type (0–6 months) | ||
| Yes | 196 (29.2) | Formula feeding | 73 (12.7) |
| No | 475 (70.8) | Exclusive Breastfeeding | 204 (35.5) |
| Maternal prepregnancy BMI (kg/m2) categories | Mixed breastfeeding | 297 (51.7) | |
| <18.5 | 120 (17.8) | Children passive smoking | |
| 18.5–23.9 | 443 (65.8) | No | 317 (48.2) |
| 24–27.9 | 89 (13.2) | Yes | 341 (51.8) |
| >28 | 21 (3.1) | Child anthropometric measures at 2 years (n = 451) | |
| Gestational Weight Gain | Child age, months | 23.8 ± 0.5 | |
| Adequate | 256 (38.4) | Length | 88.8 ± 3.0 |
| Excessive | 308 (46.2) | Weight | 12.8 ± 1.5 |
| Inadequate | 103 (15.4) | BMI (kg/m2) | 16.2 ± 1.4 |
| GDM | Weight for length z-score (ZWFL) | 0.37 ± 0.96 | |
| no | 588 (87.5) | BMI for age z-score | 0.37 ± 0.98 |
| yes | 84 (12.5) | Length for age z-score | 0.58 ± 0.94 |
| Mode of Delivery | Weight for age z-score | 0.60 ± 0.91 | |
| Vaginal delivery | 185 (27.4) | Sum of skinfold thickness (mm) | 22.8 ± 5.1 |
| C-Section | 489 (72.6) | Mid-Upper Arm Circumference (MUAC) (cm) | 15.8 ± 1.2 |
| 0–6 Months | 7–25 Months | ||||
|---|---|---|---|---|---|
| Maternal OWO | BWT-for-GA Tertile | β (95% CI) | p | β (95% CI) | p |
| Length (cm) | |||||
| No | 1st (low) | Ref. | Ref. | ||
| 2nd (medium) | 0.63 (0.38, 0.88) | <0.00001 | 1.15 (0.71, 1.58) | <0.00001 | |
| 3rd (high) | 1.02 (0.75, 1.28) | <0.00001 | 1.18 (0.70, 1.66) | <0.00001 | |
| Yes | 1st (low) | −0.02 (−0.47, 0.43) | 0.94 | −0.09 (−0.864, 0.693) | 0.83 |
| 2nd (medium) | 0.52 (0.04, 0.99) | 0.03 | 0.71 (−0.103, 1.527) | 0.09 | |
| 3rd (high) | 1.00 (0.62, 1.38) | <0.00001 | 1.04 (0.33, 1.74) | 0.004 | |
| Weight (kg) | |||||
| Maternal OWO | BWT-for-GA tertile | ||||
| No | 1st (low) | Ref. | Ref. | ||
| 2nd (medium) | 0.26 (0.17, 0.35) | <0.00001 | 0.30 (0.11, 0.50) | 0.003 | |
| 3rd (high) | 0.48 (0.39, 0.58) | <0.00001 | 0.49 (0.28, 0.69) | <0.00001 | |
| Yes | 1st (low) | 0.13 (−0.01, 0.28) | 0.07 | 0.11 (−0.22, 0.45) | 0.52 |
| 2nd (medium) | 0.40 (0.21, 0.58) | 0.00004 | 0.39 (−0.10, 0.88) | 0.12 | |
| 3rd (high) | 0.48 (0.32, 0.63) | <0.00001 | 0.87 (0.45, 1.29) | <0.0001 | |
| Weight-for-length z-score (ZWFL) | |||||
| Maternal OWO | BWT-for-GA tertile | ||||
| No | 1st (low) | Ref. | Ref. | ||
| 2nd (medium) | 0.29 (0.16, 0.43) | <0.0001 | 0.05 (−0.11, 0.21) | 0.50 | |
| 3rd (high) | 0.56 (0.42, 0.71) | <0.0001 | 0.24 (0.08, 0.39) | 0.003 | |
| Yes | 1st (low) | 0.21 (−0.02, 0.45) | 0.08 | 0.14 (−0.11, 0.40) | 0.27 |
| 2nd (medium) | 0.52 (0.30, 0.74) | <0.0001 | 0.21 (−0.13, 0.56) | 0.23 | |
| 3rd (high) | 0.55 (0.35, 0.75) | <0.0001 | 0.62 (0.31, 0.93) | <0.0001 | |
| Child Anthropometric Measures at Age 2 Years in AGA Children | ||||||||
|---|---|---|---|---|---|---|---|---|
| n | Mean ± SD | β (95% CI) | p | Mean ± SD | β (95% CI) | p | ||
| Maternal OWO | BWT-for-GA tertile | Sum of skinfold thickness (mm) | Mid-Upper Arm Circumference (MUAC) (cm) | |||||
| No | 1st (low) | 133 | 22.8 ± 4.4 | Ref. | 15.7 ± 1.1 | Ref. | ||
| 2nd (medium) | 128 | 21.8 ± 4.6 | −1.1 (−2.2, 0.1) | 0.08 | 15.7 ± 1.1 | −0.01 (−0.3, 0.3) | 0.95 | |
| 3rd (high) | 116 | 22.2 ± 4.3 | −0.6 (−1.8, 0.6) | 0.37 | 15.8 ± 1.1 | 0.1 (−0.2, 0.4) | 0.34 | |
| Yes | 1st (low) | 19 | 24.0 ± 3.7 | 1.5 (−0.9, 3.8) | 0.22 | 15.8 ± 1 | 0.1 (−0.5, 0.6) | 0.75 |
| 2nd (medium) | 16 | 25.9 ± 6.7 | 3.1 (0.6, 5.6) | 0.01 | 16.4 ± 1.4 | 0.7 (0.1, 1.3) | 0.02 | |
| 3rd (high) | 34 | 26.7 ± 8.4 | 4.1 (2.2, 5.9) | <0.0001 | 17.0 ± 2.0 | 1.3 (0.8, 1.7) | <0.0001 | |
| Weight (kg) | Weight-for-length z-score (ZWFL) | |||||||
| Maternal OWO | BWT-for-GA tertile | |||||||
| No | 1st (low) | 133 | 12.3 ± 1.3 | Ref. | 0.19 ± 0.84 | Ref. | ||
| 2nd (medium) | 130 | 12.7 ± 1.3 | 0.4 (0.06, 0.7) | 0.02 | 0.22 ± 0.97 | 0.03 (−0.20, 0.25) | 0.82 | |
| 3rd (high) | 118 | 13.0 ± 1.3 | 0.7 (0.4, 1.0) | <0.0001 | 0.46 ± 0.82 | 0.27 (0.04, 0.50) | 0.02 | |
| Yes | 1st (low) | 19 | 12.6 ± 1.3 | 0.3 (−0.4, 1.0) | 0.36 | 0.43 ± 0.76 | 0.25 (−0.20, 0.70) | 0.28 |
| 2nd (medium) | 16 | 13.3 ± 1.9 | 1.1 (0.4, 1.8) | 0.003 | 0.84 ± 0.97 | 0.65 (0.17, 1.14) | 0.01 | |
| 3rd (high) | 34 | 13.9 ± 2.3 | 1.5 (1.0, 2.0) | <0.0001 | 1.09 ± 1.42 | 0.89 (0.54, 1.24) | <0.0001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ouyang, F.; Wang, X.; Wells, J.C.; Wang, X.; Shen, L.; Zhang, J. Maternal Pre-Pregnancy Nutritional Status and Infant Birth Weight in Relation to 0–2 Year-Growth Trajectory and Adiposity in Term Chinese Newborns with Appropriate Birth Weight-for-Gestational Age. Nutrients 2023, 15, 1125. https://doi.org/10.3390/nu15051125
Ouyang F, Wang X, Wells JC, Wang X, Shen L, Zhang J. Maternal Pre-Pregnancy Nutritional Status and Infant Birth Weight in Relation to 0–2 Year-Growth Trajectory and Adiposity in Term Chinese Newborns with Appropriate Birth Weight-for-Gestational Age. Nutrients. 2023; 15(5):1125. https://doi.org/10.3390/nu15051125
Chicago/Turabian StyleOuyang, Fengxiu, Xiaobin Wang, Jonathan C. Wells, Xia Wang, Lixiao Shen, and Jun Zhang. 2023. "Maternal Pre-Pregnancy Nutritional Status and Infant Birth Weight in Relation to 0–2 Year-Growth Trajectory and Adiposity in Term Chinese Newborns with Appropriate Birth Weight-for-Gestational Age" Nutrients 15, no. 5: 1125. https://doi.org/10.3390/nu15051125