
Gut Microbiota-Derived Short Chain Fatty Acids Are Associated with Clinical Pregnancy Outcome in Women Undergoing IVF/ICSI-ET: A Retrospective Study
Abstract
:1. Introduction
2. Materials and Methods
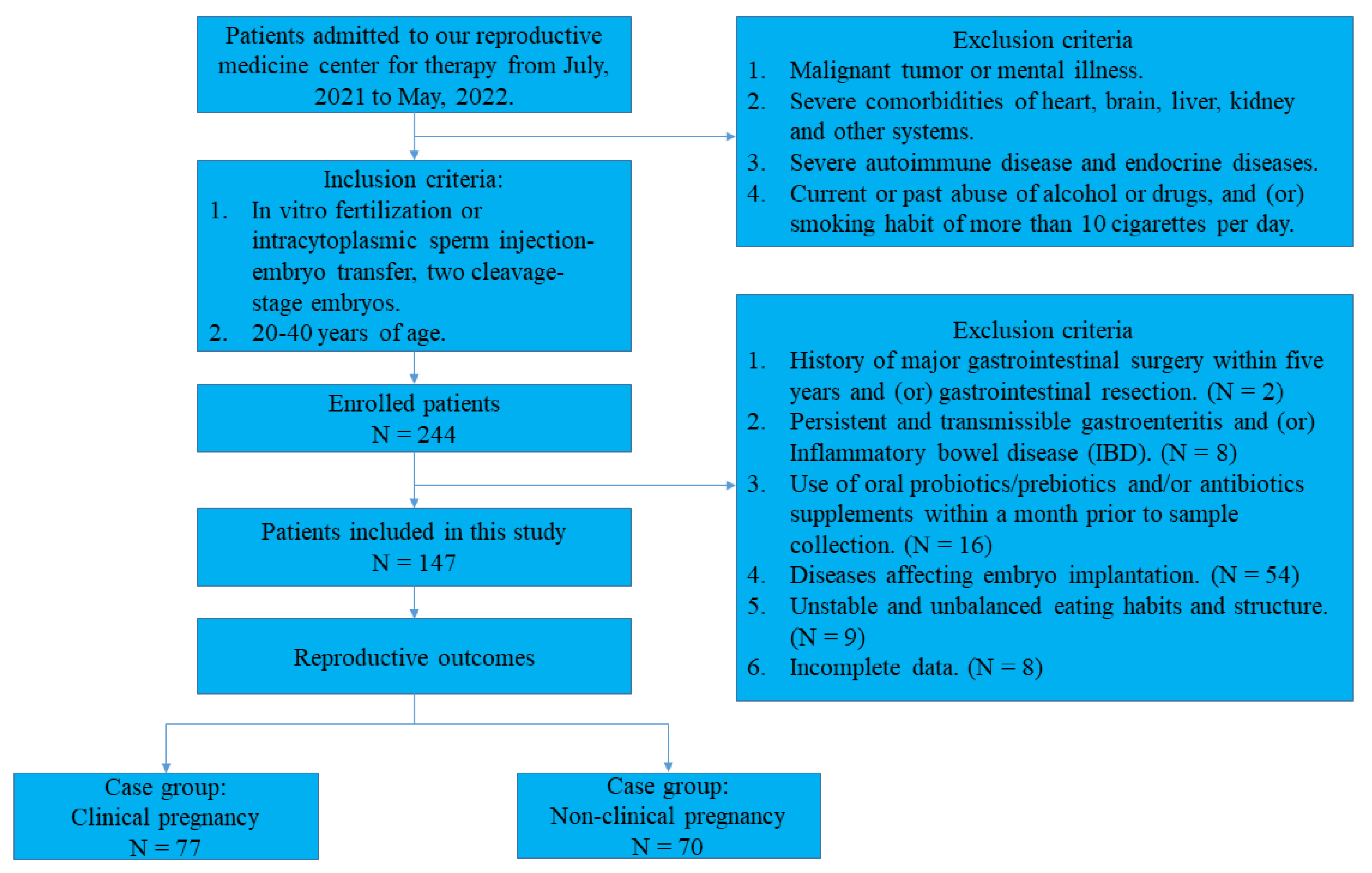
2.1. Study Design and Study Population
2.2. Blood Sample Collection and Measurement
2.3. Fecal Sample Collection and Determination of SCFA Concentrations
2.4. Statistical Analyses
3. Results
3.1. Comparison of Baseline Characteristics between the Two Study Populations
3.2. Fecal Propionate Levels Correlated with FSI, HOMA-IR, and TG
3.3. Fecal Propionate Is a Risk Factor for No Pregnancy
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Diagnostic evaluation of the infertile female: A committee opinion. Fertil. Steril. 2015, 103, e44–e50. [CrossRef] [PubMed]
- Vander Borght, M.; Wyns, C. Fertility and infertility: Definition and epidemiology. Clin. Biochem. 2018, 62, 2–10. [Google Scholar] [CrossRef]
- Wu, B. Information presentation and consumer choice: Evidence from Assisted Reproductive Technology (ART) Success Rate Reports. Health Econ. 2019, 28, 868–883. [Google Scholar] [CrossRef]
- De Geyter, C. Assisted reproductive technology: Impact on society and need for surveillance. Best Pract. Res. Clin. Endocrinol. Metab. 2019, 33, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Wahlström, A.; Sayin, S.I.; Marschall, H.U.; Bäckhed, F. Intestinal Crosstalk between Bile Acids and Microbiota and Its Impact on Host Metabolism. Cell Metab. 2016, 24, 41–50. [Google Scholar] [CrossRef]
- Qi, X.; Yun, C.; Pang, Y.; Qiao, J. The impact of the gut microbiota on the reproductive and metabolic endocrine system. Gut Microbes 2021, 13, 1894070. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; Yun, C.; Sun, L.; Xia, J.; Wu, Q.; Wang, Y.; Wang, L.; Zhang, Y.; Liang, X.; Wang, L.; et al. Gut microbiota-bile acid-interleukin-22 axis orchestrates polycystic ovary syndrome. Nat. Med. 2019, 25, 1225–1233. [Google Scholar] [CrossRef] [PubMed]
- Svensson, A.; Brunkwall, L.; Roth, B.; Orho-Melander, M.; Ohlsson, B. Associations between Endometriosis and Gut Microbiota. Reprod. Sci. 2021, 28, 2367–2377. [Google Scholar] [CrossRef]
- Gomes, A.C.; Hoffmann, C.; Mota, J.F. The human gut microbiota: Metabolism and perspective in obesity. Gut Microbes 2018, 9, 308–325. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Wei, J.; Liu, P.; Zhang, Q.; Tian, Y.; Hou, G.; Meng, L.; Xin, Y.; Jiang, X. Role of the gut microbiota in type 2 diabetes and related diseases. Metabolism 2021, 117, 154712. [Google Scholar] [CrossRef]
- Layden, B.T.; Angueira, A.R.; Brodsky, M.; Durai, V.; Lowe, W.L., Jr. Short chain fatty acids and their receptors: New metabolic targets. Transl. Res. 2013, 161, 131–140. [Google Scholar] [CrossRef]
- Morrison, D.J.; Preston, T. Formation of short chain fatty acids by the gut microbiota and their impact on human metabolism. Gut Microbes 2016, 7, 189–200. [Google Scholar] [CrossRef] [PubMed]
- Ye, Q.; Cai, S.; Wang, S.; Zeng, X.; Ye, C.; Chen, M.; Zeng, X.; Qiao, S. Maternal short and medium chain fatty acids supply during early pregnancy improves embryo survival through enhancing progesterone synthesis in rats. J. Nutr. Biochem. 2019, 69, 98–107. [Google Scholar] [CrossRef]
- Kimura, I.; Miyamoto, J.; Ohue-Kitano, R.; Watanabe, K.; Yamada, T.; Onuki, M.; Aoki, R.; Isobe, Y.; Kashihara, D.; Inoue, D.; et al. Maternal gut microbiota in pregnancy influences offspring metabolic phenotype in mice. Science 2020, 367, eaaw8429. [Google Scholar] [CrossRef] [PubMed]
- Szczuko, M.; Kikut, J.; Maciejewska, D.; Kulpa, D.; Celewicz, Z.; Ziętek, M. The Associations of SCFA with Anthropometric Parameters and Carbohydrate Metabolism in Pregnant Women. Int. J. Mol. Sci. 2020, 21, 9212. [Google Scholar] [CrossRef] [PubMed]
- Macfarlane, G.T.; Macfarlane, S. Bacteria, colonic fermentation, and gastrointestinal health. J. AOAC Int. 2012, 95, 50–60. [Google Scholar] [CrossRef]
- Kahleova, H.; Tura, A.; Hill, M.; Holubkov, R.; Barnard, N.D. A Plant-Based Dietary Intervention Improves Beta-Cell Function and Insulin Resistance in Overweight Adults: A 16-Week Randomized Clinical Trial. Nutrients 2018, 10, 189. [Google Scholar] [CrossRef]
- Meng, H.; Zhu, L.; Kord-Varkaneh, H.; Santos, H.O.; Tinsley, G.M.; Fu, P. Effects of intermittent fasting and energy-restricted diets on lipid profile: A systematic review and meta-analysis. Nutrition 2020, 77, 110801. [Google Scholar] [CrossRef]
- Hannon, B.A.; Thompson, S.V.; Edwards, C.G.; Skinner, S.K.; Niemiro, G.M.; Burd, N.A.; Holscher, H.D.; Teran-Garcia, M.; Khan, N.A. Dietary Fiber Is Independently Related to Blood Triglycerides Among Adults with Overweight and Obesity. Curr. Dev. Nutr. 2019, 3, nzy094. [Google Scholar] [CrossRef]
- Tong, J.N.; Wu, L.L.; Chen, Y.X.; Guan, X.N.; Tian, F.Y.; Zhang, H.F.; Liu, K.; Yin, A.Q.; Wu, X.X.; Prof, J.N. Fasting plasma glucose in the first trimester is related to gestational diabetes mellitus and adverse pregnancy outcomes. Endocrine 2022, 75, 70–81. [Google Scholar] [CrossRef]
- Wu, D.; Zhang, J.; Xiong, Y.; Wang, H.; Lu, D.; Guo, M.; Zhang, J.; Chen, L.; Fan, J.; Huang, H.; et al. Effect of Maternal Glucose and Triglyceride Levels during Early Pregnancy on Pregnancy Outcomes: A Retrospective Cohort Study. Nutrients 2022, 14, 3295. [Google Scholar] [CrossRef]
- Liang, J.W.; Chen, M.X.; Hu, X.A.; Zhou, M.; Zhang, Y.; Wang, L.L. Potential Biomarkers in Early Pregnancy for Predicting Gestational Diabetes Mellitus and Adverse Pregnancy Outcomes. Clin. Lab. 2021, 67. [Google Scholar] [CrossRef] [PubMed]
- Basu, M.; Garg, V. Maternal hyperglycemia and fetal cardiac development: Clinical impact and underlying mechanisms. Birth Defects Res. 2018, 110, 1504–1516. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Wang, J.; Jiang, Y.; Jiang, W. Association between blood lipid level and embryo quality during in vitro fertilization. Medicine 2020, 99, e19665. [Google Scholar] [CrossRef]
- Song, H.; Yu, Z.; Li, P.; Wang, Y.; Shi, Y. HOMA-IR for predicting clinical pregnancy rate during IVF. Gynecol. Endocrinol. 2022, 38, 33–38. [Google Scholar] [CrossRef]
- Giudice, L.C. Endometrium in PCOS: Implantation and predisposition to endocrine CA. Best Pract. Res. Clin. Endocrinol. Metab. 2006, 20, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Seppälä, M.; Taylor, R.N.; Koistinen, H.; Koistinen, R.; Milgrom, E. Glycodelin: A major lipocalin protein of the reproductive axis with diverse actions in cell recognition and differentiation. Endocr. Rev. 2002, 23, 401–430. [Google Scholar] [CrossRef] [PubMed]
- Jakobsdottir, G.; Jädert, C.; Holm, L.; Nyman, M.E. Propionic and butyric acids, formed in the caecum of rats fed highly fermentable dietary fibre, are reflected in portal and aortic serum. Br. J. Nutr. 2013, 110, 1565–1572. [Google Scholar] [CrossRef]
- Schwiertz, A.; Taras, D.; Schäfer, K.; Beijer, S.; Bos, N.A.; Donus, C.; Hardt, P.D. Microbiota and SCFA in lean and overweight healthy subjects. Obesity 2010, 18, 190–195. [Google Scholar] [CrossRef]
- Guo, W.; Zhang, Z.; Li, L.; Liang, X.; Wu, Y.; Wang, X.; Ma, H.; Cheng, J.; Zhang, A.; Tang, P.; et al. Gut microbiota induces DNA methylation via SCFAs predisposing obesity-prone individuals to diabetes. Pharmacol. Res. 2022, 182, 106355. [Google Scholar] [CrossRef]
- Canfora, E.E.; Jocken, J.W.; Blaak, E.E. Short-chain fatty acids in control of body weight and insulin sensitivity. Nat. Rev. Endocrinol. 2015, 11, 577–591. [Google Scholar] [CrossRef]
- Chambers, E.S.; Viardot, A.; Psichas, A.; Morrison, D.J.; Murphy, K.G.; Zac-Varghese, S.E.; MacDougall, K.; Preston, T.; Tedford, C.; Finlayson, G.S.; et al. Effects of targeted delivery of propionate to the human colon on appetite regulation, body weight maintenance and adiposity in overweight adults. Gut 2015, 64, 1744–1754. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Zhang, P.; Shen, L.; Niu, L.; Tan, Y.; Chen, L.; Zhao, Y.; Bai, L.; Hao, X.; Li, X.; et al. Short-Chain Fatty Acids and Their Association with Signalling Pathways in Inflammation, Glucose and Lipid Metabolism. Int. J. Mol. Sci. 2020, 21, 6356. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.; Chassaing, B.; Zhang, L.; San Yeoh, B.; Xiao, X.; Kumar, M.; Baker, M.T.; Cai, J.; Walker, R.; Borkowski, K.; et al. Microbiota-Dependent Hepatic Lipogenesis Mediated by Stearoyl CoA Desaturase 1 (SCD1) Promotes Metabolic Syndrome in TLR5-Deficient Mice. Cell Metab. 2015, 22, 983–996. [Google Scholar] [CrossRef] [PubMed]
- Tirosh, A.; Calay, E.S.; Tuncman, G.; Claiborn, K.C.; Inouye, K.E.; Eguchi, K.; Alcala, M.; Rathaus, M.; Hollander, K.S.; Ron, I.; et al. The short-chain fatty acid propionate increases glucagon and FABP4 production, impairing insulin action in mice and humans. Sci. Transl. Med. 2019, 11, 6356. [Google Scholar] [CrossRef] [PubMed]
- Komiya, S.; Naito, Y.; Okada, H.; Matsuo, Y.; Hirota, K.; Takagi, T.; Mizushima, K.; Inoue, R.; Abe, A.; Morimoto, Y. Characterizing the gut microbiota in females with infertility and preliminary results of a water-soluble dietary fiber intervention study. J. Clin. Biochem. Nutr. 2020, 67, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Patel, N.; Pal, S.; Nathani, N.; Pandit, R.; Patel, M.; Patel, N.; Joshi, C.; Parekh, B. Distinct gut and vaginal microbiota profile in women with recurrent implantation failure and unexplained infertility. BMC Womens Health 2022, 22, 113. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No Pregnancy (n = 70) | Clinical Pregnancy (n = 77) | p Value | |
|---|---|---|---|
| Age (years) | 33.57 ± 3.96 | 33.90 ± 2.97 | 0.573 a |
| BMI (kg/m2) | 24.34 ± 3.34 | 23.38 ± 2.75 | 0.059 a |
| Infertility duration (years) | 3.00 (2.00–5.00) | 3.00 (2.00–6.00) | 0.905 b |
| Education, N (%) | 0.104 c | ||
| Middle school and below | 14 (20.00) | 7 (9.09) | |
| High school | 3 (4.29) | 10 (12.99) | |
| College | 46 (65.71) | 53 (68.83) | |
| Master’s and above | 7 (10.00) | 7 (9.09) | |
| Dietary habits (n, %) | 0.316 c | ||
| Vegetarian diet | 2 (2.86) | 7 (9.10) | |
| Meat-based diet | 5 (7.14) | 6 (12.99) | |
| Meat and vegetarian diet | 63 (90.00) | 64 (77.91) | |
| Ovulation regimen (n, %) | 0.152 c | ||
| Long | 0 (0) | 1 (1.30) | |
| Super-long | 9 (12.86) | 3 (3.90) | |
| Antagonist | 49 (70.00) | 60 (77.92) | |
| PPOS | 12 (17.14) | 13 (16.88) | |
| Fertilization (n, %) | 0.596 c | ||
| IVF | 31 (44.29) | 31 (40.26) | |
| ICSI | 35 (50.00) | 38 (49.35) | |
| IVF + ICSI | 4 (5.71) | 8 (10.39) | |
| Previous pregnancies (n, %) | 37 (52.86) | 31 (40.26) | 0.126 d |
| Endometrial thickness (mm) | 9.38 ± 2.20 | 9.89 ± 2.13 | 0.150 a |
| Number of oocytes retrieved | 7.00 (5.00–9.00) | 8.00 (6.00–10.00) | 0.074 b |
| Number of 2PN oocytes | 5.00 (3.00–7.00) | 6.00 (4.00–8.00) | 0.033 b |
| Number of MII oocytes | 5.00 (3.00–7.00) | 6.00 (4.00–8.00) | 0.095 b |
| Number of suitable embryos | 4.00 (2.00–5.00) | 4.00 (2.00–7.00) | 0.093 b |
| No Pregnancy (n = 70) | Clinical Pregnancy (n = 77) | p Value | |
|---|---|---|---|
| E2 (pg/mL) | 31.65 (24.07–44.37) | 34.62 (26.04–52.97) | 0.165 a |
| P (ng/mL) | 0.46 (0.30–0.71) | 0.54 (0.36–0.66) | 0.563 a |
| PRL (ng/mL) | 13.83 (10.23–15.62) | 12.01 (9.43–16.79) | 0.337 a |
| SHBG (nmol/L) | 30.65 (20.18–56.50) | 38.80 (25.95–49.75) | 0.416 a |
| TT (ng/mL) | 0.46 (0.35–0.54) | 0.44 (0.35–0.52) | 0.695 a |
| FSH (mIU/mL) | 7.39 (6.17–8.56) | 7.30 (6.03–8.21) | 0.646 a |
| LH (mIU/mL) | 4.17 (2.81–5.83) | 3.67 (2.43–6.26) | 0.786 a |
| AMH (ng/mL) | 3.25 (1.63–5.04) | 3.92 (2.40–5.99) | 0.054 a |
| FSI (mIU/L) | 11.65 (8.50–16.40) | 9.35 (7.54–11.61) | 0.001 a |
| FPG (mmol/L) | 5.39 ± 0.57 | 5.35 ± 0.48 | 0.665 b |
| HOMA-IR | 2.76 (1.92–4.00) | 2.22 (1.79–2.75) | 0.002 a |
| CHOL (mmol/L) | 4.77 (4.31–5.15) | 4.66 (4.28–5.23) | 0.958 a |
| TG (mmol/L) | 1.28 (0.67–2.11) | 0.97 (0.66–1.35) | 0.016 a |
| HDL-C (mmol/L) | 1.38 ± 0.29 | 1.41 ± 0.30 | 0.638 b |
| LDL-C (mmol/L) | 2.93 (2.46–3.30) | 2.91 (2.37–3.45) | 0.998 a |
| TBIL (μmol/L) | 9.90 (8.25–12.93) | 11.10 (8.90–13.05) | 0.167 a |
| DBIL (μmol/L) | 2.70 (1.98–3.30) | 2.70 (2.10–3.50) | 0.441 a |
| IDBIL (μmol/L) | 7.40 (5.88–9.73) | 8.40 (6.60–9.65) | 0.192 a |
| TBA (μmol/L) | 2.11 (1.28–3.07) | 1.78 (1.08–3.47) | 0.687 a |
| Univariate Regression | Multivariate Regression | |||||
|---|---|---|---|---|---|---|
| OR | 95%CI | p Value | OR * | 95%CI | p Value | |
| Propionate (μmol/g wet feces) | 1.108 | 1.054–1.165 | <0.001 | 1.103 | 1.045–1.164 | <0.001 a |
| FSI (mIU/L) | 1.147 | 1.059–1.244 | 0.001 | 1.311 | 0.891–1.929 | 0.170 b |
| HOMA-IR | 1.688 | 1.236–2.307 | 0.001 | 0.528 | 0.118–2.372 | 0.405 c |
| TG (mmol/L) | 2.291 | 1.378–3.809 | 0.001 | 1.738 | 0.971–3.112 | 0.063 d |
| AUC | SE | Cut off | 95% CI | Sensitivity% | Specificity% | p Value | |
|---|---|---|---|---|---|---|---|
| Propionate | 0.702 | 0.043 | 14.97 | 0.617–0.786 | 57.1 | 79.2 | <0.001 |
| FSI | 0.655 | 0.046 | 13.14 | 0.565–0.745 | 42.9 | 87.0 | 0.001 |
| HOMA-IR | 0.648 | 0.047 | 3.29 | 0.556–0.739 | 42.9 | 89.6 | 0.002 |
| TG | 0.615 | 0.048 | 3.29 | 0.521–0.709 | 42.9 | 89.6 | 0.016 |
| Propionate + FSI | 0.743 | 0.041 | 0.36 | 0.663–0.822 | 82.9 | 58.4 | <0.001 |
| Propionate + HOMA-IR | 0.735 | 0.041 | 0.36 | 0.655–0.816 | 82.9 | 57.1 | <0.001 |
| Propionate + TG | 0.722 | 0.043 | 0.49 | 0.638–0.805 | 61.4 | 79.2 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yao, X.; Dong, S.; Guan, W.; Fu, L.; Li, G.; Wang, Z.; Jiao, J.; Wang, X. Gut Microbiota-Derived Short Chain Fatty Acids Are Associated with Clinical Pregnancy Outcome in Women Undergoing IVF/ICSI-ET: A Retrospective Study. Nutrients 2023, 15, 2143. https://doi.org/10.3390/nu15092143
Yao X, Dong S, Guan W, Fu L, Li G, Wang Z, Jiao J, Wang X. Gut Microbiota-Derived Short Chain Fatty Acids Are Associated with Clinical Pregnancy Outcome in Women Undergoing IVF/ICSI-ET: A Retrospective Study. Nutrients. 2023; 15(9):2143. https://doi.org/10.3390/nu15092143
Chicago/Turabian StyleYao, Xinrui, Sitong Dong, Wenzheng Guan, Lingjie Fu, Gaoyu Li, Zhen Wang, Jiao Jiao, and Xiuxia Wang. 2023. "Gut Microbiota-Derived Short Chain Fatty Acids Are Associated with Clinical Pregnancy Outcome in Women Undergoing IVF/ICSI-ET: A Retrospective Study" Nutrients 15, no. 9: 2143. https://doi.org/10.3390/nu15092143