
Very Low-Calorie Ketogenic Diet (VLCKD) as Pre-Operative First-Line Dietary Therapy in Patients with Obesity Who Are Candidates for Bariatric Surgery

 ,
,  , , , ,
, , , , 
 ,
, 
Abstract
:1. Introduction
2. Very Low-Calorie Ketogenic Diet
2.1. Definition of Ketogenic Diets
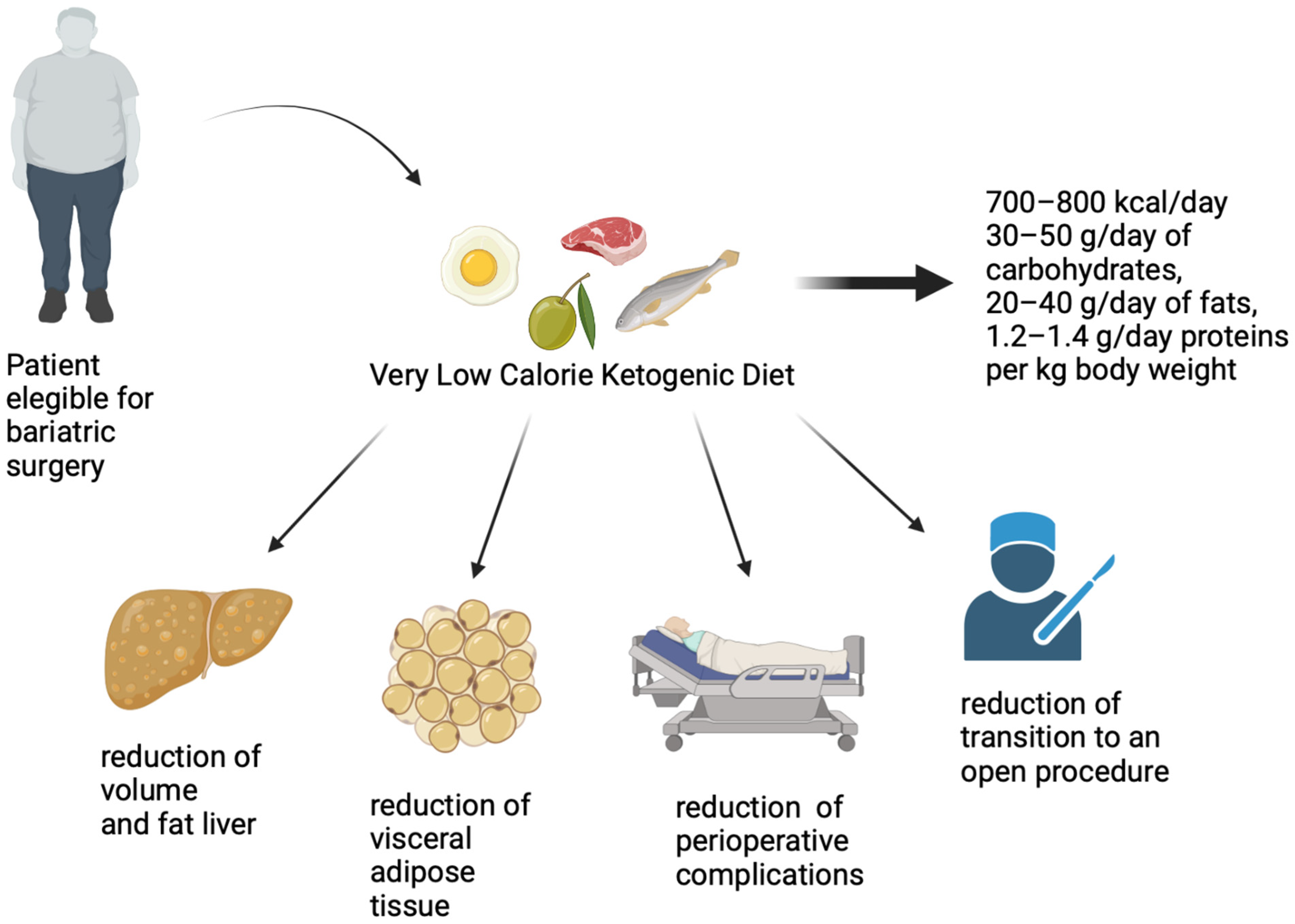
2.2. Mechanisms of Action and Benefits of Very Low-Calorie Ketogenic Diet before Bariatric Surgery
2.3. Indications and Contraindications of Very Low-Calorie Ketogenic Diet in Pre-Bariatric Surgery
2.4. Side Effects and Transient Complications of Very Low-Calorie Ketogenic Diet
2.5. Differences between Very Low-Calorie Ketogenic Diets with Meal Replacement or with Traditional Protein
3. Bariatric Surgery
3.1. Sleeve Gastrectomy
3.2. Roux-en-Y Gastric Bypass
3.3. One-Anastomosis Gastric Bypass
3.4. Single-Anastomosis Duodeno-Ileal Bypass
3.5. Perioperative Issues
3.5.1. Perioperative Technical Issues
3.5.2. Port Placement
3.5.3. Patient-Related and Intraoperative Factors
3.5.4. Anaesthesia
3.5.5. Perfusion
3.5.6. Intubation
3.5.7. Ventilation
3.5.8. Extubation
3.6. Very Low-Calorie Ketogenic Diet in Bariatric Surgery
3.6.1. The Use of Ketogenic Diet on Patients with Obesity Scheduled for Bariatric Surgery
3.6.2. Assessment of Surgical Outcomes
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Flegal, K.M.; Kit, B.K.; Orpana, H.; Graubard, B.I. Association of all-cause mortality with overweight and obesity using standard body mass index categories: A systematic review and meta-analysis. JAMA 2013, 309, 71–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muscogiuri, G.; Verde, L.; Sulu, C.; Katsiki, N.; Hassapidou, M.; Frias-Toral, E.; Cucalon, G.; Pazderska, A.; Yumuk, V.D.; Colao, A.; et al. Mediterranean Diet and Obesity-related Disorders: What is the Evidence? Curr. Obes. Rep. 2022, 11, 287–304. [Google Scholar] [CrossRef] [PubMed]
- Sjostrom, L. Review of the key results from the Swedish Obese Subjects (SOS) trial—A prospective controlled intervention study of bariatric surgery. J. Intern. Med. 2013, 273, 219–234. [Google Scholar] [CrossRef]
- Sjostrom, L.; Peltonen, M.; Jacobson, P.; Sjostrom, C.D.; Karason, K.; Wedel, H.; Ahlin, S.; Anveden, A.; Bengtsson, C.; Bergmark, G.; et al. Bariatric surgery and long-term cardiovascular events. JAMA 2012, 307, 56–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrone, F.; Bianciardi, E.; Ippoliti, S.; Nardella, J.; Fabi, F.; Gentileschi, P. Long-term effects of laparoscopic sleeve gastrectomy versus Roux-en-Y gastric bypass for the treatment of morbid obesity: A monocentric prospective study with minimum follow-up of 5 years. Updates Surg. 2017, 69, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Sundbom, M. Laparoscopic revolution in bariatric surgery. World J. Gastroenterol. 2014, 20, 15135–15143. [Google Scholar] [CrossRef]
- Riess, K.P.; Baker, M.T.; Lambert, P.J.; Mathiason, M.A.; Kothari, S.N. Effect of preoperative weight loss on laparoscopic gastric bypass outcomes. Surg. Obes. Relat. Dis. 2008, 4, 704–708. [Google Scholar] [CrossRef] [PubMed]
- Picot, J.; Jones, J.; Colquitt, J.L.; Gospodarevskaya, E.; Loveman, E.; Baxter, L.; Clegg, A.J. The clinical effectiveness and cost-effectiveness of bariatric (weight loss) surgery for obesity: A systematic review and economic evaluation. Health Technol. Assess 2009, 13, 1–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, M.L.; Drew, R.L.; Chazin-Caldie, M. Laparoscopic Roux-en-Y gastric bypass: Preoperative determinants of prolonged operative times, conversion to open gastric bypasses, and postoperative complications. Obes. Surg. 2003, 13, 734–738. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, H.; Minville, V.; Delanoue, K.; Mazerolles, M.; Concina, D.; Fourcade, O. The importance of increased neck circumference to intubation difficulties in obese patients. Anesth. Analg. 2008, 106, 1132–1136. [Google Scholar] [CrossRef] [PubMed]
- Gerber, P.; Anderin, C.; Thorell, A. Weight loss prior to bariatric surgery: An updated review of the literature. Scand. J. Surg. 2015, 104, 33–39. [Google Scholar] [CrossRef] [Green Version]
- Livhits, M.; Mercado, C.; Yermilov, I.; Parikh, J.A.; Dutson, E.; Mehran, A.; Ko, C.Y.; Gibbons, M.M. Does weight loss immediately before bariatric surgery improve outcomes: A systematic review. Surg. Obes. Relat. Dis. 2009, 5, 713–721. [Google Scholar] [CrossRef]
- Schiavo, L.; Sans, A.; Scalera, G.; Barbarisi, A.; Iannelli, A. Why Preoperative Weight Loss in Preparation for Bariatric Surgery Is Important. Obes. Surg. 2016, 26, 2790–2792. [Google Scholar] [CrossRef] [PubMed]
- Bettini, S.; Belligoli, A.; Fabris, R.; Busetto, L. Diet approach before and after bariatric surgery. Rev. Endocr. Metab. Disord. 2020, 21, 297–306. [Google Scholar] [CrossRef]
- Fried, M.; Yumuk, V.; Oppert, J.M.; Scopinaro, N.; Torres, A.J.; Weiner, R.; Yashkov, Y.; Fruhbeck, G. International Federation for the Surgery of Obesity—European, C. Interdisciplinary European Guidelines on metabolic and bariatric surgery. Obes. Facts 2013, 6, 449–468. [Google Scholar] [CrossRef]
- Mechanick, J.I.; Apovian, C.; Brethauer, S.; Garvey, W.T.; Joffe, A.M.; Kim, J.; Kushner, R.F.; Lindquist, R.; Pessah-Pollack, R.; Seger, J.; et al. Clinical Practice Guidelines for the Perioperative Nutrition, Metabolic, and Nonsurgical Support of Patients Undergoing Bariatric Procedures—2019 Update: Cosponsored by American Association of Clinical Endocrinologists/American College of Endocrinology, the Obesity Society, American Society for Metabolic & Bariatric Surgery, Obesity Medicine Association, and American Society of Anesthesiologists—Executive Summary. Endocr. Pract. 2019, 25, 1346–1359. [Google Scholar] [CrossRef] [PubMed]
- Tang, T.; Abbott, S.; le Roux, C.W.; Wilson, V.; Singhal, R.; Bellary, S.; Tahrani, A.A. Preoperative weight loss with glucagon-like peptide-1 receptor agonist treatment predicts greater weight loss achieved by the combination of medical weight management and bariatric surgery in patients with type 2 diabetes: A longitudinal analysis. Diabetes Obes. Metab. 2018, 20, 745–748. [Google Scholar] [CrossRef] [PubMed]
- Adrianzen Vargas, M.; Cassinello Fernandez, N.; Ortega Serrano, J. Preoperative weight loss in patients with indication of bariatric surgery: Which is the best method? Nutr. Hosp. 2011, 26, 1227–1230. [Google Scholar] [CrossRef]
- Busetto, L.; Segato, G.; De Luca, M.; Bortolozzi, E.; MacCari, T.; Magon, A.; Inelmen, E.M.; Favretti, F.; Enzi, G. Preoperative weight loss by intragastric balloon in super-obese patients treated with laparoscopic gastric banding: A case-control study. Obes. Surg. 2004, 14, 671–676. [Google Scholar] [CrossRef]
- Baldry, E.L.; Leeder, P.C.; Idris, I.R. Pre-operative dietary restriction for patients undergoing bariatric surgery in the UK: Observational study of current practice and dietary effects. Obes. Surg. 2014, 24, 416–421. [Google Scholar] [CrossRef]
- Holderbaum, M.S.; Buss, C. Dietary Management in the Immediate Preoperative Period of Bariatric Surgery: A National Overview: Bariatric Preoperative Diets. Obes. Surg. 2018, 28, 1688–1696. [Google Scholar] [CrossRef]
- Erdem, N.Z.; Ozelgun, D.; Taskin, H.E.; Avsar, F.M. Comparison of a pre-bariatric surgery very low-calorie ketogenic diet and the Mediterranean diet effects on weight loss, metabolic parameters, and liver size reduction. Sci. Rep. 2022, 12, 20686. [Google Scholar] [CrossRef]
- Gastaldo, I.; Casas, R.; Moize, V. Clinical Impact of Mediterranean Diet Adherence before and after Bariatric Surgery: A Narrative Review. Nutrients 2022, 14, 393. [Google Scholar] [CrossRef]
- Schiavo, L.; Scalera, G.; Sergio, R.; De Sena, G.; Pilone, V.; Barbarisi, A. Clinical impact of Mediterranean-enriched-protein diet on liver size, visceral fat, fat mass, and fat-free mass in patients undergoing sleeve gastrectomy. Surg. Obes. Relat. Dis. 2015, 11, 1164–1170. [Google Scholar] [CrossRef]
- Hollis, G.; Franz, R.; Bauer, J.; Bell, J. Implementation of a very low calorie diet program into the pre-operative model of care for obese general elective surgery patients: Outcomes of a feasibility randomised control trial. Nutr. Diet. 2020, 77, 490–498. [Google Scholar] [CrossRef] [Green Version]
- Benjaminov, O.; Beglaibter, N.; Gindy, L.; Spivak, H.; Singer, P.; Wienberg, M.; Stark, A.; Rubin, M. The effect of a low-carbohydrate diet on the nonalcoholic fatty liver in morbidly obese patients before bariatric surgery. Surg. Endosc. 2007, 21, 1423–1427. [Google Scholar] [CrossRef] [PubMed]
- Browning, J.D.; Baker, J.A.; Rogers, T.; Davis, J.; Satapati, S.; Burgess, S.C. Short-term weight loss and hepatic triglyceride reduction: Evidence of a metabolic advantage with dietary carbohydrate restriction. Am. J. Clin. Nutr. 2011, 93, 1048–1052. [Google Scholar] [CrossRef] [Green Version]
- Trimboli, P.; Castellana, M.; Bellido, D.; Casanueva, F.F. Confusion in the nomenclature of ketogenic diets blurs evidence. Rev. Endocr. Metab. Disord. 2020, 21, 1–3. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Barrea, L.; Laudisio, D.; Pugliese, G.; Salzano, C.; Savastano, S.; Colao, A. The management of very low-calorie ketogenic diet in obesity outpatient clinic: A practical guide. J. Transl. Med. 2019, 17, 356. [Google Scholar] [CrossRef] [Green Version]
- Muscogiuri, G.; El Ghoch, M.; Colao, A.; Hassapidou, M.; Yumuk, V.; Busetto, L.; Obesity Management Task Force (OMTF) of the European Association for the Study of Obesity (EASO). European Guidelines for Obesity Management in Adults with a Very Low-Calorie Ketogenic Diet: A Systematic Review and Meta-Analysis. Obes. Facts 2021, 14, 222–245. [Google Scholar] [CrossRef]
- Freeman, J.M.; Kossoff, E.H.; Hartman, A.L. The ketogenic diet: One decade later. Pediatrics 2007, 119, 535–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrea, L.; Caprio, M.; Watanabe, M.; Cammarata, G.; Feraco, A.; Muscogiuri, G.; Verde, L.; Colao, A.; Savastano, S. Could very low-calorie ketogenic diets turn off low grade inflammation in obesity? Emerging evidence. Crit. Rev. Food Sci. Nutr. 2022, 1–17. [Google Scholar] [CrossRef]
- Barrea, L.; de Alteriis, G.; Muscogiuri, G.; Vetrani, C.; Verde, L.; Camajani, E.; Aprano, S.; Colao, A.; Savastano, S. Impact of a Very Low-Calorie Ketogenic Diet (VLCKD) on Changes in Handgrip Strength in Women with Obesity. Nutrients 2022, 14, 4213. [Google Scholar] [CrossRef]
- Barrea, L.; Megna, M.; Cacciapuoti, S.; Frias-Toral, E.; Fabbrocini, G.; Savastano, S.; Colao, A.; Muscogiuri, G. Very low-calorie ketogenic diet (VLCKD) in patients with psoriasis and obesity: An update for dermatologists and nutritionists. Crit. Rev. Food Sci. Nutr. 2022, 62, 398–414. [Google Scholar] [CrossRef]
- Moriconi, E.; Camajani, E.; Fabbri, A.; Lenzi, A.; Caprio, M. Very-Low-Calorie Ketogenic Diet as a Safe and Valuable Tool for Long-Term Glycemic Management in Patients with Obesity and Type 2 Diabetes. Nutrients 2021, 13, 758. [Google Scholar] [CrossRef] [PubMed]
- Albanese, A.; Prevedello, L.; Markovich, M.; Busetto, L.; Vettor, R.; Foletto, M. Pre-operative Very Low Calorie Ketogenic Diet (VLCKD) vs. Very Low Calorie Diet (VLCD): Surgical Impact. Obes. Surg. 2019, 29, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Cappello, G.; Franceschelli, A.; Cappello, A.; De Luca, P. Ketogenic enteral nutrition as a treatment for obesity: Short term and long term results from 19,000 patients. Nutr. Metab. 2012, 9, 96. [Google Scholar] [CrossRef] [Green Version]
- Manninen, A.H. Metabolic effects of the very-low-carbohydrate diets: Misunderstood “villains” of human metabolism. J. Int. Soc. Sports Nutr. 2004, 1, 7–11. [Google Scholar] [CrossRef] [Green Version]
- Moreno, O.; Meoro, A.; Martinez, A.; Rodriguez, C.; Pardo, C.; Aznar, S.; Lopez, P.; Serrano, J.; Boix, E.; Martin, M.D.; et al. Comparison of two low-calorie diets: A prospective study of effectiveness and safety. J. Endocrinol. Invest. 2006, 29, 633–640. [Google Scholar] [CrossRef]
- Caprio, M.; Infante, M.; Moriconi, E.; Armani, A.; Fabbri, A.; Mantovani, G.; Mariani, S.; Lubrano, C.; Poggiogalle, E.; Migliaccio, S.; et al. Very-low-calorie ketogenic diet (VLCKD) in the management of metabolic diseases: Systematic review and consensus statement from the Italian Society of Endocrinology (SIE). J. Endocrinol. Invest. 2019, 42, 1365–1386. [Google Scholar] [CrossRef]
- Goday, A.; Bellido, D.; Sajoux, I.; Crujeiras, A.B.; Burguera, B.; Garcia-Luna, P.P.; Oleaga, A.; Moreno, B.; Casanueva, F.F. Short-term safety, tolerability and efficacy of a very low-calorie-ketogenic diet interventional weight loss program versus hypocaloric diet in patients with type 2 diabetes mellitus. Nutr. Diabetes 2016, 6, e230. [Google Scholar] [CrossRef] [Green Version]
- Romano, L.; Marchetti, M.; Gualtieri, P.; Di Renzo, L.; Belcastro, M.; De Santis, G.L.; Perrone, M.A.; De Lorenzo, A. Effects of a Personalized VLCKD on Body Composition and Resting Energy Expenditure in the Reversal of Diabetes to Prevent Complications. Nutrients 2019, 11, 1526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SICOB. Linee Guida di Chirurgia Dell’Obesità. Available online: https://www.sicob.org/00_materiali/linee_guida_2016.pdf (accessed on 3 April 2023).
- Fris, R.J. Preoperative low energy diet diminishes liver size. Obes. Surg. 2004, 14, 1165–1170. [Google Scholar] [CrossRef]
- Cassie, S.; Menezes, C.; Birch, D.W.; Shi, X.; Karmali, S. Effect of preoperative weight loss in bariatric surgical patients: A systematic review. Surg. Obes. Relat. Dis. 2011, 7, 760–767; discussion 767. [Google Scholar] [CrossRef]
- Stephens, D.J.; Saunders, J.K.; Belsley, S.; Trivedi, A.; Ewing, D.R.; Iannace, V.; Capella, R.F.; Wasielewski, A.; Moran, S.; Schmidt, H.J.; et al. Short-term outcomes for super-super obese (BMI > or =60 kg/m2) patients undergoing weight loss surgery at a high-volume bariatric surgery center: Laparoscopic adjustable gastric banding, laparoscopic gastric bypass, and open tubular gastric bypass. Surg. Obes. Relat. Dis. 2008, 4, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Colles, S.L.; Dixon, J.B.; Marks, P.; Strauss, B.J.; O’Brien, P.E. Preoperative weight loss with a very-low-energy diet: Quantitation of changes in liver and abdominal fat by serial imaging. Am. J. Clin. Nutr. 2006, 84, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Leonetti, F.; Campanile, F.C.; Coccia, F.; Capoccia, D.; Alessandroni, L.; Puzziello, A.; Coluzzi, I.; Silecchia, G. Very low-carbohydrate ketogenic diet before bariatric surgery: Prospective evaluation of a sequential diet. Obes. Surg. 2015, 25, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Hession, M.; Rolland, C.; Kulkarni, U.; Wise, A.; Broom, J. Systematic review of randomized controlled trials of low-carbohydrate vs. low-fat/low-calorie diets in the management of obesity and its comorbidities. Obes. Rev. 2009, 10, 36–50. [Google Scholar] [CrossRef]
- Schiavo, L.; Pilone, V.; Rossetti, G.; Barbarisi, A.; Cesaretti, M.; Iannelli, A. A 4-Week Preoperative Ketogenic Micronutrient-Enriched Diet Is Effective in Reducing Body Weight, Left Hepatic Lobe Volume, and Micronutrient Deficiencies in Patients Undergoing Bariatric Surgery: A Prospective Pilot Study. Obes. Surg. 2018, 28, 2215–2224. [Google Scholar] [CrossRef]
- Paoli, A.; Bosco, G.; Camporesi, E.M.; Mangar, D. Ketosis, ketogenic diet and food intake control: A complex relationship. Front. Psychol. 2015, 6, 27. [Google Scholar] [CrossRef] [Green Version]
- Koutnik, A.P.; D’Agostino, D.P.; Egan, B. Anticatabolic Effects of Ketone Bodies in Skeletal Muscle. Trends Endocrinol. Metab. 2019, 30, 227–229. [Google Scholar] [CrossRef]
- Marinari, G.; Foletto, M.; Nagliati, C.; Navarra, G.; Borrelli, V.; Bruni, V.; Fantola, G.; Moroni, R.; Tritapepe, L.; Monzani, R.; et al. Enhanced recovery after bariatric surgery: An Italian consensus statement. Surg. Endosc. 2022, 36, 7171–7186. [Google Scholar] [CrossRef] [PubMed]
- Di Lorenzo, N.; Antoniou, S.A.; Batterham, R.L.; Busetto, L.; Godoroja, D.; Iossa, A.; Carrano, F.M.; Agresta, F.; Alarcon, I.; Azran, C.; et al. Clinical practice guidelines of the European Association for Endoscopic Surgery (EAES) on bariatric surgery: Update 2020 endorsed by IFSO-EC, EASO and ESPCOP. Surg. Endosc. 2020, 34, 2332–2358. [Google Scholar] [CrossRef] [Green Version]
- Anderin, C.; Gustafsson, U.O.; Heijbel, N.; Thorell, A. Weight loss before bariatric surgery and postoperative complications: Data from the Scandinavian Obesity Registry (SOReg). Ann. Surg. 2015, 261, 909–913. [Google Scholar] [CrossRef]
- Carron, M.; Safaee Fakhr, B.; Ieppariello, G.; Foletto, M. Perioperative care of the obese patient. Br. J. Surg. 2020, 107, e39–e55. [Google Scholar] [CrossRef] [Green Version]
- Basciani, S.; Camajani, E.; Contini, S.; Persichetti, A.; Risi, R.; Bertoldi, L.; Strigari, L.; Prossomariti, G.; Watanabe, M.; Mariani, S.; et al. Very-Low-Calorie Ketogenic Diets With Whey, Vegetable, or Animal Protein in Patients With Obesity: A Randomized Pilot Study. J. Clin. Endocrinol. Metab. 2020, 105, 2939–2949. [Google Scholar] [CrossRef]
- Barrea, L.; Verde, L.; Vetrani, C.; Marino, F.; Aprano, S.; Savastano, S.; Colao, A.; Muscogiuri, G. VLCKD: A real time safety study in obesity. J. Transl. Med. 2022, 20, 23. [Google Scholar] [CrossRef] [PubMed]
- Hess, D.S.; Hess, D.W. Biliopancreatic diversion with a duodenal switch. Obes. Surg. 1998, 8, 267–282. [Google Scholar] [CrossRef]
- Regan, J.P.; Inabnet, W.B.; Gagner, M.; Pomp, A. Early experience with two-stage laparoscopic Roux-en-Y gastric bypass as an alternative in the super-super obese patient. Obes. Surg. 2003, 13, 861–864. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; El Chaar, M.; Ghiassi, S.; Rogers, A.M.; American Society for Metabolic and Bariatric Surgery Clinical Issues Committee. American Society for Metabolic and Bariatric Surgery updated position statement on sleeve gastrectomy as a bariatric procedure. Surg. Obes. Relat. Dis. 2017, 13, 1652–1657. [Google Scholar] [CrossRef]
- Benaiges, D.; Mas-Lorenzo, A.; Goday, A.; Ramon, J.M.; Chillaron, J.J.; Pedro-Botet, J.; Flores-Le Roux, J.A. Laparoscopic sleeve gastrectomy: More than a restrictive bariatric surgery procedure? World J. Gastroenterol. 2015, 21, 11804–11814. [Google Scholar] [CrossRef] [PubMed]
- Diamantis, T.; Apostolou, K.G.; Alexandrou, A.; Griniatsos, J.; Felekouras, E.; Tsigris, C. Review of long-term weight loss results after laparoscopic sleeve gastrectomy. Surg. Obes. Relat. Dis. 2014, 10, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Madadi, F.; Jawad, R.; Mousati, I.; Plaeke, P.; Hubens, G. Remission of Type 2 Diabetes and Sleeve Gastrectomy in Morbid Obesity: A Comparative Systematic Review and Meta-analysis. Obes. Surg. 2019, 29, 4066–4076. [Google Scholar] [CrossRef]
- Han, Y.; Jia, Y.; Wang, H.; Cao, L.; Zhao, Y. Comparative analysis of weight loss and resolution of comorbidities between laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass: A systematic review and meta-analysis based on 18 studies. Int. J. Surg. 2020, 76, 101–110. [Google Scholar] [CrossRef]
- Gu, L.; Huang, X.; Li, S.; Mao, D.; Shen, Z.; Khadaroo, P.A.; Ng, D.M.; Chen, P. A meta-analysis of the medium- and long-term effects of laparoscopic sleeve gastrectomy and laparoscopic Roux-en-Y gastric bypass. BMC Surg. 2020, 20, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.; Doumouras, A.G.; Yu, J.; Aditya, I.; Gmora, S.; Anvari, M.; Hong, D. Laparoscopic Sleeve Gastrectomy Versus Laparoscopic Roux-en-Y Gastric Bypass: A Systematic Review and Meta-analysis of Weight Loss, Comorbidities, and Biochemical Outcomes From Randomized Controlled Trials. Ann. Surg. 2021, 273, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Yeung, K.T.D.; Penney, N.; Ashrafian, L.; Darzi, A.; Ashrafian, H. Does Sleeve Gastrectomy Expose the Distal Esophagus to Severe Reflux?: A Systematic Review and Meta-analysis. Ann. Surg. 2020, 271, 257–265. [Google Scholar] [CrossRef]
- Clapp, B.; Wynn, M.; Martyn, C.; Foster, C.; O’Dell, M.; Tyroch, A. Long term (7 or more years) outcomes of the sleeve gastrectomy: A meta-analysis. Surg. Obes. Relat. Dis. 2018, 14, 741–747. [Google Scholar] [CrossRef]
- Angrisani, L.; Santonicola, A.; Iovino, P.; Vitiello, A.; Zundel, N.; Buchwald, H.; Scopinaro, N. Bariatric Surgery and Endoluminal Procedures: IFSO Worldwide Survey 2014. Obes. Surg. 2017, 27, 2279–2289. [Google Scholar] [CrossRef]
- Magema, J.; Himpens, J. “What Really Matters When Performing a Laparoscopic Roux-en Y Gastric Bypass?” Literature-Based Key Steps Towards Success and Standardization of the Procedure. Obes. Surg. 2021, 31, 5441–5445. [Google Scholar] [CrossRef]
- Mahawar, K.K.; Sharples, A.J. Contribution of Malabsorption to Weight Loss After Roux-en-Y Gastric Bypass: A Systematic Review. Obes. Surg. 2017, 27, 2194–2206. [Google Scholar] [CrossRef] [PubMed]
- Golzarand, M.; Toolabi, K.; Farid, R. The bariatric surgery and weight losing: A meta-analysis in the long- and very long-term effects of laparoscopic adjustable gastric banding, laparoscopic Roux-en-Y gastric bypass and laparoscopic sleeve gastrectomy on weight loss in adults. Surg. Endosc. 2017, 31, 4331–4345. [Google Scholar] [CrossRef]
- O’Brien, P.E.; Hindle, A.; Brennan, L.; Skinner, S.; Burton, P.; Smith, A.; Crosthwaite, G.; Brown, W. Long-Term Outcomes After Bariatric Surgery: A Systematic Review and Meta-analysis of Weight Loss at 10 or More Years for All Bariatric Procedures and a Single-Centre Review of 20-Year Outcomes After Adjustable Gastric Banding. Obes. Surg. 2019, 29, 3–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, Y.; Sha, Y.; Yao, G.; Wang, S.; Kong, F.; Liu, H.; Zhang, G.; Zhang, H.; Hu, C.; Zhang, X. Roux-en-Y Gastric Bypass Versus Medical Treatment for Type 2 Diabetes Mellitus in Obese Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Medicine 2016, 95, e3462. [Google Scholar] [CrossRef]
- Yu, Z.; Li, P.; Li, P.; Zhang, H.; Zhang, Y. Meta-analysis of Long-Term Relapse Rate of Type 2 Diabetes Following Initial Remission After Roux-en-Y Gastric Bypass. Obes. Surg. 2021, 31, 5034–5043. [Google Scholar] [CrossRef] [PubMed]
- Lupoli, R.; Lembo, E.; Saldalamacchia, G.; Avola, C.K.; Angrisani, L.; Capaldo, B. Bariatric surgery and long-term nutritional issues. World J. Diabetes 2017, 8, 464–474. [Google Scholar] [CrossRef]
- Christou, N.V.; Look, D.; Maclean, L.D. Weight gain after short- and long-limb gastric bypass in patients followed for longer than 10 years. Ann. Surg. 2006, 244, 734–740. [Google Scholar] [CrossRef]
- Carbajo, M.; Garcia-Caballero, M.; Toledano, M.; Osorio, D.; Garcia-Lanza, C.; Carmona, J.A. One-anastomosis gastric bypass by laparoscopy: Results of the first 209 patients. Obes. Surg. 2005, 15, 398–404. [Google Scholar] [CrossRef]
- De Luca, M.; Piatto, G.; Merola, G.; Himpens, J.; Chevallier, J.M.; Carbajo, M.A.; Mahawar, K.; Sartori, A.; Clemente, N.; Herrera, M.; et al. IFSO Update Position Statement on One Anastomosis Gastric Bypass (OAGB). Obes. Surg. 2021, 31, 3251–3278. [Google Scholar] [CrossRef]
- Parikh, M.; Eisenberg, D.; Johnson, J.; El-Chaar, M.; American Society for Metabolic and Bariatric Surgery Clinical Issues Committee. American Society for Metabolic and Bariatric Surgery review of the literature on one-anastomosis gastric bypass. Surg. Obes. Relat. Dis. 2018, 14, 1088–1092. [Google Scholar] [CrossRef] [PubMed]
- Keleidari, B.; Dehkordi, M.M.; Shahraki, M.S.; Ahmadi, Z.S.; Heidari, M.; Hajian, A.; Nasaj, H.T. Bile reflux after one anastomosis gastric bypass surgery: A review study. Ann. Med. Surg. 2021, 64, 102248. [Google Scholar] [CrossRef] [PubMed]
- Tourky, M.; Issa, M.; Salman, M.A.; Salman, A.; Shaaban, H.E.; Safina, A.; Elias, A.A.; Elewa, A.; Noureldin, K.; Mahmoud, A.A.; et al. Nutritional Complications After Laparoscopic Roux-en-Y Gastric Bypass and One-Anastomosis Gastric Bypass: A Comparative Systematic Review and Meta-Analysis. Cureus 2022, 14, e21114. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Pernaute, A.; Rubio Herrera, M.A.; Perez-Aguirre, E.; Garcia Perez, J.C.; Cabrerizo, L.; Diez Valladares, L.; Fernandez, C.; Talavera, P.; Torres, A. Proximal duodenal-ileal end-to-side bypass with sleeve gastrectomy: Proposed technique. Obes. Surg. 2007, 17, 1614–1618. [Google Scholar] [CrossRef]
- Verhoeff, K.; Mocanu, V.; Zalasky, A.; Dang, J.; Kung, J.Y.; Switzer, N.J.; Birch, D.W.; Karmali, S. Evaluation of Metabolic Outcomes Following SADI-S: A Systematic Review and Meta-analysis. Obes. Surg. 2022, 32, 1049–1063. [Google Scholar] [CrossRef]
- Sanchez-Pernaute, A.; Herrera, M.A.R.; Ferre, N.P.; Rodriguez, C.S.; Marcuello, C.; Panella, C.; Antonanzas, L.L.; Torres, A.; Perez-Aguirre, E. Long-Term Results of Single-Anastomosis Duodeno-ileal Bypass with Sleeve Gastrectomy (SADI-S). Obes. Surg. 2022, 32, 682–689. [Google Scholar] [CrossRef]
- Chierici, A.; Chevalier, N.; Iannelli, A. Postoperative morbidity and weight loss after revisional bariatric surgery for primary failed restrictive procedure: A systematic review and network meta-analysis. Int. J. Surg. 2022, 102, 106677. [Google Scholar] [CrossRef]
- Wehrtmann, F.S.; de la Garza, J.R.; Kowalewski, K.F.; Schmidt, M.W.; Muller, K.; Tapking, C.; Probst, P.; Diener, M.K.; Fischer, L.; Muller-Stich, B.P.; et al. Learning Curves of Laparoscopic Roux-en-Y Gastric Bypass and Sleeve Gastrectomy in Bariatric Surgery: A Systematic Review and Introduction of a Standardization. Obes. Surg. 2020, 30, 640–656. [Google Scholar] [CrossRef]
- Hasson, H.M. A modified instrument and method for laparoscopy. Am. J. Obstet. Gynecol. 1971, 110, 886–887. [Google Scholar] [CrossRef]
- Kassir, R.; Blanc, P.; Lointier, P.; Tiffet, O.; Berger, J.L.; Amor, I.B.; Gugenheim, J. Laparoscopic entry techniques in obese patient: Veress needle, direct trocar insertion or open entry technique? Obes. Surg. 2014, 24, 2193–2194. [Google Scholar] [CrossRef]
- Deffieux, X.; Ballester, M.; Collinet, P.; Fauconnier, A.; Pierre, F. Risks associated with laparoscopic entry: Guidelines for clinical practice from the French College of Gynaecologists and Obstetricians. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 158, 159–166. [Google Scholar] [CrossRef]
- Shahabi, S.; Carbajo, M.; Nimeri, A.; Kermansaravi, M.; Jazi, A.H.D.; Pazouki, A.; Mahawar, K. Factors that make Bariatric Surgery Technically Challenging: A Survey of 370 Bariatric Surgeons. World J. Surg. 2021, 45, 2521–2528. [Google Scholar] [CrossRef] [PubMed]
- Ertugrul, I.; Kayaalp, C.; Yagci, M.A.; Sumer, F.; Karagul, S.; Tolan, K. Comparison of Direct Trocar Entry and Veress Needle Entry in Laparoscopic Bariatric Surgery: Randomized Controlled Trial. J. Laparoendosc. Adv. Surg. Tech. A 2015, 25, 875–879. [Google Scholar] [CrossRef]
- Ikechebelu, J.I.; Eleje, G.U.; Joe-Ikechebelu, N.N.; Okafor, C.D.; Okpala, B.C.; Ugwu, E.O.; Nwachukwu, C.E.; Okoro, C.C.; Okam, P.C. Randomized control trial on effectiveness and safety of direct trocar versus Veress needle entry techniques in obese women during diagnostic laparoscopy. Arch. Gynecol. Obstet. 2021, 304, 815–822. [Google Scholar] [CrossRef]
- Brandt, H.G.; Jepsen, C.H.; Hendriksen, O.M.; Lindekaer, A.; Skjonnemand, M. The use of ultrasound to identify veins for peripheral venous access in morbidly obese patients. Dan. Med. J. 2016, 63, A5191. [Google Scholar]
- Wang, T.; Sun, S.; Huang, S. The association of body mass index with difficult tracheal intubation management by direct laryngoscopy: A meta-analysis. BMC Anesthesiol. 2018, 18, 79. [Google Scholar] [CrossRef]
- De Jong, A.; Molinari, N.; Pouzeratte, Y.; Verzilli, D.; Chanques, G.; Jung, B.; Futier, E.; Perrigault, P.F.; Colson, P.; Capdevila, X.; et al. Difficult intubation in obese patients: Incidence, risk factors, and complications in the operating theatre and in intensive care units. Br. J. Anaesth. 2015, 114, 297–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galinski, M.; Chouteau, M.; Lunghi, G.; Vinurel, M.; Blazy, B.; Cher, M.; Alouane, B.; Bento, H.; Germain, J.L.; Barrat, C.; et al. Multivariate Analysis of the Failure Risk of First Tracheal Intubation Attempt in a Population of Patients Scheduled for Bariatric Surgery. Obes. Surg. 2021, 31, 4392–4398. [Google Scholar] [CrossRef]
- Hashim, M.M.; Ismail, M.A.; Esmat, A.M.; Adeel, S. Difficult tracheal intubation in bariatric surgery patients, a myth or reality? Br. J. Anaesth. 2016, 116, 557–558. [Google Scholar] [CrossRef] [Green Version]
- Lekkala, S.; Taylor, E.A.; Hunt, H.B.; Donnelly, E. Effects of Diabetes on Bone Material Properties. Curr. Osteoporos Rep. 2019, 17, 455–464. [Google Scholar] [CrossRef]
- de Raaff, C.A.L.; Gorter-Stam, M.A.W.; de Vries, N.; Sinha, A.C.; Jaap Bonjer, H.; Chung, F.; Coblijn, U.K.; Dahan, A.; van den Helder, R.S.; Hilgevoord, A.A.J.; et al. Perioperative management of obstructive sleep apnea in bariatric surgery: A consensus guideline. Surg. Obes. Relat. Dis. 2017, 13, 1095–1109. [Google Scholar] [CrossRef] [PubMed]
- Raveendran, R.; Wong, J.; Singh, M.; Wong, D.T.; Chung, F. Obesity hypoventilation syndrome, sleep apnea, overlap syndrome: Perioperative management to prevent complications. Curr. Opin. Anaesthesiol. 2017, 30, 146–155. [Google Scholar] [CrossRef]
- Bazurro, S.; Ball, L.; Pelosi, P. Perioperative management of obese patient. Curr. Opin. Crit. Care 2018, 24, 560–567. [Google Scholar] [CrossRef] [PubMed]
- Kaw, R.; Wong, J.; Mokhlesi, B. Obesity and Obesity Hypoventilation, Sleep Hypoventilation, and Postoperative Respiratory Failure. Anesth. Analg. 2021, 132, 1265–1273. [Google Scholar] [CrossRef]
- Singh, P.M.; Panwar, R.; Borle, A.; Goudra, B.; Trikha, A.; van Wagensveld, B.A.; Sinha, A. Efficiency and Safety Effects of Applying ERAS Protocols to Bariatric Surgery: A Systematic Review with Meta-Analysis and Trial Sequential Analysis of Evidence. Obes. Surg. 2017, 27, 489–501. [Google Scholar] [CrossRef]
- Smit, C.; De Hoogd, S.; Bruggemann, R.J.M.; Knibbe, C.A.J. Obesity and drug pharmacology: A review of the influence of obesity on pharmacokinetic and pharmacodynamic parameters. Expert. Opin. Drug. Metab. Toxicol. 2018, 14, 275–285. [Google Scholar] [CrossRef]
- Eisenberg, D.; Shikora, S.A.; Aarts, E.; Aminian, A.; Angrisani, L.; Cohen, R.V.; De Luca, M.; Faria, S.L.; Goodpaster, K.P.S.; Haddad, A.; et al. 2022 American Society for Metabolic and Bariatric Surgery (ASMBS) and International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO): Indications for Metabolic and Bariatric Surgery. Surg. Obes. Relat. Dis. 2022, 18, 1345–1356. [Google Scholar] [CrossRef] [PubMed]
- Drai, C.; Chierici, A.; Schiavo, L.; Mazahreh, T.S.; Schneck, A.S.; Iannelli, A. Long-Term Results at 10 Years of Pouch Resizing for Roux-en-Y Gastric Bypass Failure. Nutrients 2022, 14, 4035. [Google Scholar] [CrossRef]
- Iannelli, A.; Schneck, A.S.; Hebuterne, X.; Gugenheim, J. Gastric pouch resizing for Roux-en-Y gastric bypass failure in patients with a dilated pouch. Surg. Obes. Relat. Dis. 2013, 9, 260–267. [Google Scholar] [CrossRef]
- Sarno, G.; Calabrese, P.; Frias-Toral, E.; Ceriani, F.; Fuchs-Tarlovsky, V.; Spagnuolo, M.; Cucalon, G.; Cordova, L.A.; Schiavo, L.; Pilone, V. The relationship between preoperative weight loss and intra and post-bariatric surgery complications: An appraisal of the current preoperative nutritional strategies. Crit. Rev. Food Sci. Nutr. 2022, 1–9. [Google Scholar] [CrossRef]
- Schiavo, L.; Pilone, V.; Rossetti, G.; Iannelli, A. The Role of the Nutritionist in a Multidisciplinary Bariatric Surgery Team. Obes. Surg. 2019, 29, 1028–1030. [Google Scholar] [CrossRef]
- Paoli, A.; Rubini, A.; Volek, J.S.; Grimaldi, K.A. Beyond weight loss: A review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets. Eur. J. Clin. Nutr. 2013, 67, 789–796. [Google Scholar] [CrossRef] [Green Version]
- Colangeli, L.; Gentileschi, P.; Sbraccia, P.; Guglielmi, V. Ketogenic Diet for Preoperative Weight Reduction in Bariatric Surgery: A Narrative Review. Nutrients 2022, 14, 3610. [Google Scholar] [CrossRef]
- Carter, J.; Chang, J.; Birriel, T.J.; Moustarah, F.; Sogg, S.; Goodpaster, K.; Benson-Davies, S.; Chapmon, K.; Eisenberg, D. ASMBS position statement on preoperative patient optimization before metabolic and bariatric surgery. Surg. Obes. Relat. Dis. 2021, 17, 1956–1976. [Google Scholar] [CrossRef]
- Pilone, V.; Tramontano, S.; Renzulli, M.; Romano, M.; Cobellis, L.; Berselli, T.; Schiavo, L. Metabolic effects, safety, and acceptability of very low-calorie ketogenic dietetic scheme on candidates for bariatric surgery. Surg. Obes. Relat. Dis. 2018, 14, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Schiavo, L.; De Stefano, G.; Persico, F.; Gargiulo, S.; Di Spirito, F.; Griguolo, G.; Petrucciani, N.; Fontas, E.; Iannelli, A.; Pilone, V. A Randomized, Controlled Trial Comparing the Impact of a Low-Calorie Ketogenic vs a Standard Low-Calorie Diet on Fat-Free Mass in Patients Receiving an Elipse Intragastric Balloon Treatment. Obes. Surg. 2021, 31, 1514–1523. [Google Scholar] [CrossRef] [PubMed]
- Schiavo, L.; Pierro, R.; Asteria, C.; Calabrese, P.; Di Biasio, A.; Coluzzi, I.; Severino, L.; Giovanelli, A.; Pilone, V.; Silecchia, G. Low-Calorie Ketogenic Diet with Continuous Positive Airway Pressure to Alleviate Severe Obstructive Sleep Apnea Syndrome in Patients with Obesity Scheduled for Bariatric/Metabolic Surgery: A Pilot, Prospective, Randomized Multicenter Comparative Study. Obes. Surg. 2022, 32, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Lau, D.C.; Douketis, J.D.; Morrison, K.M.; Hramiak, I.M.; Sharma, A.M.; Ur, E.; Obesity Canada Clinical Practice Guidelines Expert, P. 2006 Canadian clinical practice guidelines on the management and prevention of obesity in adults and children [summary]. CMAJ 2007, 176, S1–S13. [Google Scholar] [CrossRef] [Green Version]
- Sadhasivam, S.; Larson, C.J.; Lambert, P.J.; Mathiason, M.A.; Kothari, S.N. Refusals, denials, and patient choice: Reasons prospective patients do not undergo bariatric surgery. Surg. Obes. Relat. Dis. 2007, 3, 531–535; discussion 535–536. [Google Scholar] [CrossRef]
- van de Weijgert, E.J.; Ruseler, C.H.; Elte, J.W. Long-term follow-up after gastric surgery for morbid obesity: Preoperative weight loss improves the long-term control of morbid obesity after vertical banded gastroplasty. Obes. Surg. 1999, 9, 426–432. [Google Scholar] [CrossRef]
- Gastrointestinal surgery for severe obesity: National Institutes of Health Consensus Development Conference Statement. Am. J. Clin. Nutr. 1992, 55, 615S–619S. [CrossRef]


{kind=link}
| Regimen OPOD | ||
|---|---|---|
| VLCKD (Days 1–10) | VLCD (Days 11–20) | LCD (Days 21–30) |
Take 8–9 * scoops (one scoop = 10 g; 0.3 g of carbohydrates; 8.2 g of protein; 0.4 g of fats) of ketogenic powder per day each diluted in 100–200 mL of water and oral supplements as follows:
Limit physical activity and excessive stress. Free consumption of vegetables at lunch and dinner (minimum 500 g day). Allowed—20 g of extra virgin olive oil per day. Daily energy intake 560–595 Kcal:
| Stop VLCKD treatment and oral supplements. Start a very low-calorie diet as follows:
Daily energy intake 810 Kcal:
| Increase the amount of carbohydrates as the following scheme:
Daily energy intake 1100 Kcal:
|
| Meal | |
|---|---|
| Breakfast | Two measuring cups of protein powder in water or yogurt with a fat content of 0.1% (either plain or fruit-flavoured). Coffee is also acceptable. |
| Lunch* | A total of 180 g of animal proteins (such as beef, calf, rabbit meat, chicken, or turkey breast) or 200 g of fish proteins (such as anchovies, sardines, tuna, mackerel, lobster, shrimps, pike, cod, rhombus, sole, sea bass, grouper, snapper, sea bream, cuttlefish, squid, octopus, salmon, or swordfish) or 200 g of plant-based proteins (such as tofu, seitan, or tempeh), along with 200 g of vegetables (such as chard, chicory, zucchini, cauliflower, fennel, eggplant, broccoli, lettuce, radish, artichoke, or spinach). |
| Dinner * | Four measuring cups of protein powder in water or yogurt with a fat content of 0.1% (either plain or fruit-flavoured), along with 200 g of vegetables (such as chard, chicory, zucchini, cauliflower, fennel, eggplant, broccoli, lettuce, radish, artichoke, or spinach). |
| Meal | |
|---|---|
| Breakfast | Egg (100 g), salt (0.13 g), pepper (0.033 g), olive oil (5 g) |
| Snack | Nuts (30 g) |
| Lunch | Lamb loin 145 g), olive oil (10 g), salt (1.5 g), pepper (0.13 g), asparagus (143 g) |
| Snack | Cheddar cheese (30 g) |
| Dinner | Ketocompleat (40 g), water (250 mL) |
Total calories 1215.4 kcal:
| |
| Reference | Population | Aim and Intervention | Findings |
|---|---|---|---|
| Leonetti et al. [108] | 19 M; 31 F | Assessment of the effectiveness of a sequential diet regimen termed the OPOD in morbidly obese patients with and without type 2 diabetes mellitus scheduled for bariatric surgery. OPOD regimen: VLCKD for 10 days; VLCD for 10 days; LCD for 10 days. | Reduction in body weight, body mass index, waist circumference, and neck circumference; amelioration in fasting plasma glucose levels; reduction in liver volume; and improvement of liver steatosis. |
| Albanese et al. [30] | 39 M; 139 F | Compared surgical outcome and weight loss in two groups of patients who were offered two different pre-operative diets: VLCD and VLCKD: 72 patients followed a pre-operative VLCKD and 106 a VLCD. | Absolute weight loss was significantly better in the VLCKD than in the VLCD group, while no significant differences were observed in % of excess body mass index loss. VLCKD showed better results than VLCD on surgical outcome, influencing drainage output, post-operative haemoglobin levels, and hospital stay. |
| Pilone et al. [109] | 44 M; 75 F | Evaluation of safety, efficacy, and acceptability of a VLCKD in patients before bariatric surgery using a sequential diet regimen: VLCKD for 10 days, followed by a hypocaloric scheme for 20 days, with the progressive recovery of calorie levels. | Weight, body mass index, waist circumference, and visceral fat decreased significantly. Furthermore, a significant improvement in several clinical parameters, including liver volume and glycaemic and lipid profile parameters were observed. The majority of patients declared themselves satisfied or very satisfied. The adverse effects were mild, of short duration, and not clinically relevant. |
| Schiavo et al. [110] | 10 M; 17 F | To assess the safety and the effectiveness of a 4-week preoperative KMED in reducing body weight and left hepatic lobe volume in patients scheduled for bariatric surgery. Ketogenic food plan (from 1150 to 1250 kcal/day) consisted of 4% carbohydrates, 71% fats, and 25% proteins. Dinner was substituted by Ketocompleat (MVMedical Solutions, Serravalle, Repubblica San Marino). Ketocompleat is a supplement included on the register of food supplements of the Italian Minister of Health (code number 94721), and due to its carbohydrate-free formulation, may be associated to a low-carbohydrate ketogenic diet. | The study indicates that a 4-week preoperative KMED is safe and effective in reducing body weight and left hepatic lobe volume in patients with obesity scheduled for bariatric surgery. |
| Schiavo et al. [111] | 22 M; 26 F | To prospectively compare the effects on weight loss, fat mass, fat-free mass, and resting metabolic rate in two groups of patients who were randomized to two different diets: LCKD and a standard LCD after intragastric balloon placement. The macronutrients composition of the LCD and LCKD was 40% carbohydrates, 43% proteins, and 15% fats (~ 1200 kcal/day) and 4% carbohydrates, 25% proteins, and 71% fats (~ 1200 kcal/day), respectively. | The LCKD group showed a significantly lower decrease in free fat mass and resting metabolic rate when compared with the LCD group. Fat mass decreased more significantly with LCKD compared to LCD, without negative impact on renal function. |
| Schiavo et al. [112] | 44 M; 26 F | To assess the clinical advantage of pre-bariatric surgery CPAP alone or in combination with a LCKD on apnoea–hypopnoea index and CRP levels in patients with obesity and obstructive sleep apnoea syndrome. The ketogenic food plan (from 1150 to 1250 kcal/day) consisted of 4% carbohydrates, 71% fats, and 25% proteins. Dinner was substituted by Ketocompleat (MVMedical Solutions, Serravalle, Repubblica San Marino) | Apnoea–hypopnea index scores improved significantly in both groups. Combining CPAP and LCKD registered no advantage on the apnoea–hypopnoea index score. Furthermore, CPAP + LCKD had a greater impact on CRP levels than CPAP alone demonstrating a positive impact on chronic inflammatory status. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barrea, L.; Verde, L.; Schiavo, L.; Sarno, G.; Camajani, E.; Iannelli, A.; Caprio, M.; Pilone, V.; Colao, A.; Muscogiuri, G. Very Low-Calorie Ketogenic Diet (VLCKD) as Pre-Operative First-Line Dietary Therapy in Patients with Obesity Who Are Candidates for Bariatric Surgery. Nutrients 2023, 15, 1907. https://doi.org/10.3390/nu15081907
Barrea L, Verde L, Schiavo L, Sarno G, Camajani E, Iannelli A, Caprio M, Pilone V, Colao A, Muscogiuri G. Very Low-Calorie Ketogenic Diet (VLCKD) as Pre-Operative First-Line Dietary Therapy in Patients with Obesity Who Are Candidates for Bariatric Surgery. Nutrients. 2023; 15(8):1907. https://doi.org/10.3390/nu15081907
Chicago/Turabian StyleBarrea, Luigi, Ludovica Verde, Luigi Schiavo, Gerardo Sarno, Elisabetta Camajani, Antonio Iannelli, Massimiliano Caprio, Vincenzo Pilone, Annamaria Colao, and Giovanna Muscogiuri. 2023. "Very Low-Calorie Ketogenic Diet (VLCKD) as Pre-Operative First-Line Dietary Therapy in Patients with Obesity Who Are Candidates for Bariatric Surgery" Nutrients 15, no. 8: 1907. https://doi.org/10.3390/nu15081907
APA StyleBarrea, L., Verde, L., Schiavo, L., Sarno, G., Camajani, E., Iannelli, A., Caprio, M., Pilone, V., Colao, A., & Muscogiuri, G. (2023). Very Low-Calorie Ketogenic Diet (VLCKD) as Pre-Operative First-Line Dietary Therapy in Patients with Obesity Who Are Candidates for Bariatric Surgery. Nutrients, 15(8), 1907. https://doi.org/10.3390/nu15081907