
Effect of Vitamin E Supplementation on Chronic Insomnia Disorder in Postmenopausal Women: A Prospective, Double-Blinded Randomized Controlled Trial
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Sample Size Calculation
2.4. Randomization, Blinding, and the Study Protocol
2.5. Data Collection and Measurements
2.6. Statistical Analysis
2.7. Ethical Approval
3. Results
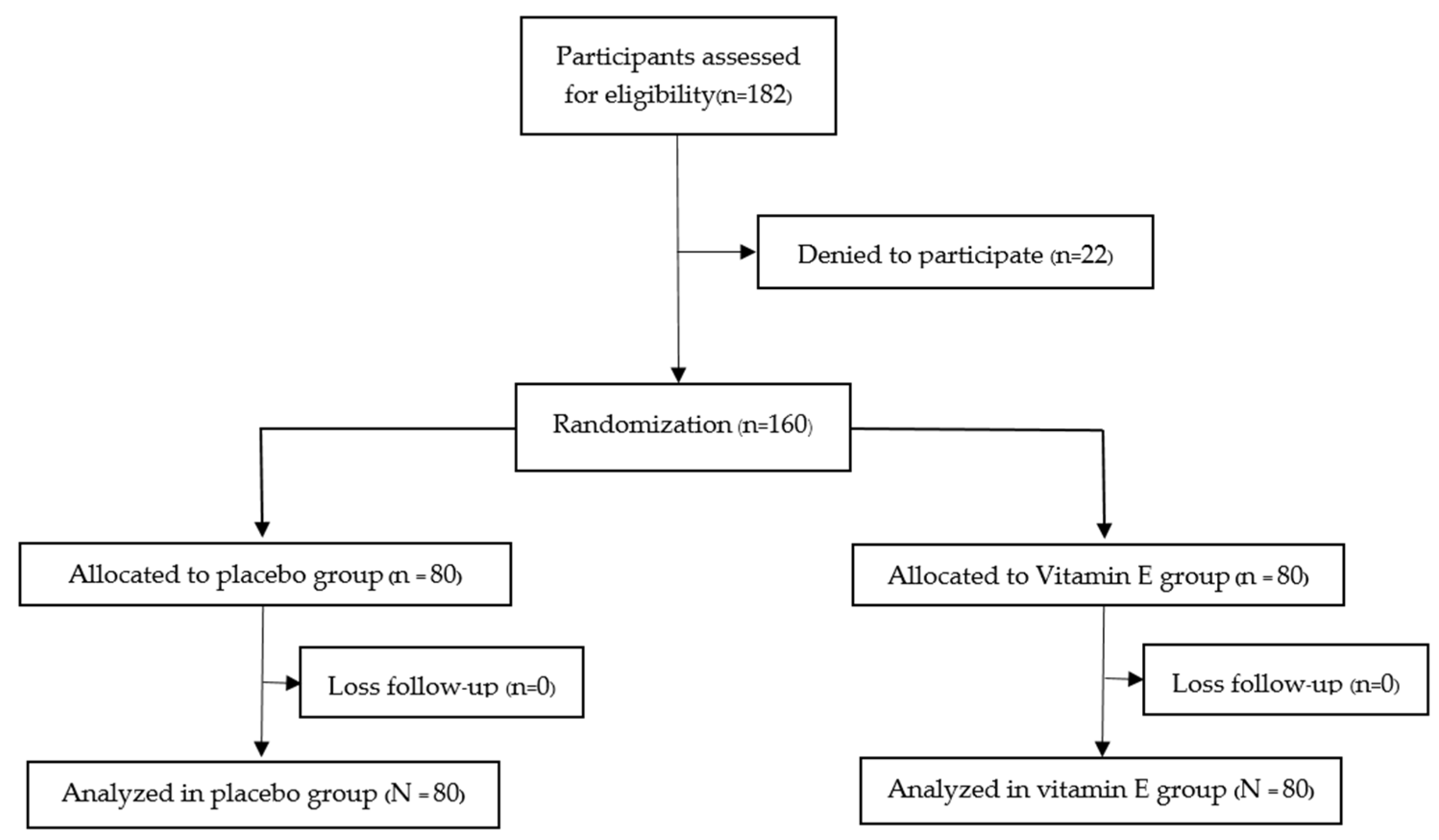
3.1. Protocol Flow Diagram
3.2. Main Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gold, E.B. The Timing of the Age at Which Natural Menopause Occurs. Obstet. Gynecol. Clin. N. Am. 2011, 38, 425–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Institute for Population and Social Research, Mahidol UniversityMahidol. Population Gazette. Available online: https://pr.mahidol.ac.th/ipsrbeta/en/Gazette.aspx (accessed on 1 October 2022).
- Santoro, N.; Epperson, C.N.; Mathews, S.B. Menopausal Symptoms and Their Management. Endocrinol. Metab. Clin. N. Am. 2015, 44, 497–515. [Google Scholar] [CrossRef] [Green Version]
- Riemann, D.; Baglioni, C.; Bassetti, C.; Bjorvatn, B.; Groselj, L.D.; Ellis, J.G.; Espie, C.A.; Garcia-Borreguero, D.; Gjerstad, M.; Gonçalves, M.; et al. European guideline for the diagnosis and treatment of insomnia. J. Sleep Res. 2017, 26, 675–700. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.; Steinberg, J.; Patel, P. Insomnia in the Elderly: A Review. J. Clin. Sleep Med. 2018, 14, 1017–1024. [Google Scholar] [CrossRef] [Green Version]
- Ohayon, M.M. Epidemiology of insomnia: What we know and what we still need to learn. Sleep Med. Rev. 2002, 6, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Joffe, H.; Massler, A.; Sharkey, K. Evaluation and Management of Sleep Disturbance during the Menopause Transition. Semin. Reprod. Med. 2010, 28, 404–421. [Google Scholar] [CrossRef] [Green Version]
- Pengo, M.; Won, C.H.; Bourjeily, G. Sleep in Women Across the Life Span. Chest 2018, 154, 196–206. [Google Scholar] [CrossRef]
- Young, T.; Rabago, D.; Zgierska, A.; Austin, D.; Finn, L. Objective and Subjective Sleep Quality in Premenopausal, Perimenopausal, and Postmenopausal Women in the Wisconsin Sleep Cohort Study. Sleep 2003, 26, 667–672. [Google Scholar] [CrossRef]
- Xu, M.; Bélanger, L.; Ivers, H.; Guay, B.; Zhang, J.; Morin, C.M. Comparison of subjective and objective sleep quality in menopausal and non-menopausal women with insomnia. Sleep Med. 2011, 12, 65–69. [Google Scholar] [CrossRef]
- Ge, L.; Guyatt, G.; Tian, J.; Pan, B.; Chang, Y.; Chen, Y.; Li, H.; Zhang, J.; Li, Y.; Ling, J.; et al. Insomnia and risk of mortality from all-cause, cardiovascular disease, and cancer: Systematic review and meta-analysis of prospective cohort studies. Sleep Med. Rev. 2019, 48, 101215. [Google Scholar] [CrossRef]
- Attarian, H.; Hachul, H.; Guttuso, T.; Phillips, B. Treatment of chronic insomnia disorder in menopause: Evaluation of literature. Menopause 2015, 22, 674–684. [Google Scholar] [CrossRef]
- Parthasarathy, S.; Vasquez, M.M.; Halonen, M.; Bootzin, R.; Quan, S.F.; Martinez, F.D.; Guerra, S. Persistent Insomnia is Associated with Mortality Risk. Am. J. Med. 2014, 128, 268–275.e2. [Google Scholar] [CrossRef] [Green Version]
- Sivertsen, B.; Pallesen, S.; Glozier, N.; Bjorvatn, B.; Salo, P.; Tell, G.S.; Ursin, R.; Øverland, S. Midlife insomnia and subsequent mortality: The Hordaland health study. BMC Public Health 2014, 15, 720. [Google Scholar] [CrossRef] [Green Version]
- Kay-Stacey, M.; Attarian, H. Advances in the management of chronic insomnia. BMJ 2016, 354, i2123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciano, C.; King, T.S.; Wright, R.R.; Perlis, M.; Sawyer, A.M. Longitudinal Study of Insomnia Symptoms Among Women During Perimenopause. J. Obstet. Gynecol. Neonatal Nurs. 2017, 46, 804–813. [Google Scholar] [CrossRef] [PubMed]
- Punyahotra, S.; Dennerstein, L.; Lehert, P. Menopausal experiences of Thai women. Part 1: Symptoms and their correlates. Maturitas 1997, 26, 1–7. [Google Scholar] [CrossRef]
- Yazdi, Z.; Sadeghniiat-Haghighi, K.; Ziaee, A.; Elmizadeh, K.; Ziaeeha, M. Influence of Sleep Disturbances on Quality of Life of Iranian Menopausal Women. Psychiatry J. 2013, 2013, 907068. [Google Scholar] [CrossRef] [Green Version]
- Lloret, A.; Esteve, D.; Lloret, M.A.; Monllor, P.; López, B.; León, J.L.; Cervera-Ferri, A. Is Oxidative Stress the Link Between Cerebral Small Vessel Disease, Sleep Disruption, and Oligodendrocyte Dysfunction in the Onset of Alzheimer’s Disease? Front. Physiol. 2021, 25, 708061. [Google Scholar] [CrossRef]
- Atrooz, F.; Salim, S. Sleep deprivation, oxidative stress and inflammation. Adv. Protein. Chem. Struct. Biol. 2020, 119, 309–336. [Google Scholar] [PubMed]
- Islam, M.T. Oxidative stress and mitochondrial dysfunction-linked neurodegenerative disorders. Neurol. Res. 2017, 39, 73–82. [Google Scholar] [CrossRef]
- El-Helaly, M.; Abu-Hashem, E. Oxidative stress, melatonin level, and sleep insufficiency among electronic equipment repairers. Indian J. Occup. Environ. Med. 2010, 14, 66–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gulec, M.; Ozkol, H.; Selvi, Y.; Tuluce, Y.; Aydin, A.; Besiroglu, L.; Ozdemir, P.G. Oxidative stress in patients with primary insomnia. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2012, 37, 247–251. [Google Scholar] [CrossRef]
- Feng, L.; Wu, H.-W.; Song, G.-Q.; Lu, C.; Li, Y.-H.; Qu, L.-N.; Chen, S.-G.; Liu, X.-M.; Chang, Q. Chronical sleep interruption-induced cognitive decline assessed by a metabolomics method. Behav. Brain Res. 2016, 302, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Azzi, A. Tocopherols, tocotrienols and tocomonoenols: Many similar molecules but only one vitamin E. Redox Biol. 2019, 26, 101259. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Panel on Dietary Antioxidants and Related Compounds. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids; National Academies Press: Washington, DC, USA, 2000. [Google Scholar]
- Ziaei, S.; Kazemnejad, A.; Zareai, M. The Effect of Vitamin E on Hot Flashes in Menopausal Women. Gynecol. Obstet. Investig. 2007, 64, 204–207. [Google Scholar] [CrossRef] [PubMed]
- Vallibhakara, S.A.-O.; Nakpalat, K.; Sophonsritsuk, A.; Tantitham, C.; Vallibhakara, O. Effect of Vitamin E Supplement on Bone Turnover Markers in Postmenopausal Osteopenic Women: A Double-Blind, Randomized, Placebo-Controlled Trial. Nutrients 2021, 13, 4226. [Google Scholar] [CrossRef]
- Guralp, O. Effects of vitamin E on bone remodeling in perimenopausal women: Mini review. Maturitas 2014, 79, 476–480. [Google Scholar] [CrossRef] [PubMed]
- Ochi, H.; Takeda, S. The Two Sides of Vitamin E Supplementation. Gerontology 2014, 61, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Abner, E.L.; Schmitt, F.A.; Mendiondo, M.S.; Marcum, J.; Kryscio, R.J. Vitamin E and All-Cause Mortality: A Meta-Analysis. Curr. Aging Sci. 2011, 4, 158–170. [Google Scholar] [CrossRef]
- Mustapha, M.; Nassir, C.M.N.C.M.; Hay, Y.K.; Yee, F.W.; Hamid, H.A. Neuroprotective Potentials of Natural Vitamin E for Cerebral Small Vessel Disease. In Neuroprotection—New Approaches and Prospects; Otero-Losada, M., Capani, F., Lloret, S.P., Eds.; IntechOpen: London, UK, 2020. [Google Scholar]
- Jain, S.K.; McVie, R.; Smith, T. Vitamin E supplementation restores glutathione and malondialdehyde to normal concentrations in erythrocytes of type 1 diabetic children. Diabetes Care 2000, 23, 1389–1394. [Google Scholar] [CrossRef] [Green Version]
- Bergin, P.; Leggett, A.; Cardwell, C.R.; Woodside, J.V.; Thakkinstian, A.; Maxwell, A.P.; McKay, G.J. The effects of vitamin E supplementation on malondialdehyde as a biomarker of oxidative stress in haemodialysis patients: A systematic review and meta-analysis. BMC Nephrol. 2021, 22, 126. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds CF 3rd Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Sitasuwan, T.; Bussaratid, S.; Ruttanaumpawan, P.; Chotinaiwattarakul, W. Reliability and validity of the Thai version of the Pittsburgh Sleep Quality Index. J. Med. Assoc. Thail. 2014, 97 (Suppl. S3), S57–S67. [Google Scholar]
- Lichstein, K.L.; Payne, K.L.; Soeffing, J.P.; Durrence, H.H.; Taylor, D.J.; Riedel, B.W.; Bush, A.J. Vitamins and sleep: An exploratory study. Sleep Med. 2007, 9, 27–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ngamjarus, C. n4Studies: Sample Size Calculation for an Epidemiological Study on a Smart Device. Siriraj Med. J. 2016, 68, 160–170. [Google Scholar]
- Proserpio, P.; Marra, S.; Campana, C.; Agostoni, E.C.; Palagini, L.; Nobili, L.; Nappi, R.E. Insomnia and menopause: A narrative review on mechanisms and treatments. Climacteric 2020, 23, 539–549. [Google Scholar] [CrossRef]
- Taavoni, S.; Ekbatani, N.; Kashaniyan, M.; Haghani, H. Effect of valerian on sleep quality in postmenopausal women: A randomized placebo-controlled clinical trial. Menopause 2011, 18, 951–955. [Google Scholar] [CrossRef]
- Hachul, H.; Brandão, L.C.; D’Almeida, V.; Bittencourt, L.; Baracat, E.C.; Tufik, S. Isoflavones decrease insomnia in postmenopause. Menopause 2011, 18, 178–184. [Google Scholar] [CrossRef]
- Alzoubi, K.H.; Khabour, O.F.; Rashid, B.A.; Damaj, I.M.; Salah, H.A. The neuroprotective effect of vitamin E on chronic sleep deprivation-induced memory impairment: The role of oxidative stress. Behav Brain Res. 2012, 226, 205–210. [Google Scholar] [CrossRef]
- Ikonte, C.J.; Mun, J.G.; Reider, C.A.; Grant, R.W.; Mitmesser, S.H. Micronutrient Inadequacy in Short Sleep: Analysis of the NHANES 2005–2016. Nutrients 2019, 11, 2335. [Google Scholar] [CrossRef] [Green Version]
- Prueksaritanond, S.; Tubtimtes, S.; Pumkompol, T.; Sukying, C. Psychotropic drug prescribing in the family medicine out-patient clinic, Ramathibodi Hospital. J. Med Assoc. Thail. 2009, 92, 266–272. [Google Scholar]
- Herzig, S.J.; Rothberg, M.B.; Moss, C.R.; Maddaleni, G.; Bertisch, S.M.; Wong, J.; Zhou, W.; Ngo, L.; Anderson, T.S.; Gurwitz, J.H.; et al. Risk of in-hospital falls among medications commonly used for insomnia in hospitalized patients. Sleep 2021, 44, zsab064. [Google Scholar] [CrossRef] [PubMed]
- Aljawadi, M.H.; Khoja, A.T.; Alhammad, A.M.; AlOtaibi, A.D.; Al-Shammari, S.A.; Khoja, T.A. The prevalence of benzodiazepines utilization and its association with falls among Saudi older adults; results from the Saudi national survey for elderly Health (SNSEH). Saudi Pharm. J. 2018, 26, 1112–1119. [Google Scholar] [CrossRef] [PubMed]
- Richardson, J.K.; Eckner, J.T.; Kim, H.; Ashton-Miller, J.A. A clinical method of evaluating simple reaction time and reaction accuracy is sensitive to a single dose of lorazepam. J. Psychopharmacol. 2020, 34, 920–925. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Vitamin E (N = 80) | Placebo (N = 80) |
|---|---|---|
| Age (years) b | 57 (53, 59) | 55 (52, 60) |
| Body mass index (kg/m2) b | 23.4 (20.7, 25.8) | 22.9 (21.4, 25.9) |
| Age at menopause (years) a | 50.4 ± 3 | 49.7 ± 2.7 |
| Years since menopause (years) a | 6.8 ± 5.4 | 7.1 ± 5.3 |
| Type of menopause c | ||
| Natural | 63 (78.75%) | 69 (86.25%) |
| Surgical | 17 (21.25%) | 11 (13.75%) |
| Marital status c | ||
| Single | 12 (15%) | 15 (18.75%) |
| Married | 51 (63.75%) | 55 (68.75%) |
| Divorced or widowed | 17 (21.25%) | 10 (12.5%) |
| Number of children c | ||
| 0 | 17 (21.25%) | 20 (25%) |
| 1 | 25 (31.25%) | 18 (22.5%) |
| ≥2 | 38 (47.5%) | 42 (52.5%) |
| Education c | ||
| Primary school | 4 (5%) | 9 (11.25%) |
| High school | 23 (28.75%) | 23 (28.75%) |
| Bachelor’s degree or higher | 53 (66.25%) | 48 (60%) |
| Underlying diseases c | ||
| Yes | 35 (43.75%) | 38 (47.5%) |
| No | 45 (56.25%) | 42 (52.5%) |
| Sedative drug used c | 24 (30%) | 14 (17.5%) |
| Caffeine consumption c | ||
| <3 drinks per week | 6 (7.5%) | 11 (13.75%) |
| >3 drinks per week | 19 (23.75%) | 17 (21.25%) |
| Financial status c | ||
| Bad | 3 (3.75%) | 6 (7.5%) |
| Fair | 61 (76.25%) | 62 (77.5%) |
| Good | 16 (20%) | 12 (15%) |
| PSQI Score | Vitamin E (N = 80) | Placebo (N = 80) | p-Value |
|---|---|---|---|
| Before | 13 (6, 20) | 11 (6, 20) | 0.019 |
| After | 6 (1, 18) | 9 (1, 19) | 0.012 |
| Improvement of PSQI | 5 (−6, 14) | 1 (−5, 13) | <0.001 |
| Sedative Drug Used | Vitamin E | Placebo |
|---|---|---|
| Before | 24 (30%) | 14 (17.5%) |
| After | 12 (15%) | 8 (10%) |
| p-Value | 0.009 | 0.077 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thongchumnum, W.; Vallibhakara, S.A.-O.; Sophonsritsuk, A.; Vallibhakara, O. Effect of Vitamin E Supplementation on Chronic Insomnia Disorder in Postmenopausal Women: A Prospective, Double-Blinded Randomized Controlled Trial. Nutrients 2023, 15, 1187. https://doi.org/10.3390/nu15051187
Thongchumnum W, Vallibhakara SA-O, Sophonsritsuk A, Vallibhakara O. Effect of Vitamin E Supplementation on Chronic Insomnia Disorder in Postmenopausal Women: A Prospective, Double-Blinded Randomized Controlled Trial. Nutrients. 2023; 15(5):1187. https://doi.org/10.3390/nu15051187
Chicago/Turabian StyleThongchumnum, Wirun, Sakda Arj-Ong Vallibhakara, Areepan Sophonsritsuk, and Orawin Vallibhakara. 2023. "Effect of Vitamin E Supplementation on Chronic Insomnia Disorder in Postmenopausal Women: A Prospective, Double-Blinded Randomized Controlled Trial" Nutrients 15, no. 5: 1187. https://doi.org/10.3390/nu15051187