Abstract
(1) Background: Cardiovascular diseases (CVDs) are the leading cause of mortality worldwide. The aim of the study was to examine the existing published results of the association between elevated serum phosphate concentrations and cardiovascular mortality, along with the CVD incidence and subclinical coronary atherosclerosis, in primary prevention among non-selected samples of the general population. (2) Methods: A systematic review and meta-analysis were carried out using literature obtained from PubMed, SCOPUS, and the Web Of Science until March 2024 and following the PRISMA guidelines. Relevant information was extracted and presented. Random and fixed effects models were used to estimate the pooled odds ratio (OR) and hazard ratio (HR) with their 95% coefficient interval (CI), and I2 was used to assess heterogeneity. (3) Results: Twenty-five studies met our inclusion criteria and were included in the meta-analysis (11 cross-sectional and 14 cohort studies). For cardiovascular mortality, which included 7 cohort studies and 41,764 adults, the pooled HR was 1.44 (95% CIs 1.28, 1.61; I2 0%) when the highest versus the reference level of serum phosphate concentrations were compared. For CVDs, which included 8 cohort studies and 61,723 adults, the pooled HR was 1.12 (95% CIs 0.99, 1.27; I2 51%). For subclinical coronary atherosclerosis, which included 11 cross-sectional studies and 24,820 adults, the pooled OR was 1.44 (95% CIs 1.15, 1.79; I2 88%). (4) Conclusions: The highest serum phosphate concentrations were positively associated with a 44% increased risk of cardiovascular mortality and subclinical coronary atherosclerosis.
1. Introduction
Cardiovascular diseases (CVDs) are the leading causes of morbidity and mortality in developed countries despite the improvements in primary prevention and treatments in recent decades [1,2,3,4,5]. Moreover, the Global Burden of Disease study in 2019 [4] showed that the incidence of CVDs has been steadily increasing for decades in almost all non-high-income countries. This burden of disease can be assessed as CVD mortality, CVD incidence, as well as the presence of subclinical coronary atherosclerosis when the disease has not been identified yet. In this sense, the incidence of atherosclerotic CVDs has declined in the past two decades in the adult population but not in the younger segment; therefore, prevention must start at the earliest possible stage [6].
Along with the traditional cardiovascular risk factors, such as dyslipidemia, hypertension, and tobacco consumption [7,8], new non-traditional exposures have been investigated. Some of them are of increasing interest due to their high presence in our habitual diet, mainly when consuming ultra-processed foods (UPFs). Among them, the exposure to phosphates has been of interest in the last 20 years [9,10,11].
Phosphorus is an essential mineral in the human body, necessary for numerous physiological functions, such as bone health, energy metabolism, and signal transduction [12,13,14]. The body obtains this mineral from food. Thus, the main dietary sources of phosphorus in its natural form (as organic phosphorus) are foods high in protein (such as dairy products, legumes, meat, and fish). However, inorganic phosphorus salts are added to food as additives, specifically in UPFs [15]. Common food items with significant amounts of added phosphorus are processed meat (such as ham and sausages), canned fish, baked goods, cola drinks, and other soft drinks [16]. Unlike organic phosphorus, inorganic phosphorus has higher bioavailability, being almost completely absorbed in the gastrointestinal tract [17,18,19,20]. In the human body, almost all phosphorus is combined with oxygen to form phosphate. Phosphate is primarily present in the blood in its organic form, bound to proteins, while the remaining (approximately 30%) is in its ionized form, also called inorganic phosphate, and freely circulates in the bloodstream [21,22].
Previously, only two meta-analyses assessing the association between serum phosphate and cardiovascular risk have been published. One of them examined the association between elevated fasting serum phosphate concentration and the risk of death and CVDs in individuals with chronic kidney disease (CKD) [23]. Therefore, the results could not be generalized to the general population. The second one assessed the association of serum phosphate with all-cause and cardiovascular mortality in the general population; however, it was based on a limited number of studies [24]. The study of this association is of great interest, and recently published articles suggest that even an elevated serum phosphate concentration within the normal range might contribute to increased cardiovascular risk independently of kidney function [25,26].
Our aim was to conduct a meta-analysis based on published epidemiological studies assessing the association between serum phosphorus concentration and cardiovascular mortality in non-selected samples of the general population. CVD incidence and subclinical coronary atherosclerosis were also considered as main outcomes.
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
From conception of this meta-analysis, we followed the Cochrane Handbook for Systematic Review of Intervention [27], and the search was conducted according to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement recommendations [28]. The results were reported according to the Meta-analysis of Observational Studies in Epidemiology (MOOSE) [29] and PRISMA reporting guidelines [28]. The review methods were established “a priori” before the review was carried out. The study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO): CRD42023433390.
An advanced search of published evidence was conducted to identify articles on the association between serum levels of phosphate and cardiovascular mortality, CVDs, and subclinical coronary atherosclerosis. The data sources included the electronic databases PubMed, SCOPUS, and the Web Of Science from inception to March 2024 (included). The review was carried out using specific keywords related to the outcomes of interest and was conducted using MeSH terms to create a uniform and comprehensive search strategy, for which the terms and language filters are listed in Table 1.

Table 1.
Search strategy in selected databases.
2.2. Study Selection
The inclusion criteria were defined according to the following items: (a) studies assessing serum phosphate–cardiovascular mortality, serum phosphate–CVD (coronary heart disease, stroke, and heart failure), and serum phosphate–subclinical coronary atherosclerosis relationships in population-based epidemiological studies (experimental, observational, as well as cross-sectional studies); (b) studies conducted in humans aged over 18 without previously established CVDs; (c) studies reporting Hazard Ratio (HR), Odds Ratio (OR), or Prevalence Ratio (PR) with their corresponding 95% Confidence Interval (CI).
The exclusion criteria were defined according to the following items: (a) pregnant women, because in this population, volume could affect serum phosphate concentrations, making the results non comparable; (b) studies assessing outcomes other than the main ones considered, such as aortic stenosis, left ventricular mass, atrial fibrillation, arterial stiffness, endothelial dysfunction, or using a score to predict cardiovascular risk; (c) studies performed in selected populations (for example, on secondary cardiovascular prevention, diabetics, patients with chronic renal disease, or multiple myeloma); (d) studies with low methodological quality for which the validity of the study results was threatened; and (e) in addition, we excluded reviews, meta-analyses, conference articles, letters to the editor, and articles in which essential information to be meta-analyzed was missing.
2.3. Data Extraction and Risk of Bias Assessment
Data extraction was undertaken independently by two reviewers (CT-B and PG-C), who screened articles titles and abstracts. Disagreements between these researchers were discussed with another author (BM-F) and settled by consensus.
After reading the full text and Supplementary Materials of the selected studies, the following data from each article were extracted: the first author’s name, publication year, country of the study (sample), sample size, men (%), age, follow-up time, outcome, diagnostics and measurements, number of cases, association estimates (HR, OR, or PR) when comparing the highest vs. the reference level of serum phosphate concentrations, and adjustment for confounding factors. Finally, the Joanna Briggs Institute (JBI) critical appraisal checklist tool for cohort and case–control studies was selected to assess the risk of bias [30].
2.4. Statistical Analysis
We calculated central pooled estimates of the association for the highest category compared to the reference category of serum phosphate concentrations and their 95% CIs. Heterogeneity among studies was assessed by using the I2 test. An I2 > 30% indicated heterogeneity, and then a random-effects model was used; otherwise, a fixed-effects model was performed. Furthermore, when a study reported data separately for men and women, we entered the data as independent studies. Publication bias was examined by visual inspection of the funnel plot as well as by calculating the Egger’s test (p value < 0.05 indicated the presence of publication bias) [31]. Analyses were performed with R statistical software (version 4.0.4).
3. Results
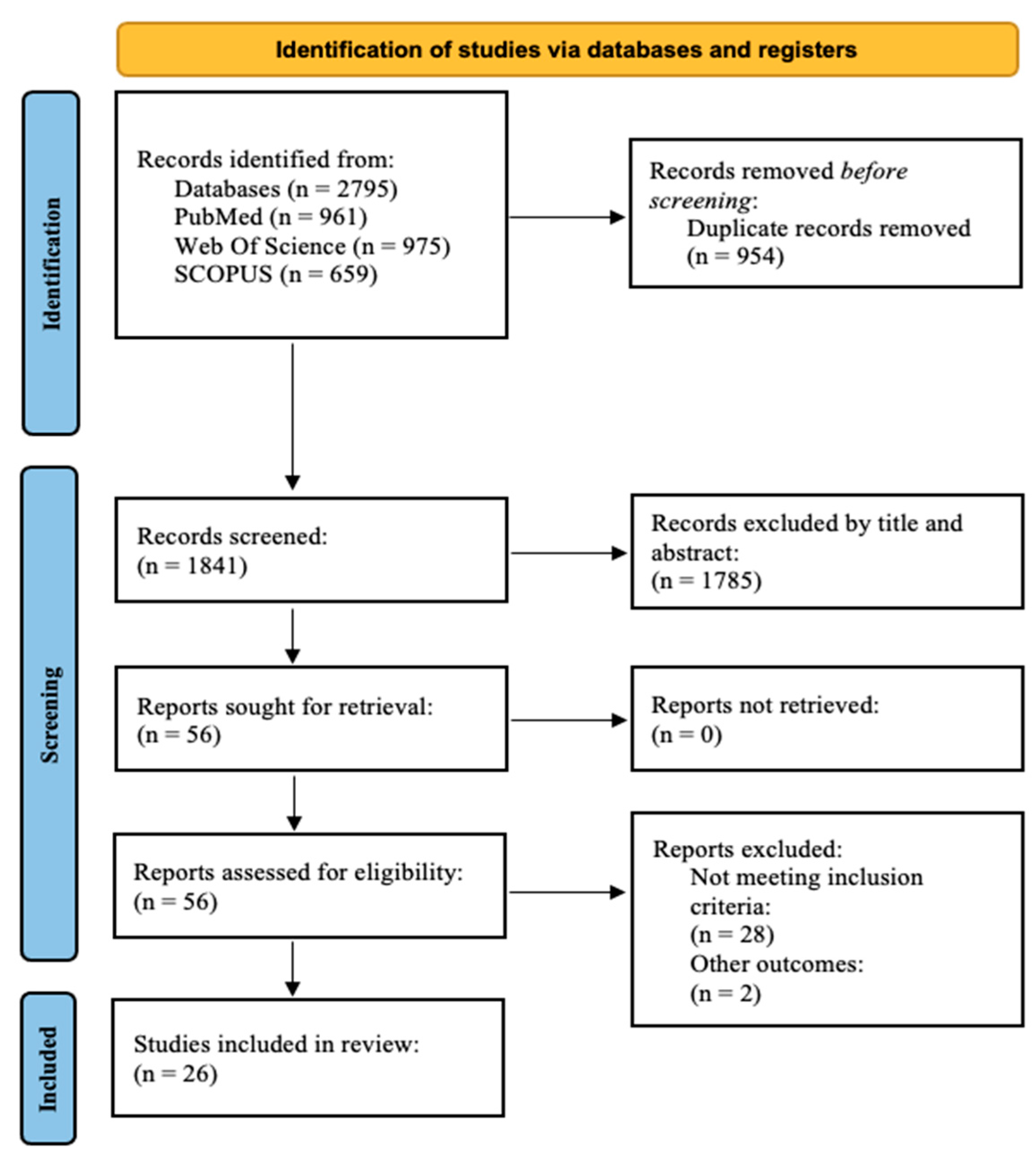
We identified 2795 records through our search. After removing replicates, exclusions were made after reading the title or the abstract. A total of 56 reports were sought for retrieval and assessed for eligibility. Of these, 29 articles were excluded because they did not meet the inclusion criteria, and two articles were excluded because other outcomes were evaluated [32,33]. Finally, 25 quality studies were included in the review (all of them were cohort or cross-sectional studies). No articles were excluded due to risk of bias (Figure 1).
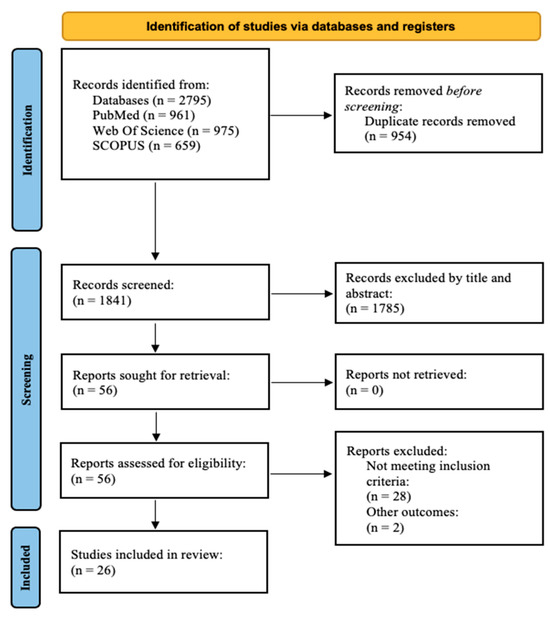
Figure 1.
PRISMA 2020 flow diagram for systematic reviews.
A total of seven articles that assessed the relationship between serum phosphate concentrations and cardiovascular mortality were included [22,34,35,36,37,38,39]. For CVDs, eight articles were included [39,40,41,42,43,44,45,46]. Finally, we found 11 articles reporting the relationship between serum phosphate concentrations and subclinical atherosclerosis (independently of the method used for measurement), whether it was reported as coronary arterial calcification (CAC) or as the presence of atheroma plaque [1,14,25,26,47,48,49,50,51,52,53].
3.1. Cardiovascular Mortality
Cardiovascular mortality was obtained based on the specific cause of death from national registries, death certificates, or medical records. Seven prospective cohort studies [22,34,35,36,37,38,39] assessed the relationship between serum phosphate concentrations and cardiovascular mortality. All of the studies had a low risk of bias, reaching at least 9 points according to the JBI critical appraisal checklist (Table 2).
Table 2.
Characteristics of the cardiovascular mortality studies sorted by year of publication.
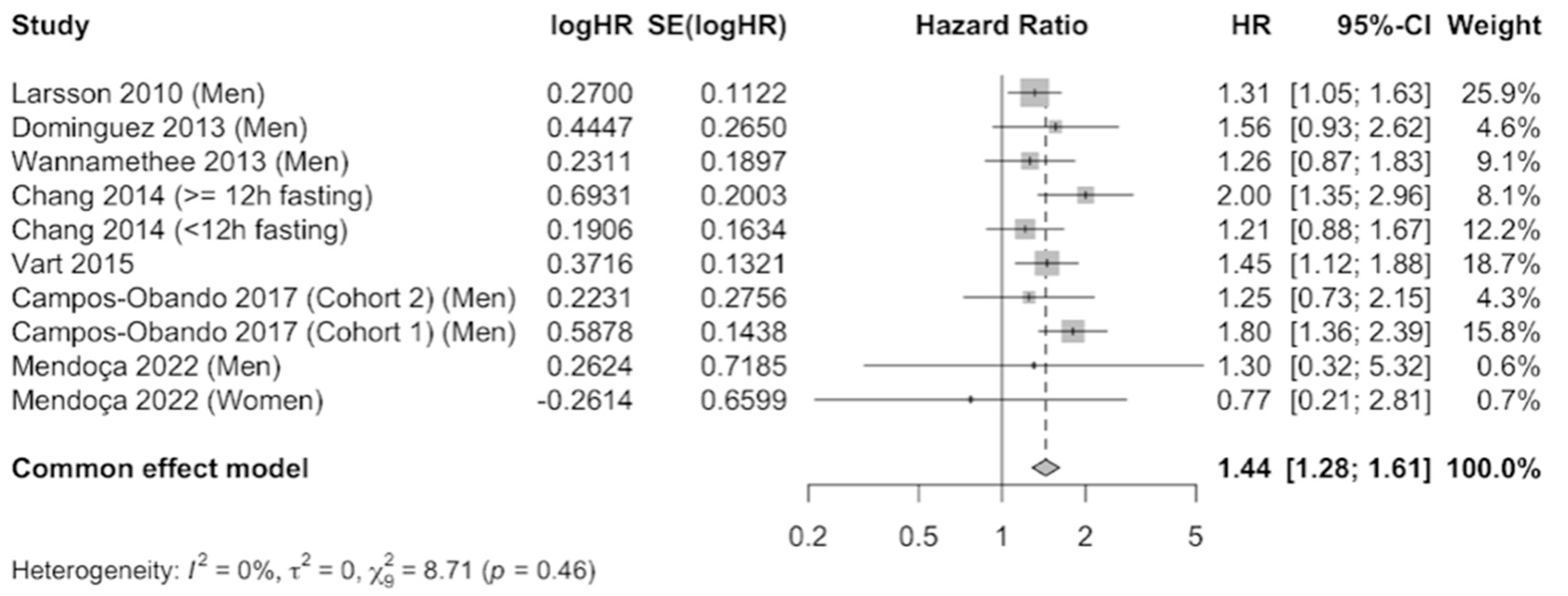
The results were meta-analyzed using a fixed-effects model because no evidence of heterogeneity was observed (I2 = 0%) after combining the results that compared the highest level of serum phosphate versus the category of reference. A total of 41,764 participants were included. The pooled estimate (HR 1.44, 95% CI 1.28–1.61, p = 0.46) showed a 44% increase in cardiovascular mortality risk in participants with elevated serum phosphate concentrations, which was statistically significant (Figure 2). Publication bias was not observed by examination of the funnel plot (Supplementary Figure S1) nor by using the Egger’s test (p = 0.7023).
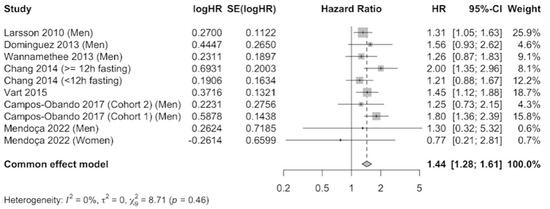
Figure 2.
Forest plot of association of serum phosphate with cardiovascular mortality using a fixed-effects model [22,34,35,36,37,38,39].
3.2. Cardiovascular Diseases
Information on CVDs was obtained by reviewing hospital records of those participants who mentioned in the interviews having suffered from coronary heart disease, stroke, or heart failure or by reviewing the country’s health databases. Thirteen articles were included in the systematic review, including seven studying the relationship with coronary heart disease [39,40,41,43,45,46], three with stroke [39,43,45], and three with heart failure [40,42,44]. The designs of the selected articles were nine prospective cohort studies and one case–control study. All of the studies had a low risk of bias according to the JBI critical appraisal checklist, reaching at least 10 points for the prospective cohort studies as well as the maximum score for the cross-sectional studies (Table 3).
Table 3.
Characteristics of the cardiovascular disease studies sorted by year of publication.
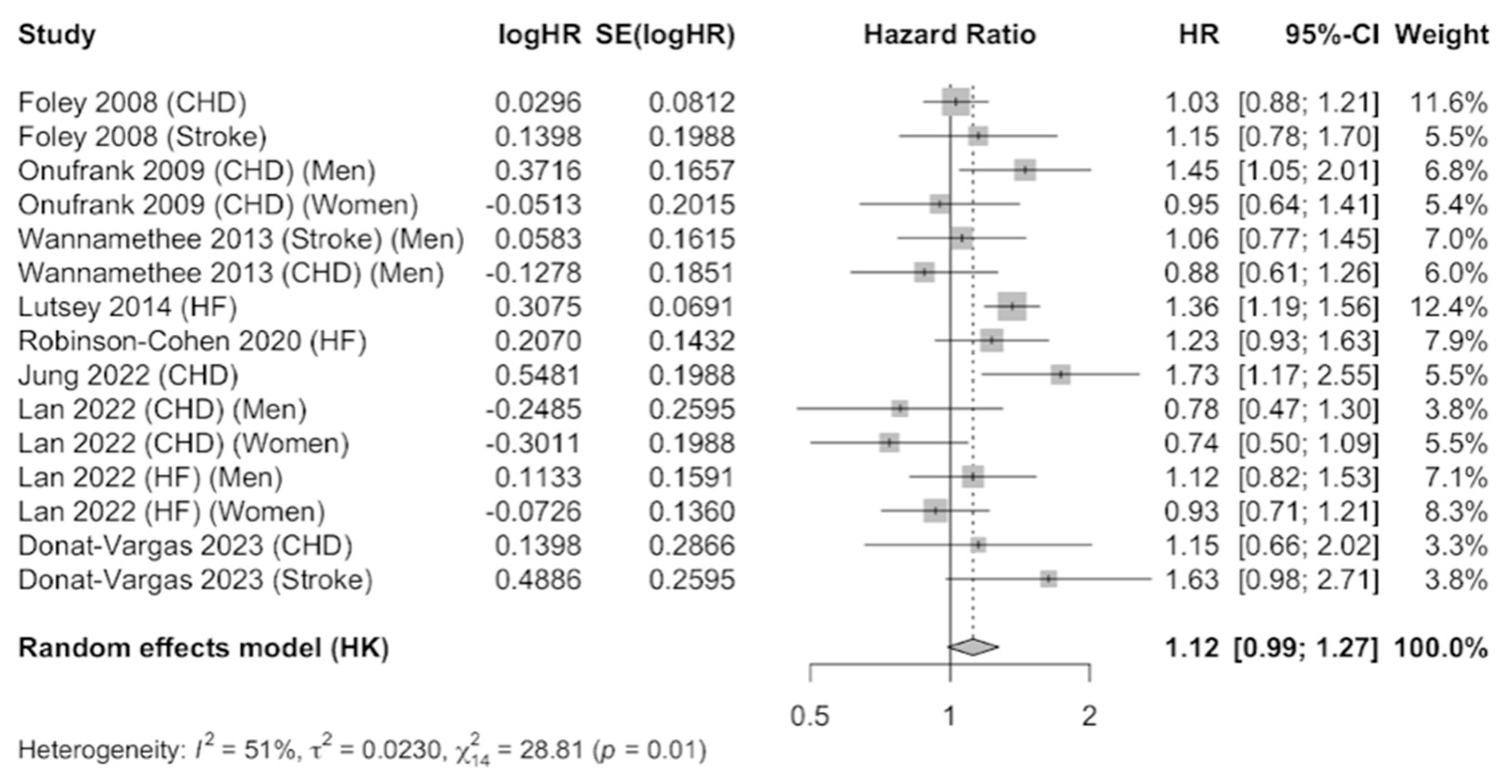
The JBI criteria for case–control studies include: (1) comparable groups; (2) cases and controls matched appropriately; (3) criteria for identification of cases and controls; (4) exposure measurement; (5) exposure measured in the same way for cases and controls; (6) confounding factors; (7) strategies to deal with confounders; (8) outcome measurement; (9) exposure period of interest sufficient; and (11) statistical analysis. The eight prospective cohort studies that were meta-analyzed [25,41,42,43,44,45,46,47] provided information on coronary heart disease (six studies), stroke (three studies), and heart failure (three studies). The results were combined using a random-effects model as evidence of heterogeneity was observed (I2 = 51%), after combining the results that compared the highest level of serum phosphate versus the category of reference. A total of 61,723 participants were included. The pooled estimate (HR 1.12, 95% CI 0.99–1.27, p < 0.01) showed a 12% increase in the incidence of CVDs in participants with elevated serum phosphate concentrations, which was marginally significant (Figure 3). Publication bias was not observed by examination of the funnel plot (Supplementary Figure S2) nor by using the Egger’s test (p = 0.3916).
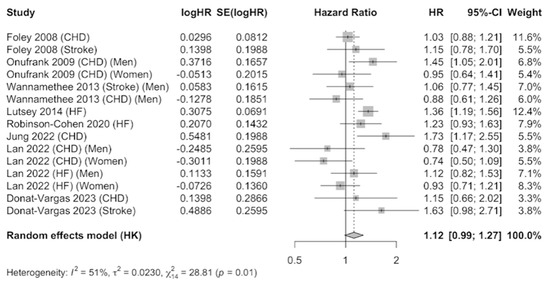
Figure 3.
Forest plot of association of serum phosphate with cardiovascular disease using a random-effects model [39,40,41,42,43,44,45,46].
3.3. Subclinical Coronary Atherosclerosis
Subclinical coronary atherosclerosis was assessed by computed tomography in all of the studies. However, subclinical atherosclerosis was measured differently by the presence of at least one plaque or by using different scores (Agatston Score, Gensi Score, and Fresinger Score). Eleven cross-sectional studies [1,14,25,26,47,48,49,50,51,52,53] assessed the relationship between serum phosphate concentrations and subclinical coronary atherosclerosis. All of the studies had a low risk of bias, reaching the maximum score according to the JBI critical appraisal checklist (Table 4).
Table 4.
Characteristics of the subclinical coronary atherosclerosis studies sorted by year of publication.
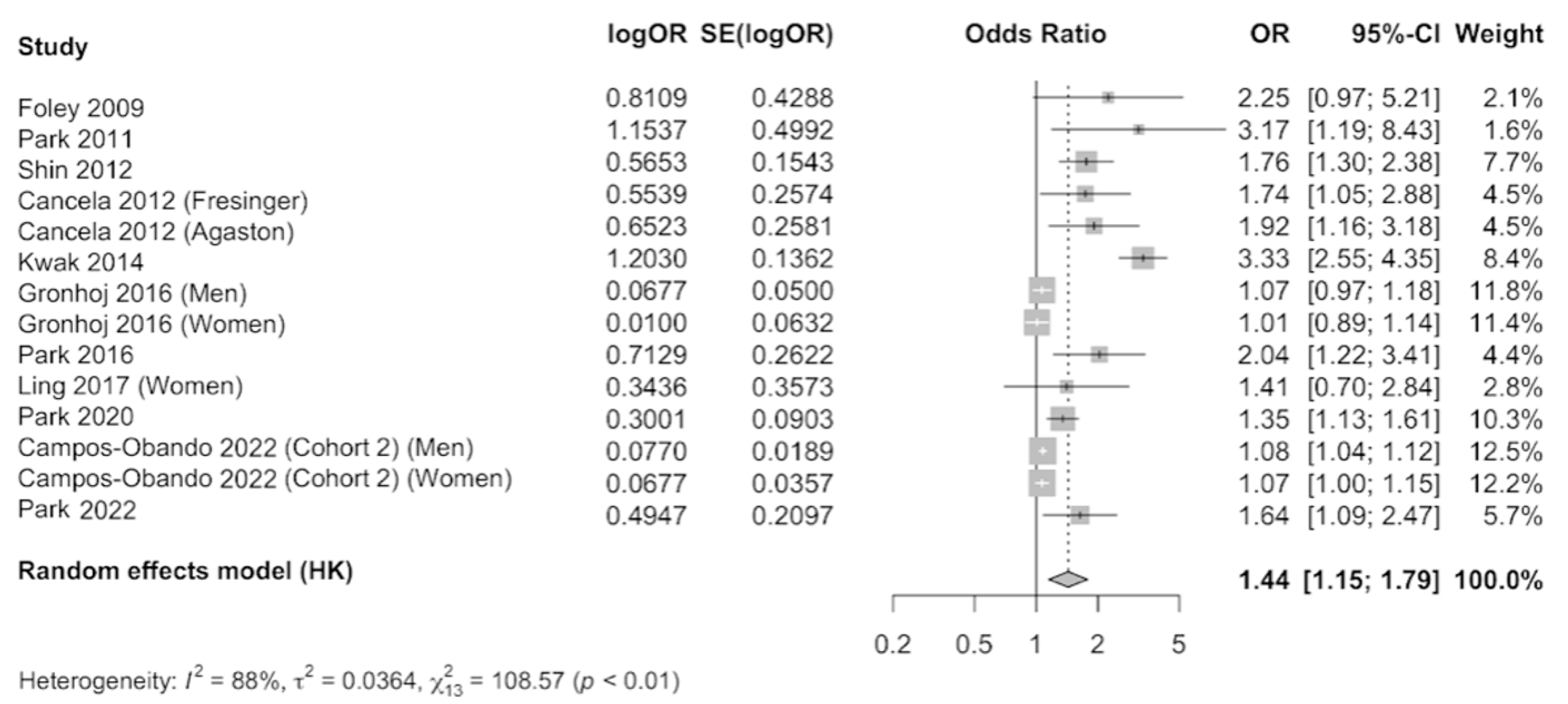
The results were meta-analyzed using a random-effects model as evidence of heterogeneity was observed (I2 = 88%), after combining the results that compared the highest level of serum phosphate versus the category of reference. A total of 24,820 participants were included. The pooled estimate (OR 1.44, 95% CI 1.15–1.79, p < 0.01) showed a 44% increase in the occurrence of subclinical coronary atherosclerosis in individuals with elevated serum phosphate concentration, which was statistically significant (Figure 4). Publication bias was observed by examination of the funnel plot (Supplementary Figure S3) and by using the Egger’s test (p = 0.004).
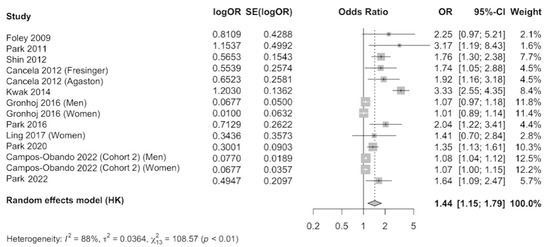
Figure 4.
Forest plot of association of serum phosphate with subclinical coronary atherosclerosis using a random-effects model [1,14,25,26,47,48,49,50,51,52,53].
4. Discussion
This updated meta-analysis is based on 25 epidemiological studies, including a total of 126,614 adults from the general population. The results provide important evidence about the consistent positive relationship between elevated serum phosphate concentrations and cardiovascular outcomes. Individuals with higher serum phosphate levels have a 44% higher risk of cardiovascular death. For subclinical coronary atherosclerosis among participants previously free of CVDs, the results are similar. Thus, individuals with higher serum phosphate levels also have a 44% higher prevalence of subclinical coronary atherosclerosis. For CVD events, the association is also positive, but marginally significant. As far as we know, this is the first meta-analysis that shows the relationships between serum phosphate and CVD events as well as subclinical coronary atherosclerosis.
For cardiovascular mortality, our findings are consistent with a previous review [24] suggesting that individuals with higher serum phosphate levels had a 36% higher risk of cardiovascular mortality. In this updated meta-analysis that comprises seven high-quality studies, the association found between serum phosphate and cardiovascular mortality is slightly higher, and no heterogeneity was observed among studies. In the same way, no evidence of publication bias was observed, suggesting that the observed association is valid. This meta-analysis provides the best available evidence to assess the studied associations. However, we do not have enough evidence to draw conclusions about the variation in associations by sex.
For cardiovascular events, 12 cohort studies were included in this meta-analysis. Our results show a positive association without achieving statistical significance. High heterogeneity was found, probably due to the inclusion of three different outcomes (coronary heart disease, stroke, and heart failure). The number of studies was not enough to carry out separate analyses. Therefore, more evidence is needed for this outcome.
For subclinical coronary atherosclerosis, 11 studies were selected. High heterogeneity across studies was found, probably due to the different definitions used to characterize subclinical coronary atherosclerosis (presence of plaques or different calcium scores). It is of note that all of the studies had a cross-sectional design. However, since subclinical coronary atherosclerosis is asymptomatic, participants did not modify their behaviors (including dietary habits) because of the presence of the disease. We also highlight that all of the articles had a high-quality score and low risk of bias. However, in this analysis, we could not rule out the presence of publication bias.
Dietary phosphorus derived from inorganic sources may have a greater influence on serum phosphate [54]. High absolute phosphorus intake has been associated with all-cause mortality starting from 1400 milligrams of phosphorus per day, which is twice the U.S. Recommended Daily Allowance for adults. Also, it has been reported that more than one-third of Americans consume more than 1400 mg of phosphorus per day [55]. Phosphorus additives are often added to UPFs during their processing to improve certain product characteristics, such as flavor, creaminess, preservation, and juiciness, or to prevent separation of beverages into individual ingredients [17]. Currently, there is considerable concern about the increased consumption of UPFs in recent decades [56,57], as a UPF-rich diet increases daily phosphorus intake by 250–1000 mg compared with a diet based on fresh and unprocessed foods [58]. Therefore, effective algorithms have been proposed to identify children at intermediate-high risk of future CVDs in order to promote the development of preventive programs that may personalize healthy lifestyles, behavioral modifications, and improved nutritional habits [59].
Serum phosphate levels are regulated by several complex compensatory mechanisms, including gastrointestinal absorption, intracellular displacement, and renal excretion [60,61]. Intestinal absorption of phosphorus depends on its form and source. Natural organic phosphorus sources are less digested and therefore less bioavailable, with absorption from 20 to 60% [62]. By contrast, inorganic phosphorus is more bioavailable, being almost completely absorbed in the digestive tract, as it does not require enzymatic digestion and dissociates rapidly in stomach acid; phosphorus additives are composed of inorganic phosphate [15,17,18,19,20]. In addition, it is possible that dietary phosphorus derived from inorganic sources may have a greater influence on serum phosphate and parathyroid hormones [62].
In healthy subjects, serum phosphate is almost completely filtered through the renal glomerulus, and 80–90% is reabsorbed. Total renal phosphate excretion is balanced with phosphorous intake [20,63]. Therefore, the measurement of urinary phosphate excretion in individuals with preserved renal function is considered a reliable marker of intestinal phosphorus absorption.
Regarding CVDs and serum phosphate, both postprandial elevation of serum phosphate and continued elevation of serum phosphate should be considered in the development of CVDs [64]. Certain in vitro studies have shown that hyperphosphatemia induces phenotypic conversion of vascular smooth muscle cells into osteoblast-like cells that express biochemical markers characteristic of bone tissue, resulting in vascular calcification in humans [65]. In addition, both in vitro and in vivo studies have demonstrated that high dietary phosphorus intake causes endothelial dysfunction within a short period, suggesting that the elevation of serum phosphate concentrations due to dietary phosphorus load may be a risk factor for endothelial dysfunction in both healthy individuals and those with CKD [64]. However, the causal relationship between higher serum phosphate concentrations and coronary atherosclerosis has not been fully explained yet.
Our study has some strengths. First, we explore separately the association between serum levels of phosphate and the risk of mortality, CVDs, and subclinical coronary atherosclerosis in primary prevention. Therefore, for CVD incidence and subclinical coronary atherosclerosis, studies involving individuals with previous CVDs were excluded. In addition, the included studies in these meta-analyses had high methodological quality. In cohort studies as well as in cross-sectional studies, the results were adjusted for an important number of confounding factors. Finally, the PRISMA guidelines were followed in performing the meta-analysis and reporting the results.
However, our study also has some possible limitations. First, the results show a high degree of heterogeneity in two of the study outcomes (I2 = 51% for CVDs and I2 = 88% for subclinical coronary atherosclerosis). This heterogeneity and the presence of a certain degree of publication bias for subclinical coronary atherosclerosis could be related to differences in the measurement of serum phosphate as well as the quantification of subclinical coronary atherosclerosis, as different measurements were used. Moreover, all CVDs were meta-analyzed together, without being able to distinguish among different types. Also, in all cases, serum phosphate concentrations were measured at a single time point, without considering changes over time, which could lead to non-differential misclassification. Similarly, changes in weight loss [66] or changes in other confounding factors were not taken into account in the published articles, which could have led to regression dilution bias.
5. Conclusions
Higher serum phosphate concentrations are positively associated with a 44% increase in mortality and subclinical coronary atherosclerosis in the general population. In the future, it is desirable to publish more studies that evaluate the association between serum phosphate and incident CVDs in order to independently assess the association for coronary heart disease, stroke, and heart failure.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/nu16111599/s1, Figure S1: Funnel plot of association between serum phosphate and cardiovascular mortality; Figure S2: Funnel plot of association between serum phosphate and cardiovascular disease; Figure S3: Funnel plot of association between serum phosphate and subclinical coronary atherosclerosis.
Author Contributions
The authors’ contributions were as follows—C.T.-B.: analysis, writing—original draft and visualization. B.M.-F.: methodology, resources, investigation, writing—review and editing and supervision. P.G.-C.: conceptualization, methodology, writing—review and editing, validation, and project administration. A.M.-C.: analysis, writing—review and editing. N.C.-G., J.A.C. and C.S.-O.: writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This work was funded by the following grants: FIS PI19/948 and FIS PI20/144 (State Secretary of R + D and FEDER/FSE), the CIBERESP, CIBERobn, and CIBERCV Instituto de Salud Carlos III, Madrid, Spain.
Data Availability Statement
Data described in the manuscript, code book, and analytic code will be made available upon request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Grønhøj, M.H.; Gerke, O.; Mickley, H.; Hald, F.; Lambrechtsen, J.; Sand, N.P.R.; Rasmussen, L.M.; Olsen, M.H.; Diederichsen, A. Associations between Calcium-Phosphate Metabolism and Coronary Artery Calcification; a Cross Sectional Study of a Middle-Aged General Population. Atherosclerosis 2016, 251, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Xia, C.; Vonder, M.; Sidorenkov, G.; Den Dekker, M.; Oudkerk, M.; Van Bolhuis, J.N.; Pelgrim, G.J.; Rook, M.; De Bock, G.H.; Van Der Harst, P.; et al. Cardiovascular Risk Factors and Coronary Calcification in a Middle-Aged Dutch Population: The ImaLife Study. J. Thorac. Imaging 2021, 36, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Vliegenthart, R.; Oudkerk, M.; Hofman, A.; Oei, H.H.S.; Van Dijck, W.; Van Rooij, F.J.A.; Witteman, J.C.M. Coronary Calcification Improves Cardiovascular Risk Prediction in the Elderly. Circulation 2005, 112, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Gregory, R.; Gregory, M.; Catherine, J.; Giovanni, A.; Enrico, A.; Larry, B.; Noël, B.; Andrea, B. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2020 Update a Report from the American Heart Association. Circulation 2020, 141, E139–E596. [Google Scholar] [CrossRef] [PubMed]
- Vikulova, D.N.; Grubisic, M.; Zhao, Y.; Lynch, K.; Humphries, K.H.; Pimstone, S.N.; Brunham, L.R. Premature Atherosclerotic Cardiovascular Disease: Trends in Incidence, Risk Factors, and Sex-Related Differences, 2000 to 2016. J. Am. Heart Assoc. 2019, 8, e012178. [Google Scholar] [CrossRef] [PubMed]
- Wilson, P.W.F.; D’agostino, R.B.; Levy, D.; Belanger, A.M.; Silbershatz, H.; Kannel, W.B. Prediction of Coronary Heart Disease Using Risk Factor Categories. Circulation 1998, 97, 1837–1847. [Google Scholar] [CrossRef] [PubMed]
- Conroy, R.M.; Pyörälä, K.; Fitzgerald, A.P.; Sans, S.; Menotti, A.; De Backer, G.; De Bacquer, D.; Ducimetière, P.; Jousilahti, P.; Keil, U.; et al. Estimation of Ten-Year Risk of Fatal Cardiovascular Disease in Europe: The SCORE Project. Eur. Heart J. 2003, 24, 987–1003. [Google Scholar] [CrossRef]
- Sheridan, K.; Logomarsino, J.V. Effects of Serum Phosphorus on Vascular Calcification in a Healthy, Adult Population: A Systematic Review. J. Vasc. Nurs. 2017, 35, 157–169. [Google Scholar] [CrossRef]
- Zhou, C.; Shi, Z.; Ouyang, N.; Ruan, X. Hyperphosphatemia and Cardiovascular Disease. Front. Cell. Dev. Biol. 2021, 9, 644363. [Google Scholar] [CrossRef]
- Villa-Bellosta, R. Vascular Calcification: Key Roles of Phosphate and Pyrophosphate. Int. J. Mol. Sci. 2021, 22, 13536. [Google Scholar] [CrossRef]
- Chonchol, M.; Dale, R.; Schrier, R.W.; Estacio, R. Serum Phosphorus and Cardiovascular Mortality in Type 2 Diabetes. Am. J. Med. 2009, 122, 380–386. [Google Scholar] [CrossRef]
- Volk, C.; Schmidt, B.; Brandsch, C.; Kurze, T.; Schlegelmilch, U.; Grosse, I.; Ulrich, C.; Girndt, M.; Stangl, G.I. Acute Effects of an Inorganic Phosphorus Additive on Mineral Metabolism and Cardiometabolic Risk Factors in Healthy Subjects. J. Clin. Endocrinol. Metab. 2022, 107, E852–E864. [Google Scholar] [CrossRef]
- Ling, Y.; Wang, Z.; Wu, B.; Gao, X. Association of Bone Metabolism Markers with Coronary Atherosclerosis and Coronary Artery Disease in Postmenopausal Women. J. Bone Miner. Metab. 2017, 36, 352–363. [Google Scholar] [CrossRef]
- Younes, M.; Aquilina, G.; Castle, L.; Engel, K.H.; Fowler, P.; Frutos Fernandez, M.J.; Fürst, P.; Gürtler, R.; Husøy, T.; Mennes, W.; et al. Re-Evaluation of Phosphoric Acid–Phosphates–Di-, Tri- and Polyphosphates (E 338–341, E 343, E 450–452) as Food Additives and the Safety of Proposed Extension of Use. EFSA J. 2019, 17, e05674. [Google Scholar] [CrossRef]
- Ritz, E.; Hahn, K.; Ketteler, M.; Kuhlmann, M.K.; Mann, J. Phosphate Additives in Food—A Health Risk. Dtsch. Arztebl. Int. 2012, 109, 49–55. [Google Scholar] [CrossRef]
- Calvo, M.S.; Uribarri, J. Contributions to Total Phosphorus Intake: All Sources Considered. Semin. Dial. 2013, 26, 54–61. [Google Scholar] [CrossRef]
- McCarty, M.F.; DiNicolantonio, J.J. Bioavailable Dietary Phosphate, a Mediator of Cardiovascular Disease, May Be Decreased with Plant-Based Diets, Phosphate Binders, Niacin, and Avoidance of Phosphate Additives. Nutrition 2014, 30, 739–747. [Google Scholar] [CrossRef]
- Cupisti, A.; Kalantar-Zadeh, K. Management of Natural and Added Dietary Phosphorus Burden in Kidney Disease. Semin. Nephrol. 2013, 33, 180–190. [Google Scholar] [CrossRef]
- Chang, A.R.; Anderson, C. Dietary Phosphorus Intake and the Kidney. Annu. Rev. Nutr. 2017, 37, 321–346. [Google Scholar] [CrossRef]
- Standing Committee on the Scientific Evaluation of Dietary Reference Intakes; Institute of Medicine (US). Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride; National Academies Press: Washington, DC, USA, 1997; ISBN 0-309-06350-7. [Google Scholar]
- Campos-Obando, N.; Lahousse, L.; Brusselle, G.; Stricker, B.H.; Hofman, A.; Franco, O.H.; Uitterlinden, A.G.; Zillikens, M.C. Serum Phosphate Levels Are Related to All-Cause, Cardiovascular and COPD Mortality in Men. Eur. J. Epidemiol. 2018, 33, 859–871. [Google Scholar] [CrossRef] [PubMed]
- Palmer, S.C.; ChB, M.; Hayen, A.; Macaskill, P.; Pellegrini, F.; Craig, J.C.; Elder, G.J.; Strippoli, M.G.F.; Renal Group, C.; Craig, A. Serum Levels of Phosphorus, Parathyroid Hormone, and Calcium and Risks of Death and Cardiovascular Disease in Individuals with Chronic Kidney Disease A Systematic Review and Meta-Analysis. JAMA 2011, 305, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Bai, W.; Li, J.; Liu, J. Serum Phosphorus, Cardiovascular and All-Cause Mortality in the General Population: A Meta-Analysis. Clin. Chim. Acta 2016, 461, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Park, K.S.; Lee, H.; Jeon, Y.-J.; Park, S.; Ann, S.H.; Kim, Y.-G.; Lee, Y.; Park, J.; Choi, S.H.; Park, G.-M. Serum Phosphorus and Subclinical Coronary Atherosclerosis in Asymptomatic Subjects without Kidney Dysfunction. Clin. Nephrol. 2022, 98, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Campos-Obando, N.; Bosman, A.; Kavousi, M.; Medina-Gomez, C.; van der Eerden, B.C.J.; Bos, D.; Franco, O.H.; Uitterlinden, A.G.; Zillikens, M.C. Genetic Evidence for a Causal Role of Serum Phosphate in Coronary Artery Calcification: The Rotterdam Study. J. Am. Heart Assoc. 2022, 11, e023024. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-Analysis of Observational Studies in Epidemiology: A Proposal for Reporting. Meta-Analysis of Observational Studies in Epidemiology (MOOSE) Group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Joanna Briggs Institute Critical-Appraisal-Tools—Critical Appraisal Tools|JBI. Available online: https://jbi.global/critical-appraisal-tools (accessed on 12 April 2023).
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. Br. Med. J. 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Abramowitz, M.; Muntner, P.; Coco, M.; Southern, W.; Lotwin, I.; Hostetter, T.H.; Melamed, M.L. Serum Alkaline Phosphatase and Phosphate and Risk of Mortality and Hospitalization. Clin. J. Am. Soc. Nephrol. 2010, 5, 1064–1071. [Google Scholar] [CrossRef]
- McGovern, A.P.; de Lusignan, S.; van Vlymen, J.; Liyanage, H.; Tomson, C.R.; Gallagher, H.; Rafiq, M.; Jones, S. Serum Phosphate as a Risk Factor for Cardiovascular Events in People with and without Chronic Kidney Disease: A Large Community Based Cohort Study. PLoS ONE 2013, 8, e74996. [Google Scholar] [CrossRef]
- Dominguez, J.R.; Kestenbaum, B.; Chonchol, M.; Block, G.; Laughlin, G.A.; Lewis, C.E.; Katz, R.; Barrett-Connor, E.; Cummings, S.; Orwoll, E.S.; et al. Relationships between Serum and Urine Phosphorus with All-Cause and Cardiovascular Mortality: The Osteoporotic Fractures in Men (MrOS) Study. Am. J. Kidney Dis. 2013, 61, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.R.; Grams, M.E. Serum Phosphorus and Mortality in the Third National Health and Nutrition Examination Survey (NHANES III): Effect Modification by Fasting. Am. J. Kidney Dis. 2014, 64, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Larsson, T.E.; Olauson, H.; Hagström, E.; Ingelsson, E.; Ärnlöv, J.; Lind, L.; Sundström, J. Conjoint Effects of Serum Calcium and Phosphate on Risk of Total, Cardiovascular, and Noncardiovascular Mortality in the Community. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Vart, P.; Nigatu, Y.T.; Jaglan, A.; van Zon, S.K.R.; Shafique, K. Joint Effect of Hypertension and Elevated Serum Phosphorus on the Risk of Mortality in National Health and Nutrition Examination Survey-III. J. Am. Heart Assoc. 2015, 4, e001706. [Google Scholar] [CrossRef]
- Mendonça, L.; Gonçalves, F.; Sampaio, S.; Castro-Chaves, P.; Pereira, L. Association between Serum Phosphorus and Mortality in NHANES 2003–2006: The Effect of Gender and Renal Function. J. Nephrol. 2022, 35, 165–178. [Google Scholar] [CrossRef]
- Wannamethee, S.G.; Sattar, N.; Papcosta, O.; Lennon, L.; Whincup, P.H. Alkaline Phosphatase, Serum Phosphate, and Incident Cardiovascular Disease and Total Mortality in Older Men. Arterioscler. Thromb. Vasc. Bio. 2013, 33, 1070–1076. [Google Scholar] [CrossRef]
- Lan, Q.; Zhang, Y.; Lin, F.; Meng, Q.; Buys, N.; Fan, H.; Sun, J. Sex-Specific Associations Between Serum Phosphate Concentration and Cardiometabolic Disease. Diabetes Metab. Syndr. Obes. 2022, 15, 813–826. [Google Scholar] [CrossRef]
- Jung, D.H.; Park, B.; Lee, Y.J. Longitudinal Effects of Serum Calcium and Phosphate Levels and Their Ratio on Incident Ischemic Heart Disease among Korean Adults. Biomolecules 2022, 12, 103. [Google Scholar] [CrossRef]
- Robinson-Cohen, C.; Shlipak, M.; Sarnak, M.; Katz, R.; Peralta, C.; Young, B.; Hoofnagle, A.N.; Szklo, M.; Ix, J.H.; Psaty, B.M.; et al. Impact of Race on the Association of Mineral Metabolism with Heart Failure: The Multi-Ethnic Study of Atherosclerosis. J. Clin. Endocrinol. Metab. 2020, 105, E1144–E1151. [Google Scholar] [CrossRef]
- Foley, R.N.; Collins, A.J.; Ishani, A.; Kalra, P.A. Calcium-Phosphate Levels and Cardiovascular Disease in Community-Dwelling Adults: The Atherosclerosis Risk in Communities (ARIC) Study. Am. Heart J. 2008, 156, 556–563. [Google Scholar] [CrossRef]
- Lutsey, P.L.; Alonso, A.; Michos, E.D.; Loehr, L.R.; Astor, B.C.; Coresh, J.; Folsom, A.R. Serum Magnesium, Phosphorus, and Calcium Are Associated with Risk of Incident Heart Failure: The Atherosclerosis Risk in Communities (ARIC) Study. Am. J. Clin. Nutr. 2014, 100, 756–764. [Google Scholar] [CrossRef]
- Donat-Vargas, C.; Guallar-Castillon, P.; Nyström, J.; Larsson, S.C.; Kippler, M.; Vahter, M.; Faxén-Irving, G.; Michaelsson, K.; Wolk, A.; Stenvinkel, P.; et al. Urinary Phosphate Is Associated with Cardiovascular Disease Incidence. J. Intern. Med. 2023, 294, 358–369. [Google Scholar] [CrossRef]
- Onufrak, S.J.; Bellasi, A.; Cardarelli, F.; Vaccarino, V.; Muntner, P.; Shaw, L.J.; Raggi, P. Investigation of Gender Heterogeneity in the Associations of Serum Phosphorus with Incident Coronary Artery Disease and All-Cause Mortality. Am. J. Epidemiol. 2009, 169, 67–77. [Google Scholar] [CrossRef]
- Cancela, A.L.; Santos, R.D.; Titan, S.M.; Goldenstein, P.T.; Rochitte, C.E.; Lemos, P.A.; dos Reis, L.M.; Graciolli, F.G.; Jorgetti, V.; Moysés, R.M. Phosphorus Is Associated with Coronary Artery Disease in Patients with Preserved Renal Function. PLoS ONE 2012, 7, e36883. [Google Scholar] [CrossRef]
- Park, K.S.; Park, J.; Choi, S.H.; Ann, S.H.; Singh, G.B.; Shin, E.S.; Lee, J.S.; Chung, H.C. Serum Phosphorus Concentration and Coronary Artery Calcification in Subjects without Renal Dysfunction. PLoS ONE 2016, 11, e0151007. [Google Scholar] [CrossRef]
- Park, K.S.; Chang, J.W.; Kim, T.Y.; Kim, H.W.; Lee, E.K.; Kim, H.S.; Yang, W.S.; Kim, S.B.; Park, S.K.; Lee, S.K.; et al. Lower Concentrations of Serum Phosphorus within the Normal Range Could Be Associated with Less Calcification of the Coronary Artery in Koreans with Normal Renal Function. Am. J. Clin. Nutr. 2011, 94, 1465–1470. [Google Scholar] [CrossRef]
- Shin, S.; Kim, K.J.; Chang, H.J.; Cho, I.; Kim, Y.J.; Choi, B.W.; Rhee, Y.; Lim, S.K.; Yang, W.I.; Shim, C.Y.; et al. Impact of Serum Calcium and Phosphate on Coronary Atherosclerosis Detected by Cardiac Computed Tomography. Eur. Heart J. 2012, 33, 2873–2881. [Google Scholar] [CrossRef]
- Foley, R.N.; Collins, A.J.; Herzog, C.A.; Ishani, A.; Kalra, P.A. Serum Phosphorus Levels Associate with Coronary Atherosclerosis in Young Adults. J. Am. Soc. Nephrol. 2009, 20, 397–404. [Google Scholar] [CrossRef]
- Park, K.S.; Lee, Y.; Park, G.M.; Park, J.H.; Kim, Y.G.; Yang, D.H.; Kang, J.W.; Lim, T.H.; Kim, H.K.; Choe, J.; et al. Association between Serum Phosphorus and Subclinical Coronary Atherosclerosis in Asymptomatic Korean Individuals without Kidney Dysfunction. Am. J. Clin. Nutr. 2020, 112, 66–73. [Google Scholar] [CrossRef]
- Kwak, S.M.; Kim, J.S.; Choi, Y.; Chang, Y.; Kwon, M.J.; Jung, J.G.; Jeong, C.; Ahn, J.; Kim, H.S.; Shin, H.; et al. Dietary Intake of Calcium and Phosphorus and Serum Concentration in Relation to the Risk of Coronary Artery Calcification in Asymptomatic Adults. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1763–1769. [Google Scholar] [CrossRef]
- Bringhurst, F.; Demay, M.; Krane, S.; Kronenberg, H. Bone and Mineral Metabolism in Health and Disease. In Harrison’s Principles of Internal Medicine, 20th ed.; Kasper, D., Fauci, A., Hauser, S., Longo, D., Jameson, J., Lozcalzo, J., Eds.; McGraw-Hill Education: New York, NY, USA, 2018; Available online: https://accessmedicine.mhmedical.com/content.aspx?bookid=2129§ionid=192530305 (accessed on 10 April 2023).
- Chang, A.R.; Lazo, M.; Appel, L.J.; Gutiérrez, O.M.; Grams, M.E. High Dietary Phosphorus Intake Is Associated with All-Cause Mortality: Results from NHANES III1-3. Am. J. Clin. Nutr. 2014, 99, 320–327. [Google Scholar] [CrossRef]
- Mertens, E.; Colizzi, C.; Peñalvo, J.L. Ultra-Processed Food Consumption in Adults across Europe. Eur. J. Nutr. 2022, 61, 1521–1539. [Google Scholar] [CrossRef]
- Huybrechts, I.; Rauber, F.; Nicolas, G.; Casagrande, C.; Kliemann, N.; Wedekind, R.; Biessy, C.; Scalbert, A.; Touvier, M.; Aleksandrova, K.; et al. Characterization of the Degree of Food Processing in the European Prospective Investigation into Cancer and Nutrition: Application of the Nova Classification and Validation Using Selected Biomarkers of Food Processing. Front. Nutr. 2022, 9, 1035580. [Google Scholar] [CrossRef]
- Gutiérrez, O.M. Sodium- and Phosphorus-Based Food Additives: Persistent but Surmountable Hurdles in the Management of Nutrition in Chronic Kidney Disease. Adv. Chronic Kidney Dis. 2013, 20, 150–156. [Google Scholar] [CrossRef]
- Ferraro, S.; Benedetti, S.; Mannarino, S.; Marcovina, S.; Biganzoli, E.M.; Zuccotti, G. Prediction of atherosclerotic cardiovascular risk in early childhood. Clin. Chim. Acta 2024, 552, 117684. [Google Scholar] [CrossRef]
- Kestenbaum, B. Phosphate Metabolism in the Setting of Chronic Kidney Disease: Significance and Recommendations for Treatment. Semin. Dial. 2007, 20, 286–294. [Google Scholar] [CrossRef]
- Sun, Q.; Bertrand, K.A.; Franke, A.A.; Rosner, B.; Curhan, G.C.; Willett, W.C. Reproducibility of Urinary Biomarkers in Multiple 24-h Urine Samples. Am. J. Clin. Nutr. 2017, 105, 159–168. [Google Scholar] [CrossRef]
- Karp, H.J.; Vaihia, K.P.; Kärkkäinen, M.U.M.; Niemistö, M.J.; Lamberg-Allardt, C.J.E. Acute Effects of Different Phosphorus Sources on Calcium and Bone Metabolism in Young Women: A Whole-Foods Approach. Calcif. Tissue Int. 2007, 80, 251–258. [Google Scholar] [CrossRef]
- Laflamme, D.; Backus, R.; Brown, S.; Butterwick, R.; Czarnecki-Maulden, G.; Elliott, J.; Fascetti, A.; Polzin, D. A Review of Phosphorus Homeostasis and the Impact of Different Types and Amounts of Dietary Phosphate on Metabolism and Renal Health in Cats. J. Vet. Intern. Med. 2020, 34, 2187–2196. [Google Scholar] [CrossRef] [PubMed]
- Shuto, E.; Taketani, Y.; Tanaka, R.; Harada, N.; Isshiki, M.; Sato, M.; Nashiki, K.; Amo, K.; Yamamoto, H.; Higashi, Y.; et al. Dietary Phosphorus Acutely Impairs Endothelial Function. J. Am. Soc. Nephrol. 2009, 20, 1504–1512. [Google Scholar] [CrossRef] [PubMed]
- Jono, S.; Mckee, M.D.; Murry, C.E.; Shioi, A.; Nishizawa, Y.; Mori, K.; Morii, H.; Giachelli, C.M. Phosphate regulation of vascular smooth muscle cell calcification. Circ. Res. 2000, 87, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Christou, G.A. Not Only the Status of Body Weight and Metabolic Health Matters for Cardiovascular Events, but Also the Temporal Changes. Eur. J. Prev. Cardiol. 2021, 28, E25–E27. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).