
A Randomized, Double-Blind, Placebo-Controlled Clinical Trial on the Effect of a Dietary Supplement Containing Dry Artichoke and Bergamot Extracts on Metabolic and Vascular Risk Factors in Individuals with Suboptimal Cholesterol Levels

 ,
,  , ,
, ,  and
and 
Abstract

1. Introduction
2. Materials and Methods
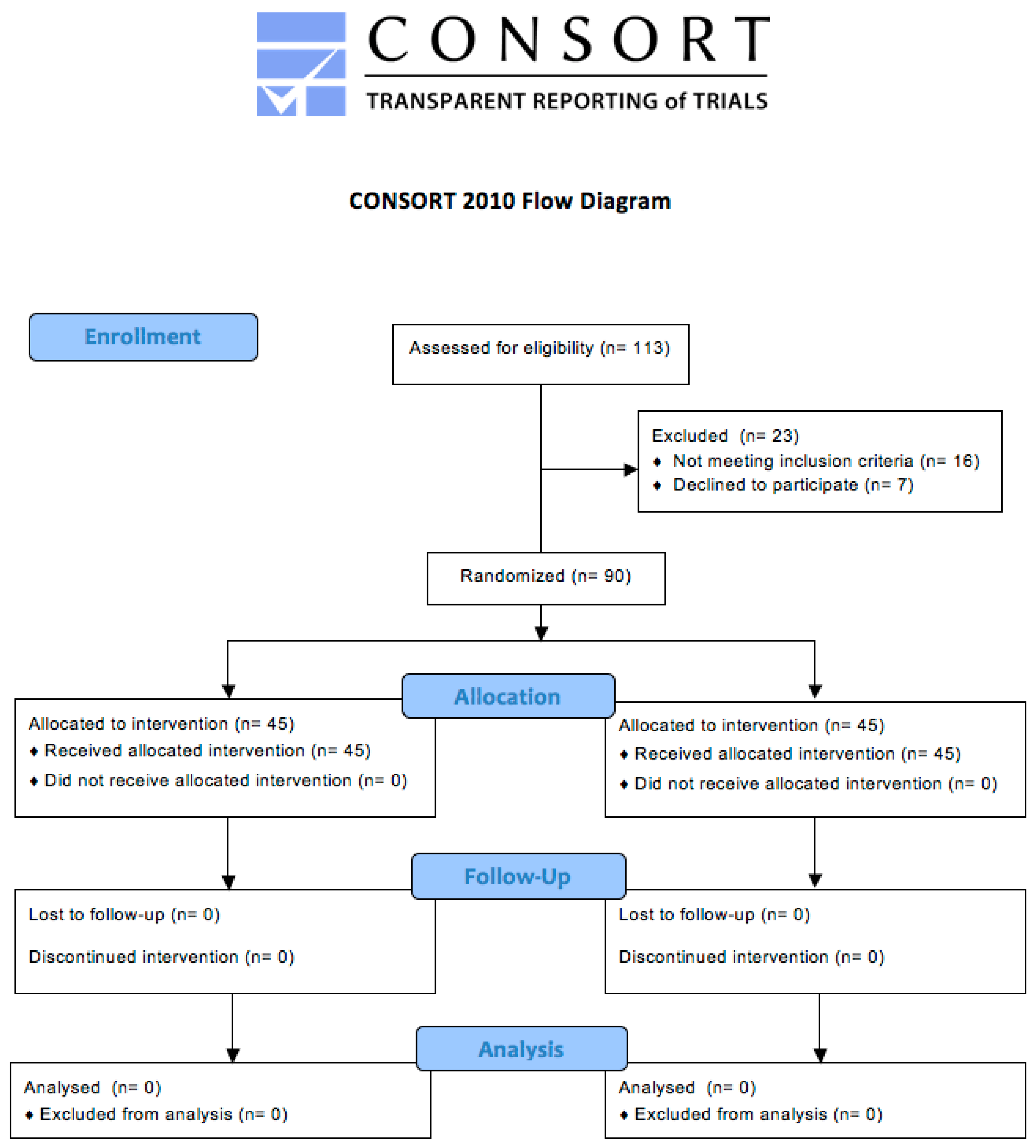
2.1. Trial Design and Participants
2.2. Treatment
2.3. Assessments
2.3.1. Clinical Data
2.3.2. Laboratory Analyses
2.3.3. Blood Pressure Measurements
2.3.4. Endothelial Reactivity
2.3.5. Assessment of Safety and Tolerability
2.4. Statistical Analysis
3. Results
3.1. Efficacy Analysis
3.2. Safety Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Mean Cholesterol. Available online: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/2384 (accessed on 21 January 2024).
- Ray, K.K.; Molemans, B.; Schoonen, W.M.; Giovas, P.; Bray, S.; Kiru, G.; Murphy, J.; Banach, M.; De Servi, S.; Gaita, D.; et al. EU-Wide Cross-Sectional Observational Study of Lipid-Modifying Therapy Use in Secondary and Primary Care: The DA VINCI study. Eur. J. Prev. Cardiol. 2021, 11, 1279–1289. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Repositioning of the global epicentre of non-optimal cholesterol. Nature 2020, 582, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Visioli, F.; Poli, A. Dietary advice to cardiovascular patients. A brief update for physicians. Monaldi Arch. Chest Dis. 2019, 89, 1071. [Google Scholar] [CrossRef] [PubMed]
- Poli, A.; Catapano, A.L.; Corsini, A.; Manzato, E.; Werba, J.P.; Catena, G.; Cetin, I.; Cicero, A.F.G.; Cignarella, A.; Colivicchi, F.; et al. LDL-cholesterol control in the primary prevention of cardiovascular diseases: An expert opinion for clinicians and health professionals. Nutr. Metab. Cardiovasc. Dis. 2023, 33, 245–257. [Google Scholar] [CrossRef] [PubMed]
- Belfort-DeAguiar, R.; Lomonaco, R.; Cusi, K. Approach to the Patient With Nonalcoholic Fatty Liver Disease. J. Clin. Endocrinol. Metab. 2023, 108, 483–495. [Google Scholar] [CrossRef]
- Lee, E.C.Z.; Anand, V.V.; Razavi, A.C.; Alebna, P.L.; Muthiah, M.D.; Siddiqui, M.S.; Chew, N.W.S.; Mehta, A. The Global Epidemic of Metabolic Fatty Liver Disease. Curr. Cardiol. Rep. 2024, 26, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Zaini, N.S.; Karim, R.; Abdull Razis, A.F.; Zawawi, N. Utilizing Nutritional and Polyphenolic Compounds in Underutilized Plant Seeds for Health Application. Molecules 2022, 27, 6813. [Google Scholar] [CrossRef] [PubMed]
- Tangney, C.C.; Rasmussen, H.E. Polyphenols, inflammation, and cardiovascular disease. Curr. Atheroscler. Rep. 2013, 15, 324. [Google Scholar] [CrossRef] [PubMed]
- Martín, M.Á.; Ramos, S. Impact of Dietary Flavanols on Microbiota, Immunity and Inflammation in Metabolic Diseases. Nutrients 2021, 13, 850. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Pandey, A.K. Chemistry and biological activities of flavonoids: An overview. Sci. World J. 2013, 2013, 162750. [Google Scholar] [CrossRef] [PubMed]
- Di Lorenzo, C.; Colombo, F.; Biella, S.; Stockley, C.; Restani, P. Polyphenols and Human Health: The Role of Bioavailability. Nutrients 2021, 13, 273. [Google Scholar] [CrossRef] [PubMed]
- Mazidi, M.; Katsiki, N.; Banach, M. A Greater Flavonoid Intake Is Associated with Lower Total and Cause-Specific Mortality: A Meta-Analysis of Cohort Studies. Nutrients 2020, 12, 2350. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Giacosa, A.; Morazzoni, P.; Guido, D.; Grassi, M.; Morandi, G.; Bologna, C.; Riva, A.; Allegrini, P.; Perna, S. MediterrAsian Diet Products That Could Raise HDL-Cholesterol: A Systematic Review. BioMed Res. Int. 2016, 2016, 2025687. [Google Scholar] [CrossRef] [PubMed]
- Zayed, A.; Serag, A.; Farag, M.A. Cynara cardunculus L.: Outgoing and potential trends of phytochemical, industrial, nutritive and medicinal merits. J. Funct. Foods 2020, 69, 103937. [Google Scholar] [CrossRef]
- Authors/Task Force Members; ESC Committee for Practice Guidelines (CPG); ESC National Cardiac Societies. 2019 ESC/EAS guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Atherosclerosis 2019, 290, 140–205. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.G.; Caliceti, C.; Fogacci, F.; Giovannini, M.; Calabria, D.; Colletti, A.; Veronesi, M.; Roda, A.; Borghi, C. Effect of apple polyphenols on vascular oxidative stress and endothelium function: A translational study. Mol. Nutr. Food Res. 2017, 61, 1700373. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular fltration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Bedogni, G.; Kahn, H.S.; Bellentani, S.; Tiribelli, C. A simple index of lipid overaccumulation is a good marker of liver steatosis. BMC Gastroenterol. 2010, 10, 98. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J. Hypertens. 2018, 36, 1953–2041. [Google Scholar] [PubMed]
- Thijssen, D.H.J.; Bruno, R.M.; van Mil, A.C.C.M.; Holder, S.M.; Faita, F.; Greyling, A.; Zock, P.L.; Taddei, S.; Deanfield, J.E.; Luscher, T.; et al. Expert consensus and evidence-based recommendations for the assessment of flow-mediated dilation in humans. Eur. Heart J. 2019, 40, 2534–2547. [Google Scholar] [CrossRef]
- Corretti, M.C.; Anderson, T.J.; Benjamin, E.J.; Celermajer, D.; Charbonneau, F.; Creager, M.A.; Deanfield, J.; Drexler, H.; Gerhard-Herman, M.; Herrington, D.; et al. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: A report of the International Brachial Artery Reactivity Task Force. J. Am. Coll. Cardiol. 2002, 39, 257–265. [Google Scholar] [CrossRef] [PubMed]
- McGreevy, C.; Barry, M.; Bennett, K.; Williams, D. Repeatability of the measurement of aortic pulse wave velocity (aPWV) in the clinical assessment of arterial stiffness in community-dwelling older patients using the Vicorder(®) device. Scand. J. Clin. Lab. Investig. 2013, 73, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Day, L.M.; Maki-Petaja, K.M.; Wilkinson, I.B.; McEniery, C.M. Assessment of brachial artery reactivity using the endocheck: Repeatability, reproducibility and preliminary comparison with ultrasound. Artery Res. 2013, 7, 119–120. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Fogacci, F.; Veronesi, M.; Strocchi, E.; Grandi, E.; Rizzoli, E.; Poli, A.; Marangoni, F.; Borghi, C. A randomized Placebo-Controlled Clinical Trial to Evaluate the Medium-Term Effects of Oat Fibers on Human Health: The Beta-Glucan Effects on Lipid Profile, Glycemia and inTestinal Health (BELT) Study. Nutrients 2020, 12, 686. [Google Scholar] [CrossRef] [PubMed]
- Visioli, F.; Poli, A. Prevention and Treatment of Atherosclerosis: The Use of Nutraceuticals and Functional Foods. Handb. Exp. Pharmacol. 2022, 270, 271–285. [Google Scholar] [CrossRef] [PubMed]
- Feldman, F.; Koudoufio, M.; Desjardins, Y.; Spahis, S.; Delvin, E.; Levy, E. Efficacy of Polyphenols in the Management of Dyslipidemia: A Focus on Clinical Studies. Nutrients 2021, 13, 672. [Google Scholar] [CrossRef] [PubMed]
- Fogacci, F.; Giovannini, M.; Imbalzano, E.; Grandi, E.; Rizzoli, E.; D’Addato, S.; Cicero, A.F.G. Metabolic and vascular effect of a new standardized bergamot phytocomplex: A three-arm, placebocontrolled, double-blind clinical trial. Arch. Med. Sci. 2023, 19, 1228–1235. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.G.; Fogacci, F.; Stoian, A.P.; Vrablik, M.; Al Rasadi, K.; Banach, M.; Toth, P.P.; Rizzo, M. Nutraceuticals in the Management of Dyslipidemia: Which, When, and for Whom? Could Nutraceuticals Help Low-Risk Individuals with Non-optimal Lipid Levels? Curr. Atheroscler. Rep. 2021, 23, 57. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Colletti, A.; Bajraktari, G.; Descamps, O.; Djuric, D.M.; Ezhov, M.; Fras, Z.; Katsiki, N.; Langlois, M.; Latkovskis, G.; et al. Lipid lowering nutraceuticals in clinical practice: Position paper from an International Lipid Expert Panel. Arch. Med. Sci. 2017, 13, 965–1005. [Google Scholar] [CrossRef] [PubMed]
- Arnaboldi, L.; Corsini, A.; Bellosta, S. Artichoke and bergamot extracts: A new opportunity for the management of dyslipidemia and related risk factors. Minerva Medica 2022, 113, 141–157. [Google Scholar] [CrossRef]
- Gebhardt, R. Inhibition of cholesterol biosynthesis in primary cultured rat hepatocytes by artichoke (Cynara scolymus L.) extracts. J. Pharmacol. Exp. Ther. 1998, 286, 1122–1128. [Google Scholar] [PubMed]
- Cicero, A.F.G.; Fogacci, F.; Tocci, G.; D’Addato, S.; Grandi, E.; Banach, M.; Borghi, C. Three arms, double-blind, non-inferiority, randomized clinical study testing the lipid-lowering effect of a novel dietary supplement containing red yeast rice and artichoke extracts compared to Armolipid Plus® and placebo. Arch. Med. Sci. 2023, 19, 1169–1179. [Google Scholar] [CrossRef]
- Ballistreri, G.; Amenta, M.; Fabroni, S.; Consoli, V.; Grosso, S.; Vanella, L.; Sorrenti, V.; Rapisarda, P. Evaluation of lipid and cholesterol-lowering effect of bioflavonoids from bergamot extract. Nat. Prod. Res. 2021, 35, 5378–5383. [Google Scholar] [CrossRef]
- Giglio, R.V.; Patti, A.M.; Nikolic, D.; Li Volti, G.; Al-Rasadi, K.; Katsiki, N.; Mikhailidis, D.P.; Montalto, G.; Ivanova, E.; Orekhov, A.N.; et al. The effect of bergamot on dyslipidemia. Phytomedicine 2016, 23, 1175–1181. [Google Scholar] [CrossRef] [PubMed]
- Sahebkar, A.; Pirro, M.; Banach, M.; Mikhailidis, D.P.; Atkin, S.L.; Cicero, A.F.G. Lipid-lowering activity of artichoke extracts: A systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2018, 58, 2549–2556. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi-Dehsahraei, H.; Esmaeili Gouvarchin Ghaleh, H.; Mirnejad, R.; Parastouei, K. The effect of bergamot (KoksalGarry) supplementation on lipid profiles: A systematic review and meta-analysis of randomized controlled trials. Phytother. Res. 2022, 36, 4409–4424. [Google Scholar] [CrossRef] [PubMed]
- Osadnik, T.; Goławski, M.; Lewandowski, P.; Morze, J.; Osadnik, K.; Pawlas, N.; Lejawa, M.; Jakubiak, G.K.; Mazur, A.; Schwingschackl, L.; et al. A network meta-analysis on the comparative effect of nutraceuticals on lipid profile in adults. Pharmacol. Res. 2022, 183, 106402. [Google Scholar] [CrossRef] [PubMed]
- Fogacci, F.; Rizzoli, E.; Giovannini, M.; Bove, M.; D’Addato, S.; Borghi, C.; Cicero, A.F.G. Effect of Dietary Supplementation with Eufortyn® Colesterolo Plus on Serum Lipids, Endothelial Reactivity, Indexes of Non-Alcoholic Fatty Liver Disease and Systemic Inflammation in Healthy Subjects with Polygenic Hypercholesterolemia: The ANEMONE Study. Nutrients 2022, 14, 2099. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Fogacci, F.; Bove, M.; Giovannini, M.; Borghi, C. Three-arm, placebo-controlled, randomized clinical trial evaluating the metabolic effect of a combined nutraceutical containing a bergamot standardized flavonoid extract in dyslipidemic overweight subjects. Phytother. Res. 2019, 33, 2094–2101. [Google Scholar] [CrossRef]
- Coppola, A.; Gazzaruso, C.; Montalcini, T.; Pujia, A.; Paone, S.; Mollace, V.; Mazza, E. A nutraceutical with Citrus bergamia and Cynara cardunculus improves endothelial function in adults with non-alcoholic fatty liver disease. Nutrition 2024, 118, 112294. [Google Scholar] [CrossRef] [PubMed]
- Baigent, C.; Keech, A.; Kearney, P.M.; Blackwell, L.; Buck, G.; Pollicino, C.; Kirby, A.; Sourjina, T.; Peto, R.; Collins, R.; et al. Cholesterol Treatment Trialists’ (CTT) Collaborators. Efficacy and safety of cholesterol-lowering treatment: Prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005, 366, 1267–1278. [Google Scholar] [CrossRef] [PubMed]
- Silverman, M.G.; Ference, B.A.; Im, K.; Wiviott, S.D.; Giugliano, R.P.; Grundy, S.M.; Braunwald, E.; Sabatine, M.S. Association Between Lowering LDL-C and Cardiovascular Risk Reduction Among Different Therapeutic Interventions: A Systematic Review and Meta-analysis. JAMA 2016, 316, 1289–1297. [Google Scholar] [CrossRef] [PubMed]
- Matsuzawa, Y.; Kwon, T.G.; Lennon, R.J.; Lerman, L.O.; Lerman, A. Prognostic Value of Flow-Mediated Vasodilation in Brachial Artery and Fingertip Artery for Cardiovascular Events: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2015, 4, e002270. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Guan, S.; Xu, H.; Zhang, N.; Huang, M.; Liu, Z. Inflammation biomarkers are associated with the incidence of cardiovascular disease: A meta-analysis. Front. Cardiovasc. Med. 2023, 10, 1175174. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.; Galimberti, F.; Olmastroni, E.; Luscher, T.F.; Carugo, S.; Catapano, A.L.; Casula, M.; META-LIPID Group. Effect of lipid-lowering therapies on C-reactive protein levels: A comprehensive meta-analysis of randomized controlled trials. Cardiovasc. Res. 2024, 120, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Xia, J.; Yu, J.; Xu, H.; Zhou, Y.; Li, H.; Yin, S.; Xu, D.; Wang, Y.; Xia, H.; Liao, W.; et al. Comparative effects of vitamin and mineral supplements in the management of type 2 diabetes in primary care: A systematic review and network meta-analysis of randomized controlled trials. Pharmacol. Res. 2023, 188, 106647. [Google Scholar] [CrossRef]
- Ference, B.A.; Yoo, W.; Alesh, I.; Mahajan, N.; Mirowska, K.K.; Mewada, A.; Kahn, J.; Afonso, L.; Williams, K.A., Sr.; Flack, J.M. Effect of long-term exposure to lower low-density lipoprotein cholesterol beginning early in life on the risk of coronary heart disease: A Mendelian randomization analysis. J. Am. Coll. Cardiol. 2012, 60, 2631–2639. [Google Scholar] [CrossRef]
- Domínguez-Fernández, M.; Ludwig, I.A.; De Peña, M.P.; Cid, C. Bioaccessibility of Tudela artichoke (Cynara scolymus cv. Blanca de Tudela) (poly)phenols: The effects of heat treatment, simulated gastrointestinal digestion and human colonic microbiota. Food Funct. 2021, 12, 1996–2011. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Ingredients | Quantity per Tablet |
|---|---|
| Artichoke dry extract (Cynara scolymus L.) | 700 mg |
| equivalent to caffeoylquinic acids | 52.5 mg |
| chlorogenic acid | 35 mg |
| flavonoids | 11.9 mg |
| Bergamot dry extract (Citrus bergamia Risso & Poit) | 375 mg |
| equivalent to flavonoids | 150 mg |
| Astaxanthin-rich oleoresin from Haematococcus pluvialis algae | 20 mg |
| equivalent to astaxanthin | 0.5 mg |
| Chromium picolinate | 320 µg |
| equivalent to chromium | 40 µg |
| Folic acid | 200 µg |
| Parameters | Dietary Supplement Containing Artichoke and Bergamot Dry Extracts (N. 45) | Placebo (N. 45) | ||
|---|---|---|---|---|
| Baseline | 12-Week Follow-Up | Baseline | 12-Week Follow-Up | |
| Total energy (Kcal/day) | 1499 ± 119 | 1501 ± 125 | 1494 ± 111 | 1486 ± 129 |
| Carbohydrates (% of total energy) | 54.2 ± 2.7 | 52.2 ± 2.6 | 53.5 ± 3.1 | 53.4 ± 2.8 |
| Proteins (% of total energy) | 18.1 ± 1.5 | 17.4 ± 1.9 | 18.3 ± 1.9 | 18.5 ± 1.7 |
| Animal protein (% of total energy) | 10.5 ± 0.9 | 9.7 ± 0.8 | 10.6 ± 1.1 | 10.9 ± 0.7 |
| Vegetal protein (% of total energy) | 6.9 ± 0.7 | 7.3 ± 0.9 | 6.6 ± 0.6 | 6.8 ± 0.8 |
| Total fats (% of total energy) | 28.7 ± 2.4 | 28.5 ± 2.5 | 28.2 ± 1.6 | 29.4 ± 2.2 |
| Saturated fatty acids (% of total energy) | 8.9 ± 0.8 | 9.2 ± 0.7 | 9.3 ± 0.7 | 8.8 ± 0.9 |
| MUFA (% of total energy) | 12.6 ± 0.9 | 12.2 ± 1.0 | 12.8 ± 1.1 | 12.3 ± 1.2 |
| PUFA (% of total energy) | 6.7 ± 0.6 | 6.3 ± 0.4 | 6.6 ± 0.4 | 6.8 ± 0.5 |
| Total dietary fibers (g/day) | 17.9 ± 1.5 | 18.1 ± 1.8 | 18.1 ± 1.5 | 17.7 ± 1.4 |
| Cholesterol (mg/day) | 193.2 ± 14.3 | 188.2 ± 13.3 | 193.9 ± 13.5 | 195.8 ± 13.7 |
| Parameters | Dietary Supplement Containing Artichoke and Bergamot Dry Extracts (N. 45) | Placebo (N. 45) | ||||
|---|---|---|---|---|---|---|
| Baseline | 6-Week Follow-Up | 12-Week Follow-Up | Baseline | 6-Week Follow-Up | 12-Week Follow-Up | |
| Age (years) | 46.2 ± 3.7 | - | - | 47.3 ± 3.2 | - | - |
| BMI (Kg/m2) | 26.9 ± 1.9 | 26.6 ± 1.5 | 26.4 ± 1.4 | 26.8 ± 1.7 | 26.8 ± 1.6 | 26.6 ± 1.7 |
| SBP (mmHg) | 126 ± 9 | 126 ± 7 | 125 ± 6 | 128 ± 8 | 127 ± 9 | 129 ± 9 |
| DBP (mmHg) | 84 ± 7 | 85 ± 5 | 84 ± 4 | 85 ± 6 | 83 ± 6 | 83 ± 5 |
| Total Cholesterol (mg/dL) | 245 ± 13 | 207 ± 10 *° | 205 ± 9 *° | 238 ± 12 | 229 ± 10 | 228 ± 12 |
| LDL-C (mg/dL) | 157 ± 12 | 136 ± 7 *° | 132 ± 6 *° | 161 ± 9 | 154 ± 10 | 154 ± 8 |
| HDL-C (mg/dL) | 44 ± 3 | 45 ± 4 | 47 ± 3 * | 45 ± 2 | 45 ± 3 | 45 ± 3 |
| Non-HDL-C (mg/dL) | 211 ± 13 | 162 ± 9 *° | 158 ± 8 *° | 203 ± 11 | 184 ± 11 * | 183 ± 10 * |
| Triglycerides (mg/dL) | 151 ± 13 | 132 ± 9 * | 129 ± 7 *° | 159 ± 12 | 142 ± 11 * | 140 ± 9 * |
| Apolipoprotein B100 (mg/dL) | 127 ± 9 | 115 ± 5 * | 117 ± 7 * | 124 ± 8 | 121 ± 7 | 123 ± 8 |
| Apolipoprotein AI (mg/dL) | 142 ± 12 | 148 ± 8 * | 149 ± 9 * | 145 ± 11 | 147 ± 10 | 146 ± 9 |
| Fasting glucose (mg/dL) | 87 ± 6 | 84 ± 6 | 82 ± 5 * | 90 ± 9 | 88 ± 9 | 87 ± 10 |
| AST (U/L) | 18 ± 6 | 17 ± 3 | 16 ± 3 | 21 ± 6 | 22 ± 5 | 21 ± 4 |
| ALT (U/L) | 21 ± 5 | 19 ± 5 | 17 ± 6 * | 23 ± 7 | 23 ± 4 | 22 ± 5 |
| gGT (U/L) | 25 ± 7 | 22 ± 6 | 21 ± 4 * | 28 ± 9 | 26 ± 6 | 25 ± 6 |
| Lipid Accumulation Product | 63 ± 12 | 60 ± 9 | 58 ± 9 * | 64 ± 14 | 63 ± 11 | 63 ± 9 |
| Hepatic Steatosis Index | 37 ± 5 | 36 ± 4 | 35 ± 4 * | 38 ± 5 | 37 ± 4 | 37 ± 3 |
| Fatty Liver Index | 55 ± 9 | 52 ± 9 | 51 ± 7 *° | 57 ± 11 | 56 ± 10 | 56 ± 9 |
| CPK (U/L) | 129 ± 37 | 118 ± 27 | 122 ± 22 | 134 ± 42 | 142 ± 28 | 139 ± 31 |
| eGFR (mL/min) | 83.9 ± 3.3 | 84.2 ± 3.7 | 84.5 ± 2.8 | 84.3 ± 3.4 | 85.3 ± 3.6 | 83.9 ± 3.9 |
| hs-CRP (mg/L) | 3.01 ± 0.22 | 2.71 ± 0.16 *° | 2.68 ± 0.17 *° | 2.90 ± 0.25 | 2.82 ± 0.32 | 2.87 ± 0.29 |
| Pulse Volume (%) | 63.9 ± 6.3 | 64.8 ± 4.8 | 69.2 ± 3.7 *° | 65.4 ± 6.1 | 66.5 ± 5.1 | 64.1 ± 4.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fogacci, F.; Giovannini, M.; Di Micoli, A.; Fiorini, G.; Grandi, E.; Borghi, C.; Cicero, A.F.G. A Randomized, Double-Blind, Placebo-Controlled Clinical Trial on the Effect of a Dietary Supplement Containing Dry Artichoke and Bergamot Extracts on Metabolic and Vascular Risk Factors in Individuals with Suboptimal Cholesterol Levels. Nutrients 2024, 16, 1587. https://doi.org/10.3390/nu16111587
Fogacci F, Giovannini M, Di Micoli A, Fiorini G, Grandi E, Borghi C, Cicero AFG. A Randomized, Double-Blind, Placebo-Controlled Clinical Trial on the Effect of a Dietary Supplement Containing Dry Artichoke and Bergamot Extracts on Metabolic and Vascular Risk Factors in Individuals with Suboptimal Cholesterol Levels. Nutrients. 2024; 16(11):1587. https://doi.org/10.3390/nu16111587
Chicago/Turabian StyleFogacci, Federica, Marina Giovannini, Antonio Di Micoli, Giulia Fiorini, Elisa Grandi, Claudio Borghi, and Arrigo F. G. Cicero. 2024. "A Randomized, Double-Blind, Placebo-Controlled Clinical Trial on the Effect of a Dietary Supplement Containing Dry Artichoke and Bergamot Extracts on Metabolic and Vascular Risk Factors in Individuals with Suboptimal Cholesterol Levels" Nutrients 16, no. 11: 1587. https://doi.org/10.3390/nu16111587
APA StyleFogacci, F., Giovannini, M., Di Micoli, A., Fiorini, G., Grandi, E., Borghi, C., & Cicero, A. F. G. (2024). A Randomized, Double-Blind, Placebo-Controlled Clinical Trial on the Effect of a Dietary Supplement Containing Dry Artichoke and Bergamot Extracts on Metabolic and Vascular Risk Factors in Individuals with Suboptimal Cholesterol Levels. Nutrients, 16(11), 1587. https://doi.org/10.3390/nu16111587