
Association between Meal Frequency and Type 2 Diabetes Mellitus in Rural Adults: A Large-Scale Cross-Sectional Study

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Assessment of Meal Frequency
2.3. Definition of T2DM
2.4. Covariates Estimate
2.5. Statistical Analysis
3. Results
3.1. Basic Characteristics of Participants
3.2. Association between the Weekly Total Meal Frequency and T2DM
3.3. Association between the Weekly Frequency of Breakfast, Lunch, and Dinner and T2DM
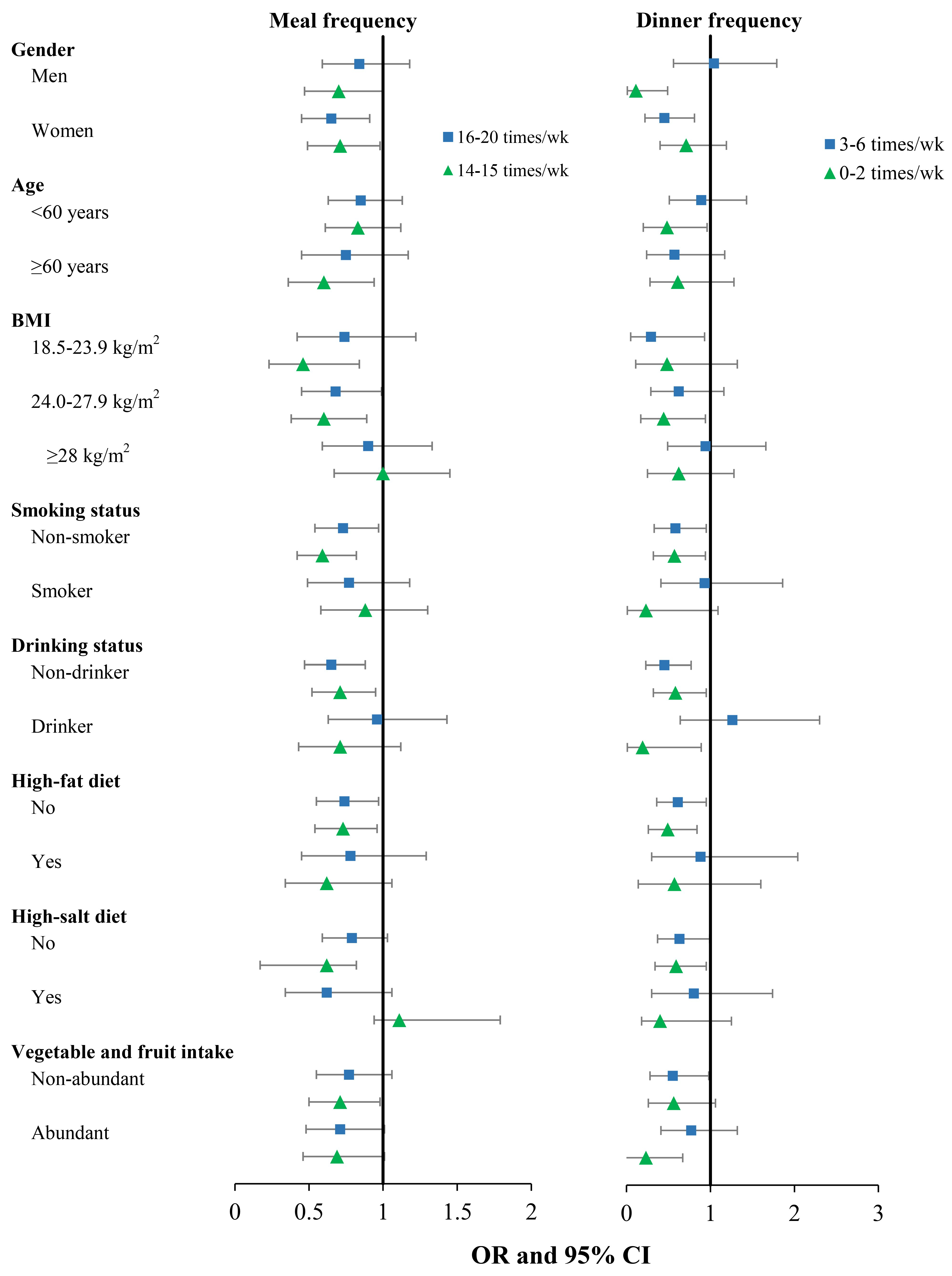
3.4. Stratified Analysis
4. Discussion
5. Conclusions
- Dietary behaviors as a modifiable factor might have potential effects on metabolic health.
- Previous studies have shown that reducing diet frequency (including intermittent fasting, calorie restriction) and then extending the fasting period might have beneficial effects on health conditions.
- Evidence on the health effects of intermittent fasting or calorie restriction comes mainly from a few experimental studies with a small sample and short duration.
- General population-based evidence of reducing diet frequency was still limited and inconclusive, especially lacking evidence from low and middle-income areas.
- Intermittent reduction in meal frequency was associated with a lower prevalence of T2DM.
- Moderating the frequency of dinner might reduce the risk of T2DM.
- Those associations were significant among participants with relatively healthy lifestyles.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| T2DM: | type 2 diabetes mellitus |
| FBG: | fasting blood glucose |
| IDF: | International Diabetes Federation |
| FFQ: | food frequency questionnaire |
| IPAQ: | International Physical Activity Questionnaire |
| BMI: | body mass index |
| SD: | standard deviation |
| ORs: | odds ratios |
| 95%CIs: | 95% confidence intervals |
| RR: | risk ratio |
| IF: | intermittent fasting |
| TRE: | time-restricted eating patterns |
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- Safiri, S.; Karamzad, N.; Kaufman, J.S.; Bell, A.W.; Nejadghaderi, S.A.; Sullman, M.J.M.; Moradi-Lakeh, M.; Collins, G.; Kolahi, A.-A. Prevalence, Deaths and Disability-Adjusted-Life-Years (DALYs) Due to Type 2 Diabetes and Its Attributable Risk Factors in 204 Countries and Territories, 1990–2019: Results from the Global Burden of Disease Study 2019. Front. Endocrinol. 2022, 13, 838027. [Google Scholar] [CrossRef]
- Wang, L.; Peng, W.; Zhao, Z.; Zhang, M.; Shi, Z.; Song, Z.; Zhang, X.; Li, C.; Huang, Z.; Sun, X.; et al. Prevalence and Treatment of Diabetes in China, 2013–2018. JAMA 2021, 326, 2498–2506. [Google Scholar] [CrossRef]
- Liu, X.; Li, Y.; Li, L.; Zhang, L.; Ren, Y.; Zhou, H.; Cui, L.; Mao, Z.; Hu, D.; Wang, C. Prevalence, awareness, treatment, control of type 2 diabetes mellitus and risk factors in Chinese rural population: The RuralDiab study. Sci. Rep. 2016, 6, 31426. [Google Scholar] [CrossRef]
- Mattson, M.P.; Allison, D.B.; Fontana, L.; Harvie, M.; Longo, V.D.; Malaisse, W.J.; Mosley, M.; Notterpek, L.; Ravussin, E.; Scheer, F.A.; et al. Meal frequency and timing in health and disease. Proc. Natl. Acad. Sci. USA 2014, 111, 16647–16653. [Google Scholar] [CrossRef]
- Wang, X.W.; Hu, Y.H.; Qin, L.Q.; Dong, J.Y. Meal frequency and incidence of type 2 diabetes: A prospective study. Brit. J. Nutr. 2021, 128, 273–278. [Google Scholar] [CrossRef]
- Mekary, R.A.; Giovannucci, E.; Willett, W.C.; van Dam, R.M.; Hu, F.B. Eating patterns and type 2 diabetes risk in men: Breakfast omission, eating frequency, and snacking. Am. J. Clin. Nutr. 2012, 95, 1182–1189. [Google Scholar] [CrossRef]
- Papakonstantinou, E.; Kontogianni, M.D.; Mitrou, P.; Magriplis, E.; Vassiliadi, D.; Nomikos, T.; Lambadiari, V.; Georgousopoulou, E.; Dimitriadis, G. Effects of 6 vs. 3 eucaloric meal patterns on glycaemic control and satiety in people with impaired glucose tolerance or overt type 2 diabetes: A randomized trial. Diabetes Metab. 2018, 44, 226–234. [Google Scholar] [CrossRef]
- Yoshida, J.; Eguchi, E.; Nagaoka, K.; Ito, T.; Ogino, K. Association of night eating habits with metabolic syndrome and its components: A longitudinal study. BMC Public Health 2018, 18, 1366. [Google Scholar] [CrossRef]
- Hermenegildo-López, Y.; Donat-Vargas, C.; Sandoval-Insausti, H.; Moreno-Franco, B.; Rodríguez-Ayala, M.; Rey-García, J.; Banegas, J.R.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. A Higher Intake of Energy at Dinner Is Associated with Incident Metabolic Syndrome: A Prospective Cohort Study in Older Adults. Nutrients 2021, 13, 3035. [Google Scholar] [CrossRef] [PubMed]
- Paoli, A.; Tinsley, G.; Bianco, A.; Moro, T. The Influence of Meal Frequency and Timing on Health in Humans: The Role of Fasting. Nutrients 2019, 11, 719. [Google Scholar] [CrossRef] [PubMed]
- Hutchison, A.T.; Heilbronn, L.K. Metabolic impacts of altering meal frequency and timing—Does when we eat matter? Biochimie 2016, 124, 187–197. [Google Scholar] [CrossRef]
- Di Francesco, A.; Di Germanio, C.; Bernier, M.; de Cabo, R. A time to fast. Science 2018, 362, 770–775. [Google Scholar] [CrossRef]
- Mekary, R.A.; Giovannucci, E.; Cahill, L.; Willett, W.C.; van Dam, R.M.; Hu, F.B. Eating patterns and type 2 diabetes risk in older women: Breakfast consumption and eating frequency. Am. J. Clin. Nutr. 2013, 98, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Neuhouser, M.L.; Wertheim, B.C.; Perrigue, M.M.; Hingle, M.; Tinker, L.F.; Shikany, J.M.; Johnson, K.C.; Waring, M.E.; Seguin-Fowler, R.A.; Vitolins, M.Z.; et al. Associations of Number of Daily Eating Occasions with Type 2 Diabetes Risk in the Women’s Health Initiative Dietary Modification Trial. Curr. Dev. Nutr. 2020, 4, nzaa126. [Google Scholar] [CrossRef] [PubMed]
- Yaribeygi, H.; Atkin, S.L.; Ramezani, M.; Sahebkar, A. A review of the molecular pathways mediating the improvement in diabetes mellitus following caloric restriction. J. Cell. Physiol. 2019, 234, 8436–8442. [Google Scholar] [CrossRef]
- Caristia, S.; Vito, M.; Sarro, A.; Leone, A.; Pecere, A.; Zibetti, A.; Filigheddu, N.; Zeppegno, P.; Prodam, F.; Faggiano, F.; et al. Is Caloric Restriction Associated with Better Healthy Aging Outcomes? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2020, 12, 2290. [Google Scholar] [CrossRef]
- de Cabo, R.; Mattson, M.P. Effects of Intermittent Fasting on Health, Aging, and Disease. N. Engl. J. Med. 2019, 381, 2541–2551. [Google Scholar] [CrossRef]
- Vasim, I.; Majeed, C.N.; DeBoer, M.D. Intermittent Fasting and Metabolic Health. Nutrients 2022, 14, 631. [Google Scholar] [CrossRef]
- Cho, Y.; Hong, N.; Kim, K.W.; Cho, S.J.; Lee, M.; Lee, Y.H.; Lee, Y.H.; Kang, E.S.; Cha, B.S.; Lee, B.W. The Effectiveness of Intermittent Fasting to Reduce Body Mass Index and Glucose Metabolism: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 1645. [Google Scholar] [CrossRef] [PubMed]
- Dong, T.A.; Sandesara, P.B.; Dhindsa, D.S.; Mehta, A.; Arneson, L.C.; Dollar, A.L.; Taub, P.R.; Sperling, L.S. Intermittent Fasting: A Heart Healthy Dietary Pattern? Am. J. Med. 2020, 133, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Morales-Suarez-Varela, M.; Collado Sánchez, E.; Peraita-Costa, I.; Llopis-Morales, A.; Soriano, J.M. Intermittent Fasting and the Possible Benefits in Obesity, Diabetes, and Multiple Sclerosis: A Systematic Review of Randomized Clinical Trials. Nutrients 2021, 13, 3179. [Google Scholar] [CrossRef] [PubMed]
- Zang, B.Y.; He, L.X.; Xue, L. Intermittent Fasting: Potential Bridge of Obesity and Diabetes to Health? Nutrients 2022, 14, 981. [Google Scholar] [CrossRef] [PubMed]
- Varady, K.A.; Cienfuegos, S.; Ezpeleta, M.; Gabel, K. Cardiometabolic Benefits of Intermittent Fasting. Annu. Rev. Nutr. 2021, 41, 333–361. [Google Scholar] [CrossRef] [PubMed]
- Ulgherait, M.; Midoun, A.M.; Park, S.J.; Gatto, J.A.; Tener, S.J.; Siewert, J.; Klickstein, N.; Canman, J.C.; Ja, W.W.; Shirasu-Hiza, M. Circadian autophagy drives iTRF-mediated longevity. Nature 2021, 598, 353–358. [Google Scholar] [CrossRef]
- Liu, X.; Mao, Z.; Li, Y.; Wu, W.; Zhang, X.; Huo, W.; Yu, S.; Shen, L.; Li, L.; Tu, R.; et al. Cohort Profile: The Henan Rural Cohort: A prospective study of chronic non-communicable diseases. Int. J. Epidemiol. 2019, 48, 1756–1756j. [Google Scholar] [CrossRef]
- Xue, Y.; Yang, K.L.; Wang, B.Y.; Liu, C.; Mao, Z.X.; Yu, S.C.; Li, X.; Wang, Y.; Sun, H.L.; Wang, C.J.; et al. Reproducibility and validity of an FFQ in the Henan Rural Cohort Study. Public Health Nutr. 2020, 23, 34–40. [Google Scholar] [CrossRef]
- Huseinovic, E.; Winkvist, A.; Bertz, F.; Bertéus Forslund, H.; Brekke, H.K. Eating frequency, energy intake and body weight during a successful weight loss trial in overweight and obese postpartum women. Eur. J. Clin. Nutr. 2014, 68, 71–76. [Google Scholar] [CrossRef]
- Ohkawara, K.; Cornier, M.A.; Kohrt, W.M.; Melanson, E.L. Effects of increased meal frequency on fat oxidation and perceived hunger. Obesity 2013, 21, 336–343. [Google Scholar] [CrossRef]
- Perrigue, M.M.; Drewnowski, A.; Wang, C.Y.; Neuhouser, M.L. Higher Eating Frequency Does Not Decrease Appetite in Healthy Adults. J. Nutr. 2016, 146, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Higgins, K.A.; Hudson, J.L.; Hayes, A.M.R.; Braun, E.; Cheon, E.; Couture, S.C.; Gunaratna, N.S.; Hill, E.R.; Hunter, S.R.; McGowan, B.S.; et al. Systematic Review and Meta-Analysis on the Effect of Portion Size and Ingestive Frequency on Energy Intake and Body Weight among Adults in Randomized Controlled Feeding Trials. Adv. Nutr. 2022, 13, 248–268. [Google Scholar] [CrossRef] [PubMed]
- Varady, K.A. Meal frequency and timing: Impact on metabolic disease risk. Curr. Opin. Endocrinol. Diabetes Obes. 2016, 23, 379–383. [Google Scholar] [CrossRef] [PubMed]
- Mahdi, S.; Mazidi, M.; Davies, I.G.; Beigrezaei, S.; Mozaffari-Khosravi, H.; Mirzaei, M.; Lane, K.E.; Khayyatzadeh, S.S. Dietary habits are associated with the prevalence of type 2 diabetes: A study among a middle eastern population. J. Nutr. Sci. 2022, 11, E78. [Google Scholar] [CrossRef] [PubMed]
- Munoz-Hernandez, L.; Marquez-Lopez, Z.; Mehta, R.; Aguilar-Salinas, C.A. Intermittent Fasting as Part of the Management for T2DM: From Animal Models to Human Clinical Studies. Curr. Diabetes Rep. 2020, 20, 13. [Google Scholar] [CrossRef]
- Carew, A.S.; Mekary, R.A.; Kirkland, S.; Theou, O.; Siddiqi, F.; Urquhart, R.; George, M.; Blanchard, C.; Biggs, M.L.; Djoussé, L.; et al. Prospective study of breakfast frequency and timing and the risk of incident type 2 diabetes in community-dwelling older adults: The Cardiovascular Health Study. Am. J. Clin. Nutr. 2022, 116, 325–334. [Google Scholar] [CrossRef]
- Kahleova, H.; Belinova, L.; Malinska, H.; Oliyarnyk, O.; Trnovska, J.; Skop, V.; Kazdova, L.; Dezortova, M.; Hajek, M.; Tura, A.; et al. Eating two larger meals a day (breakfast and lunch) is more effective than six smaller meals in a reduced-energy regimen for patients with type 2 diabetes: A randomised crossover study. Diabetologia 2014, 57, 1552–1560. [Google Scholar] [CrossRef]
- Cienfuegos, S.; McStay, M.; Gabel, K.; Varady, K.A. Time restricted eating for the prevention of type 2 diabetes. J. Physiol. 2022, 600, 1253–1264. [Google Scholar] [CrossRef]
- Xie, Z.; Sun, Y.; Ye, Y.; Hu, D.; Zhang, H.; He, Z.; Zhao, H.; Yang, H.; Mao, Y. Randomized controlled trial for time-restricted eating in healthy volunteers without obesity. Nat. Commun. 2022, 13, 1003. [Google Scholar] [CrossRef]
- Ren, X.; Yang, X.; Jiang, H.; Han, T.; Sun, C. The association of energy and macronutrient intake at dinner vs. breakfast with the incidence of type 2 diabetes mellitus in a cohort study: The China Health and Nutrition Survey, 1997–2011. J. Diabetes 2021, 13, 882–892. [Google Scholar] [CrossRef]
- Han, T.; Gao, J.; Wang, L.; Li, C.; Qi, L.; Sun, C.; Li, Y. The Association of Energy and Macronutrient Intake at Dinner Versus Breakfast with Disease-Specific and All-Cause Mortality Among People With Diabetes: The, U.S. National Health and Nutrition Examination Survey, 2003–2014. Diabetes Care 2020, 43, 1442–1448. [Google Scholar] [CrossRef]
- Park, S.E.; Seo, M.H.; Cho, J.H.; Kwon, H.; Kim, Y.H.; Han, K.D.; Jung, J.H.; Park, Y.G.; Rhee, E.J.; Lee, W.Y. Dose-Dependent Effect of Smoking on Risk of Diabetes Remains after Smoking Cessation: A Nationwide Population-Based Cohort Study in Korea. Diabetes Metab. J. 2021, 45, 539–546. [Google Scholar] [CrossRef]
- Holst, C.; Becker, U.; Jørgensen, M.E.; Grønbæk, M.; Tolstrup, J.S. Alcohol drinking patterns and risk of diabetes: A cohort study of 70,551 men and women from the general Danish population. Diabetologia 2017, 60, 1941–1950. [Google Scholar] [CrossRef]
- Duan, Y.; Zeng, L.; Zheng, C.; Song, B.; Li, F.; Kong, X.; Xu, K. Inflammatory Links Between High Fat Diets and Diseases. Front. Immunol. 2018, 9, 2649. [Google Scholar] [CrossRef]
- Fang, M.; Hu, Z.F.; Feng, L.J. Association between dietary pattern and the risk of type 2 diabetes mellitus in Zhejiang Province, China: A case-control study. Asia Pac. J. Clin. Nutr. 2020, 29, 821–826. [Google Scholar]
- Monteiro, R.; Azevedo, I. Chronic inflammation in obesity and the metabolic syndrome. Mediat. Inflamm. 2010, 2010, 289645. [Google Scholar] [CrossRef]
- Kumar, A.A.; Satheesh, G.; Vijayakumar, G.; Chandran, M.; Prabhu, P.R.; Simon, L.; Kutty, V.R.; Kartha, C.C.; Jaleel, A. Postprandial Metabolism is Impaired in Overweight Normoglycemic Young Adults without Family History of Diabetes. Sci. Rep. 2020, 10, 353. [Google Scholar] [CrossRef]
- Mattson, M.P.; Moehl, K.; Ghena, N.; Schmaedick, M.; Cheng, A.W. Intermittent metabolic switching, neuroplasticity and brain health. Nat. Rev. Neurosci. 2018, 19, 81–94. [Google Scholar] [CrossRef]
- Anton, S.D.; Moehl, K.; Donahoo, W.T.; Marosi, K.; Lee, S.A.; Mainous, A.G., 3rd; Leeuwenburgh, C.; Mattson, M.P. Flipping the Metabolic Switch: Understanding and Applying the Health Benefits of Fasting. Obesity 2018, 26, 254–268. [Google Scholar] [CrossRef]
- Mehrabani, S.; Bagherniya, M.; Askari, G.; Read, M.I.; Sahebkar, A. The effect of fasting or calorie restriction on mitophagy induction: A literature review. J. Cachexia Sarcopenia Muscle 2020, 11, 1447–1458. [Google Scholar] [CrossRef]
- Joaquim, L.; Faria, A.; Loureiro, H.; Matafome, P. Benefits, mechanisms, and risks of intermittent fasting in metabolic syndrome and type 2 diabetes. J. Physiol. Biochem. 2022, 78, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Bagherniya, M.; Butler, A.E.; Barreto, G.E.; Sahebkar, A. The effect of fasting or calorie restriction on autophagy induction: A review of the literature. Ageing Res. Rev. 2018, 47, 183–197. [Google Scholar] [CrossRef] [PubMed]
- Mattson, M.P.; Longo, V.D.; Harvie, M. Impact of intermittent fasting on health and disease processes. Ageing Res. Rev. 2017, 39, 46–58. [Google Scholar] [CrossRef]
- Mattson, M.P. Energy intake, meal frequency, and health: A neurobiological perspective. Annu. Rev. Nutr. 2005, 25, 237–260. [Google Scholar] [CrossRef] [PubMed]
- Savas, H.B.; Gultekin, F.; Ciris, I.M. Positive effects of meal frequency and calorie restriction on antioxidant systems in rats. North Clin. Istanb. 2017, 4, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Sutton, E.F.; Beyl, R.; Early, K.S.; Cefalu, W.T.; Ravussin, E.; Peterson, C.M. Early Time-Restricted Feeding Improves Insulin Sensitivity, Blood Pressure, and Oxidative Stress Even without Weight Loss in Men with Prediabetes. Cell Metab. 2018, 27, 1212–1221.e1213. [Google Scholar] [CrossRef] [PubMed]
- Chamorro, R.; Basfi-Fer, K.; Sepúlveda, B.; Farías, R.; Rojas, P.; Carrasco, F.; Codoceo, J.; Inostroza, J.; Ruz, M. Meal timing across the day modulates daily energy intake in adult patients with type 2 diabetes. Eur. J. Clin. Nutr. 2022, 76, 1470–1477. [Google Scholar] [CrossRef]
- Yu, D.; Zheng, W.; Cai, H.; Xiang, Y.B.; Li, H.; Gao, Y.T.; Shu, X.O. Long-term Diet Quality and Risk of Type 2 Diabetes Among Urban Chinese Adults. Diabetes Care 2018, 41, 723–730. [Google Scholar] [CrossRef]
- Mena, B.; Ashman, H.; Dunshea, F.R.; Hutchings, S.; Ha, M.; Warner, R.D. Exploring Meal and Snacking Behaviour of Older Adults in Australia and China. Foods 2020, 9, 426. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total (n = 29,405) | T2DM (n = 2585) | Non-T2DM (n = 26,820) | p-Value |
|---|---|---|---|---|
| Age (years) (mean ± SD) | 55.48 ± 12.32 | 60.37 ± 9.42 | 55.01 ± 12.47 | <0.001 a |
| Gender, n (%) | 0.060 b | |||
| Men | 12,022 (40.88) | 1012 (39.15) | 11,010 (41.05) | |
| Women | 17,383 (59.12) | 1573 (60.85) | 15,810 (58.95) | |
| Marital status, n (%) | 0.132 b | |||
| Married/cohabitating | 26,524 (90.2) | 2310 (89.36) | 24,214 (90.28) | |
| Unmarried/divorced/widowed | 2881 (9.80) | 275 (10.64) | 2606 (9.72) | |
| Average monthly income, n (%) | <0.001 b | |||
| <500 RMB | 10,607 (36.07) | 1030 (39.85) | 9577 (35.71) | |
| 500-RMB | 9278 (31.55) | 796 (30.79) | 8482 (31.63) | |
| 1000-RMB | 9520 (32.38) | 759 (29.36) | 8761 (32.67) | |
| Education level, n (%) | <0.001 b | |||
| Elementary school or below | 13,055 (44.40) | 1408 (54.47) | 11,647 (43.43) | |
| Junior high school | 11,431 (38.87) | 858 (33.19) | 10,573 (39.42) | |
| High school or above | 4919 (16.73) | 319 (12.34) | 4600 (17.15) | |
| Smoking status, n (%) | 0.002 b | |||
| Non-smokers | 21,150 (71.93) | 1928 (74.58) | 19,222 (71.67) | |
| Smokers | 8255 (28.07) | 657 (25.42) | 7598 (28.33) | |
| Drinking status, n (%) | 0.084 b | |||
| Non-drinkers | 22,819 (77.60) | 2041 (78.96) | 20,778 (77.47) | |
| Drinkers | 6586 (22.40) | 544 (21.04) | 6024 (22.53) | |
| Physical activity, n (%) | <0.001 b | |||
| Low | 9326 (31.72) | 971 (37.56) | 8355 (31.15) | |
| Moderate | 10,821 (36.80) | 865 (33.46) | 9956 (37.12) | |
| High | 9258 (31.48) | 749 (28.97) | 8509 (31.73) | |
| High-salt diet, n (%) | 4751 (16.16) | 435 (16.85) | 4316 (16.12) | 0.335 b |
| Abundant vegetable and fruit intake, n (%) | 14,097 (74.94) | 1117 (43.21) | 12,980 (48.40) | <0.001 b |
| High-fat diet, n (%) | 5343 (18.17) | 388 (15.01) | 4955 (18.48) | <0.001 b |
| BMI (kg/m2), (mean ± SD) | 24.73 ± 3.56 | 26.19 ± 3.67 | 24.59 ± 3.52 | <0.001 a |
| Total energy intake (kcal/d) | 2433.02 ± 676.15 | 2377.60 ± 682.41 | 2438.36 ± 675.32 | <0.001 a |
| Basal metabolic rate (KJ/m2/h) (mean ± SD) | 1378.39 ± 214.35 | 1411.18 ± 223.73 | 1375.25 ± 213.17 | <0.001 a |
| Family history of T2DM, n (%) | 1111 (3.78) | 253 (9.79) | 858 (3.20) | <0.001 b |
| FBG (mmol/L, mean ± SD) | 5.51 ± 1.47 | 9.00 ± 2.82 | 5.17 ± 0.58 | <0.001 a |
| Total meal frequency (times/week) | 20.53 ± 1.59 | 20.71 ± 1.27 | 20.51 ± 1.62 | <0.001 a |
| Breakfast frequency (times/week) | 6.66 ± 1.38 | 6.80 ± 1.08 | 6.64 ± 1.40 | <0.001 a |
| Lunch frequency (times/week) | 6.98 ± 0.28 | 6.98 ± 0.36 | 6.98 ± 0.27 | 0.411 a |
| Dinner frequency (times/week) | 6.89 ± 0.76 | 6.94 ± 0.58 | 6.89 ± 0.77 | <0.001 a |
| Variables | OR (95% CI) | * p trend | |||
|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | * Per Level Risk | ||
| Total meal frequency | 0.82 (0.73–0.92) | 0.001 | |||
| 21 times/week (n = 26,621) | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) | ||
| 16–20 times/week (n = 1440) | 0.55 (0.43–0.69) | 0.83 (0.64–1.04) | 0.75 (0.58–0.95) | ||
| 14–15 times/week (n = 1344) | 0.57 (0.45–0.72) | 0.81 (0.63–1.02) | 0.70 (0.54–0.90) | ||
| Each time reduction | 0.91 (0.88–0.94) | 0.97 (0.94–1.00) | 0.95 (0.92–0.98) | ||
| Breakfast frequency | 0.89 (0.79–1.02) | 0.090 | |||
| 7 times/week (n = 27,359) | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) | ||
| 3–6 times/week (n = 861) | 0.53 (0.38–0.71) | 0.86 (0.62–1.16) | 0.81 (0.58–1.11) | ||
| 0–2 times/week (n = 1185) | 0.55 (0.42–0.71) | 0.86 (0.65–1.11) | 0.83 (0.63–1.08) | ||
| Each time reduction | 0.90 (0.87–0.94) | 0.97 (0.94–1.01) | 0.97 (0.93–1.01) | ||
| Lunch frequency | 1.08 (0.72–1.62) | 0.703 | |||
| 7 times/week (n = 29,195) | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) | ||
| 3–6 times/week (n = 172) | 0.51 (0.23–0.96) | 0.69 (0.31–1.31) | 0.64 (0.28–1.24) | ||
| 0–2 times/week (n = 38) | 2.34 (0.95–5.01) | 2.34 (0.93–5.12) | 2.18 (0.80–5.05) | ||
| Each time reduction | 1.06 (0.93–1.20) | 1.08 (0.96–1.23) | 1.06 (0.93–1.22) | ||
| Dinner frequency | 0.70 (0.56–0.87) | 0.002 | |||
| 7 times/week (n = 28,621) | 1.00 (Ref.) | 1.00 (Ref.) | 1.00 (Ref.) | ||
| 3–6 times/week (n = 463) | 0.56 (0.36–0.83) | 0.76 (0.49–1.13) | 0.66 (0.42–0.99) | ||
| 0–2 times/week (n = 321) | 0.57 (0.34–0.91) | 0.62 (0.37–0.99) | 0.51 (0.29–0.82) | ||
| Each time reduction | 0.89 (0.83–0.96) | 0.92 (0.86–0.99) | 0.89 (0.83–0.96) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baheti, B.; Liu, X.; Wang, M.; Zhang, C.; Dong, X.; Kang, N.; Li, L.; Li, X.; Yu, S.; Hou, J.; et al. Association between Meal Frequency and Type 2 Diabetes Mellitus in Rural Adults: A Large-Scale Cross-Sectional Study. Nutrients 2023, 15, 1348. https://doi.org/10.3390/nu15061348
Baheti B, Liu X, Wang M, Zhang C, Dong X, Kang N, Li L, Li X, Yu S, Hou J, et al. Association between Meal Frequency and Type 2 Diabetes Mellitus in Rural Adults: A Large-Scale Cross-Sectional Study. Nutrients. 2023; 15(6):1348. https://doi.org/10.3390/nu15061348
Chicago/Turabian StyleBaheti, Bota, Xiaotian Liu, Mu Wang, Caiyun Zhang, Xiaokang Dong, Ning Kang, Linlin Li, Xing Li, Songcheng Yu, Jian Hou, and et al. 2023. "Association between Meal Frequency and Type 2 Diabetes Mellitus in Rural Adults: A Large-Scale Cross-Sectional Study" Nutrients 15, no. 6: 1348. https://doi.org/10.3390/nu15061348
APA StyleBaheti, B., Liu, X., Wang, M., Zhang, C., Dong, X., Kang, N., Li, L., Li, X., Yu, S., Hou, J., Mao, Z., & Wang, C. (2023). Association between Meal Frequency and Type 2 Diabetes Mellitus in Rural Adults: A Large-Scale Cross-Sectional Study. Nutrients, 15(6), 1348. https://doi.org/10.3390/nu15061348