
Dietary Patterns of Off-Reserve Indigenous Peoples in Canada and Their Association with Chronic Conditions
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Dietary Assessment
2.3. Sociodemographic and Lifestyle Characteristics
2.4. Statistical Analysis
2.5. Cluster and Regression Analyses
3. Results
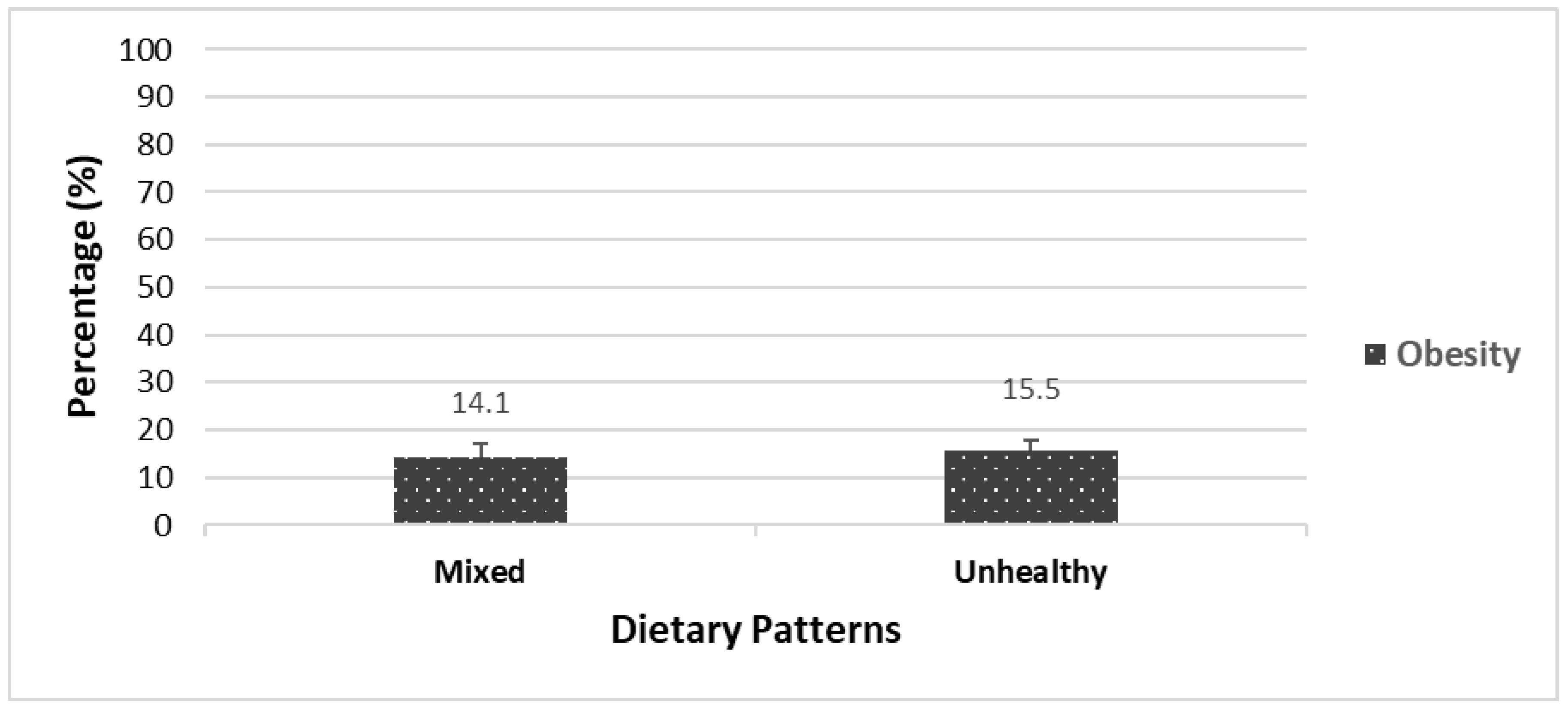
3.1. Prevalence of Obesity and Chronic Diseases across Dietary Patterns
3.2. Association of Related Factors across Dietary Patterns
4. Discussion
4.1. Dietary Patterns and Their Associated Factors among Indigenous Adults
4.2. Dietary Patterns and Their Associated Factors among Indigenous Children
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Noncommunicable Diseases Country Profiles. 2018. Available online: https://apps.who.int/iris/handle/10665/274512 (accessed on 1 February 2023).
- Hahmann, T.; Kumar, M. Unmet Health Care Needs during the Pandemic and Resulting Impacts among First Nations People Living Off Reserve, Métis and Inuit. StatCan COVID-19: Data to Insights for a Better Canada. 2022. Available online: https://www150.statcan.gc.ca/n1/pub/45-28-0001/2022001/article/00008-eng.htm (accessed on 30 August 2022).
- Pollex, R.L.; Zinman, B.H.A.; Harris, S.B.; Hegele, R.A. Clinical and Genetic Associations with Hypertriglyceridemic Waist in a Canadian Aboriginal Population. Int. J. Obes. 2006, 30, 484–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weir, G.C.; Bonner-Weir, S. Five stages of evolving beta-cell dysfunction during progression to diabetes. Diabetes 2004, 53, S16–S21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kant, A. Dietary patterns and health outcomes. J. Am. Diet. Assoc. 2004, 104, 615–635. [Google Scholar] [CrossRef] [PubMed]
- Truth and Reconciliation Commission of Canada: Calls to Action. Available online: https://www2.gov.bc.ca/assets/gov/british-columbians-our-governments/indigenous-people/aboriginal-peoples-documents/calls_to_action_english2.pdf (accessed on 1 February 2023).
- Guyot, M.; Dickson, C.; Paci, C.; Furgal, C.; Chan, H.M. Local observations of climate change and impacts on traditional food security in two northern Aboriginal communities. Int. J. Circumpolar Health 2006, 65, 403–415. [Google Scholar] [CrossRef]
- Sheikh, N.; Egeland, G.M.; Johnson-Down, L.; Kuhnlein, H.V. Changing dietary patterns and body mass index over time in Canadian Inuit communities. Int. J. Circumpolar Health 2011, 70, 511–519. [Google Scholar] [CrossRef]
- Gittelsohn, J.; Wolever, T.M.; Harris, S.B.; Harris-Giraldo, R.; Hanley, A.J.; Zinman, B. Specific patterns of food consumption and preparation are associated with diabetes and obesity in a Native Canadian community. J. Nutr. 1998, 128, 541–547. [Google Scholar] [CrossRef] [Green Version]
- Carter, P.; Gray, L.J.; Troughton, J.; Khunti, K.; Davies, M.J. Fruit and vegetable intake and incidence of type 2 diabetes mellitus: Systematic review and meta-analysis. BMJ 2010, 19, 341. [Google Scholar] [CrossRef] [Green Version]
- Power, E. Conceptualizing food security for Aboriginal people in Canada. Can. J. Public Health 2008, 99, 95–97. [Google Scholar] [CrossRef]
- Shafiee, M.; Keshavarz, P.; Lane, G.; Pahwa, P.; Szafron, M.; Jennings, D.; Vatanparast, H. Food Security Status of Indigenous Peoples in Canada According to the 4 Pillars of Food Security: A Scoping Review. Adv. Nutr. 2022, 13, 2537–2558. [Google Scholar] [CrossRef]
- Boult, D. Hunger in the Arctic: Food (In) Security in Inuit Communities a Discussion Paper. 2004. Available online: https://ruor.uottawa.ca/bitstream/10393/30217/1/2004_Inuit_Food_Security.pdf (accessed on 30 August 2022).
- McAuley, C.K.L. Impacts of traditional food consumption advisories: Compliance, changes in diet and loss of confidence in traditional foods. Environ. Health 2011, 10, 55. [Google Scholar] [CrossRef] [Green Version]
- Ellulu, M.; Abed, Y.; Rahmat, A.; Ranneh, Y.; Ali, F. Epidemiology of obesity in developing countries: Challenges and prevention. Glob. Epidemic Obes. 2014, 2, 2. [Google Scholar] [CrossRef] [Green Version]
- Foulds, H.J.; Bredin, S.S.; Warburton, D.E. The relationship between hypertension and obesity across different ethnicities. J. Hypertens. 2012, 30, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Reedy, J.; Krebs-Smith, S.M.; Miller, P.E.; Liese, A.D.; Kahle, L.L.; Park, Y.; Subar, A.F. Higher diet quality is associated with decreased risk of all-cause, cardiovascular disease, and cancer mortality among older adults. J. Nutr. 2014, 144, 881–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGuire, S. Scientific report of the 2015 dietary guidelines advisory committee. Washington, dc: Us departments of agriculture and health and human services 2015. Adv. Nutr. 2016, 7, 202–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldman, N.; Weinstein, M.; Cornman, J.; Singer, B.; Seeman, T.; Goldman, N.; Chang, M.C. Sex differentials in biological risk factors for chronic disease: Estimates from population-based surveys. J. Women’s Health 2004, 13, 393–403. [Google Scholar] [CrossRef] [Green Version]
- Misra, R.; Lager, J. Ethnic and gender differences in psychosocial factors, glycemic control, and quality of life among adult type 2 diabetic patients. J. Diabetes Complicat. 2009, 23, 54–64. [Google Scholar] [CrossRef]
- Guggenbuhl, P. Osteoporosis in males and females: Is there really a difference? Joint Bone Spine 2009, 76, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Diaz, H.; Marshak, H.H.; Montgomery, S.; Rea, B.; Backman, D. Acculturation and gender: Influence on healthy dietary outcomes for Latino adolescents in California. J. Nutr. Educ. Behav. 2009, 41, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Canadian Community Health Survey, Cycle 2.2, Nutrition (2004): A Guide to Accessing and Interpreting the Data. Ottawa, ON: Health Canada. 2004. Available online: http://www.hc-sc.gc.ca/fn-an/surveill/nutrition/commun/cchs_guide_escc-eng.php (accessed on 1 February 2023).
- Canadian Community Health Survey (CCHS). Reference Guide to Understanding and Using Data 2015 Canadian Community Health Survey—Nutrition. Government of Canada. Available online: http://www23.statcan.gc.ca/imdbbmdi/pub/document/5049_D23_T9_V1-eng.pdf (accessed on 1 February 2023).
- US Department of Agriculture & Agricultural Research Service. USDA Automated Multiple-Pass Method. 2009. Available online: http://www.ars.usda.gov/Services/docs.htm?docid=7710 (accessed on 1 February 2023).
- Moshfegh, A.J.; Borrud, L.; Perloff, B.; LaComb, R. Improved method for the 24-hour dietary recall for use in national surveys. FASEB J. 1999, 13, A603. [Google Scholar]
- Maillot, M.; Vieux, F.; Delaere, F.; Lluch, A.; Darmon, N. Dietary changes needed to reach nutritional adequacy without increasing diet cost according to income: An analysis among French adults. PLoS ONE 2017, 12, e0174679. [Google Scholar] [CrossRef]
- Barr, S.I.; Vatanparast, H.; Smith, J. Breakfast in Canada, revalence of Consumption, Contribution to Nutrient and Food Group Intakes, and Variability across Tertiles of Daily Diet Quality. A Study from the International Breakfast Research Initiative. Nutrients 2020, 12, 2675. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). WHO AnthroPlus Software. Available online: https://www.who.int/growthref/tools/en/ (accessed on 1 February 2023).
- Makles, A. Stata tip 110: How to get the optimal k-means cluster solution. Stata J. 2012, 12, 347–351. [Google Scholar] [CrossRef] [Green Version]
- Garriguet, D. Canadians’ eating habits. Health Rep. 2007, 18, 17–32. [Google Scholar] [PubMed]
- Garriguet, D. Obesity and the eating habits of the Aboriginal population. Health Rep. 2008, 19, 21. [Google Scholar] [PubMed]
- Johnson-Down, L.; Labonte, M.E.; Martin, I.D.; Tsuji, L.J.; Nieboer, E.; Dewailly, E.; Egeland, G.; Lucas, M. Quality of diet is associated with insulin resistance in the Cree (Eeyouch) indigenous population of northern Quebec. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Sheehy, T.; Kolahdooz, F.; Roache, C.; Sharma, S. Traditional food consumption is associated with better diet quality and adequacy among Inuit adults in Nunavut, Canada. Int. J. Food Sci. Nutr. 2015, 66, 445–451. [Google Scholar] [CrossRef]
- Kuhnlein, H.V.; Receveur, O.; Soueida, R.; Egeland, G.M. Arctic indigenous peoples experience the nutrition transition with changing dietary patterns and obesity. J. Nutr. 2004, 134, 1447–1453. [Google Scholar] [CrossRef] [Green Version]
- Chan, H.M.; Fediuk, K.; Batal, M.; Sadik, T.; Tikhonov, C.; Ing, A.; Barwin, L. First Nations Food, Nutrition and Environment Study (FNFNES): Results from Quebec 2016; Assembly of First Nations: Ottawa, ON, Canada, 2019. [Google Scholar]
- Chan, L. First Nations Food, Nutrition and Environment Study (FNFNES); University of Ottawa: Ottawa, ON, Canada, 2012. [Google Scholar]
- Chan, L. First Nations Food, Nutrition and Environment Study (FNFNES): Results from the Atlantic 2014; University of Ottawa: Ottawa, ON, Canada, 2017. [Google Scholar]
- Setiono, F.J.; Jock, B.; Trude, A.; Wensel, C.R.; Poirier, L.; Pardilla, M.; Gittelsohn, J. Associations between Food Consumption Patterns and Chronic Diseases and Self-Reported Morbidities in 6 American Indian Communities. Curr. Dev. Nutr. 2019, 3, 69–80. [Google Scholar] [CrossRef] [Green Version]
- Ng, C.; Corey, P.N.; Young, T.K. Socio-economic patterns of obesity among aboriginal and non-Aboriginal Canadians. Can. J. Public Health 2011, 102, 264–268. [Google Scholar] [CrossRef]
- Sarkar, D.; Walker-Swaney, J.; Shetty, K. Food diversity and indigenous food systems to combat diet-linked chronic diseases. Curr. Dev. Nutr. 2020, 4, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Gracey, M. Historical, cultural, political, and social influences on dietary patterns and nutrition in Australian Aboriginal children. Am. J. Clin. Nutr. 2000, 72, 1361s–1367s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langlois, K.A.; Findlay, L.C.; Kohen, D.E. Dietary habits of Aboriginal children. Health Rep. 2013, 24, 3–7. [Google Scholar] [PubMed]
- Foulds, H.J.; Bredin, S.S.; Warburton, D.E. An evaluation of the physical activity and health status of British Columbian Aboriginal populations. Appl. Physiol. Nutr. Metab. 2012, 37, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Newby, P.K.; Tucker, K.L. Empirically derived eating patterns using factor or cluster analysis: A review. Nutr. Rev. 2004, 62, 177–203. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| CCHS 2004 | CCHS 2015 | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adults | Adults | |||||||||||||||
| Dietary pattern | Soups Wgt N a = 89,702 | Fruits and Vegetables/Pasta Wgt N = 110,945 | Mixed Wgt N = 270,138 | Mixed Wgt N = 98,071 | Unhealthy Wgt N = 289,433 | |||||||||||
| Top five foods | Food name | Mean b ± SD (g) | % c | Food name | Mean ± SD (g) | % | Food name | Mean ± SD (g) | % | Food name | Mean ± SD (g) | % | Food name | Mean ± SD (g) | % | |
| 1. Soups | 538 ± 3.5 | 41 | Vegetables | 446 ± 30.1 | 31 | Vegetables | 78 ± 3.5 | 11 | Vegetables | 191 ± 16.8 | 13 | Fast foods | 171 ± 6.9 | 13 | ||
| 2. Vegetables | 95 ± 15 | 7 | Fruits | 187 ± 36.3 | 13 | Fruits | 59 ± 4.7 | 8 | Fruits | 168 ± 15.9 | 12 | Vegetables | 144 ± 7 | 11 | ||
| 3. Potato | 66 ± 1.4 | 5 | Pasta | 172 ± 30.1 | 12 | Potato | 56 ± 5 | 8 | Fast foods | 156 ± 18 | 11 | Fruits | 121 ± 9.2 | 9 | ||
| 4. Beef | 61 ± 22.3 | 5 | Added fats | 72 ± 7.7 | 5 | Beef | 52 ± 3.8 | 8 | Whole grains | 104 ± 10.6 | 7 | Added fats | 94 ± 8.6 | 7 | ||
| 5. Whole grains | 53 ± 13.2 | 4 | Beef | 61 ± 10 | 4 | Added fats | 51 ± 2.9 | 7 | Soups | 101 ± 20.7 | 7 | Sweet baked goods | 79 ± 5.9 | 6 | ||
| NRF d (mean ± SD) | 395.9 ± 17.8 * | 518.5 ± 24.7 | 449.7 ± 12 | 547.5 ± 4.2 | 466.3 ± 6.2 | |||||||||||
| Age (mean ± SD) | 42.8 ± 2.3 | 38.1 ± 2.6 | 42 ± 1.1 | 45.7 ± 2.2 | 45.5 ± 2.4 | |||||||||||
| Weight (kg) | 83.7 ± 9.1 | 79.4 ± 6.2 | 78.5 ± 2.2 | 77.2 ± 0.9 | 86.9 ± 2.4 | |||||||||||
| Gender (% woman) | 39.6 | 53.4 | 58.0 | 48.0 | 40.0 | |||||||||||
| BMI (%) | Normal | 51.0 | 20.6 | 30.3 | 26.0 | 17.0 | ||||||||||
| Overweight | 7.8 | 36.7 | 31.8 | 20.0 | 38.5 | |||||||||||
| Obese | 41.2 | 42.7 | 37.8 | 54.0 | 44.5 | |||||||||||
| Income (%) | Low | 87.6 | 43.0 | 69.1 | 52.0 | 46.0 | ||||||||||
| High | 12.4 | 57.0 | 30.9 | 48.0 | 54.0 | |||||||||||
| Education (%) | Below bachelor’s level | 97.8 | 83.7 | 90.9 | 81.0 | 79.5 | ||||||||||
| Bachelor’s level and above | 2.2 | 16.3 | 9.1 | 19.0 | 41.0 | |||||||||||
| Smoking (%) | Non-smoker | 25.4 | 57.7 | 47.7 | 73.0 | 59.0 | ||||||||||
| Smoker | 74.6 | 42.3 | 52.3 | 27.0 | 41.0 | |||||||||||
| Activity (%) | Active | 29.2 | 48.3 | 38.9 | 52.0 | 46.0 | ||||||||||
| Inactive | 70.8 | 51.7 | 61.1 | 48.0 | 54.0 | |||||||||||
| Food security (%) | Food insecure | 41.1 | 23.5 | 36.5 | 25.0 | 35.0 | ||||||||||
| Food secure | 58.9 | 76.5 | 63.5 | 75.0 | 65.0 | |||||||||||
| CCHS 2004 | CCHS 2015 | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Men | Men | |||||||||||||||||
| Dietary pattern | Unhealthy Wgt N a = 200,190 | Soup Wgt N = 25,126 | Potato Wgt N = 87,919 | Mixed Wgt N = 140,819 | Soup Wgt N = 40,828 | High-Fat Wgt N = 63,532 | ||||||||||||
| Top five foods | Food name | Mean b ± SD (g) | % c | Food name | Mean ± SD (g) | % | Food name | Mean ± SD (g) | % | Food name | Mean ± SD (g) | % | Food name | Mean ± SD (g) | % | Food name | Mean ± SD (g) | % |
| Vegetables | 106 ± 10.4 | 14 | Soups | 662 ± 69 | 38 | Potato | 318 ± 30 | 25 | Vegetables | 138 ± 13 | 11 | Soups | 752 ± 87 | 37 | Fast foods | 625 ± 30 | 33 | |
| Fruits | 68 ± 9.5 | 9 | Vegetables | 247 ± 69 | 14 | Vegetables | 173 ± 23.6 | 14 | Fruits | 96 ± 11 | 8 | Vegetables | 209 ± 44 | 10 | Vegetables | 148 ± 22 | 8 | |
| Beef | 59 ± 6.5 | 8 | Whole grains | 90 ± 24.7 | 5 | Beef | 138 ± 22.9 | 11 | Fast foods | 95 ± 8 | 8 | Whole grains | 144 ± 44 | 7 | Whole grains | 139 ± 20 | 7 | |
| Added fats | 53 ± 4.6 | 7 | Fruit | 76 ± 26.5 | 4 | Whole grains | 82 ± 25.3 | 7 | Chicken | 91 ± 14 | 8 | Fast foods | 137 ± 35 | 7 | Fruits | 119 ± 30 | 6 | |
| Confectionary | 47 ± 10.3 | 6 | Beef | 73 ± 39 | 4 | Added fats | 72 ± 12 | 6 | Potato | 89 ± 13 | 7 | Chicken | 91 ± 34 | 4 | Added fats | 91 ± 10 | 5 | |
| NRF d (mean ± SD) | 425.8 * ± 17.8 | 400 ± 24.3 | 488 ± 30.2 | 485 ± 21.3 | 409.4 ± 36.9 | 404.9 ± 19.8 | ||||||||||||
| CCHS 2004 | CCHS 2015 | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Women | Women | |||||||||||||||||
| Dietary pattern | Soups Wgt N a = 27,959 | Fruits Wgt N = 2,983,971 | Mixed Wgt N = 302,010 | Vegetables Wgt N = 25,741 | Mixed Wgt N = 676,074 | Healthy-like Wgt N = 1,245,903 | ||||||||||||
| Top five foods | Food name | Mean b ± SD (g) | % c | Food name | Mean ± SD (g) | % | Food name | Mean ± SD (g) | % | Food name | Mean ± SD (g) | % | Food name | Mean ± SD (g) | % | Food name | Mean ± SD (g) | % |
| 1. Soups | 358 ± 28 | 36 | Fruits | 368 ± 37 | 34 | Vegetables | 83 ± 4.9 | 14 | Vegetables | 582 ± 51 | 44 | Vegetables | 134 ± 9.8 | 13 | Soups | 412 ± 45.2 | 25 | |
| 2. Vegetables | 78 ± 11 | 8 | Vegetables | 97 ± 16 | 9 | Added fats | 49 ± 4.2 | 8 | Pasta | 105 ± 30 | 8 | Fast foods | 117 ± 9.6 | 11 | Fruits | 264 ± 38.6 | 16 | |
| 3. Beef | 54 ± 16 | 5 | Confectionery | 63 ± 25 | 6 | Potato | 47 ± 5.1 | 8 | Fruits | 99 ± 49 | 7 | Fruits | 104 ± 8.8 | 10 | Vegetables | 250 ± 39 | 15 | |
| 4. Pasta | 47 ± 21 | 5 | Whole grains | 51 ± 12 | 5 | Beef | 42 ± 4.4 | 7 | Added fats | 72 ± 13 | 5 | Whole grains | 73 ± 6.3 | 7 | Whole grains | 87 ± 12 | 5 | |
| 5. Potato | 46 ± 16 | 5 | Added fats | 49 ± 6.2 | 5 | Whole grains | 34 ± 4 | 6 | Pork | 43 ± 14 | 3 | Chicken | 71 ± 10 | 7 | Sweet baked goods | 76 ± 19 | 5 | |
| NRF d (mean ± SD) | 407 * ± 26 | 526.4 ± 28.7 | 455 ± 16.8 | 568.7 ± 42.7 | 481.7 ± 10.9 | 568.4 ± 37.3 | ||||||||||||
| CCHS 2004 | CCHS 2015 | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Children | Children | |||||||||||||||
| Dietary pattern | Soups Wgt N a = 16,287 | High fat-High sugar Wgt N = 159,354 | Mixed Wgt N = 27,695 | Mixed Wgt N = 120,825 | Unhealthy Wgt N = 39,517 | |||||||||||
| Top five foods | Food name | Mean b ± SD (g) | % c | Food name | Mean ± SD (g) | % | Food name | Mean ± SD (g) | % | Food name | Mean ± SD (g) | % | Food name | Mean ± SD (g) | % | |
| 1. Soups | 406 ± 33 | 37 | Vegetables | 66 ± 5.5 | 11 | Fruits | 235 ± 20 | 20 | Fruits | 161 ± 15 | 15 | Fast foods | 411 ± 28 | 29 | ||
| 2. Vegetables | 89 ± 19 | 8 | Whole grains | 43 ± 4.7 | 7 | Confectionery | 167 ± 26 | 14 | Vegetables | 102 ± 8.3 | 9 | Whole grains | 133 ± 16 | 9 | ||
| 3. Fruits | 79 ± 17 | 7 | Added Fats | 42 ± 3 | 7 | Pasta | 133 ± 24 | 11 | Sweet baked goods | 72 ± 6.7 | 7 | Fruits | 93 ± 15 | 7 | ||
| 4. Pasta | 48 ± 15 | 4 | Confectionery | 36 ± 3 | 6 | Vegetables | 100 ± 18 | 9 | Whole grains | 66 ± 5.9 | 6 | Confectionery | 82 ± 14 | 6 | ||
| 5. Confectionery | 49 ± 11 | 4 | Fast foods | 33 ± 3 | 5 | Whole grains | 60 ± 12 | 5 | Soups | 64 ± 11 | 6 | Sweet baked goods | 70 ± 12.7 | 5 | ||
| NRF d (mean ± SD) | 425.5 ± 18.6 | 457.5 ± 12 | 470.9 ± 36 | 510.4 ± 9.3 * | 427.8 ± 13.5 | |||||||||||
| Age (mean ± SD) | 9.5 ± 1 | 11 ± 0.5 | 10 ± 0.7 | 9.9 ± 0.3 | 11.8 ± 0.6 | |||||||||||
| Weight (mean ± SD) | 41.4 ± 6.7 | 48 ± 3.1 | 51 ± 3.6 | 47 ± 2.7 | 57.7 ± 4.4 | |||||||||||
| Gender (% women) | 44. | 59.4 | 69.3 | 52 | 33 | |||||||||||
| BMI (mean ± SD) | 0.8 ± 0.3 | 0.87 ± 0.1 | 1.1 ± 0.1 | 0.9 ± 0.1 | 1.1 ± 0.3 | |||||||||||
| Income (%) | Low | 71.7 | 76.3 | 72.1 | 34 | 37 | ||||||||||
| High | 28.2 | 23.6 | 27.8 | 66 | 63 | |||||||||||
| Education (%) | Below = bachelor’s level | 96 | 91 | 95 | 83 | 83 | ||||||||||
| Bachelor’s level and above | 3.9 | 8.8 | 4.8 | 17 | 17 | |||||||||||
| Activity (%) | Active | 100 | 3.1 | 0.5 | 49 | 27 | ||||||||||
| Inactive | 0 | 96.8 | 99.4 | 51 | 73 | |||||||||||
| Food security (%) | Food insecure | 43.2 | 52 | 47 | 42 | 44 | ||||||||||
| Food secure | 56.7 | 47.9 | 52.7 | 58 | 56 | |||||||||||
| Variables | CCHS 2004 | CCHS 2015 |
|---|---|---|
| Adjusted Odds Ratio 1 (95% CI) | Adjusted Odds Ratio (95% CI) | |
| Gender | ||
| Men | 1 # | 1 |
| Women | 3.2 (0.8–12.3) | 1.2 (0.45–3.3) |
| Age Groups | ||
| ≥30 and <45 years | 1 | 1 |
| ≥45 and >65 years | 3.3 (0.6–4.7) | 5.8 (1.6–6.5) * |
| ≥65 years | 5.2 (0.6–6) | 6.9 (1.6–8) |
| Education | ||
| No university degree | 1 | 1 |
| A university degree | 0.18 (0.01–3) | 0.31 (0.06–1.6) |
| Income | ||
| Low income | 1 | 1 |
| High income | 0.14 (0.04–0.5) | 0.6 (0.2–1.8) |
| Smoking Status | ||
| Non-smoker | 1 | 1 |
| Smoker | 0.35 (0.1–1.1) | 1.1 (0.3–1.4) |
| Physical Activity | ||
| Active | 1 | 1 |
| Inactive | 1.5 (0.5–4.5) | 1.2 (0.4–3.2) |
| NRF 2 | ||
| 1st tertile | 1 | 1 |
| 2nd tertile | 0.3 (0.06–2.1) | 0.4 (0.1–1.4) |
| 3rd tertile | 0.3 (0.05–2.1) | 0.6 (0.1–2.8) |
| Dietary Patterns | Soups: 1 | Mixed: 1 |
| Fruit/Veg/Pasta: 0.4 (0.03–6.1) | Unhealthy: 2.7 (0.6–4) | |
| Mixed: 0.8 (0.1–4.9) | ||
| BMI 3 | ||
| Normal | 1 | 1 |
| Overweight | 0.3 (0.09–1.6) | 1.4 (0.3–5.4) |
| Obese | 0.8 (0.16–4.7) | 3 (0.8–5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keshavarz, P.; Lane, G.; Pahwa, P.; Lieffers, J.; Shafiee, M.; Finkas, K.; Desmarais, M.; Vatanparast, H. Dietary Patterns of Off-Reserve Indigenous Peoples in Canada and Their Association with Chronic Conditions. Nutrients 2023, 15, 1485. https://doi.org/10.3390/nu15061485
Keshavarz P, Lane G, Pahwa P, Lieffers J, Shafiee M, Finkas K, Desmarais M, Vatanparast H. Dietary Patterns of Off-Reserve Indigenous Peoples in Canada and Their Association with Chronic Conditions. Nutrients. 2023; 15(6):1485. https://doi.org/10.3390/nu15061485
Chicago/Turabian StyleKeshavarz, Pardis, Ginny Lane, Punam Pahwa, Jessica Lieffers, Mojtaba Shafiee, Kelly Finkas, Marisa Desmarais, and Hassan Vatanparast. 2023. "Dietary Patterns of Off-Reserve Indigenous Peoples in Canada and Their Association with Chronic Conditions" Nutrients 15, no. 6: 1485. https://doi.org/10.3390/nu15061485