
Prognostic Value of Nutritional Assessments on Overall Survival in Head and Neck Cancer Survivors with Radiation-Induced Brain Necrosis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
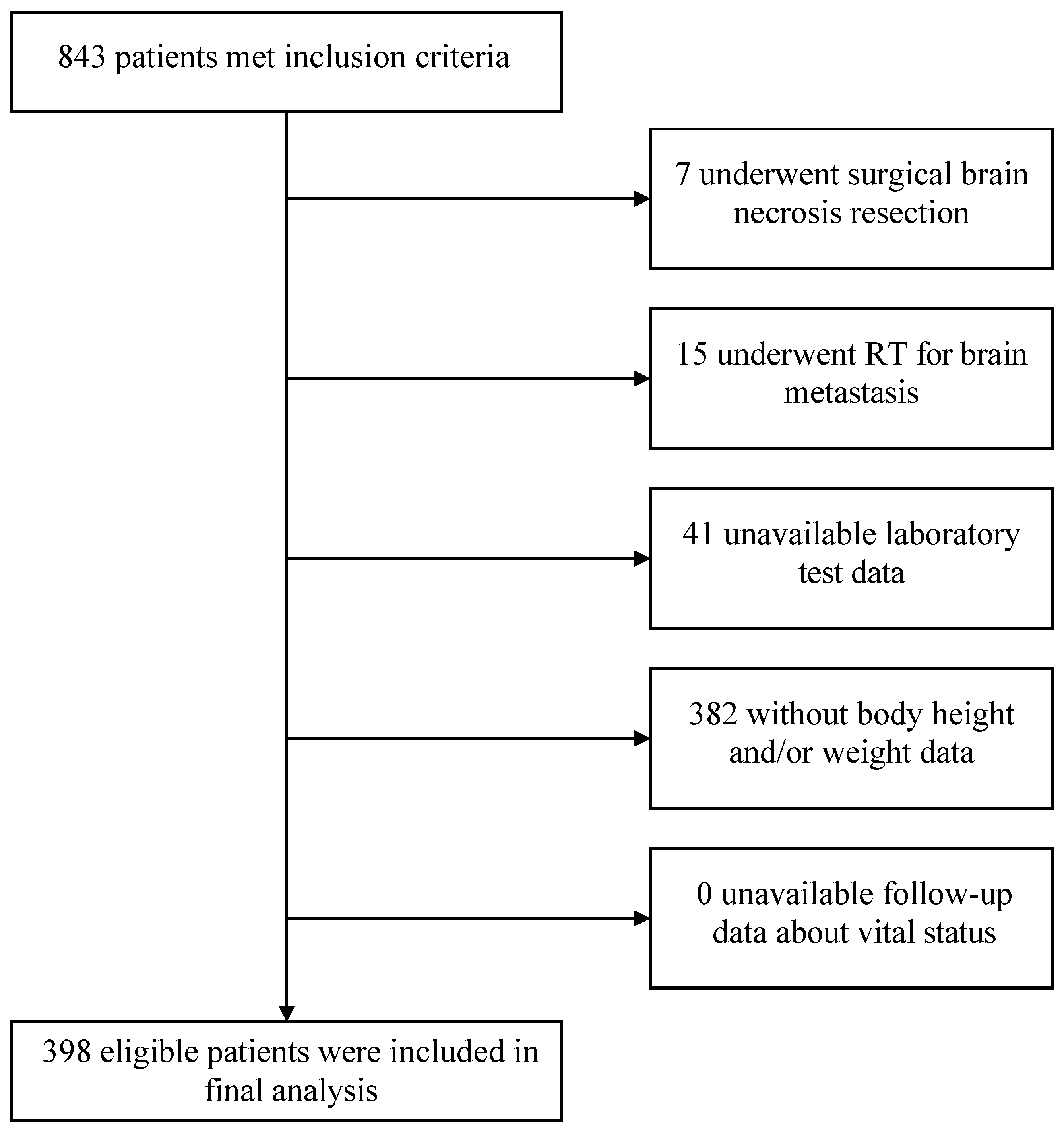
2.1. Study Design and Patients
2.2. Data Collection
2.3. Assessments of Baseline Nutritional Risk Status
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Cohort Characteristics
3.2. Nutritional Risk Status on Post-RN Survival Using Cox Regression Models
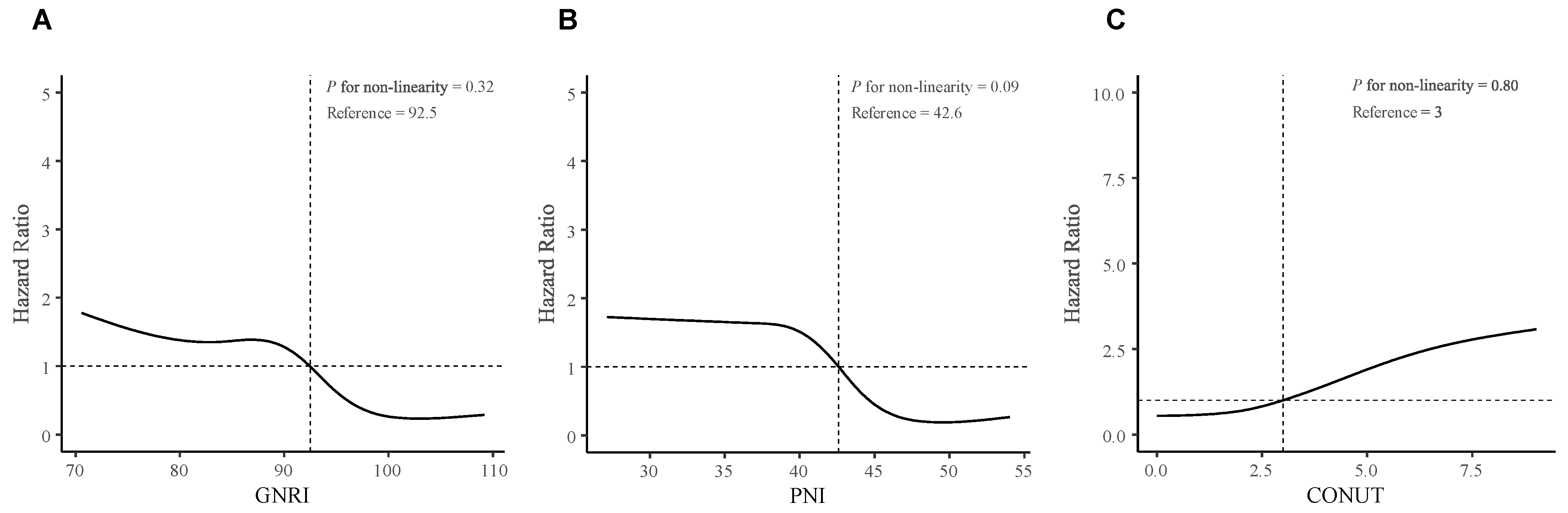
3.3. Examination of Nonlinear Associations and the Optimal Cut-off Points of All Three Nutritional Risk Indices
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Na, A.; Haghigi, N.; Drummond, K.J. Cerebral radiation necrosis. Asia Pac. J. Clin. Oncol. 2014, 10, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Ali, F.S.; Arevalo, O.; Zorofchian, S.; Patrizz, A.; Riascos, R.; Tandon, N.; Blanco, A.; Ballester, L.Y.; Esquenazi, Y. Cerebral Radiation Necrosis: Incidence, Pathogenesis, Diagnostic Challenges, and Future Opportunities. Curr. Oncol. Rep. 2019, 21, 66. [Google Scholar] [CrossRef] [PubMed]
- Rahmathulla, G.; Marko, N.F.; Weil, R.J. Cerebral radiation necrosis: A review of the pathobiology, diagnosis and management considerations. J. Clin. Neurosci. 2013, 20, 485–502. [Google Scholar] [CrossRef]
- Chen, J.; Dassarath, M.; Yin, Z.; Liu, H.; Yang, K.; Wu, G. Radiation induced temporal lobe necrosis in patients with nasopharyngeal carcinoma: A review of new avenues in its management. Radiat. Oncol. 2011, 6, 128. [Google Scholar] [CrossRef]
- Kitpanit, S.; Lee, A.; Pitter, K.L.; Fan, D.; Chow, J.C.H.; Neal, B.; Han, Z.; Fox, P.; Sine, K.; Mah, D.; et al. Temporal Lobe Necrosis in Head and Neck Cancer Patients after Proton Therapy to the Skull Base. Int. J. Part Ther. 2020, 6, 17–28. [Google Scholar] [CrossRef]
- Hebuterne, X.; Lemarie, E.; Michallet, M.; de Montreuil, C.B.; Schneider, S.M.; Goldwasser, F. Prevalence of malnutrition and current use of nutrition support in patients with cancer. JPEN J. Parenter. Enteral. Nutr. 2014, 38, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Bossi, P.; Delrio, P.; Mascheroni, A.; Zanetti, M. The Spectrum of Malnutrition/Cachexia/Sarcopenia in Oncology According to Different Cancer Types and Settings: A Narrative Review. Nutrients 2021, 13, 1980. [Google Scholar] [CrossRef]
- Kristensen, M.B.; Isenring, E.; Brown, B. Nutrition and swallowing therapy strategies for patients with head and neck cancer. Nutrition 2020, 69, 110548. [Google Scholar] [CrossRef]
- Li, H.; Li, L.; Huang, X.; Li, Y.; Zou, T.; Zhuo, X.; Chen, Y.; Liu, Y.; Tang, Y. Radiotherapy-induced dysphagia and its impact on quality of life in patients with nasopharyngeal carcinoma. Strahlenther. Onkol. 2019, 195, 457–467. [Google Scholar] [CrossRef]
- Bullock, A.F.; Greenley, S.L.; McKenzie, G.A.G.; Paton, L.W.; Johnson, M.J. Relationship between markers of malnutrition and clinical outcomes in older adults with cancer: Systematic review, narrative synthesis and meta-analysis. Eur. J. Clin. Nutr. 2020, 74, 1519–1535. [Google Scholar] [CrossRef]
- Zhang, X.; Edwards, B.J. Malnutrition in Older Adults with Cancer. Curr. Oncol. Rep. 2019, 21, 80. [Google Scholar] [CrossRef]
- Zhang, X.; Pang, L.; Sharma, S.V.; Li, R.; Nyitray, A.G.; Edwards, B.J. Malnutrition and overall survival in older patients with cancer. Clin. Nutr. 2021, 40, 966–977. [Google Scholar] [CrossRef] [PubMed]
- Martino, A.; Krainik, A.; Pasteris, C.; Hoffmann, D.; Chabardes, S.; Berger, F.; Le Bas, J.F.; Cantin, S.; Attye, A.; Grand, S. Neurological imaging of brain damages after radiotherapy and/or chimiotherapy. J. Neuroradiol. 2014, 41, 52–70. [Google Scholar] [CrossRef] [PubMed]
- Carr, C.M.; Benson, J.C.; DeLone, D.R.; Diehn, F.E.; Kim, D.K.; Merrell, K.W.; Nagelschneider, A.A.; Madhavan, A.A.; Johnson, D.R. Intracranial long-term complications of radiation therapy: An image-based review. Neuroradiology 2021, 63, 471–482. [Google Scholar] [CrossRef] [PubMed]
- Buzby, G.P.; Knox, L.S.; Crosby, L.O.; Eisenberg, J.M.; Haakenson, C.M.; McNeal, G.E.; Page, C.P.; Peterson, O.L.; Reinhardt, G.F.; Williford, W.O. Study protocol: A randomized clinical trial of total parenteral nutrition in malnourished surgical patients. Am. J. Clin. Nutr. 1988, 47, 366–381. [Google Scholar] [CrossRef]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef]
- Minamisawa, M.; Seidelmann, S.B.; Claggett, B.; Hegde, S.M.; Shah, A.M.; Desai, A.S.; Lewis, E.F.; Shah, S.J.; Sweitzer, N.K.; Fang, J.C.; et al. Impact of Malnutrition Using Geriatric Nutritional Risk Index in Heart Failure With Preserved Ejection Fraction. JACC Heart Fail 2019, 7, 664–675. [Google Scholar] [CrossRef]
- Li, H.; Cen, K.; Sun, W.; Feng, B. Prognostic value of geriatric nutritional risk index in elderly patients with heart failure: A meta-analysis. Aging Clin. Exp. Res. 2021, 33, 1477–1486. [Google Scholar] [CrossRef]
- Smale, B.F.; Mullen, J.L.; Buzby, G.P.; Rosato, E.F. The efficacy of nutritional assessment and support in cancer surgery. Cancer 1981, 47, 2375–2381. [Google Scholar] [CrossRef]
- Buzby, G.P.; Mullen, J.L.; Matthews, D.C.; Hobbs, C.L.; Rosato, E.F. Prognostic nutritional index in gastrointestinal surgery. Am. J. Surg. 1980, 139, 160–167. [Google Scholar] [CrossRef]
- Sugita, Y.; Miyazaki, T.; Shimada, K.; Shimizu, M.; Kunimoto, M.; Ouchi, S.; Aikawa, T.; Kadoguchi, T.; Kawaguchi, Y.; Shiozawa, T.; et al. Correlation of Nutritional Indices on Admission to the Coronary Intensive Care Unit with the Development of Delirium. Nutrients 2018, 10, 1712. [Google Scholar] [CrossRef] [PubMed]
- Yuan, K.; Zhu, S.; Wang, H.; Chen, J.; Zhang, X.; Xu, P.; Xie, Y.; Zhu, X.; Zhu, W.; Sun, W.; et al. Association between malnutrition and long-term mortality in older adults with ischemic stroke. Clin. Nutr. 2021, 40, 2535–2542. [Google Scholar] [CrossRef]
- Ignacio de Ulibarri, J.; Gonzalez-Madrono, A.; de Villar, N.G.; Gonzalez, P.; Gonzalez, B.; Mancha, A.; Rodriguez, F.; Fernandez, G. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar] [PubMed]
- Camp, R.L.; Dolled-Filhart, M.; Rimm, D.L. X-tile: A new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin. Cancer Res. 2004, 10, 7252–7259. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Cai, J.; Li, Y.; Rong, X.; Li, Y.; He, L.; Li, H.; Liang, Y.; Huang, H.; Xu, Y.; et al. Baseline Objective Malnutritional Indices as Immune-Nutritional Predictors of Long-Term Recurrence in Patients with Acute Ischemic Stroke. Nutrients 2022, 14, 1337. [Google Scholar] [CrossRef]
- Pan, D.; Rong, X.; Zhu, Y.; Ng, W.T.; Chen, D.; Li, H.; Xu, Y.; Tang, Y.; Radiation Oncology Palliative Care Collaborative, G. A novel nomogram to predict overall survival in head and neck cancer survivors with radiation-induced brain necrosis. Radiother. Oncol. 2022, 168, 121–129. [Google Scholar] [CrossRef]
- Aggarwal, P.; Zaveri, J.S.; Goepfert, R.P.; Shi, Q.; Du, X.L.; Swartz, M.; Lai, S.Y.; Fuller, C.D.; Lewin, J.S.; Piller, L.B.; et al. Swallowing-related outcomes associated with late lower cranial neuropathy in long-term oropharyngeal cancer survivors: Cross-sectional survey analysis. Head Neck 2019, 41, 3880–3894. [Google Scholar] [CrossRef]
- Cereda, E.; Vanotti, A. The new Geriatric Nutritional Risk Index is a good predictor of muscle dysfunction in institutionalized older patients. Clin. Nutr. 2007, 26, 78–83. [Google Scholar] [CrossRef]
- Cederholm, T.; Jensen, G.L.; Correia, M.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Serum albumin, g/L | level | ≥35 | 30–34.9 | 25–29.9 | <25 |
| point | 0 | 2 | 4 | 6 | |
| Total cholesterol, mg/dL | level | ≥180 | 140–179 | 100–139 | <100 |
| point | 0 | 1 | 2 | 3 | |
| Lymphocyte count, ×109/L | level | ≥1.60 | 1.20–1.59 | 0.80–1.19 | <0.80 |
| point | 0 | 1 | 2 | 3 | |
| CONUT score | point | 0–1 | 2–4 | 5–8 | 9–12 |
| Risk strata | Absent risk | Mild risk | Moderate risk | Severe risk |
| Baseline Characteristics | All | Alive | Dead | p-Values |
|---|---|---|---|---|
| N = 398 | N = 356 | N = 42 | ||
| Sex—male, n (%) | 291 (73.1%) | 256 (71.9%) | 35 (83.3%) | 0.16 |
| Age—yrs, median (IQR) | 50.9 (44.5–57.0) | 50.6 (43.9–56.6) | 53.8 (45.9–60.2) | 0.08 |
| Follow-up period—yrs, median (IQR) | 2.3 (1.1–3.6) | 2.3 (1.2–3.6) | 1.4 (0.7–3.3) | 0.02 |
| GNRI—point, median (IQR) | 92.4 (83.1–99.5) | 93.2 (83.4–99.9) | 86.9 (78.3–95.5) | 0.02 |
| GNRI strata | 0.10 | |||
| >98—Absent risk | 128 (32.2%) | 119 (33.4%) | 9 (21.4%) | |
| >92, ≤98—Mild risk | 77 (19.3%) | 71 (19.9%) | 6 (14.3%) | |
| >82, ≤92—Moderate risk | 104 (26.1%) | 92 (25.8%) | 12 (28.6%) | |
| ≤82—Severe risk | 89 (22.4%) | 74 (20.8%) | 15 (35.7%) | |
| PNI—point, median (IQR) | 42.6 (36.5–47.2) | 42.8 (37.1–47.3) | 38.9 (34.0–43.3) | 0.02 |
| PNI strata | 0.03 | |||
| >38—Absent risk | 278 (69.8%) | 256 (71.9%) | 22 (52.4%) | |
| >35, ≤38—Moderate risk | 38 (9.5%) | 31 (8.7%) | 7 (16.7%) | |
| ≤35—Severe risk | 82 (20.6%) | 69 (19.4%) | 13 (31.0%) | |
| CONUT—point, median (IQR) | 3.0 (2.0–5.0) | 3.0 (1.0–5.0) | 4.0 (2.0–6.0) | 0.01 |
| CONUT strata | 0.05 | |||
| 0~1—Absent risk | 99 (24.9%) | 92 (25.8%) | 7 (16.7%) | |
| 2~4—Mild risk | 187 (47.0%) | 171 (48.0%) | 16 (38.1%) | |
| 5~8—Moderate risk | 90 (22.6%) | 76 (21.3%) | 14 (33.3%) | |
| 9~12—Severe risk | 22 (5.5%) | 17 (4.8%) | 5 (11.9%) | |
| Height—cm, mean (SD) | 165.4 (7.3) | 165.2 (7.3) | 166.9 (7.0) | 0.15 |
| Weight—kg, mean (SD) | 59.1 (10.7) | 59.3 (10.9) | 57.1 (8.4) | 0.12 |
| BMI—kg/m2, mean (SD) | 21.5 (3.2) | 21.7 (3.2) | 20.5 (3.0) | 0.03 |
| Tumor progression before RN—Yes, n (%) | 47 (11.8%) | 40 (11.2%) | 7 (16.7%) | 0.31 |
| Lower cranial nerves injury—Yes, n (%) | 177 (44.5%) | 150 (42.1%) | 27 (64.3%) | 0.01 |
| Hypertension—Yes, n (%) | 47 (11.8%) | 41 (11.5%) | 6 (14.3%) | 0.61 |
| Diabetes—Yes, n (%) | 15 (3.8%) | 14 (3.9%) | 1 (2.4%) | >0.99 |
| Stroke—Yes, n (%) | 33 (8.3%) | 29 (8.1%) | 4 (9.5%) | 0.77 |
| Cigarette Smoking—Yes, n (%) | 57 (14.3%) | 52 (14.6%) | 5 (11.9%) | 0.81 |
| Alcohol consumption—Yes, n (%) | 24 (6.0%) | 20 (5.6%) | 4 (9.5%) | 0.30 |
| Laboratory tests—median (IQR) | ||||
| Red blood cells—×10^9/L | 4.4 (4.1–4.8) | 4.4 (4.1–4.8) | 4.5 (4.1–4.7) | 0.93 |
| Hemoglobin—g/L | 129.1 (16.5) | 129.6 (16.0) | 124.6 (19.5) | 0.12 |
| White blood cells—×10^9/L | 5.6 (4.5–7.0) | 5.6 (4.4–6.9) | 6.2 (4.7–7.6) | 0.15 |
| Neutrophils—×10^9/L | 3.7 (2.7–5.2) | 3.7 (2.7–5.0) | 4.6 (3.2–5.6) | 0.01 |
| Lymphocyte—×10^9/L | 1.2 (0.9–1.5) | 1.2 (0.9–1.6) | 1.0 (0.8–1.2) | 0.01 |
| Total cholesterol—mg/dL | 196 (167–222) | 197 (168–223) | 182 (159–205) | 0.07 |
| Albumin—g/L | 36.7 (30.1–40.5) | 36.8 (30.2–40.7) | 34.4 (28.2–38.3) | 0.09 |
| Brain MRI assessment—n (%) | ||||
| Bilateral necrosis | 181 (45.5%) | 158 (44.4%) | 23 (54.8%) | 0.27 |
| Involving ≥2 brain regions | 73 (18.3%) | 55 (15.4%) | 18 (42.9%) | <0.001 |
| Anti-RN treatment—n (%) | ||||
| Corticosteroids | 176 (44.2%) | 157 (44.1%) | 19 (45.2%) | >0.99 |
| Bevacizumab | 84 (21.1%) | 78 (21.9%) | 6 (14.3%) | 0.34 |
| None of the above | 168 (42.2%) | 148 (41.6%) | 20 (47.6%) | 0.56 |
| Time from RT to RN—yrs, median (IQR) | 3.4 (2.5–6.2) (n = 283) | 3.4 (2.5–6.1) (n = 254) | 3.4 (3.0–8.0) (n = 29) | 0.21 |
| TNM stage—n (%) | 0.78 | |||
| I | 5/272 (1.8%) | 5/244 (2.0%) | 0/28 (0.0%) | |
| II | 22/272 (8.1%) | 20/244 (8.2%) | 2/28 (7.1%) | |
| III | 138/272 (50.7%) | 121/244 (49.6%) | 17/28 (60.7%) | |
| IV | 107/272 (39.3%) | 98/244 (40.2%) | 9/28 (32.1%) | |
| RT technique—IMRT, n (%) | 156/261 (59.8%) | 146/234 (62.4%) | 10/27 (37.0%) | 0.02 |
| Tumor RT dose—Gy, mean (SD) | 69.1 (7.6) (n = 266) | 69.2 (6.9) (n = 239) | 68.7 (12.6) (n = 27) | 0.84 |
| Neck RT dose—Gy, mean (SD) | 54.0 (22.8) (n = 278) | 54.2 (22.6) (n = 250) | 52.4 (25.1) (n = 28) | 0.73 |
| Chemotherapy—n (%) | 231/277 (83.4%) | 209/249 (83.9%) | 22/28 (78.6%) | 0.43 |
| Neoadjuvant | 123/277 (44.4%) | 112/249 (45.0%) | 11/28 (39.3%) | 0.71 |
| Concurrent | 190/277 (68.6%) | 175/249 (70.3%) | 15/28 (53.6%) | 0.11 |
| Adjuvant | 18/277 (6.5%) | 15/249 (6.0%) | 3/28 (10.7%) | 0.41 |
| NUTRITIONAL INDICES | Model 0 | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|---|
| Unadjusted-HR (95% CI) | p-Values | Adjusted-HR (95% CI) | p-Values | Adjusted-HR (95% CI) | p-Values | ||
| GNRI | |||||||
| Absent risk | (GNRI > 98) | [Ref] | ·· | [Ref] | ·· | [Ref] | ·· |
| Mild risk | (92 < GNRI ≤ 98) | 1.56 (0.55–4.40) | 0.40 | 1.38 (0.47–4.07) | 0.56 | 1.06 (0.39–6.52) | 0.51 |
| Moderate risk | (82 < GNRI ≤ 92) | 4.45 (1.67–11.85) | 0.003 | 4.19 (1.44–12.21) | 0.009 | 5.62 (1.23–25.80) | 0.03 |
| Severe risk | (GNRI ≤ 82) | 6.33(2.37–16.88) | <0.001 | 4.43 (1.58–12.40) | 0.005 | 5.59 (1.30–23.96) | 0.02 |
| GNRI per 1-point decreased | 1.06 (1.03–1.09) | <0.001 | 1.05 (1.02–1.09) | 0.001 | 1.06 (1.01–1.10) | 0.01 | |
| PNI | |||||||
| Absent risk | (PNI > 38) | [Ref] | ·· | [Ref] | ·· | [Ref] | ·· |
| Moderate risk | (35 < PNI ≤ 38) | 3.80 (1.55–9.30) | 0.004 | 2.92 (1.17–7.30) | 0.02 | 3.80 (0.97–14.97) | 0.06 |
| Severe risk | (PNI ≤ 35) | 3.56 (1.65–7.66) | 0.001 | 2.65 (1.19–5.89) | 0.02 | 2.16 (0.70–6.64) | 0.18 |
| PNI per 1-point decreased | 1.09 (1.04–1.14) | <0.001 | 1.07 (1.03–1.12) | 0.002 | 1.08 (1.01–1.15) | 0.02 | |
| CONUT | |||||||
| Absent risk | (CONUT 0–1) | [Ref] | ·· | [Ref] | ·· | [Ref] | ·· |
| Mild risk | (CONUT 2–4) | 1.33 (0.55–3.24) | 0.53 | 1.40 (0.56–3.52) | 0.47 | 1.79 (0.57–5.62) | 0.32 |
| Moderate risk | (CONUT 5–8) | 4.12 (1.55–10.92) | 0.004 | 3.72 (1.33–10.37) | 0.01 | 3.33 (0.85–13.06) | 0.09 |
| Severe risk | (CONUT 9–12) | 6.11 (1.83–20.36) | 0.003 | 4.67 (1.33–16.37) | 0.02 | 3.25 (0.61–17.43) | 0.17 |
| COUNT per 1-point increased | 1.26 (1.12–1.40) | <0.001 | 1.22 (1.08–1.37) | 0.001 | 1.16 (0.99–1.36) | 0.06 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, D.; Shen, Q.; Li, Y.; Rong, X.; Li, H.; Xu, Y.; He, B.; Zuo, X.; Deng, Z.; Tang, Y. Prognostic Value of Nutritional Assessments on Overall Survival in Head and Neck Cancer Survivors with Radiation-Induced Brain Necrosis. Nutrients 2023, 15, 1973. https://doi.org/10.3390/nu15081973
Pan D, Shen Q, Li Y, Rong X, Li H, Xu Y, He B, Zuo X, Deng Z, Tang Y. Prognostic Value of Nutritional Assessments on Overall Survival in Head and Neck Cancer Survivors with Radiation-Induced Brain Necrosis. Nutrients. 2023; 15(8):1973. https://doi.org/10.3390/nu15081973
Chicago/Turabian StylePan, Dong, Qingyu Shen, Yi Li, Xiaoming Rong, Honghong Li, Yongteng Xu, Baixuan He, Xuzheng Zuo, Zhenhong Deng, and Yamei Tang. 2023. "Prognostic Value of Nutritional Assessments on Overall Survival in Head and Neck Cancer Survivors with Radiation-Induced Brain Necrosis" Nutrients 15, no. 8: 1973. https://doi.org/10.3390/nu15081973
APA StylePan, D., Shen, Q., Li, Y., Rong, X., Li, H., Xu, Y., He, B., Zuo, X., Deng, Z., & Tang, Y. (2023). Prognostic Value of Nutritional Assessments on Overall Survival in Head and Neck Cancer Survivors with Radiation-Induced Brain Necrosis. Nutrients, 15(8), 1973. https://doi.org/10.3390/nu15081973