
Association of Dietary Retinol Intake and Serum Neurofilament Light Chain Levels: Results from NHANES 2013–2014

Abstract
:1. Introduction
2. Materials and Methods
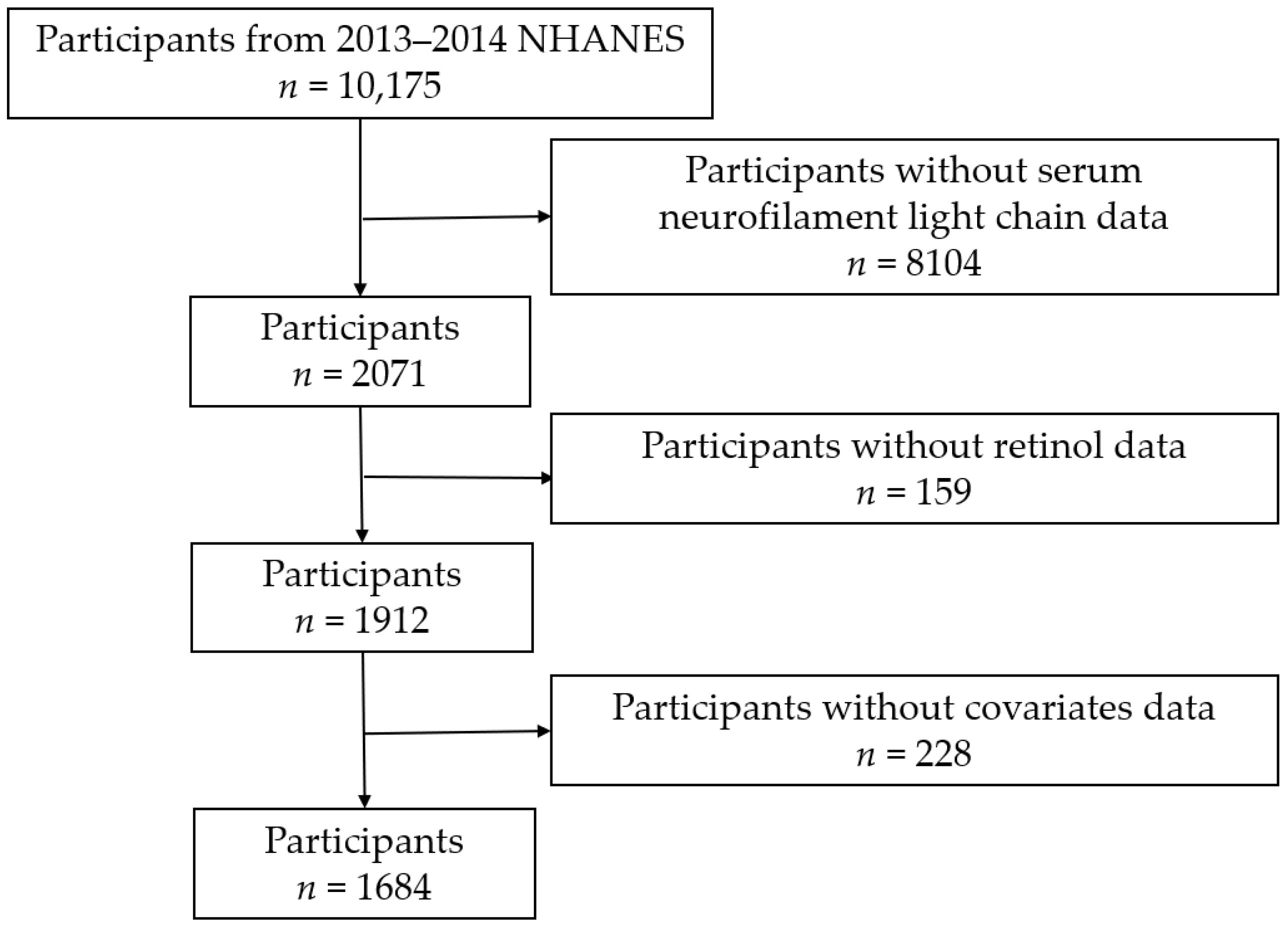
2.1. Study Population Samples
2.2. Dietary Retinol Intake Assessment
2.3. Measurement of sNfL Levels
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics for All Participants
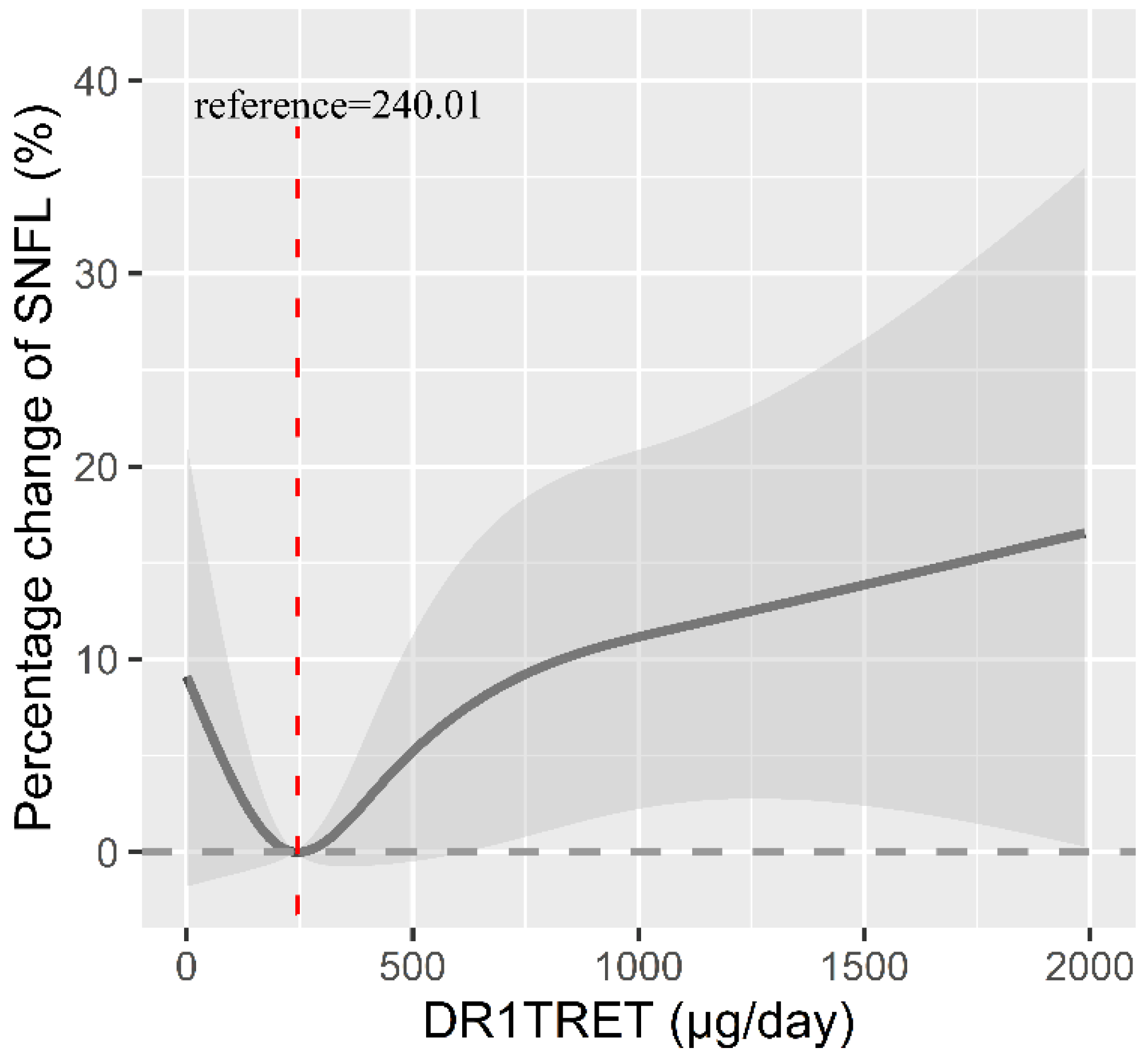
3.2. Association between Retinol Intake and sNfL Levels
3.3. Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abu-Rumeileh, S.; Abdelhak, A.; Foschi, M.; D’Anna, L.; Russo, M.; Steinacker, P.; Kuhle, J.; Tumani, H.; Blennow, K.; Otto, M. The multifaceted role of neurofilament light chain protein in non-primary neurological diseases. Brain 2023, 146, 421–437. [Google Scholar] [CrossRef] [PubMed]
- Gaetani, L.; Blennow, K.; Calabresi, P.; Di Filippo, M.; Parnetti, L.; Zetterberg, H. Neurofilament light chain as a biomarker in neurological disorders. J. Neurol. Neurosurg. Psychiatry 2019, 90, 870–881. [Google Scholar] [CrossRef] [PubMed]
- Gafson, A.R.; Barthélemy, N.R.; Bomont, P.; Carare, R.O.; Durham, H.D.; Julien, J.P.; Kuhle, J.; Leppert, D.; Nixon, R.A.; Weller, R.O.; et al. Neurofilaments: Neurobiological foundations for biomarker applications. Brain 2020, 143, 1975–1998. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, M.; Rayner, M.L.D.; Guillemot-Legris, O.; Platt, I.; Brown, H.; Quick, T.; Phillips, J.B. Serum neurofilament light chain measurements following nerve trauma. J. Peripher. Nerv. Syst. 2023, 28, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Dietmann, A.S.; Kruse, N.; Stork, L.; Gloth, M.; Brück, W.; Metz, I. Neurofilament light chains in serum as biomarkers of axonal damage in early MS lesions: A histological-serological correlative study. J. Neurol. 2023, 270, 1416–1429. [Google Scholar] [CrossRef] [PubMed]
- Brune, S.; Høgestøl, E.A.; de Rodez Benavent, S.A.; Berg-Hansen, P.; Beyer, M.K.; Leikfoss, I.S.; Bos, S.D.; Sowa, P.; Brunborg, C.; Andorra, M.; et al. Serum neurofilament light chain concentration predicts disease worsening in multiple sclerosis. Mult. Scler. 2022, 28, 1859–1870. [Google Scholar] [CrossRef] [PubMed]
- Blaner, W.S. Vitamin A signaling and homeostasis in obesity, diabetes, and metabolic disorders. Pharmacol. Ther. 2019, 197, 153–178. [Google Scholar] [CrossRef] [PubMed]
- Woldie, H.; Kebede, Y.; Tariku, A. Factors Associated with Anemia among Children Aged 6-23 Months Attending Growth Monitoring at Tsitsika Health Center, Wag-Himra Zone, Northeast Ethiopia. J. Nutr. Metab. 2015, 2015, 928632. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.; Zamwar, U.M.; Mudey, A. Etiology, Epidemiology, Pathophysiology, Signs and Symptoms, Evaluation, and Treatment of Vitamin A (Retinol) Deficiency. Cureus 2023, 15, e49011. [Google Scholar] [CrossRef]
- Alapatt, P.; Guo, F.; Komanetsky, S.M.; Wang, S.; Cai, J.; Sargsyan, A.; Rodríguez Díaz, E.; Bacon, B.T.; Aryal, P.; Graham, T.E. Liver retinol transporter and receptor for serum retinol-binding protein (RBP4). J. Biol. Chem. 2013, 288, 1250–1265. [Google Scholar] [CrossRef] [PubMed]
- Mangrolia, P.; Murphy, R.M. Retinol-Binding Protein Interferes with Transthyretin-Mediated β-Amyloid Aggregation Inhibition. Biochemistry 2018, 57, 5029–5040. [Google Scholar] [CrossRef] [PubMed]
- Gião, T.; Saavedra, J.; Vieira, J.R.; Pinto, M.T.; Arsequell, G.; Cardoso, I. Neuroprotection in early stages of Alzheimer’s disease is promoted by transthyretin angiogenic properties. Alzheimers Res. Ther. 2021, 13, 143. [Google Scholar] [CrossRef] [PubMed]
- Hyung, S.J.; Deroo, S.; Robinson, C.V. Retinol and retinol-binding protein stabilize transthyretin via formation of retinol transport complex. ACS Chem. Biol. 2010, 5, 1137–1146. [Google Scholar] [CrossRef] [PubMed]
- Stoney, P.N.; McCaffery, P. A Vitamin on the Mind: New Discoveries on Control of the Brain by Vitamin A. World Rev. Nutr. Diet. 2016, 115, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Janesick, A.; Wu, S.C.; Blumberg, B. Retinoic acid signaling and neuronal differentiation. Cell. Mol. Life Sci. 2015, 72, 1559–1576. [Google Scholar] [CrossRef] [PubMed]
- Hou, N.; Ren, L.; Gong, M.; Bi, Y.; Gu, Y.; Dong, Z.; Liu, Y.; Chen, J.; Li, T. Vitamin A deficiency impairs spatial learning and memory: The mechanism of abnormal CBP-dependent histone acetylation regulated by retinoic acid receptor alpha. Mol. Neurobiol. 2015, 51, 633–647. [Google Scholar] [CrossRef] [PubMed]
- Bonhomme, D.; Minni, A.M.; Alfos, S.; Roux, P.; Richard, E.; Higueret, P.; Moisan, M.P.; Pallet, V.; Touyarot, K. Vitamin A status regulates glucocorticoid availability in Wistar rats: Consequences on cognitive functions and hippocampal neurogenesis? Front. Behav. Neurosci. 2014, 8, 20. [Google Scholar] [CrossRef] [PubMed]
- Hviid, C.V.B.; Madsen, A.T.; Winther-Larsen, A. Biological variation of serum neurofilament light chain. Clin. Chem. Lab. Med. 2022, 60, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Lee, B.H.; Yip, W.; Chou, P.; Yip, B.S. Neurofilament Proteins as Prognostic Biomarkers in Neurological Disorders. Curr. Pharm. Des. 2020, 25, 4560–4569. [Google Scholar] [CrossRef] [PubMed]
- Bi, Z.; Meng, Y.; Ji, Q.; Zhang, A.; Liu, M.; Xu, X.; Zhan, Y. Association between volatile organic compounds and serum neurofilament light chain in US adults. Sci. Total Environ. 2024, 926, 171893. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, K.C.; Sotirchos, E.S.; Smith, M.D.; Lord, H.N.; DuVal, A.; Mowry, E.M.; Calabresi, P.A. Contributors to Serum NfL Levels in People without Neurologic Disease. Ann. Neurol. 2022, 92, 688–698. [Google Scholar] [CrossRef] [PubMed]
- Ciardullo, S.; Muraca, E.; Bianconi, E.; Ronchetti, C.; Cannistraci, R.; Rossi, L.; Perra, S.; Zerbini, F.; Perseghin, G. Serum neurofilament light chain levels are associated with all-cause mortality in the general US population. J. Neurol. 2023, 270, 3830–3838. [Google Scholar] [CrossRef]
- Wu, M.; Shu, Y.; Wang, L.; Song, L.; Chen, S.; Liu, Y.; Bi, J.; Li, D.; Yang, Y.; Hu, Y.; et al. Metabolic syndrome severity score and the progression of CKD. Eur. J. Clin. Investig. 2022, 52, e13646. [Google Scholar] [CrossRef]
- Stukas, S.; Cooper, J.; Higgins, V.; Holmes, D.; Adeli, K.; Wellington, C.L. Pediatric reference intervals for serum neurofilament light and glial fibrillary acidic protein using the Canadian Laboratory Initiative on Pediatric Reference Intervals (CALIPER) cohort. Clin. Chem. Lab. Med. 2024, 62, 698–705. [Google Scholar] [CrossRef]
- Beltran, T.A. Normative Values for Serum Neurofilament Light Chain in US Adults. J. Clin. Neurol. 2024, 20, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.M.; Chu, P.L.; Wang, C.; Lin, C.Y. Association between urinary glyphosate levels and serum neurofilament light chain in a representative sample of US adults: NHANES 2013-2014. J. Expo. Sci. Environ. Epidemiol. 2023, 34, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Simonsen, A.H.; Gleerup, H.S.; Musaeus, C.S.; Sellebjerg, F.; Hansen, M.B.; Søndergaard, H.B.; Waldemar, G.; Hasselbalch, S.G. Neurofilament light chain levels in serum among a large mixed memory clinic cohort: Confounders and diagnostic usefulness. Alzheimer’s Dement. J. 2023, 15, e12512. [Google Scholar] [CrossRef]
- Liu, X.; Chen, J.; Meng, C.; Zhou, L.; Liu, Y. Serum neurofilament light chain and cognition decline in US elderly: A cross-sectional study. Ann. Clin. Transl. Neurol. 2024, 11, 17–29. [Google Scholar] [CrossRef]
- Gawde, S.; Agasing, A.; Bhatt, N.; Toliver, M.; Kumar, G.; Massey, K.; Nguyen, A.; Mao-Draayer, Y.; Macwana, S.; DeJager, W.; et al. Biomarker panel increases accuracy for identification of an MS relapse beyond sNfL. Mult. Scler. Relat. Disord. 2022, 63, 103922. [Google Scholar] [CrossRef]
- Rosso, M.; Gonzalez, C.T.; Healy, B.C.; Saxena, S.; Paul, A.; Bjornevik, K.; Kuhle, J.; Benkert, P.; Leppert, D.; Guttmann, C.; et al. Temporal association of sNfL and gad-enhancing lesions in multiple sclerosis. Ann. Clin. Transl. Neurol. 2020, 7, 945–955. [Google Scholar] [CrossRef]
- Berends, M.; Brunger, A.F.; Bijzet, J.; Kroesen, B.J.; Drost, G.; Lange, F.; Teunissen, C.E.; Int Veld, S.; Vrancken, A.F.; Gans, R.O.B.; et al. Longitudinal analysis of serum neurofilament light chain levels as marker for neuronal damage in hereditary transthyretin amyloidosis. Amyloid 2024, 31, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Simone, M.; De Giacomo, A.; Palumbi, R.; Palazzo, C.; Lucisano, G.; Pompamea, F.; Micella, S.; Pascali, M.; Gabellone, A.; Marzulli, L.; et al. Serum Neurofilament Light Chain and Glial Fibrillary Acidic Protein as Potential Diagnostic Biomarkers in Autism Spectrum Disorders: A Preliminary Study. Int. J. Mol. Sci. 2023, 24, 3057. [Google Scholar] [CrossRef] [PubMed]
- Huppke, B.; Reinert, M.C.; Hummel-Abmeier, H.; Stark, W.; Gärtner, J.; Huppke, P. Pretreatment Neurofilament Light Chain Serum Levels, Early Disease Severity, and Treatment Response in Pediatric Multiple Sclerosis. Neurology 2023, 101, e1873–e1883. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Fan, J.; Yuan, L.; Nan, Y.; Nan, S. Serum Neurofilament Light Predicts Severity and Prognosis in Patients with Ischemic Stroke. Neurotox. Res. 2020, 37, 987–995. [Google Scholar] [CrossRef] [PubMed]
- De Schaepdryver, M.; Goossens, J.; De Meyer, S.; Jeromin, A.; Masrori, P.; Brix, B.; Claeys, K.G.; Schaeverbeke, J.; Adamczuk, K.; Vandenberghe, R.; et al. Serum neurofilament heavy chains as early marker of motor neuron degeneration. Ann. Clin. Transl. Neurol. 2019, 6, 1971–1979. [Google Scholar] [CrossRef] [PubMed]
- Bock, M.; Steffen, F.; Zipp, F.; Bittner, S. Impact of Dietary Intervention on Serum Neurofilament Light Chain in Multiple Sclerosis. Neurol. Neuroimmunol. Neuroinflamm. 2022, 9, 1. [Google Scholar] [CrossRef] [PubMed]
- Oh, U.; Woolbright, E.; Lehner-Gulotta, D.; Coleman, R.; Conaway, M.; Goldman, M.D.; Brenton, J.N. Serum neurofilament light chain in relapsing multiple sclerosis patients on a ketogenic diet. Mult. Scler. Relat. Disord. 2023, 73, 104670. [Google Scholar] [CrossRef] [PubMed]
- Wassif, G.A.; Alrehely, M.S.; Alharbi, D.M.; Aljohani, A.A. The Impact of Vitamin D on Neuropsychiatric Disorders. Cureus 2023, 15, e47716. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Rani, N.; Gangwar, A.; Singh, R.; Kaur, R.; Upadhyaya, K. Diabetic Neuropathy: A Repercussion of Vitamin D Deficiency. Curr. Diabetes Rev. 2023, 19, e170822207592. [Google Scholar] [CrossRef]
- Anwar, M.J.; Alenezi, S.K.; Alhowail, A.H. Molecular insights into the pathogenic impact of vitamin D deficiency in neurological disorders. Biomed. Pharmacother. 2023, 162, 114718. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Li, Y.; Meng, X. Vitamin D and neurodegenerative diseases. Heliyon 2023, 9, e12877. [Google Scholar] [CrossRef] [PubMed]
- Holmøy, T.; Røsjø, E.; Zetterberg, H.; Blennow, K.; Lindstrøm, J.C.; Steffensen, L.H.; Kampman, M.T. Vitamin D supplementation and neurofilament light chain in multiple sclerosis. Acta Neurol. Scand. 2019, 139, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Hänninen, K.; Jääskeläinen, O.; Herukka, S.K.; Soilu-Hänninen, M. Vitamin D supplementation and serum neurofilament light chain in interferon-beta-1b-treated MS patients. Brain Behav. 2020, 10, e01772. [Google Scholar] [CrossRef] [PubMed]
- Hammond, B.R. Dietary Carotenoids and the Nervous System. Foods 2015, 4, 698–701. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.R. The neurotoxic effects of vitamin A and retinoids. An. Acad. Bras. Cienc. 2015, 87, 1361–1373. [Google Scholar] [CrossRef] [PubMed]
- Ladang, A.; Kovacs, S.; Lengelé, L.; Locquet, M.; Reginster, J.Y.; Bruyère, O.; Cavalier, E. Neurofilament light chain concentration in an aging population. Aging Clin. Exp. Res. 2022, 34, 331–339. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, P.D.; Hinder, L.M.; Callaghan, B.C.; Feldman, E.L. Neurological consequences of obesity. Lancet Neurol. 2017, 16, 465–477. [Google Scholar] [CrossRef] [PubMed]
- Mazon, J.N.; de Mello, A.H.; Ferreira, G.K.; Rezin, G.T. The impact of obesity on neurodegenerative diseases. Life Sci. 2017, 182, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Määttä, L.L.; Andersen, S.T.; Parkner, T.; Hviid, C.V.B.; Bjerg, L.; Kural, M.A.; Charles, M.; Søndergaard, E.; Kuhle, J.; Tankisi, H.; et al. Longitudinal Change in Serum Neurofilament Light Chain in Type 2 Diabetes and Early Diabetic Polyneuropathy: ADDITION-Denmark. Diabetes Care 2024, 47, 986–994. [Google Scholar] [CrossRef] [PubMed]
- Tang, R.; Panizzon, M.S.; Elman, J.A.; Gillespie, N.A.; Hauger, R.L.; Rissman, R.A.; Lyons, M.J.; Neale, M.C.; Reynolds, C.A.; Franz, C.E.; et al. Association of neurofilament light chain with renal function: Mechanisms and clinical implications. Alzheimers Res. Ther. 2022, 14, 189. [Google Scholar] [CrossRef] [PubMed]
- Voskuhl, R.; Kuhle, J.; Siddarth, P.; Itoh, N.; Patel, K.; MacKenzie-Graham, A. Decreased neurofilament light chain levels in estriol-treated multiple sclerosis. Ann. Clin. Transl. Neurol. 2022, 9, 1316–1320. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristic | All | Quartile of Dietary Retinol Intake (μg/day) | ||||
|---|---|---|---|---|---|---|
| Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | p-Value | ||
| N | 1684 | 420 | 421 | 419 | 424 | |
| Age, years (mean (SD)) | 46.59 ± 15.5 | 46.19 (15.6) | 47.05 (15.5) | 47.18 (15.4) | 45.93 (15.4) | 0.569 |
| Sex, n (%) | <0.001 | |||||
| male | 812 (48.2) | 189 (45.0) | 168 (39.9) | 189 (45.1) | 266 (62.7) | |
| female | 872 (51.8) | 231 (55.0) | 253 (60.1) | 230 (54.9) | 158 (37.3) | |
| BMI, kg/m2 (%) | 0.345 | |||||
| <30 kg/m2 | 1040 (61.8) | 275 (65.5) | 256 (60.8) | 252 (60.1) | 257 (60.6) | |
| ≥30 kg/m2 | 644 (38.2) | 145 (34.5) | 165 (39.2) | 167 (39.9) | 167 (39.4) | |
| Race, n (%) | <0.001 | |||||
| Mexican American or other | 447 (26.6) | 135 (32.1) | 125 (29.7) | 110 (26.3) | 77 (18.2) | |
| Non-Hispanic black | 302 (17.9) | 104 (24.8) | 61 (14.5) | 69 (16.5) | 68 (16.0) | |
| Non-Hispanic white | 783 (46.5) | 137 (32.6) | 203 (48.2) | 200 (47.7) | 243 (57.3) | |
| Other Hispanic | 152 (9.0) | 44 (10.5) | 32 (7.6) | 40 (9.5) | 36 (8.5) | |
| Education, n (%) | 0.545 | |||||
| <High school | 93 (5.5) | 29 (6.9) | 19 (4.5) | 24 (5.7) | 21 (5.0) | |
| High school | 233 (13.8) | 58 (13.8) | 59 (14.0) | 65 (15.5) | 51 (12.0) | |
| College or above | 1358 (80.6) | 333 (79.3) | 343 (81.5) | 330 (78.8) | 352 (83.0) | |
| PIR (mean (SD)) | 2.54 ± 1.7 | 2.38 (1.6) | 2.62 (1.7) | 2.53 (1.7) | 2.63 (1.7) | 0.119 |
| Smoke (%) | 0.837 | |||||
| No | 949 (56.4) | 237 (56.4) | 238 (56.5) | 229 (54.7) | 245 (57.8) | |
| Yes | 735 (43.6) | 183 (43.6) | 183 (43.5) | 190 (45.3) | 179 (42.2) | |
| Alcohol (%) | 0.879 | |||||
| No | 422 (25.1) | 110 (26.2) | 107 (25.4) | 104 (24.8) | 101 (23.8) | |
| Yes | 1262 (74.9) | 310 (73.8) | 314 (74.6) | 315 (75.2) | 323 (76.2) | |
| Diabetes (%) | 0.997 | |||||
| No | 1384 (82.2) | 344 (81.9) | 347 (82.4) | 345 (82.3) | 348 (82.1) | |
| Yes | 300 (17.8) | 76 (18.1) | 74 (17.6) | 74 (17.7) | 76 (17.9) | |
| eGFR, mL/min/1.73 m2 (mean (SD)) | 96.05 ± 21.4 | 96.79 (21.13) | 96.06 (21.39) | 95.95 (22.19) | 95.41 (20.75) | 0.825 |
| MET (mean (SD)) | 638.6 ± 2638.8 | 572.89 (815.9) | 543.99 (839.0) | 556.89 (795.8) | 878.24 (5063.8) | 0.195 |
| DR1TKCAL (mean (SD)) | 2172.03 ± 1037.0 | 1608.65 (789.6) | 1975.81 (800.0) | 2252.26 (840.0) | 2845.65 (1230.2) | <0.001 |
| DR1TRET (mean (SD)) | 309 (374) | 74.39 (43.96) | 229.26 (45.09) | 405.03 (63.69) | 888.06 (457.65) | <0.001 |
| SNFL (median [IQR]) | 16.6 ± 20.6 | 11.55 [8.0, 18.7] | 12.30 [8.1, 19.0] | 12.40 [8.1, 17.8] | 12.50 [8.7, 19.7] | 0.388 |
| Models | Percentage Change (%) and 95% CI | p-Value |
|---|---|---|
| Model 1 | 3.62 (0.52, 6.81) | 0.022 |
| Model 2 | 3.38 (0.67, 6.17) | 0.014 |
| Model 3 | 3.47 (0.54, 6.49) | 0.020 |
| Retinol Intake (μg/day) | Crude Model | Adjusted Model | ||
|---|---|---|---|---|
| Percentage Change (%) and 95% CI | p-Value | Percentage Change (%) and 95% CI | p-Value | |
| Fitting by two piecewise linear models | ||||
| ≤240.01 | −0.48 (−25.78, 33.45) | 0.974 | −14.21 (−34.23, 11.89) | 0.258 |
| >240.01 | 4.20 (0.35, 8.20) | 0.032 | 4.39 (0.89, 8.01) | 0.014 |
| Participants | N | Models | Percentage Change (%) and 95% CI | p-Value | p for Interaction |
|---|---|---|---|---|---|
| Age subgroup | 0.535 | ||||
| <60 | 1246 | Model 1 | 4.48 (1.19, 7.87) | 0.007 | |
| Model 2 | 3.49 (0.20, 6.90) | 0.038 | |||
| Model 3 | 3.80 (0.43, 7.28) | 0.027 | |||
| ≥60 | 438 | Model 1 | 3.72 (−2.28,10.08) | 0.230 | |
| Model 2 | 4.60 (−1.72, 11.33) | 0.158 | |||
| Model 3 | 3.39 (−3.49, 10.78) | 0.343 | |||
| Sex subgroup | |||||
| Male | 812 | Model 1 | 2.39 (−1.28, 6.21) | 0.205 | 0.428 |
| Model 2 | 2.83 (−0.46, 6.22) | 0.093 | |||
| Model 3 | 3.04 (−0.56, 6.77) | 0.100 | |||
| Female | 872 | Model 1 | 4.53 (−1.39, 10.80) | 0.137 | |
| Model 2 | 4.72 (−0.21, 9.90) | 0.061 | |||
| Model 3 | 4.52 (−0.76, 10.07) | 0.095 | |||
| BMI subgroup | 0.115 | ||||
| Non-obese (<30 kg/m2) | 1040 | Model 1 | 5.68 (1.95, 9.54) | 0.003 | |
| Model 2 | 5.30 (2.05, 8.65) | 0.001 | |||
| Model 3 | 6.28 (2.66, 10.02) | <0.001 | |||
| Obese (≥30 kg/m2) | 644 | Model 1 | 0.64 (−4.64, 6.20) | 0.818 | |
| Model 2 | 0.67 (−3.95, 5.50) | 0.781 | |||
| Model 3 | 0.22 (−4.67, 5.37) | 0.930 | |||
| eGFR subgroup | 0.140 | ||||
| Healthy (≥90 mL/min/1.73 m2) | 1076 | Model 1 | 1.23 (−2.30, 4.88) | 0.501 | |
| Model 2 | 0.10 (−3.11, 3.40) | 0.954 | |||
| Model 3 | 0.96 (−2.53, 4.59) | 0.594 | |||
| Damaged (<90 mL/min/1.73 m2) | 608 | Model 1 | 6.16 (1.21, 11.35) | 0.015 | |
| Model 2 | 8.56 (3.81, 13.52) | <0.001 | |||
| Model 3 | 6.90 (1.44, 12.65) | 0.013 | |||
| Diabetes subgroup | 0.351 | ||||
| No | 1384 | Model 1 | 4.75 (1.49, 8.11) | 0.004 | |
| Model 2 | 3.75 (0.91, 6.67) | 0.009 | |||
| Model 3 | 4.17 (1.08, 7.36) | 0.008 | |||
| Yes | 300 | Model 1 | −1.96 (−10.28, 7.12) | 0.662 | |
| Model 2 | 0.65 (−7.64, 9.67) | 0.883 | |||
| Model 3 | −4.59 (−13.33, 5.05) | 0.340 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, N.; Li, H.; Zhang, K.; Wang, Y.; Xiang, L.; Xiao, L.; Luo, G. Association of Dietary Retinol Intake and Serum Neurofilament Light Chain Levels: Results from NHANES 2013–2014. Nutrients 2024, 16, 1763. https://doi.org/10.3390/nu16111763
Liang N, Li H, Zhang K, Wang Y, Xiang L, Xiao L, Luo G. Association of Dietary Retinol Intake and Serum Neurofilament Light Chain Levels: Results from NHANES 2013–2014. Nutrients. 2024; 16(11):1763. https://doi.org/10.3390/nu16111763
Chicago/Turabian StyleLiang, Na, Hao Li, Keyi Zhang, Yan Wang, Lu Xiang, Lin Xiao, and Gang Luo. 2024. "Association of Dietary Retinol Intake and Serum Neurofilament Light Chain Levels: Results from NHANES 2013–2014" Nutrients 16, no. 11: 1763. https://doi.org/10.3390/nu16111763