Abstract
Gut microbiome-modulating agents (MMAs), including probiotics, prebiotics, postbiotics, and synbiotics, are shown to ameliorate type 1 diabetes (T1D) by restoring the microbiome from dysbiosis. The objective of this systematic review and meta-analysis was to assess the impact of MMAs on hemoglobin A1c (HbA1c) and biomarkers associated with (T1D). A comprehensive search was conducted in PubMed, Web of Science, Embase, Cochrane Library, National Knowledge Infrastructure, WeiPu, and WanFang Data up to 30 November 2023. Ten randomized controlled trials (n = 630) were included, with study quality evaluated using the Cochrane risk-of-bias tool. Random-effect models with standardized mean differences (SMDs) were utilized. MMA supplementation was associated with improvements in HbA1c (SMD = −0.52, 95% CI [−0.83, −0.20]), daily insulin usage (SMD = −0.41, 95% confidence interval (CI) [−0.76, −0.07]), and fasting C-peptide (SMD = 0.99, 95% CI [0.17, 1.81]) but had no effects on FBG, CRP, TNF-α, IL-10, LDL, HDL, and the Shannon index. Subgroup analysis of HbA1c indicated that a long-term intervention (>3 months) might exert a more substantial effect. These findings suggest an association between MMAs and glycemic control in T1D. Further large-scale clinical trials are necessary to confirm these findings with investigations on inflammation and gut microbiota composition while adjusting confounding factors such as diet, physical activity, and the dose and form of MMA intervention.
1. Introduction
Type 1 diabetes (T1D) refers to an autoimmune disease leading to the self-destruction of insulin-producing pancreatic ß cells and insulin deficiency, which leads to impaired glucose metabolism [1]. T1D places heavy burdens on public health due to the rapid increase in prevalence rate and its complex condition for glucose management, especially in resource-limited countries [2]. Insulin therapy is the most accepted treatment for T1D, which requires subcutaneous insulin injection several times per day [3]. It causes several challenges, including high expenses, weight gain, risk of hypoglycemia, and low adherence [4]. Therefore, novel and economic therapy with high adherence and accessibility is needed to slow down the progression of T1D [5].
The gut microbiome has been shown to impact the occurrence and pathogenesis of T1D in recent years [6]. Case–control studies indicate that compared with healthy control subjects, T1D is associated with a significantly lower microbiota diversity, a higher relative abundance of Bacteroides, Ruminococcus, Blautia, and Streptococcus genera, and a lower relative abundance of Bifidobacterium, Roseburia, and Faecalibacterium [7]. An imbalanced Bacteroidetes-to-Firmicutes ratio leads to dysbiosis, which changes intestinal mucosa and alters gut permeability, resulting in a leaky gut [8,9]. In T1D subjects, the disharmonized intestinal microenvironment causes an increased level of proinflammatory cytokines and lipopolysaccharides (LPSs), and they enter into the bloodstream with greater accessibility since the tight junctions between colonocytes are damaged, resulting in an increased level of inflammatory substances in the bloodstream [10]. As a result, the inflammation status causes islet autoimmunity, leading to decreased fasting C-peptide (FCP) and elevated glycemic levels. FCP reflects endogenous insulin production and provides insights into residual beta-cell activity, which is commonly used to assess the effectiveness of interventions aimed at preserving or enhancing insulin secretion [11]. Glycated hemoglobin (HbA1c), a widely used biomarker for assessing long-term glucose control in individuals with diabetes, reflects the average blood glucose levels over the past 2–3 months, providing information about the effectiveness of diabetes management strategies [12].
Tackling dysbiosis is suggested to be a novel strategy for treating T1D, and using MMAs is considered to be a feasible way of restoring the gut microbiota [13]. MMAs are substances that regulate the gut microbiota, including probiotics, prebiotics, synbiotics, and postbiotics. Supplementation with probiotics in T1D adults has shown improved glycemic control and increased synthesis of Glucagon-like peptide-1 [14]. Prebiotics play a role in an increase in the number of lactic acid-producing bacteria and have immuno-modulatory properties [15]. Postbiotics from various microbiomes inhibit the growth of pathogenic bacteria [16]. Synbiotics exert a synergistic effect on the restoration of the gut microbiota [17]. Therefore, MMAs might play a role in maintaining gut microbiota homeostasis, stabilizing blood glucose levels, and reducing the level of proinflammatory cytokines while increasing anti-inflammatory cytokines, resulting in a slower T1D progression [18].
While there are abundant reviews exploring the relationship between MMAs and glycemic control, the majority of the literature predominantly focuses on type 2 diabetes (T2D). Conversely, the literature specifically addressing T1D is notably limited, with only two existing reviews identified. One review, encompassing five randomized controlled trials (RCTs) up to 8 October 2022, examined the impact of probiotics and synbiotics on glycemic control, focusing on outcomes such as fasting blood glucose (FBG), HbA1c, fasting C-peptide (FCP), and daily insulin usage (DIU) [19]. However, it did not delve into the outcomes related to T1D pathogenesis, such as inflammatory cytokines and gut microbiota composition. Another recent review aimed to explore the effects of probiotic and synbiotic interventions on both T1D and T2D [20]. Despite its inclusion of a large overall sample size, individuals with T1D represented only 2.8% (n = 84), and the review excluded patients with diabetes under 18, a demographic where T1D is prevalent. Moreover, this review was unable to differentiate the outcomes between T1D and T2D, which is crucial due to their distinct pathophysiologies, treatment modalities, and potential responses to interventions. Consequently, there remains a gap in the literature regarding quantitative review studies on T1D. To address this gap, the current meta-analysis updates the evidence up to 30 November 2023, incorporating ten studies covering children, adolescents, and adults and employing a more comprehensive set of outcome measures.
2. Materials and Methods
2.1. Data Sources and Literature Search
This meta-analysis was recorded in the International Prospective Register for Systematic Reviews (PROSPERO) under registration number CRD42023395896. The review adhered to the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [21], which can be found in Supplementary S1, and a comprehensive literature search was undertaken by two independent researchers across seven databases, namely PubMed, Web of Science, Embase, Cochrane Library, National Knowledge Infrastructure (CNKI), WeiPu (VIP), and WanFang Data (WanFang), until 30 November 2023. Published reviews and their references were also manually searched to identify any additional studies meeting the inclusion criteria. A combination of MeSH terms and free text were utilized, encompassing terms such as ‘type 1 diabetes’, ‘probiotics’, ‘synbiotics’, and ‘randomized controlled trials’. Boolean operators were employed for sensitivity (‘OR’) and precision (‘AND’), customized to the syntax of each individual database. As an example, the search methodology applied in PubMed was structured as (‘Diabetes Mellitus, Type 1’[Majr]) AND (‘Probiotics’[Majr] OR ‘Prebiotics’[Majr] OR ‘inulin’[Majr] OR ‘bifidobacterium’[Majr] OR ‘lactoccocus’[Majr] OR ‘butyrate’[Majr]) with a clinical trial filter. The details of the search methodologies employed are provided in Supplementary S2.
2.2. Inclusion and Exclusion Criteria
A study was included if the following criteria were met: (1) RCT; (2) the literature was published before 30 November 2023; (3) the subjects must be diagnosed specifically with T1D; notably, no specific criteria were set for participants’ age or disease duration, aiming to encompass a broad spectrum of eligible studies; (4) interventions were limited to probiotics, synbiotics, prebiotics, and postbiotics with no requirement on duration; and (5) the primary outcome was HbA1c, and the secondary outcomes were FBG, FCP, DIU, C-reactive protein (CRP), interleukin-10 (IL-10), tumor necrosis factor-α (TNF-α), high-density lipoprotein (HDL), low-density lipoprotein (LDL), and Shannon index.
The exclusion criteria were as follows: (1) the subjects had other types of disease; (2) the probiotics were taken within three months before the trial; and (3) duplicate studies.
2.3. Selection and Data Extraction Process
Rayyan is a screening tool used for systematic reviews and meta-analyses, facilitating the efficient selection and management of relevant studies [22], and was employed in this review. During the initial round of title and abstract screening, both reviewers independently assessed all 831 records. Subsequently, in the second phase of full-text screening, a panel of two reviewers collectively evaluated the articles. Any disparities or disagreements that emerged during this process were addressed through collaborative discussion between the two reviewers, persisting until unanimous agreements were reached.
Two authors conducted data extraction independently, encompassing key aspects including (1) first author, publication year, and study country; (2) study design and intervention duration; (3) comprehensive details regarding the intervention and placebo, including specific probiotic strain, dosage, and daily intake time; (4) baseline characteristics like age, disease duration, and body mass index (BMI); and (5) metabolic outcomes, which were measured both before and after interventions. The extracted data underwent a verification process by both authors. In instances where data were not explicitly presented in the publications, the data analyst sought information in Supplementary Materials. If the necessary details remained elusive, the corresponding authors were contacted via email to solicit the missing data. A systematic follow-up protocol was implemented: After the initial contact, a one-week interval was allowed for a response. If no reply was received, a second contact attempt was made. In the event of continued non-response after the second attempt, the study was excluded from the analysis.
2.4. Quality Assessment
The quality assessment of each RCT was independently conducted by two reviewers utilizing the Cochrane risk-of-bias tool (ROB2) [23]. Additionally, the ROBVIS tool [24] was employed for visualization purposes. Adhering to the ROB2 guidelines, the following biases were systematically assessed: (1) bias arising from the randomization process; (2) bias due to deviations from intended interventions; (3) bias due to missing outcome data; (4) bias in the measurement of the outcome; and (5) bias in the selection of the reported result. The tool automatically synthesized the overall risk of bias, represented as low risk in green, some concerns in yellow, and high risk in red. Any disparities in the assessment were meticulously resolved through collaborative discussions between the two reviewers, persisting until consensus was achieved. The overall certainty of evidence across the studies was graded according to the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) working group guidelines. The quality of evidence was classified into four categories, namely high, moderate, low, and very low, according to the corresponding evaluation criteria.
2.5. Data Synthesis and Statistical Analyses
For the synthesis and quantitative analysis of data, Review Manager (Revman) 5.3 software was employed in this study. Continuous data were presented as the mean difference with standard deviation (m ± SD). In cases where data were initially expressed as median with interquartile range (IQR) or range, the skewness was assessed using the website (www.math.hkbu.edu.hk, accessed on 1 April 2024) [25,26]. If the data were not significantly skewed, transformation into mean with SD was undertaken. The standardized mean difference (SMD) with 95% confidence intervals (CIs) was calculated using random-effect models. In random-effect models, the treatment effect estimates observed in studies may vary due to genuine disparities in treatment effects across each study, along with sampling variability. This diversity in treatment effects could be attributed to discrepancies in study populations (e.g., patient age), interventions administered (e.g., drug dosage), duration of follow-up, and other variables. Thus, a random-effect model was utilized by facilitating the extension of findings beyond the included studies by assuming that these studies represented random samples from a broader population. Statistical significance was established at p < 0.05. Heterogeneity was evaluated through I2, and I2 values of 25%, 50%, and 75% were suggested to be indicators of low, moderate, and high heterogeneity, respectively [27]. Sensitivity analyses were performed for results displaying high heterogeneity to assess whether the combined outcomes and heterogeneity altered, aiming to evaluate the robustness of the findings. Subgroup analyses were further performed based on the different MMAs used, age, disease duration, and intervention duration differences. In cases where more than 10 studies were included, potential publication bias was investigated utilizing funnel plots [28].
3. Results
3.1. Literature Search Results
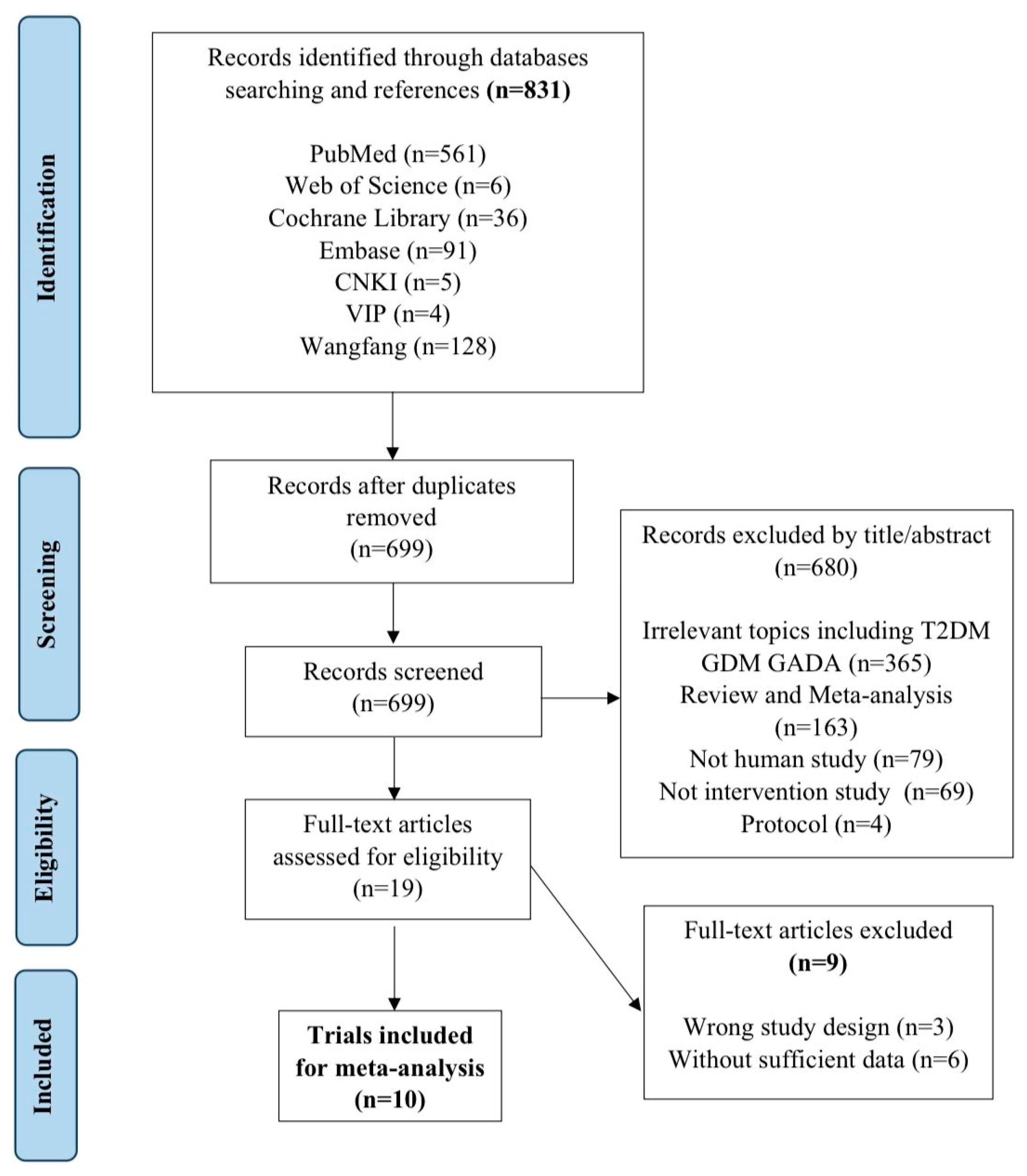
This review initially identified 831 records, of which 132 were excluded due to duplication. During the process of screening titles and abstracts, 680 studies were eliminated, primarily on the basis of irrelevant diseases, including type 2 diabetes (T2D), gestational diabetes mellitus (GDM), and latent autoimmune diabetes in adults (LADA); non-human studies including in vivo and in vitro studies; non-interventional studies, such as cross-sectional, cohort, and case–control studies; and reviews and protocols. In total, 19 full articles were reviewed for eligibility, and eventually, 10 clinical trials were included with 630 patients’ records in this meta-analysis (Figure 1). The exclusion reasons for the other nine articles are indicated in Supplementary S2.
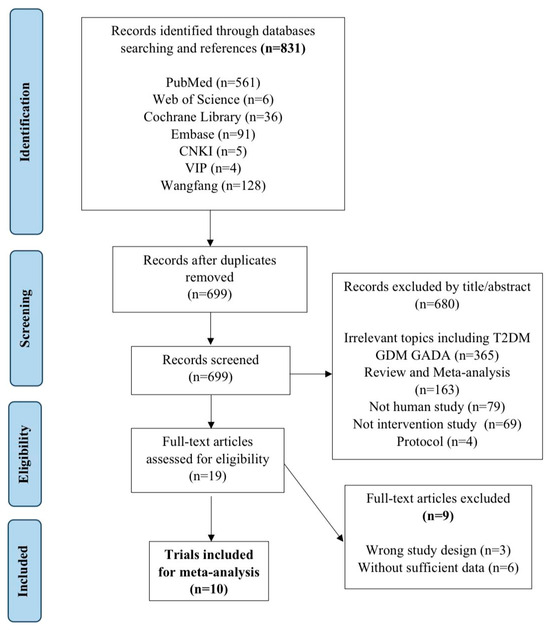
Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
3.2. Basic Characteristics of the Included Studies
Table 1 Summarizes essential data from the 10 included RCTs. One trial included children with three age groups [29]. Thus, each age group was considered as an individual report, and 12 subgroups were obtained eventually. A total of 630 participants (315 in the intervention group and 315 in the control group) underwent re-analysis. All clinical trials included both genders, maintaining a balanced male-to-female ratio (1.02).
Regarding interventions, one study used a prebiotic (inulin) [13], two studies used a postbiotic (sodium butyrate) [30,31], one study used a single-strain probiotic (Lactobacillus rhamnosus GG) [32], and six used multistrain probiotic or synbiotic supplements [29,33,34,35,36,37]. To maximize inclusivity, eligibility criteria did not impose restrictions based on age or the duration of T1D. Planned subgroup analyses considered age differences and disease duration. Mean participant age ranged from 5.5 to 56 years, and T1D duration ranged from 1.5 to 30 years. Six studies implemented MMA supplementation for 3 months [30,31,32,33,35], with one study using less than 3 months [34] and three studies exceeding 3 months [29,34,37]. Beyond post-intervention assessments, three studies also measured outcomes 3 months and 6 months after intervention completion [15,34,37]. None of the trials reported any significant adverse events in the MMA intervention group.

Table 1.
Characteristics of 10 RCTs that investigated the effect of MMAs on T1D.
Table 1.
Characteristics of 10 RCTs that investigated the effect of MMAs on T1D.
| Author/Year | Country | Sample Size | Age † | T1D Duration (Year) | Intervention; Control | Dose | Follow-Up | Main Measured Biomarkers |
|---|---|---|---|---|---|---|---|---|
| Bianchini et al., 2020 [30] | Italy | Probiotic: 34 | 13.4 (4.67) | NA | Probiotic drop: Lactobacillus rhamnosus GG | 5 × 109 LGG/drops, BID | 3 mo | HbA1c |
| Control: 30 | 13.1 (4.7) | Placebo drop: with a similar formulation but not containing probiotic | 5 drops, BID | |||||
| Groele et al., 2021 [37] | Poland | Probiotic: 48 | 12.3 (2.13) | <2 months | Multistrain probiotic capsule: L. rhamnosus GG ATCC 53103 and B. lactis Bb12 DSM 15954 | 109 CFU/capsule, QD | 6 mo; 6 mo AI | HbA1c, AUCC-peptide, FCP, DIU, IL-10, TNF-α |
| Control: 48 | 13.17 (2.59) | Placebo capsule: maltodextrin | 1 capsule, QD | |||||
| Groot et al., 2020 [29] | The Netherlands | Postbiotic: 50 | 32.5 (22–61) ‡ | 8 (4–16) | Postbiotic capsule: sodium butyrate | 2 g/capsule, TID | 3 mo | HbA1c, DIU, FCP, CRP, LDL, Fecal SCFA |
| Control: 50 | 32.5 (22–61) ‡ | Placebo capsule | 2 g/capsule, TID | |||||
| Ho et al., 2019 [15] | Canada | Prebiotic: 17 | 12.52 (2.76) | 7.31 (3.93) | Prebiotic capsule: oligofructose enriched inulin (chicory root-derived) | 8 g/capsule, QD | 3 mo; 3 mo AI | HbA1c, FCP, gut microbiota |
| Control: 21 | 11.94 (2.61) | 4.70 (3.07) | Placebo capsule: maltodextrin | 3.3 g/capsule, QD | ||||
| Javid et al., 2020 [36] | Iran | Synbiotic: 22 | 10.36 (2.53) | 4.45 (1.96) | Synbiotic powder: Lactobacillus sporogenes GBI-30, maltodextrin, and fructooligosaccharide | 2 g powder (109 CFU), QD | 2 mo | HbA1c, FBG, FCP, DIU, HDL, LDL, CRP |
| Control: 22 | 10.04 (2.08) | 4.04 (1.36) | Placebo powder: starch | 2 g powder, QD | ||||
| Kumar et al., 2021 [33] | India | Probiotic: 47 | 7.92 (3.92) | <2 months | Multistrain probiotic capsule: L. paracasei DSM 24733, L. plantarum DSM 24730, L. acidophilus DSM 24735, and L. delbrueckii subsp. bulgaricus DSM 24734, B. longum DSM 24736, B. infantis DSM 24737, B. breve DSM 24732, and Streptococcus thermophilus DSM 24731 | 1.125 × 1011 bacteria/capsule, QD | 3 mo | HbA1c, FBG, FCP, DIU |
| Control: 49 | 9.1 (4.95) | <2 months | Placebo capsule: microcrystalline cellulose | 1 capsule, QD | ||||
| Lin et al., 2021 [29] | China | Probiotic: 35 | 1–15 (3 age groups) | >1 year | Multistrain probiotic capsule: Bifidobacterium longum, Lactobacterium bulagricumi, and Streptococcus thermophilus | 4.2 × 107 CFU/capsule, 2–4 TID (based on age) | 6 mo | HbA1c, FCP, DIU CD4+/CD8+ |
| Control: 35 | Placebo: insulin therapy | |||||||
| Tougaard et al., 2022 [30] | Finland | Postbiotic: 28 | 56 (11) | 29 (17) | Postbiotic granules: sodium butyrate | 1.8 g, TID | 3 mo | HbA1c, fecal SCFA |
| Control: 25 | 52 (15) | 32 (14) | Placebo capsule: microcrystalline cellulose | QD | ||||
| Wang et al., 2022 [34] | Taiwan, China | Probiotic: 27 | 14.1 (5.1) | 6.2 (4.5) | Multistrain probiotic capsule: 1:1 mixture ratio of Lactobacillus salivarius subsp. salicinius AP-32, L. johnsonii MH-68, and Bifidobacterium animalis subsp. lactis CP-9 | 5 × 109 CFU/capsule, QD | 6 mo; 3 mo AI | HbA1c, FBG, TNF-α, gut microbiota |
| Control: 29 | 14.3 (4.6) | 6.4 (4.1) | Placebo: insulin therapy | |||||
| Zhang et al., 2023 [35] | China | Probiotic: 27 | 38 (14) | 10 (4, 16) | Multistrain probiotic capsule: Bifidobacterium longum, Lactobacterium bulagricumi, and Streptococcus thermophilus | 4.2 × 107 CFU/capsule, TID | 3 mo | HbA1c, FBG, FCP, DIU, LDL, HDL CGM |
| Control: 23 | 39 (8) | 10 (7, 16) | Placebo capsule: same substances but without the bacteria | 1 capsule, TID |
† Note: normally distributed quantitative variables are presented as the mean ± SD. ‡ Non-normally distributed quantitative variables are presented as the median (interquartile range, IQR). Functional abbreviations: CFU, colony forming unit; QD, once a day; TID, three times a day; CGM, continuous glucose monitoring; mo, months; AI, after intervention, meaning the study included a follow-up for a period of time when intervention completed. Study outcome abbreviations: HbA1c, glycated hemoglobin; AUCC-peptide, area under the curve of the C-peptide level during 2 h responses to a mixed meal; FCP, fasting C-peptide; DIU, daily insulin usage; TNF-α, tumor necrosis factor-α; FBG, fasting blood glucose; SCFA, short-chain fatty acid; CRP, C-reactive protein; HDL, high-density lipoprotein; LDL, low-density lipoprotein; NA, Data not applicable; BID, twice a day.
3.3. Risk-of-Bias Assessment
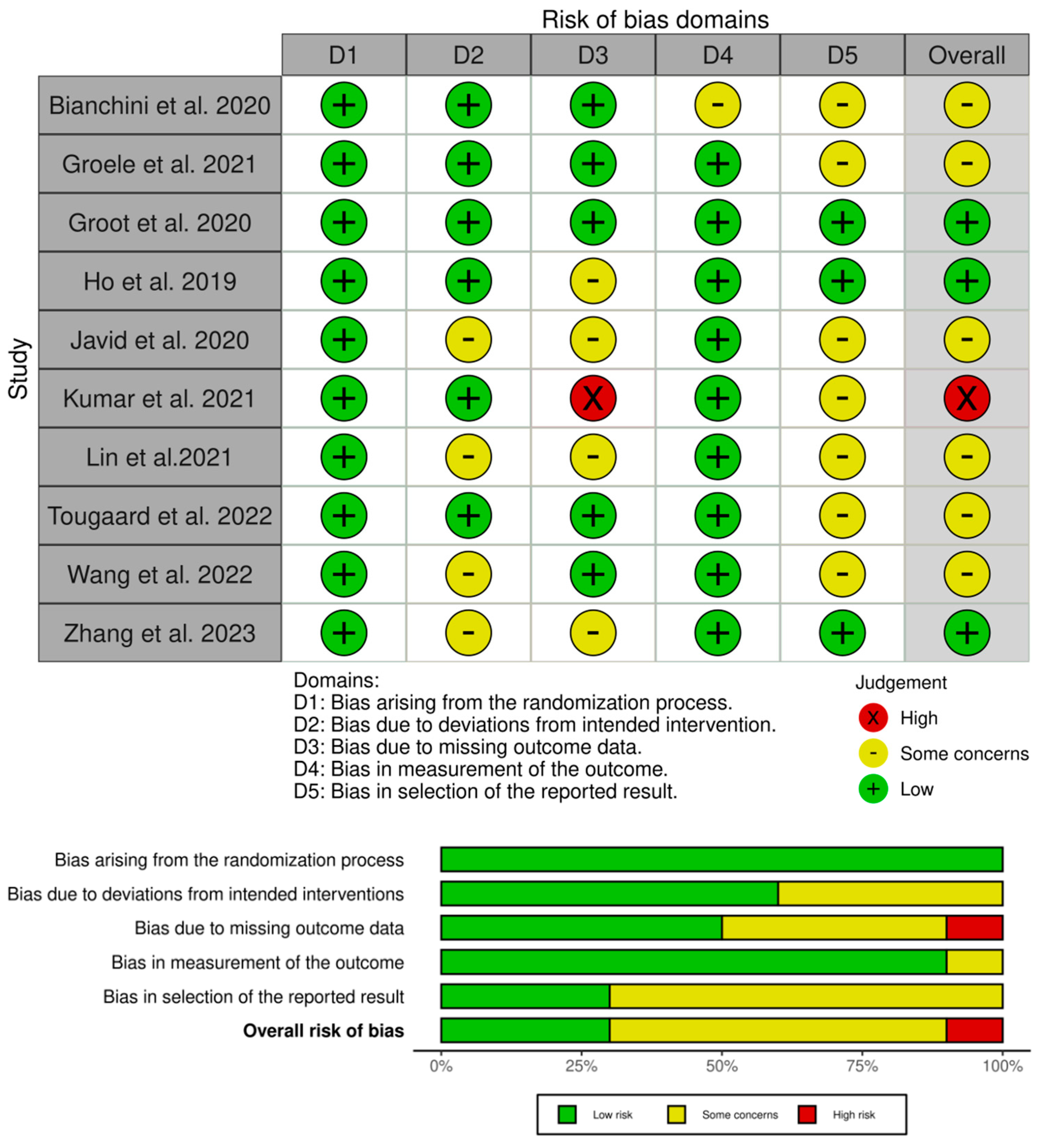
The results of Cochrane’s risk-of-bias assessment in Figure 2 show that the overall risk of bias was of some concern. All studies described the generation of random sequences in detail, six studies reported proper allocation concealment [15,30,31,32,33,37], and six studies demonstrated the integrity of data [15,30,31,32,34,37]. One study had incomplete results due to missing data [32]. In seven studies, it was unclear whether there was reporting bias [29,30,32,33,34,36,37].
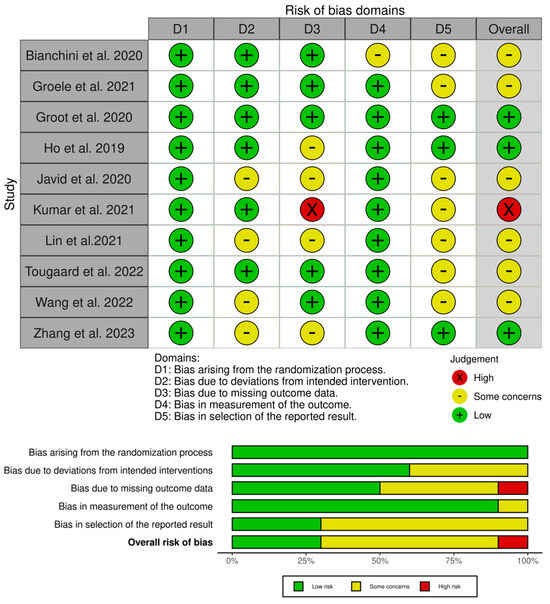
Figure 2.
Risk-of-bias assessment for the included 10 studies [15,29,30,31,32,33,34,35,36,37].
3.4. Meta-Analysis Results
3.4.1. Effects of MMA Intervention on HbA1c
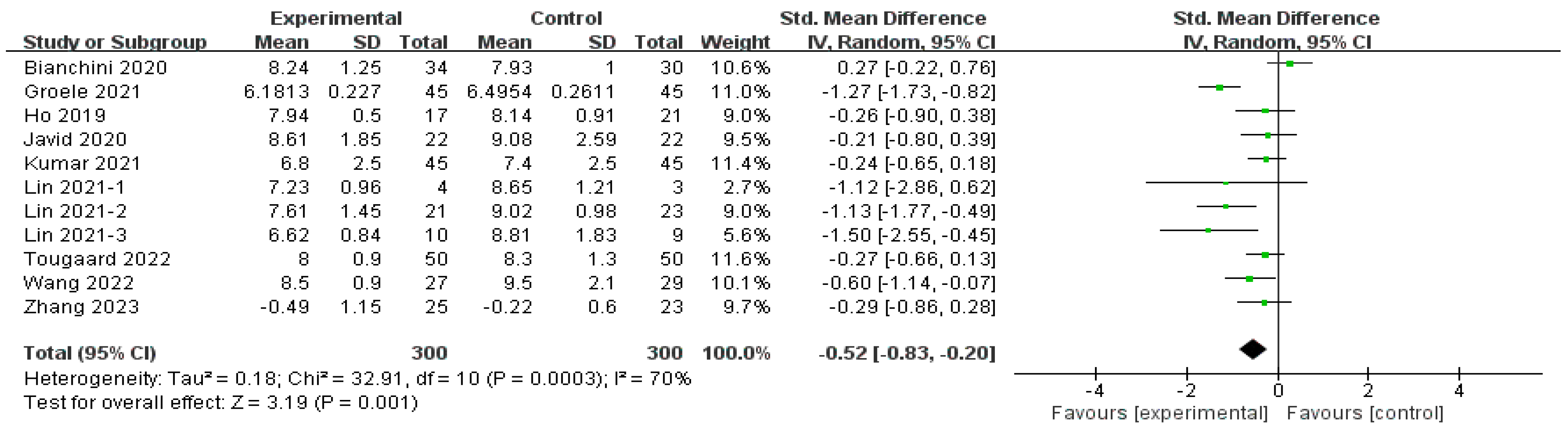
The effect of MMAs on HbA1c was reported by 10 studies (n = 600) [29,30,32,33,34,36,37], as depicted in Figure 3. The overall effect (SMD = −0.52, 95% CI [−0.83, −0.20], p < 0.01) indicated a significant improvement in HbA1c with MMA intervention but with moderate heterogeneity (I2 = 70%, p < 0.01, Tau2 = 0.18). The sensitivity analysis revealed that the omission of any single study did not significantly alter the result. Subgroup analyses were conducted based on four parameters, namely the duration of intervention, the MMAs used, age, and the disease duration of the T1D patients, which are discussed in Section 3.4.5.
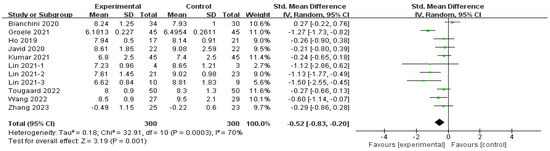
Figure 3.
Forest plot of the effect of MMA intervention on HbA1c [15,29,30,31,32,33,34,35,36,37].
3.4.2. The Effect of MMA Intervention on Daily Insulin Usage
The effect of MMAs on DIU was reported by three studies with five subgroups (n = 250) [29,33,37] and a significant decrease in usage was found (SMD = −0.41, 95% CI [−0.76, −0.07], p = 0.02); the heterogeneity was moderate (I2 = 35%, p = 0.19, Tau2 = 0.05) (Figure 4).

Figure 4.
Forest plot of the effect of MMA intervention on daily insulin usage [29,33,37].
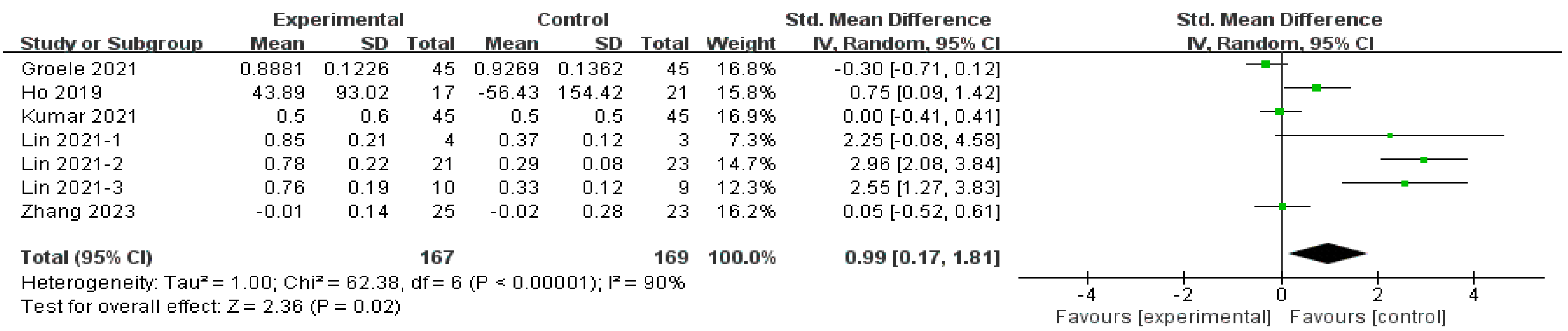
3.4.3. The Effect of MMA Intervention on Fasting C-Peptide
The effect of MMAs on FCP was reported by five studies with seven subgroups (n = 336) [15,29,33,35,37], and the reports indicated a significant improvement (SMD = 0.99, 95% CI [0.17, 1.81], p = 0.02) (Figure 5). Sensitivity analysis was performed due to high heterogeneity (I2 = 90%, p = 0.01, Tau2 = 1.00). The omission of any single study or subgroup did not significantly alter the result; thus, subgroup analyses were performed.
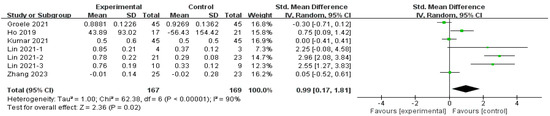
Figure 5.
Forest plot of the effect of MMA intervention on fasting C-peptide [15,29,33,35,37].
3.4.4. The Effect of MMA Intervention on Other Results
FBG was reported in three studies (n = 154) [34,35,36], and the result was not significant (SMD = −0.29, 95% CI [−0.62, 0.03], p = 0.08). CRP was reported in three studies (n = 192) [30,35,36], and the result was not significant (SMD = −0.25, 95% CI [−0.84, 0.33], p = 0.40). TNF-α was reported in three studies (n = 184) [13,32,35], and the result was not significant (SMD = −0.03, 95% CI [−0.58, 0.52], p = 0.91). IL−10 was reported in two studies (n = 128) [15,37], and the result was not significant (SMD = 0.31, 95% CI [−0.04, 0.66], p = 0.08). There were two studies (n = 92) that investigated HDL (SMD = 0.27, 95% CI [−0.25, 0.80], p = 0.31) and LDL (SMD = −0.23, 95% CI [−0.98, 0.51], p = 0.54), and both results were insignificant [35,36]. The Shannon index was reported in two studies (n = 68) [15,31], and there was no difference (SMD = −0.66; 95% CI [−1.62, 0.30], p = 0.18). All the results above are shown in Supplementary S3. Regarding adverse events, none of the included studies reported any occurrences.
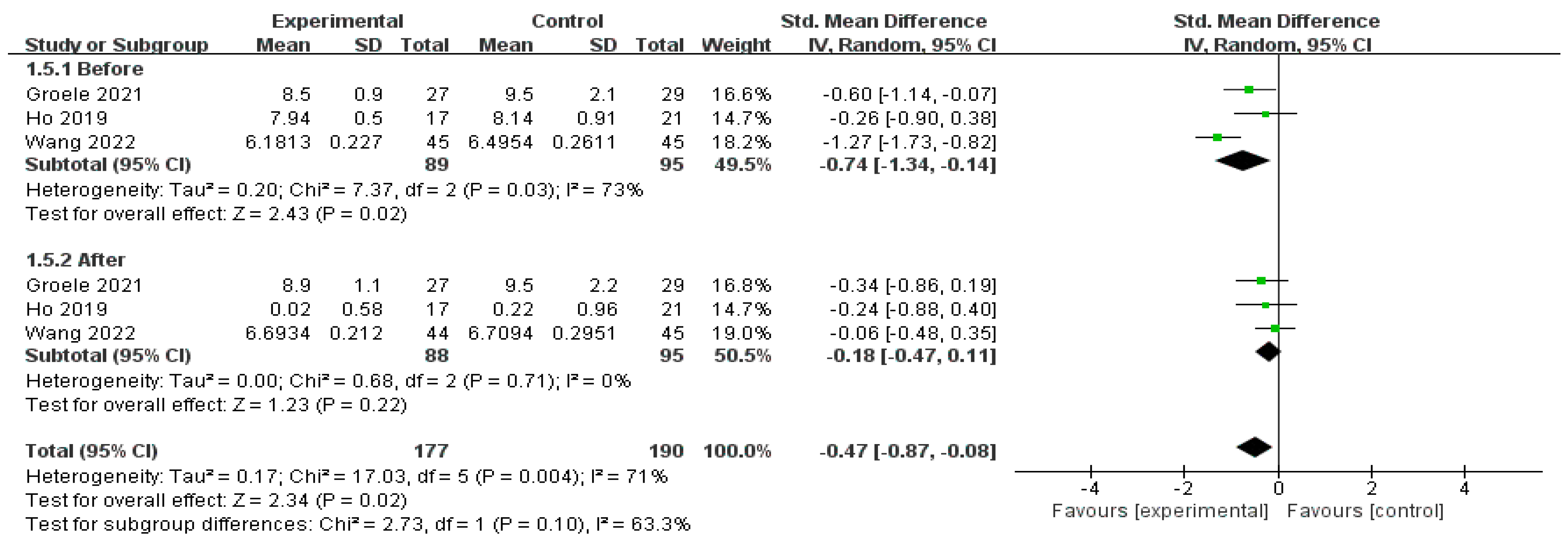
The efficacy of MMAs as evidenced by the post-interventional results of HbA1c was reported by three studies (n = 367) [15,34,37]. After aggregating the outcome at the end of the intervention (SMD = −0.74, 95% CI [−1.34, −0.41], p = 0.02), and after 3 months (SMD = −0.18, 95% CI [−0.47, 0.11], p = 0.22), a diminished effect was observed, as shown in Figure 6.
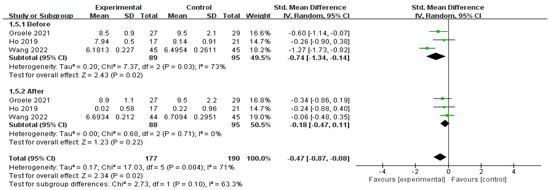
Figure 6.
Forest plot of the effect of MMA intervention on HbA1c post-intervention [15,34,37].
3.4.5. Subgroup Analysis
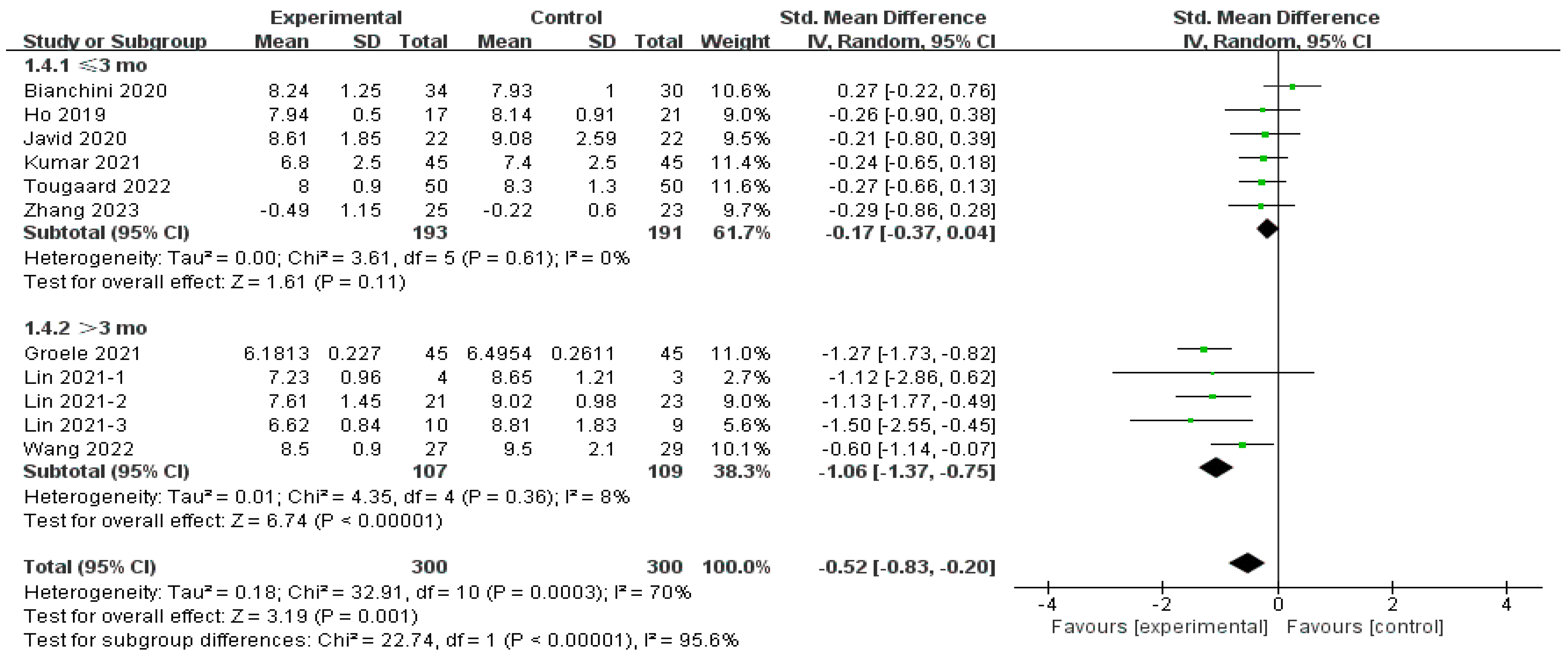
Influence of Intervention Duration on HbA1c
The subgroup analysis involving the intervention duration demonstrated a considerable impact in the subgroup of more than 3 months (SMD = −1.06, 95% CI [−1.37, −0.75], p < 0.01) [29,34,37] and an insignificant effect in the other subgroup (SMD = −0.17, 95% CI [−0.37, 0.04], p = 0.11) [15,30,32,33,34,36], as shown in Figure 7. Heterogeneity rates in both subgroups were low (8% for more than 3 months, and 0% for equal or less than 3 months), and the test for subgroup differences indicated a statistically significant effect (Chi2 = 22.74, df = 1 (p < 0.001), I2 = 95.6%).
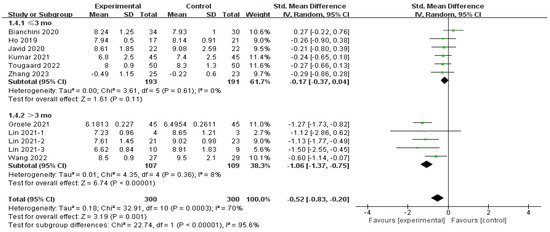
Figure 7.
Subgroup analysis of the effect of different intervention durations on HbA1c [15,29,30,32,33,34,35,36,37].
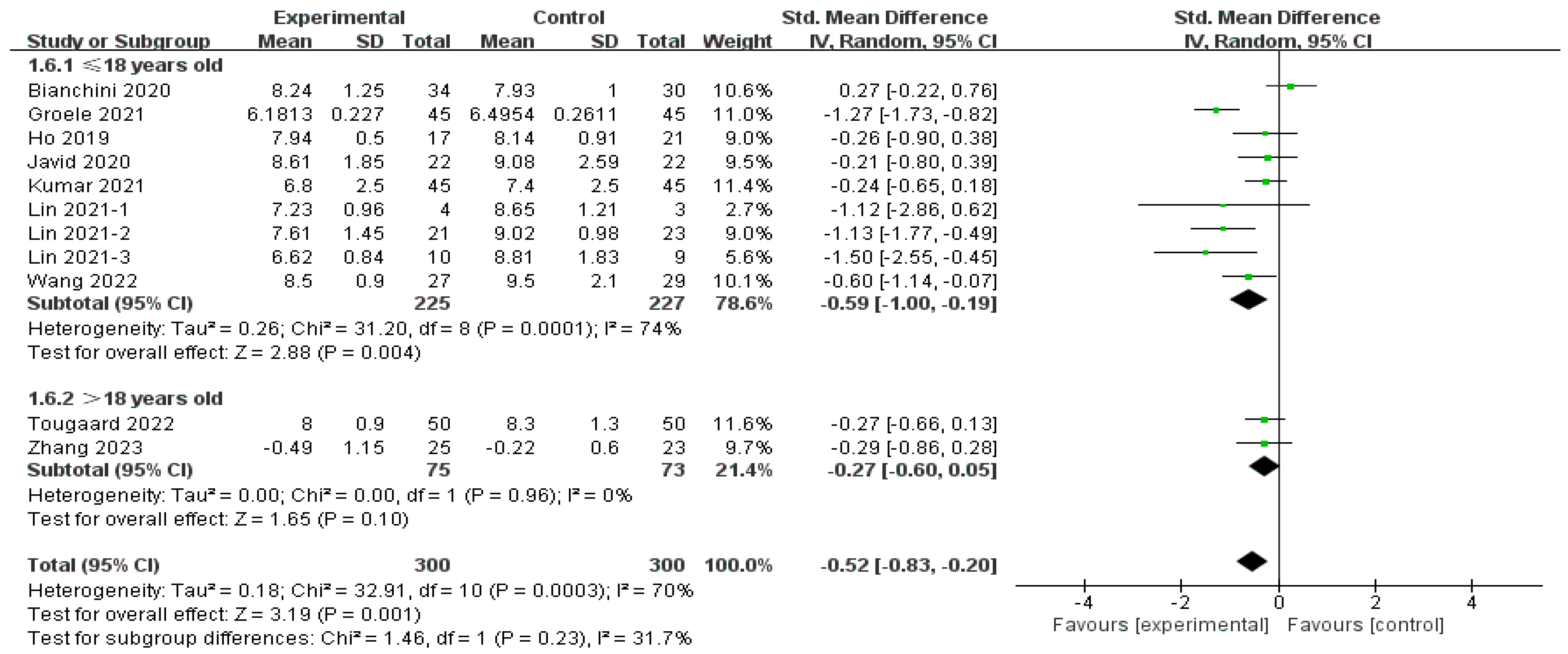
Influence of Age on HbA1c
Subgroup analysis involving age showed a significant effect (SMD = −0.59, 95% CI [−1.00, −0.19], p < 0.01) in the children and adolescent groups [15,29,32,33,36], whereas this was not observed in adults (SMD = −0.27, 95% CI [−0.60, 0.05], p = 0.10) [28,33], as shown in Figure 8. Heterogeneity was considerable in the children subgroup (I2 = 74%), and very low among adults (I2 = 0%). In addition, there was no significant difference between these two subgroups (Chi2 = 1.46, df = 1 (p = 0.23), I2 = 31.7%).
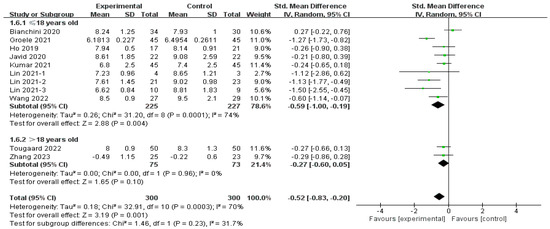
Figure 8.
Subgroup analysis of the effect of age on HbA1c [15,29,30,32,33,34,35,36,37].
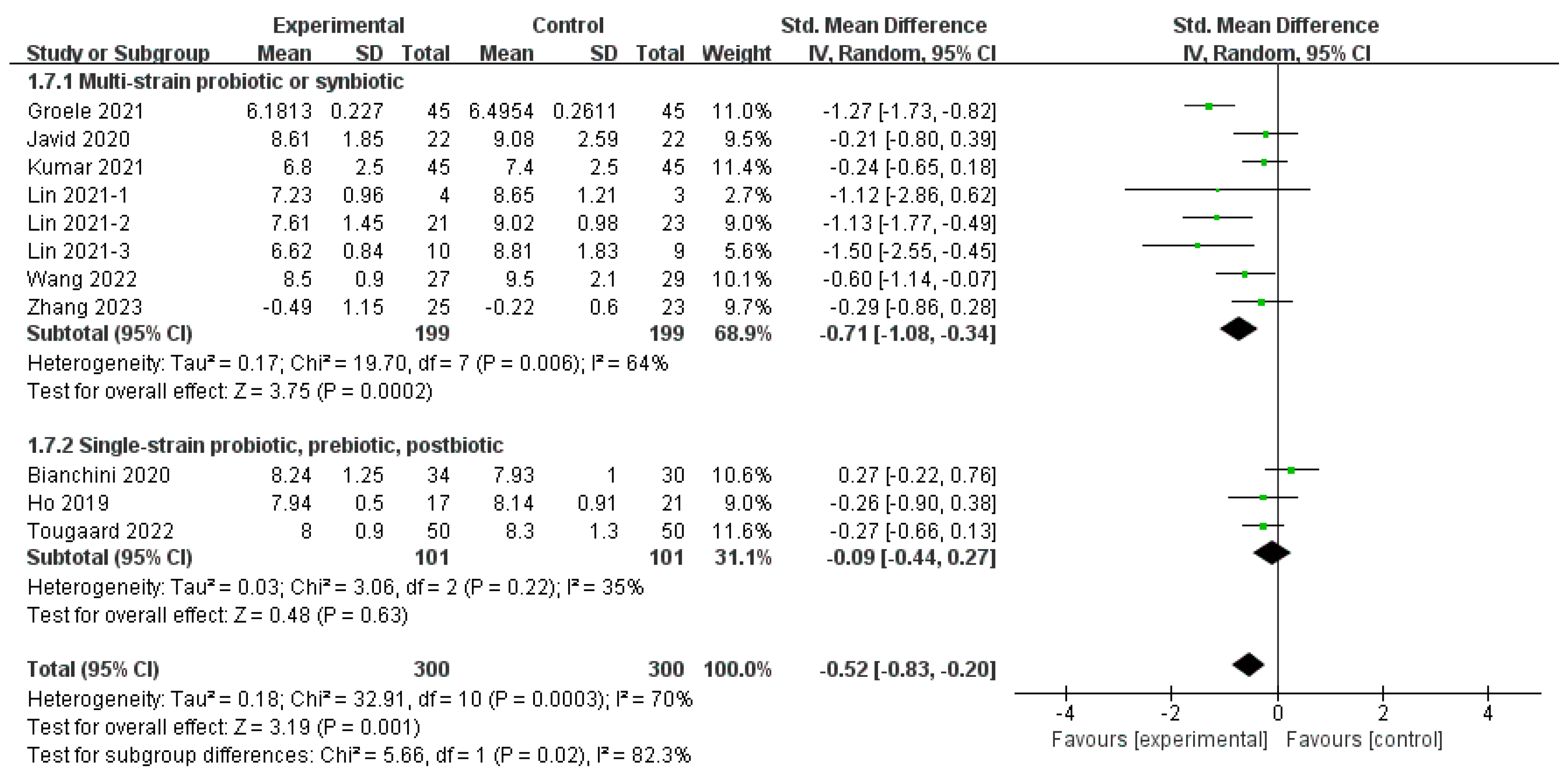
Influence of Different MMAs on HbA1c
The subgroup analysis involving different MMAs revealed a distinct pattern between subgroups (Chi2 = 5.66, df = 1 (p = 0.02), I2 = 82.3%), as shown in Figure 5. The intention was to group each MMA, but studies on single-strain probiotics [32], prebiotics [15], and postbiotics [30] only involved one group, not allowing for separate grouping; thus, two subgroups were established. Studies on multistrain probiotics and synbiotics [29,33,34,35,36,37] revealed significant effects (SMD = −0.71, 95% CI [−1.08, −0.34], p < 0.01), whereas an insignificant improvement was found in another subgroup (SMD = −0.09, 95% CI [−0.44, 0.27], p = 0.63) (Figure 9). Heterogeneity was considerable in the multispecies subgroup (I2 = 35) and not significant in the monospecies subgroup (I2 = 35%).
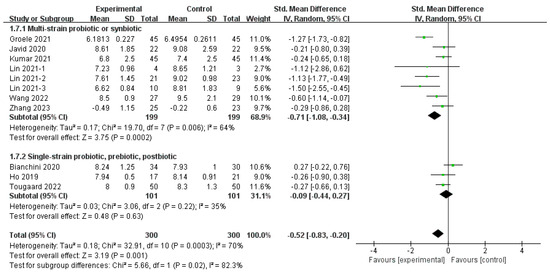
Figure 9.
Subgroup analysis of the effect of different MMAs on HbA1c [15,29,30,32,33,34,35,36,37].
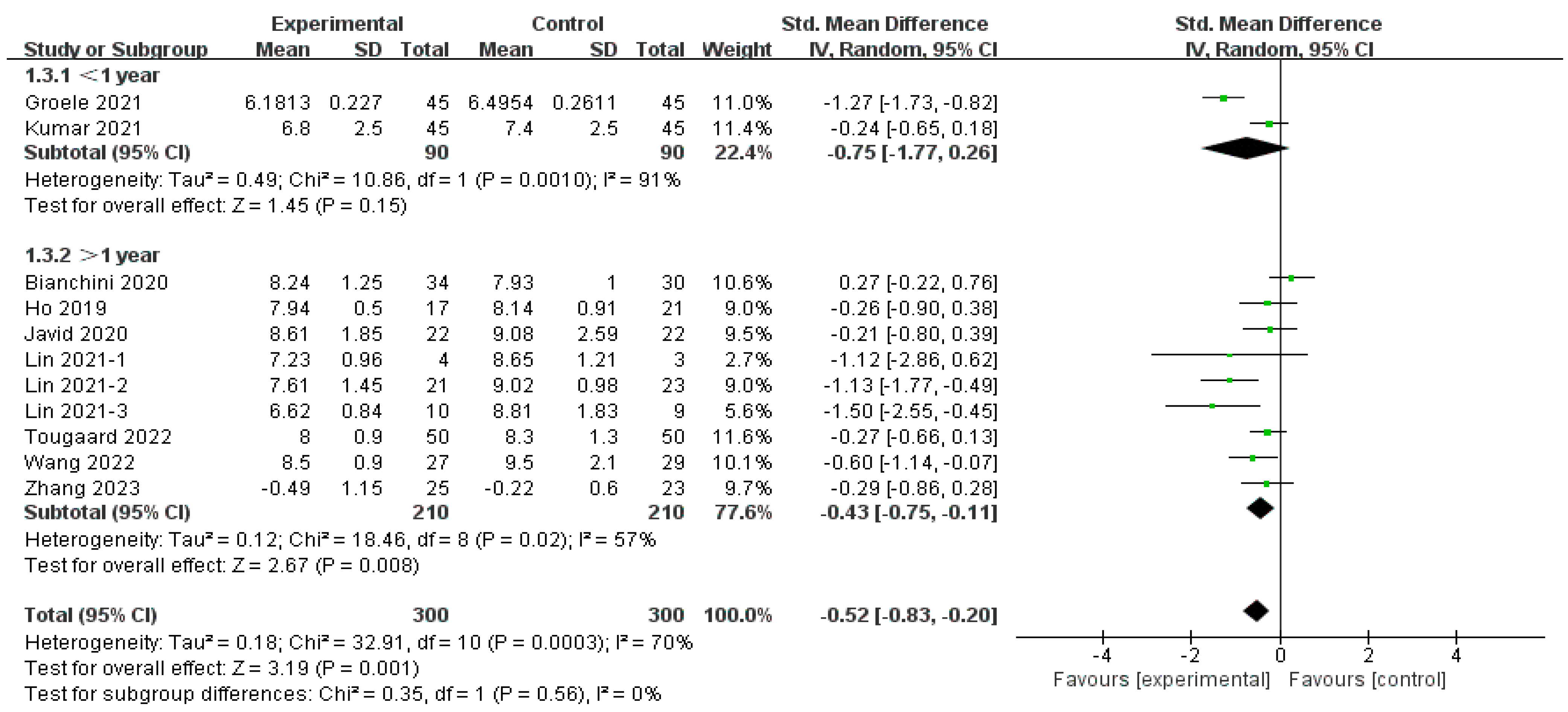
Influence of Disease Duration of MMAs on HbA1c
Subgroup analysis by disease duration showed a significant improvement in long-term T1D (SMD = −0.43, 95% CI [−0.75, −0.11], p < 0.01) [29,33,34,35,36,37] and an insignificant effect on onset T1D (SMD = −0.75, 95% CI [−1.77, 0.26], p = 0.15) [33,37], as depicted in Figure 10. Heterogeneity was considerable in the onset-T1D subgroup (I2 = 91%) and moderate in the long-term-T1D subgroup (I2 = 35%). Additionally, an in-between difference was not observed in these two subgroups (Chi2 = 0.35, df = 1 (p = 0.56), I2 = 0%).
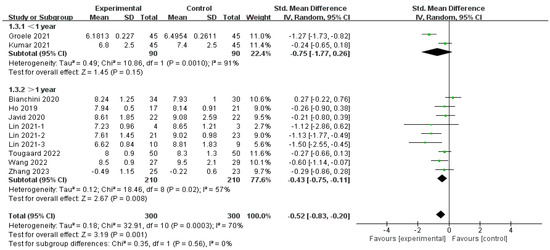
Figure 10.
Subgroup analysis of the effect of disease duration on HbA1c [15,29,30,32,33,34,35,36,37].
Influence of Age, MMAs, and Disease Duration on Fasting C-Peptide
Subgroup analyses involving FCP are presented in Supplementary S4. One study included participants more than 18 years old and showed no effect (SMD = 0.05, 95% CI [−0.52, 0.61], p = 0.88); individuals with an age less than or equal to 18 years showed a significant improvement (SMD = 1.21, 95% CI [0.20, 2.21], p = 0.02). The results of multistrain probiotics and synbiotics showed a significant improvement in FCP (SMD = 1.06, 95% CI [0.09, 2.02], p = 0.03). The other group contained one study and indicated an improvement (SMD = 0.75, 95% CI [0.09, 1.42], p = 0.03). There was no significant improvement among individuals with disease duration less than or equal to 1 year (SMD = −0.15, 95% CI [−0.44, 0.15], p = 0.32), whereas significant improvement was observed among individuals with disease duration more than 1 year (SMD = 1.61, 95% CI [0.37, 2.86], p = 0.01).
3.5. Publication Bias
Publication bias was assessed for HbA1c since it was the only biomarker that exceeded 10 studies and subgroups. The plot shows a concentrated distribution of all studies, suggesting an absence of publication bias (Supplementary S3).
3.6. Grading of Evidence
An evaluation of the quality of evidence using the GRADE approach is presented in Table 2. The quality of evidence was moderate for HbA1c due to inconsistency (I2 = 70%), low quality for FCP, and very low quality for DIU, owing to limitations on imprecision (n = 336 and n = 250 for sample size, respectively), as well as limitations on inconsistency for FCP (I2 = 90%) and risk of bias in DIU and publication bias (two studies had an overall uncertain risk, and one was with high risk of bias).
Table 2.
GRADE profile of MMAs for glycemic indices.
4. Discussion
This systematic review and meta-analysis focused on probiotics, prebiotics, synbiotics, and postbiotics as adjuvant therapy in T1D management. With the inclusion of 10 clinical trials, comprising a sample size of 630 T1D patients, significant improvements were observed in HbA1c, FCP, and DIU, while no effects were found in FBG, CRP, TNF-α, IL-10, HDL, LDL, and the Shannon index. Subgroup analyses based on HbA1c revealed the effects of the intervention period, types of MMAs, age, and the disease duration of the patients. A considerable effect on HbA1c was found in the subgroup receiving multistrain probiotics or synbiotics, a supplementation period for more than 3 months, and in patients under 18 years old with long-term T1D. The grading of the quality of evidence indicated moderate quality of evidence in HbA1c and low/very low quality of evidence in FCP and DIU.
Comprising roughly 1000 species and weighing approximately 1.5 kg, the gut microbiota is integral to human health, and alterations in its composition, known as dysbiosis, have been implicated in the pathogenesis of T1D [38]. The gut microbiome composition was different in healthy versus TID in both human and animal models [39]. Animal studies indicated higher alpha-diversity in the gut microbiota of non-obese diabetic (NOD) mice compared with mice that later progressed to T1D [40], and in mice with reduced T1D progression, a higher Bacteroidetes-to-Firmicutes ratio was observed [41]. Similar to animal models, case–control studies indicated a significantly lower Bacteroidetes-to-Firmicutes ratio in the T1D group [7,8]. The “Teddy study (The Environmental Determinants of Diabetes in the Young)” showed a lower abundance of Streptococcus thermophilus and Lactococcus lactis in children at the onset of T1D with respect to healthy subjects [42]. In addition, children with T1D were observed with decreased numbers of bacteria that were essential to maintain gut integrity such as lactic acid-producing bacteria, butyrate-producing bacteria, and mucin-degrading bacteria. Aberrant gut microbiota composition might play a pivotal role in the development of T1D mainly by modulating the formation of SCFA [43], compromising the gut barrier by loosening the tight junction between cells, allowing pathogenic substances such as TNF-α to enter the bloodstream, and triggering autoimmune responses underlying T1D [44].
The modulation of the gut microbiota is a strategy aiming at reversing dysbiosis by using different types of MMAs [45]. Single-strain probiotics, multistrain probiotics, synbiotics, prebiotics, and postbiotics were included in this review, with multistrain probiotics appearing to exert a greater efficacy, aligning with the literature [46]. Treating NOD mice with probiotic strains belonging to families Bifidobacteriaceae and Lactobacillaceae and the Streptococcus thermophilus genus has been shown to ameliorate T1D [47]. The mechanism of action might be through the downregulation of the proinflammatory TLR signaling pathway, which decreases the level of proinflammatory cytokines, including IL-6, IL-1β, and TNF-α while increasing that of anti-inflammatory cytokines, such as transforming growth factor-β (TGF-β) and IL-10 [48]. However, the quantitative analysis results on the Shannon index, CRP, TNF-α, IL-10, and IFN-γ revealed negative values, which might be attributed to the inability to stratify different MMAs, given the limited number of outcomes covering the same indicators, each with only two trials examined. They employed different MMAs (varied strains of multistrain probiotics, synbiotics, inulin, and sodium butyrate) targeting distinct mechanisms for gut modulation and T1D amelioration. In this review, one study showed an enriched composition of beneficial gut microbiota, including Bifidobacterium animalis, Lactobacillus salivarius, and Akkermansia muciniphila, and an improved level of TGF-β1 and TNF-α after supplementing with Lactobacillus salivarius and Bifidobacterium animalis [34]. This was aligned with an intervention study using Jinshuangqi (a triple live probiotic tablet sold in China consisting of Bifidobacterium longum, Lactobacterium bulagricumi, and Streptococcus thermophilus), indicating a decreased level of IFN-γ, Bifidobacterium, and Lactobacillus and a restored Th1/Th2 cell balance in children with T1D [49]. The use of synbiotics (a combination of probiotics and prebiotics) resulted in a significant increase in the levels of SCFAs, ketones, carbon disulfides, and methyl acetates, which was observed to have a greater efficacy on blood glycemic control and inflammation than probiotic usage alone [50,51]. One study in this review indicated a decreased CRP level and an increase in total antioxidant capacity [34].
Sodium butyrate is the most common type of postbiotic, indicating promising glycemic control in streptozotocin (STZ)-induced T1D mice by improving the islet morphology and downregulating the NF-κB-mediated inflammatory signal pathway [50]. In an antibiotic-driven T1D mice model, butyrate ameliorated disease in the female offspring of NOD mice, and in their formal study, butyrate directly shaped pancreatic immune tolerance and dampened T1D progression [51]. Nevertheless, human studies did not support any of these findings [28,29], nor an increase in fecal butyrate. Unlike inulin, a type of prebiotic derived from chicory increased SCFA and interleukin-22 potentially by preventing and/or treating T1D in NOD mice and mitigating symptoms among individuals with T2D through the inhibition of JNK and P38 MAPK pathways [52]. Clinical evidence demonstrated an improvement in gut integrity and higher relative abundance of Streptococcus, Roseburia inulinivorans, Terrisporobacter, and Faecalitalea with inulin supplementation in children with T1D [13]. This suggests that the oral intake of postbiotic metabolites from gut microbiota might not act directly and efficiently in promoting the intestinal environment like other supplementations.
Intervention duration and the characteristics of the T1D patients might also play important roles, as revealed in this meta-analysis. MMA intervention for over 3 months demonstrated a significant decrease in HbA1c levels. The between-group heterogeneity for different intervention periods significantly decreased (I2 = 0% for ≥3 months, I2 = 8% for >3 months), and the test for subgroup difference reached significance (I2 = 95.6%), indicating that variations in the intervention period might serve as a probable source of heterogeneity. Different types of MMAs might also be a source of heterogeneity, as indicated by the test in subgroup differences (I2 = 82.3%). MMA intervention might be more effective in lowering HbA1c in children and adolescents and those with long-term T1D. This could be attributed to the greater adaptability of children’s intestinal flora and the altered glucose metabolism in long-term T1D cases, indicating the increased efficacy of MMA intervention over time [53]. However, the subgroup difference tests revealed that age (I2 = 31.7%) and disease duration (and I2 = 0) might not be the source of heterogeneity.
Other potential sources of heterogeneity included dietary factors, physical activity, and the dose and form of MMAs. Only one RCT recorded the dietary factor at baseline and post-intervention, though it reported an unchanged effect after adjusting this confounding factor. The diet also plays a role as studies have shown that HbA1c is lower in patients following a diet with balanced-glycemic-index food [54]. Similarly, a moderate level of PA resulted in better glycemic control in T1D patients [55], but no trials included in this review reported any information on this factor. Lastly, the dose and form of MMAs used may contribute to heterogeneous results, but they are incomparable between different types of MMA, since the unit for probiotics is CFU, while it is gram in postbiotics and prebiotics. While the moderate heterogeneity aligned with the literature [20], the combined effect varied, which might be attributed to the differentiation between T1D and T2D. This review further demonstrated an improvement in DIU and FCP, contradicting the negative results from another review [19]. Furthermore, three studies conducted post-interventional biochemical examinations, revealing no significant difference between the MMA and control groups [15,34,37]. This transient effect aligned with another systematic review, indicating the absence of consistent effects on gut microbiota composition alterations after four to eight weeks of probiotic intervention, suggesting that individuals may require a longer duration of treatment to have therapeutic effects [56].
This is the first systematic review and meta-analysis exclusively focusing on the effect of MMAs and T1D and attempting to investigate inflammation and gut microbiota indicators in addition to glycemic control. However, it is not without limitations. Despite including more than twice the number of studies and sample size compared to previously published research [17,18], the number of ten RCTs was not sufficient for the extrapolation of the results. Meanwhile, even though most of the included studies presented a low or unclear risk of bias, the overall quality and reliability might be compromised due to unclear reporting and missing data. Unclear reporting in studies may lead to difficulties in assessing the true risk of bias, and missing data may result in attrition bias, which may skew the results and reduce the precision of the estimated effects. This review endeavored to quantitatively analyze the gut microbiota composition and inflammatory cytokines post-MMA interventions. However, due to variations in outcome measures, different properties, and targeted outcomes of MMAs, the scope of quantitative analysis was limited, raising the possibility that the insignificant effects on biomarkers other than HbA1c, FCP, and DIU may have been by chance. In addition, statistical heterogeneity was observed in the analyses, confounding factors such as ethnicity differences, dietary factors PA, dose, and form of the intervention were not analyzed in this review.
5. Conclusions
In conclusion, this systematic review and meta-analysis suggested that MMA supplementation is associated with improved HbA1c, DIU, and FCP, with moderate quality of evidence in HbA1c and low/very low quality of evidence in FCP and DIU. Multistrain probiotics and synbiotics might exhibit a more significant effect under long-term intervention (<3 months.) Despite the moderate-to-high heterogeneity found in HbA1c and FCP, the evidence supports the potential of MMAs as an adjuvant therapy for glycemic control. The study findings did not substantiate a favorable association between MMA intervention and FBG, CRP, TNF-α, IL-10, LDL, HDL, and the Shannon index, but this might be by chance due to the insufficient number of included studies. Further large-scale clinical trials are necessary to confirm these findings with investigations on inflammation and gut microbiota composition while adjusting confounding factors such as diet, physical activity, and the dose and form of MMA intervention.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/nu16111675/s1, Supplementary S1: PRISMA flow diagram. Supplementary S2: Details of searching strategy and screening process. Supplementary S3: Forest plots of the effects of MMA intervention on FBG, CRP, TNF-a, IL-10, HDL, LDL, and Shannon index. Supplementary S4: Forest plots of subgroup analysis of FCP. Refs. [57,58,59,60,61,62,63,64,65] are cited in Supplementary Materials.
Author Contributions
Conceptualization, Y.Z.; methodology, Y.Z. and A.H.; software, Y.Z.; validation, A.H. and J.L.; data curation, Y.Z.; writing—original draft preparation, Y.Z.; writing—review and editing, Y.Z., W.M., U.M.P.P., S.C. and L.Y.; visualization, Y.Z.; supervision, L.Y.; project administration, Y.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
The authors express great appreciation to all researchers who sought to conduct studies of T1D and would particularly like to thank all participants and their families in the included trials. The authors would also like to thank Xiaohong Zhang for providing original data and Professor Xinyin Wu and Yinyan Gao for providing professional help.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Boldison, J.; Wong, F.S. Immune and Pancreatic β Cell Interactions in Type 1 Diabetes. Trends Endocrinol. Metab. 2016, 27, 856–867. [Google Scholar] [CrossRef] [PubMed]
- Magliano, D.J.; Boyko, E.J.; IDA 10th Edition Scientific Committee. What is diabetes? In IDF DIABETES ATLAS [Internet], 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK581938/ (accessed on 2 March 2024).
- Ogle, G.D.; James, S.; Dabelea, D.; Pihoker, C.; Svennson, J.; Maniam, J.; Klatman, E.L.; Patterson, C.C. Global estimates of incidence of type 1 diabetes in children and adolescents: Results from the International Diabetes Federation Atlas, 10th edition. Diabetes Res. Clin. Pract. 2022, 183, 109083. [Google Scholar] [CrossRef] [PubMed]
- Perkins, B.A.; Sherr, J.L.; Mathieu, C. Type 1 diabetes glycemic management: Insulin therapy, glucose monitoring, and automation. Science 2021, 373, 522–527. [Google Scholar] [CrossRef]
- Ludvigsson, J. Novel therapies in the management of type I diabetes mellitus. Panminerva Med. 2012, 54, 257–270. [Google Scholar]
- Quinn, L.M.; Wong, F.S.; Narendran, P. Environmental Determinants of Type 1 Diabetes: From Association to Proving Causality. Front. Immunol. 2021, 12, 737964. [Google Scholar] [CrossRef]
- Leiva-Gea, I.; Sánchez-Alcoholado, L.; Martín-Tejedor, B.; Castellano-Castillo, D.; Moreno-Indias, I.; Urda-Cardona, A.; Tinahones, F.J.; Fernández-García, J.C.; Queipo-Ortuño, M.I. Gut Microbiota Differs in Composition and Functionality Between Children with Type 1 Diabetes and MODY2 and Healthy Control Subjects: A Case-Control Study. Diabetes Care 2018, 41, 2385–2395. [Google Scholar] [CrossRef] [PubMed]
- Murri, M.; Leiva, I.; Gomez-Zumaquero, J.M.; Tinahones, F.J.; Cardona, F.; Soriguer, F.; Queipo-Ortuño, M.I. Gut microbiota in children with type 1 diabetes differs from that in healthy children: A case-control study. BMC Med. 2013, 11, 46. [Google Scholar] [CrossRef] [PubMed]
- Salamon, D.; Sroka-Oleksiak, A.; Kapusta, P.; Szopa, M.; Mrozinska, S.; Ludwig-Slomczynska, A.H.; Wolkow, P.P.; Bulanda, M.; Klupa, T.; Malecki, M.T.; et al. Characteristics of gut microbiota in adult patients with type 1 and type 2 diabetes based on next-generation sequencing of the 16S rRNA gene fragment. Pol. Arch. Intern. Med. 2018, 128, 336–343. [Google Scholar] [CrossRef]
- Vaarala, O.; Atkinson, M.A.; Neu, J. The “perfect storm” for type 1 diabetes: The complex interplay between intestinal microbiota, gut permeability, and mucosal immunity. Diabetes 2008, 57, 2555–2562. [Google Scholar] [CrossRef]
- Hoekstra, J.B.; van Rijn, H.J.; Erkelens, D.W.; Thijssen, J.H. C-peptide. Diabetes Care 1982, 5, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Nathan, D.M.; Cleary, P.A.; Backlund, J.Y.; Genuth, S.M.; Lachin, J.M.; Orchard, T.J.; Raskin, P.; Zinman, B.; Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study Research Group. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N. Engl. J. Med. 2005, 353, 2643–2653. [Google Scholar] [PubMed]
- Winiarska-Mieczan, A.; Tomaszewska, E.; Donaldson, J.; Jachimowicz, K. The Role of Nutritional Factors in the Modulation of the Composition of the Gut Microbiota in People with Autoimmune Diabetes. Nutrients 2022, 14, 2498. [Google Scholar] [CrossRef] [PubMed]
- Yadav, H.; Lee, J.H.; Lloyd, J.; Walter, P.; Rane, S.G. Beneficial metabolic effects of a probiotic via butyrate-induced GLP-1 hormone secretion. J. Biol. Chem. 2013, 288, 25088–25097. [Google Scholar] [CrossRef]
- Ho, J.; Nicolucci, A.C.; Virtanen, H.; Schick, A.; Meddings, J.; Reimer, R.A.; Huang, C. Effect of Prebiotic on Microbiota, Intestinal Permeability, and Glycemic Control in Children With Type 1 Diabetes. J. Clin. Endocrinol. Metab. 2019, 104, 4427–4440. [Google Scholar] [CrossRef]
- Zhao, H.; Zhang, F.; Chai, J.; Wang, J. Effect of lactic acid bacteria on Listeria monocytogenes infection and innate immunity in rabbits. Czech J. Anim. Sci. 2020, 65, 23–30. [Google Scholar] [CrossRef]
- Wang, X.; Yang, J.; Qiu, X.; Wen, Q.; Liu, M.; Zhou, D.; Chen, Q. Probiotics, Pre-biotics and Synbiotics in the Treatment of Pre-diabetes: A Systematic Review of Randomized Controlled Trials. Front. Public Health 2021, 9, 645035. [Google Scholar] [CrossRef]
- Zheng, P.; Li, Z.; Zhou, Z. Gut microbiome in type 1 diabetes: A comprehensive review. Diabetes Metab. Res. Rev. 2018, 34, e3043. [Google Scholar] [CrossRef]
- Moravejolahkami, A.R.; Shakibaei, M.; Fairley, A.M.; Sharma, M. Probiotics, prebiotics, and synbiotics in type 1 diabetes mellitus: A systematic review and meta-analysis of clinical trials. Diabetes Metab. Res. 2023, 40, e3655. [Google Scholar] [CrossRef] [PubMed]
- Baroni, I.; Fabrizi, D.; Luciani, M.; Magon, A.; Conte, G.; De Angeli, G.; Paglione, G.; Ausili, D.; Caruso, R. Probiotics and synbiotics for glycemic control in diabetes: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2024, 43, 1041–1061. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Mean Variance Estimation. Available online: https://www.math.hkbu.edu.hk/~tongt/papers/median2mean.html (accessed on 22 December 2023).
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef]
- Huedo-Medina, T.B.; Sánchez-Meca, J.; Marín-Martínez, F.; Botella, J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol. Methods 2006, 11, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Lin, X.; Zhang, X. Analysis of the Curative Effect of Triple Live Bacteria of Bifidobacterium and Lactobacillus in the Treatment of Type 1 Diabetes. Diabetes New World 2021, 24, 89–92. [Google Scholar] [CrossRef]
- Tougaard, N.H.; Frimodt-Møller, M.; Salmenkari, H.; Stougaard, E.B.; Zawadzki, A.D.; Mattila, I.M.; Hansen, T.W.; Legido-Quigley, C.; Hörkkö, S.; Forsblom, C.; et al. Effects of Butyrate Supplementation on Inflammation and Kidney Parameters in Type 1 Diabetes: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Clin. Med. 2022, 11, 3573. [Google Scholar] [CrossRef] [PubMed]
- de Groot, P.F.; Nikolic, T.; Imangaliyev, S.; Bekkering, S.; Duinkerken, G.; Keij, F.M.; Herrema, H.; Winkelmeijer, M.; Kroon, J.; Levin, E.; et al. Oral butyrate does not affect innate immunity and islet autoimmunity in individuals with longstanding type 1 diabetes: A randomised controlled trial. Diabetologia 2020, 63, 597–610. [Google Scholar] [CrossRef]
- Bianchini, S.; Orabona, C.; Camilloni, B.; Berioli, M.G.; Argentiero, A.; Matino, D.; Alunno, A.; Albini, E.; Vacca, C.; Pallotta, M.T.; et al. Effects of probiotic administration on immune responses of children and adolescents with type 1 diabetes to a quadrivalent inactivated influenza vaccine. Hum. Vaccines Immunother. 2020, 16, 86–94. [Google Scholar] [CrossRef]
- Kumar, S.; Kumar, R.; Rohilla, L.; Jacob, N.; Yadav, J.; Sachdeva, N. A high potency multi-strain probiotic improves glycemic control in children with new-onset type 1 diabetes mellitus: A randomized, double-blind, and placebo-controlled pilot study. Pediatr. Diabetes 2021, 22, 1014–1022. [Google Scholar] [CrossRef]
- Wang, C.H.; Yen, H.R.; Lu, W.L.; Ho, H.H.; Lin, W.Y.; Kuo, Y.W.; Huang, Y.Y.; Tsai, S.Y.; Lin, H.C. Adjuvant Probiotics of Lactobacillus salivarius subsp. salicinius AP-32, L. johnsonii MH-68, and Bifidobacterium animalis subsp. lactis CP-9 Attenuate Glycemic Levels and Inflammatory Cytokines in Patients with Type 1 Diabetes Mellitus. Front. Endocrinol. 2022, 13, 754401. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhang, Y.; Luo, L.; Le, Y.; Li, Y.; Yuan, F.; Wu, Y.; Xu, P. The Beneficial Effects of a Multispecies Probiotic Supplement on Glycaemic Control and Metabolic Profile in Adults with Type 1 Diabetes: A Randomised, Double-Blinded, Placebo-Controlled Pilot-Study. Diabetes Metab. Syndr. Obes. 2023, 16, 829–840. [Google Scholar] [CrossRef] [PubMed]
- Zare Javid, A.; Aminzadeh, M.; Haghighi-Zadeh, M.H.; Jamalvandi, M. The Effects of Synbiotic Supplementation on Glycemic Status, Lipid Profile, and Biomarkers of Oxidative Stress in Type 1 Diabetic Patients. A Placebo-Controlled, Double-Blind, Randomized Clinical Trial. Diabetes Metab. Syndr. Obes. 2020, 13, 607–617. [Google Scholar] [CrossRef]
- Groele, L.; Szajewska, H.; Szalecki, M.; Świderska, J.; Wysocka-Mincewicz, M.; Ochocińska, A.; Stelmaszczyk-Emmel, A.; Demkow, U.; Szypowska, A. Lack of effect of Lactobacillus rhamnosus GG and Bifidobacterium lactis Bb12 on beta-cell function in children with newly diagnosed type 1 diabetes: A randomised controlled trial. BMJ Open Diabetes Res. Care 2021, 9, e001523. [Google Scholar] [CrossRef] [PubMed]
- Bidell, M.R.; Hobbs, A.L.V.; Lodise, T.P. Gut microbiome health and dysbiosis: A clinical primer. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2022, 42, 849–857. [Google Scholar] [CrossRef]
- Del Chierico, F.; Rapini, N.; Deodati, A.; Matteoli, M.C.; Cianfarani, S.; Putignani, L. Pathophysiology of Type 1 Diabetes and Gut Microbiota Role. Int. J. Mol. Sci. 2022, 23, 14650. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Peng, J.; Li, F.; Wong, F.S.; Wen, L. Evaluation of different mucosal microbiota leads to gut microbiota-based prediction of type 1 diabetes in NOD mice. Sci. Rep. 2018, 8, 15451. [Google Scholar] [CrossRef]
- Hänninen, A.; Toivonen, R.; Pöysti, S.; Belzer, C.; Plovier, H.; Ouwerkerk, J.P.; Emani, R.; Cani, P.D.; De Vos, W.M. Akkermansia muciniphila induces gut microbiota remodelling and controls islet autoimmunity in NOD mice. Gut 2018, 67, 1445–1453. [Google Scholar] [CrossRef]
- Vatanen, T.; Franzosa, E.A.; Schwager, R.; Tripathi, S.; Arthur, T.D.; Vehik, K.; Lernmark, Å.; Hagopian, W.A.; Rewers, M.J.; She, J.-X.; et al. The human gut microbiome in early-onset type 1 diabetes from the TEDDY study. Nature 2018, 562, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Sun, M.; Wang, T.; Zhang, S.; Song, X.; Liu, X.; Wei, J.; Chen, Q.; Zhong, T.; Qin, J. Gut microbiota and type 1 diabetes: A two-sample bidirectional Mendelian randomization study. Front. Cell. Infect. Microbiol. 2023, 13, 1163898. [Google Scholar] [CrossRef]
- Devi, M.B.; Sarma, H.K.; Mukherjee, A.K.; Khan, M.R. Mechanistic Insights into Immune-Microbiota Interactions and Preventive Role of Probiotics Against Autoimmune Diabetes Mellitus. Probiotics Antimicro Prot. 2023, 15, 983–1000. [Google Scholar] [CrossRef]
- Alshrari, A.S.; Hudu, S.A.; Elmigdadi, F.; Imran, M. The Urgent Threat of Clostridioides difficile Infection: A Glimpse of the Drugs of the Future, with Related Patents and Prospects. Biomedicines 2023, 11, 426. [Google Scholar] [CrossRef]
- Chapman, C.M.; Gibson, G.R.; Rowland, I. Health benefits of probiotics: Are mixtures more effective than single strains? Eur. J. Nutr. 2011, 50, 1–17. [Google Scholar] [CrossRef]
- Dolpady, J.; Sorini, C.; Di Pietro, C.; Cosorich, I.; Ferrarese, R.; Saita, D.; Clementi, M.; Canducci, F.; Falcone, M. Oral Probiotic VSL#3 Prevents Autoimmune Diabetes by Modulating Microbiota and Promoting Indoleamine 2,3-Dioxygenase-Enriched Tolerogenic Intestinal Environment. J. Diabetes Res. 2016, 2016, 7569431. [Google Scholar] [CrossRef]
- Mishra, S.P.; Wang, S.; Nagpal, R.; Miller, B.; Singh, R.; Taraphder, S.; Yadav, H. Probiotics and Prebiotics for the Amelioration of Type 1 Diabetes: Present and Future Perspectives. Microorganisms 2019, 7, 67. [Google Scholar] [CrossRef]
- Niu, W.; Ding, X. Influence of Live combined Bifidobacterium and Lactobacillus Tablet for Intestinal Microflora and Serum IFN-γ, IL-4 in Children with Type 1 Diabetes Mellitus. J. Henan Univ. Sci. Technol. (Med. Sci.) 2016, 34, 196–198. [Google Scholar] [CrossRef]
- Jumpertz, R.; Le, D.S.; Turnbaugh, P.J.; Trinidad, C.; Bogardus, C.; Gordon, J.I.; Krakoff, J. Energy-balance studies reveal associations between gut microbes, caloric load, and nutrient absorption in humans. Am. J. Clin. Nutr. 2011, 94, 58–65. [Google Scholar] [CrossRef]
- Pandey, K.R.; Naik, S.R.; Vakil, B.V. Probiotics, prebiotics and synbiotics- a review. J. Food Sci. Technol. 2015, 52, 7577–7587. [Google Scholar] [CrossRef]
- Ning, C.; Wang, X.; Gao, S.; Mu, J.; Wang, Y.; Liu, S.; Zhu, J.; Meng, X. Chicory inulin ameliorates type 2 diabetes mellitus and suppresses JNK and MAPK pathways in vivo and in vitro. Mol. Nutr. Food Res. 2017, 61, 1600673. [Google Scholar] [CrossRef] [PubMed]
- Derrien, M.; Alvarez, A.S.; de Vos, W.M. The Gut Microbiota in the First Decade of Life. Trends Microbiol. 2019, 27, 997–1010. [Google Scholar] [CrossRef] [PubMed]
- Quarta, A.; Guarino, M.; Tripodi, R.; Giannini, C.; Chiarelli, F.; Blasetti, A. Diet and Glycemic Index in Children with Type 1 Diabetes. Nutrients 2023, 15, 3507. [Google Scholar] [CrossRef] [PubMed]
- Quirk, H.; Blake, H.; Tennyson, R.; Randell, T.L.; Glazebrook, C. Physical activity interventions in children and young people with Type 1 diabetes mellitus: A systematic review with meta-analysis. Diabet. Med. 2014, 31, 1163–1173. [Google Scholar] [CrossRef]
- Ng, Q.X.; Lim, Y.L.; Yaow, C.Y.L.; Ng, W.K.; Thumboo, J.; Liew, T.M. Effect of Probiotic Supplementation on Gut Microbiota in Patients with Major Depressive Disorders: A Systematic Review. Nutrients 2023, 15, 1351. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Savilahti, E.; Härkönen, T.; Savilahti, E.M.; Kukkonen, K.; Kuitunen, M.; Knip, M. Probiotic intervention in infancy is not associated with development of beta cell autoimmunity and type 1 diabetes. Diabetologia 2018, 61, 2668–2670. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, S.M.; Coren, A.T.; Pant, T.; Ciecko, A.E.; Jia, S.; Roethle, M.F.; Simpson, P.M.; Atkinson, S.N.; Salzman, N.H.; Chen, Y.G.; et al. Probiotic normalization of systemic inflammation in siblings of type 1 diabetes patients: An open-label pilot study. Sci. Rep. 2022, 12, 3306. [Google Scholar] [CrossRef] [PubMed]
- Mondanelli, G.; Orecchini, E.; Volpi, C.; Panfili, E.; Belladonna, M.L.; Pallotta, M.T.; Moretti, S.; Galarini, R.; Esposito, S.; Orabona, C. Effect of Probiotic Administration on Serum Tryptophan Metabolites in Pediatric Type 1 Diabetes Patients. Int. J. Tryptophan Res. 2020, 13, 1178646920956646. [Google Scholar] [CrossRef] [PubMed]
- Ross, P. Expression of concern: Metabolic and genetic response to probiotics supplementation in patients with diabetic nephropathy: A randomized, double-blind, placebo-controlled trial. Food Funct. 2022, 13, 4229. [Google Scholar] [CrossRef]
- Soleimani, A.; Motamedzadeh, A.; Zarrati Mojarrad, M.; Bahmani, F.; Amirani, E.; Ostadmohammadi, V.; Tajabadi-Ebrahimi, M.; Asemi, Z. The Effects of Synbiotic Supplementation on Metabolic Status in Diabetic Patients Undergoing Hemodialysis: A Randomized, Double-Blinded, Placebo-Controlled Trial. Probiotics Antimicrob. Proteins 2019, 11, 1248–1256. [Google Scholar] [CrossRef]
- Soleimani, A.; Mojarrad, M.Z.; Bahmani, F.; Taghizadeh, M.; Ramezani, M.; Tajabadi-Ebrahimi, M.; Jafari, P.; Esmaillzadeh, A.; Asemi, Z. Probiotic supplementation in diabetic hemodialysis patients has beneficial metabolic effects. Kidney Int. 2017, 91, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Soleimani, A.; Mojarrad, M.Z.; Bahmani, F.; Taghizadeh, M.; Ramezani, M.; Tajabadi-Ebrahimi, M.; Jafari, P.; Esmaillzadeh, A.; Asemi, Z. Metabolite-based dietary supplementation in human type 1 diabetes is associated with microbiota and immune modulation. Microbiome 2022, 10, 9. [Google Scholar] [CrossRef] [PubMed]
- Lai, S.; Lingström, P.; Cagetti, M.G.; Cocco, F.; Meloni, G.; Arrica, M.A.; Campus, G. Effect of Lactobacillus brevis CD2 containing lozenges and plaque pH and cariogenic bacteria in diabetic children: A randomised clinical trial. Clin. Oral Investig. 2021, 25, 115–123. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).