

Quantity, Duration, Adherence, and Reasons for Dietary Supplement Use among Adults: Results from NHANES 2011–2018


Abstract
1. Introduction
2. Materials and Methods
2.1. Key Variables
2.2. Statistical Analyses
3. Results
3.1. Quantity, Duration, and Adherence of Supplements
3.2. Reasons for Taking Supplements
3.2.1. Reasons for Taking Supplements by Own Initiative
3.2.2. Recommended Reasons from Health Professionals for Supplement Use
3.2.3. Effect of Sex on Reasons for Supplement Use
3.2.4. Effect of Age on Reasons for Supplement Use
3.2.5. Effect of Race/Ethnicity on Reasons for Supplement Use
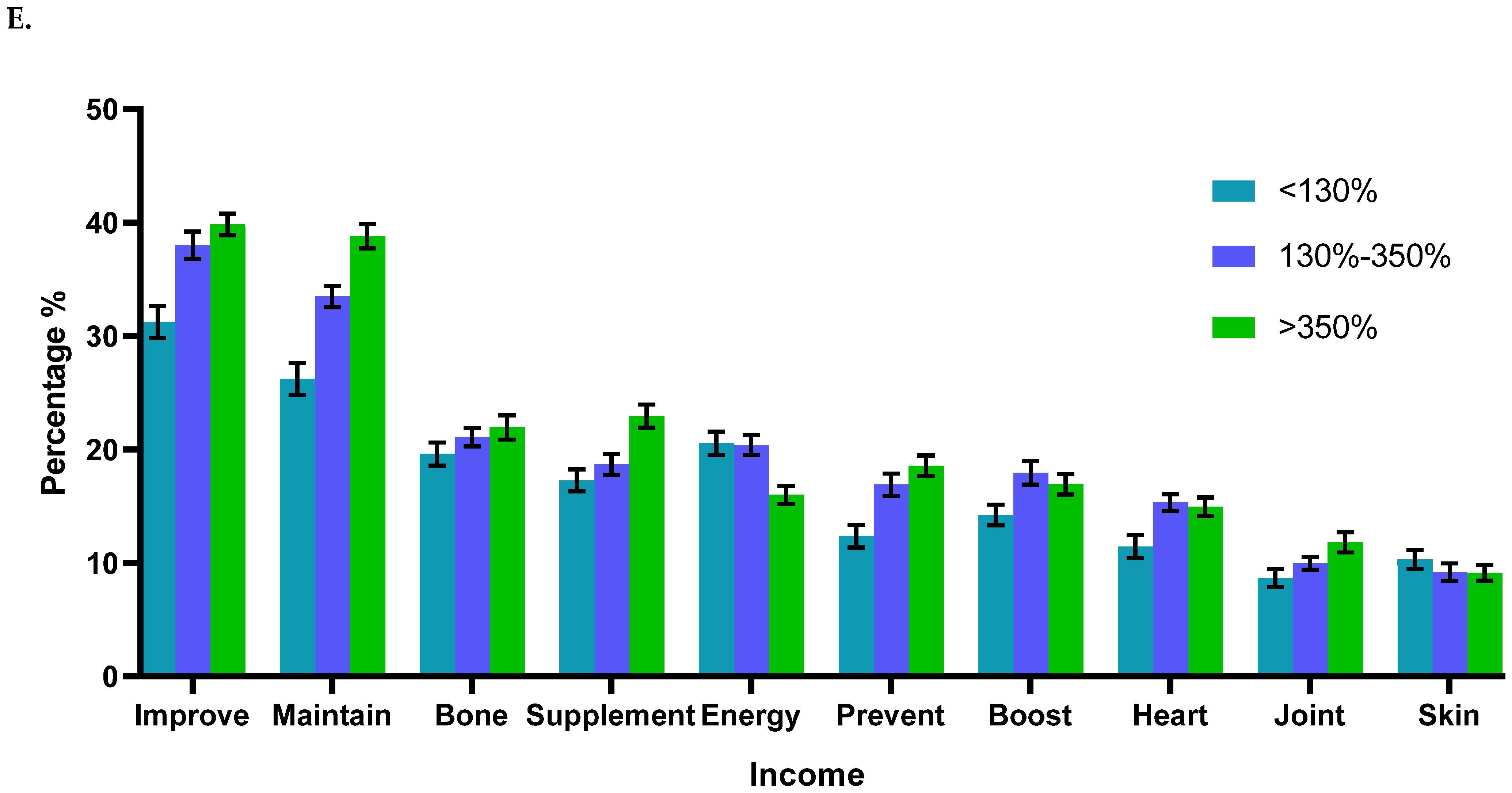
3.2.6. Effect of Income and Education Level on Reasons for Supplement Use
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Cowan, A.E.; Tooze, J.A.; Gahche, J.J.; A Eicher-Miller, H.; Guenther, P.M.; Dwyer, J.T.; Potischman, N.; Bhadra, A.; Carroll, R.J.; Bailey, R.L. Trends in Overall and Micronutrient-Containing Dietary Supplement Use in US Adults and Children, NHANES 2007–2018. J. Nutr. 2022, 152, 2789–2801. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Djaoudene, O.; Romano, A.; Bradai, Y.D.; Zebiri, F.; Ouchene, A.; Yousfi, Y.; Amrane-Abider, M.; Sahraoui-Remini, Y.; Madani, K. A Global Overview of Dietary Supplements: Regulation, Market Trends, Usage during the COVID-19 Pandemic, and Health Effects. Nutrients 2023, 15, 3320. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Soltani, A.; Jaam, M.; Nazar, Z.; Stewart, D.; Shaito, A. Attitudes and beliefs regarding the use of herbs and supplementary medications with COVID-19: A systematic review. Res. Soc. Adm. Pharm. 2022, 19, 343–355. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kantor, E.D.; Rehm, C.D.; Du, M.; White, E.; Giovannucci, E.L. Trends in Dietary Supplement Use Among US Adults From 1999-2012. JAMA 2016, 316, 1464–1474. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lordan, R. Dietary supplements and nutraceuticals market growth during the coronavirus pandemic—Implications for consumers and regulatory oversight. PharmaNutrition 2021, 18, 100282. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rautiainen, S.; Manson, J.E.; Lichtenstein, A.H.; Sesso, H.D. Dietary supplements and disease prevention—A global overview. Nat. Rev. Endocrinol. 2016, 12, 407–420. [Google Scholar] [CrossRef] [PubMed]
- Lentjes, M.A.H. The balance between food and dietary supplements in the general population. Proc. Nutr. Soc. 2018, 78, 97–109. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ronis, M.J.; Pedersen, K.B.; Watt, J. Adverse Effects of Nutraceuticals and Dietary Supplements. Annu. Rev. Pharmacol. Toxicol. 2017, 58, 583–601. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhang, F.F.; Barr, S.I.; McNulty, H.; Li, D.; Blumberg, J.B. Health effects of vitamin and mineral supplements. BMJ 2020, 369, m2511. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chen, F.; Du, M.; Blumberg, J.B.; Chui, K.K.H.; Ruan, M.; Rogers, G.; Shan, Z.; Zeng, L.; Zhang, F.F. Association Among Dietary Supplement Use, Nutrient Intake, and Mortality Among US Adults A Cohort Study. Ann. Intern. Med. 2019, 170, 604–613. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Force, U.P.S.T.; Mangione, C.M.; Barry, M.J.; Nicholson, W.K.; Cabana, M.; Chelmow, D.; Coker, T.R.; Davis, E.M.; Donahue, K.E.; Doubeni, C.A.; et al. Vitamin, Mineral, and Multivitamin Supplementation to Prevent Cardiovascular Disease and Cancer. JAMA 2022, 327, 2326–2333. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.L.; Gahche, J.J.; Miller, P.E.; Thomas, P.R.; Dwyer, J.T. Why US Adults Use Dietary Supplements. JAMA Intern. Med. 2013, 173, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Cowan, A.E.; Jun, S.; Gahche, J.J.; Tooze, J.A.; Dwyer, J.T.; Eicher-Miller, H.A.; Bhadra, A.; Guenther, P.M.; Potischman, N.; Dodd, K.W.; et al. Dietary Supplement Use Differs by Socioeconomic and Health-Related Characteristics among U.S. Adults, NHANES 2011–2014. Nutrients 2018, 10, 1114. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gardiner, P.; Graham, R.E.; Legedza, A.T.R.; Eisenberg, D.M.; Phillips, R.S. Factors Associated With Dietary Supplement Use Among Prescription Medication Users. Arch. Intern. Med. 2006, 166, 1968–1974. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, P.; Graham, R.; Legedza, A.T.R.; Ahn, A.C.; Eisenberg, D.M.; Phillips, R.S. Factors associated with herbal therapy use by adults in the United States. Altern. Ther. Health Med. 2007, 13, 22–29. [Google Scholar] [PubMed]
- Dickinson, A.; MacKay, D. Health habits and other characteristics of dietary supplement users: A review. Nutr. J. 2014, 13, 14. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dong, W.; Sun, Z.; Bai, R. Prevalence of and Factors Associated With Nutritional Supplement Use Among Older Chinese Adults: A Nationwide Cross-Sectional Study in China. Front. Public Health 2022, 10, 822087. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Foote, J.A.; Murphy, S.P.; Wilkens, L.R.; Hankin, J.H.; Henderson, B.E.; Kolonel, L.N. Factors Associated with Dietary Supplement Use among Healthy Adults of Five Ethnicities: The Multiethnic Cohort Study. Am. J. Epidemiol. 2003, 157, 888–897. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tan, E.C.K.; Eshetie, T.C.; Gray, S.L.; Marcum, Z.A. Dietary Supplement Use in Middle-aged and Older Adults. J. Nutr. Health Aging 2022, 26, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Congress, E.P.; Lyons, B.P. Cultural Differences in Health Beliefs: Implications for social work practice in health care settings. Soc. Work Health Care 1992, 17, 81–96. [Google Scholar] [CrossRef] [PubMed]
- van Lenthe, F.J.; Kamphuis, C.B.; A Beenackers, M.; Jansen, T.; Looman, C.W.; Nusselder, W.J.; Mackenbach, J.P. Cohort Profile: Understanding socioeconomic inequalities in health and health behaviours: The GLOBE study. Leuk. Res. 2013, 43, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S.; Stierman, B.; Gahche, J.J.; Potischman, N. Dietary Supplement Use Among Adults: United States, 2017–2018. NCHS Data Brief. 2021, 399, 1–8. [Google Scholar] [PubMed]
- Nichter, M.; Thompson, J.J. For my wellness, not just my illness: North Americans’ use of dietary supplements. Cult. Med. Psychiatry 2006, 30, 175–222. [Google Scholar] [CrossRef] [PubMed]
- Albright, C.L.; Schembre, S.M.; Steffen, A.D.; Wilkens, L.R.; Monroe, K.R.; Yonemori, K.M.; Murphy, S.P. Differences by Race/Ethnicity in Older Adults’ Beliefs about the Relative Importance of Dietary Supplements vs Prescription Medications: Results from the SURE Study. J. Acad. Nutr. Diet. 2012, 112, 1223–1229. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dickinson, A.; Blatman, J.; El-Dash, N.; Franco, J.C. Consumer Usage and Reasons for Using Dietary Supplements: Report of a Series of Surveys. J. Am. Coll. Nutr. 2014, 33, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, A.; Shao, A.; Boyon, N.; Franco, J.C. Use of dietary supplements by cardiologists, dermatologists and orthopedists: Report of a survey. Nutr. J. 2011, 10, 20. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dickinson, A.; Bonci, L.; Boyon, N.; Franco, J.C. Dietitians use and recommend dietary supplements: Report of a survey. Nutr. J. 2012, 11, 14. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Marra, M.V.; Bailey, R.L. Position of the Academy of Nutrition and Dietetics: Micronutrient Supplementation. J. Acad. Nutr. Diet. 2018, 118, 2162–2173. [Google Scholar] [CrossRef] [PubMed]
- Rooney, M.R.; Michos, E.D.; Hootman, K.C.; Harnack, L.; Lutsey, P.L. Trends in calcium supplementation, National Health and Nutrition Examination Survey (NHANES) 1999–2014. Bone 2018, 111, 23–27. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, D.; Rooney, M.R.; Burmeister, L.A.; Basta, N.E.; Lutsey, P.L. Trends in Daily Use of Biotin Supplements Among US Adults, 1999-2016. JAMA 2020, 324, 605–607. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Trepanowski, N.; Moore, K.J.; Kim, D.Y.; Hartman, R.I. Trends in hair, skin, and nails supplement use: Data from the National Health and Nutrition Examination Survey 2011-2020. J. Am. Acad. Dermatol. 2023, 89, 161–163. [Google Scholar] [CrossRef] [PubMed]
- Gooneratne, N.S.; Vitiello, M.V. Sleep in Older Adults: Normative changes, sleep disorders, and treatment options. Clin. Geriatr. Med. 2014, 30, 591–627. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Soenen, S.; Chapman, I.M. Body Weight, Anorexia, and Undernutrition in Older People. J. Am. Med. Dir. Assoc. 2013, 14, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Somers, V.K.; Xu, H.; Lopez-Jimenez, F.; Covassin, N. Trends in Use of Melatonin Supplements Among US Adults, 1999-2018. JAMA 2022, 327, 483–485. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chou, Y.-H.; Chen, Y.-M. Aging and Renal Disease: Old Questions for New Challenges. Aging Dis. 2021, 12, 515–528. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Curtis, E.; Litwic, A.; Cooper, C.; Dennison, E. Determinants of Muscle and Bone Aging. J. Cell. Physiol. 2015, 230, 2618–2625. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Flint, B.; Tadi, P. Physiology, Aging. [Updated 2023 January 4]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK556106/ (accessed on 10 April 2024).
- Maylahn, C.; Gohdes, D.M.; Balamurugan, A.; A Larsen, B. Age-related Eye Diseases: An Emerging Challenge for Public Health Professionals. Prev. Chronic Dis. 2005, 2, A17. [Google Scholar] [PubMed] [PubMed Central]
- Kini, V.; Ho, P.M. Interventions to Improve Medication Adherence: A Review. JAMA 2018, 320, 2461–2473. [Google Scholar] [CrossRef] [PubMed]
- Sadovsky, R.; Collins, N.; Tighe, A.P.; Brunton, S.A.; Safeer, R. Patient use of dietary supplements: A clinician’s perspective. Curr. Med. Res. Opin. 2008, 24, 1209–1216. [Google Scholar] [CrossRef] [PubMed]
- Tarn, D.M.; Paterniti, D.A.; Good, J.S.; Coulter, I.D.; Galliher, J.M.; Kravitz, R.L.; Karlamangla, A.S.; Wenger, N.S. Physician–patient communication about dietary supplements. Patient Educ. Couns. 2013, 91, 287–294. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tarn, D.M.; Karlamangla, A.; Coulter, I.D.; Paterniti, D.A.; Knox, L.; Khang, P.S.; Hui, K.-K.; Wenger, N.S. A cross-sectional study of provider and patient characteristics associated with outpatient disclosures of dietary supplement use. Patient Educ. Couns. 2015, 98, 830–836. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chiba, T.; Tanemura, N. Differences in the Perception of Dietary Supplements between Dietary Supplement/Medicine Users and Non-Users. Nutrients 2022, 14, 4114. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N (%) | |||||
|---|---|---|---|---|---|
| 2011–2012 (n = 2947) | 2013–2014 (n = 3059) | 2015–2016 (n = 3179) | 2017–2018 (n = 3344) | Overall (n = 12,529) | |
| Sex | |||||
| Male | 1295 (43.9) | 1305 (42.7) | 1402 (44.1) | 1496 (44.7) | 5498 (43.9) |
| Female | 1652 (56.1) | 1754 (57.3) | 1777 (55.9) | 1848 (55.3) | 7031 (56.1) |
| Age range, y | |||||
| 20–39 | 808 (27.4) | 760 (24.8) | 792 (24.9) | 727 (21.7) | 3087 (24.6) |
| 40–64 | 1273 (43.2) | 1377 (45.0) | 1383 (43.5) | 1460 (43.7) | 5493 (43.8) |
| 65–79 | 604 (20.5) | 646 (21.1) | 717 (22.6) | 814 (24.3) | 2781 (22.2) |
| ≥80 | 262 (8.9) | 276 (9.0) | 287 (9.0 | 343 (10.3) | 1168 (9.3) |
| Race/ethnicity | |||||
| Hispanic | 458 (15.5) | 572 (18.7) | 852 (26.8) | 665 (19.9) | 2547 (20.3) |
| Non-Hispanic White | 1296 (44.0) | 1512 (49.4) | 1217 (38.3) | 1317 (39.4) | 5342 (42.6) |
| Non-Hispanic Black | 687 (23.3) | 512 (16.7) | 601 (18.9) | 708 (21.2) | 2508 (20.0) |
| Non-Hispanic Asian | 415 (14.1) | 381 (12.5) | 393 (12.4) | 477 (14.3) | 1666 (13.3) |
| Other Races | 91 (3.1) | 82 (2.7) | 116 (3.6) | 177 (5.3) | 466 (3.7) |
| Education level | |||||
| <High school | 550 (18.7) | 515 (16.8) | 598 (18.8) | 533 (15.9) | 2196 (17.5) |
| High school | 562 (19.2) | 648 (21.2) | 631 (19.8) | 739 (22.1) | 2583 (20.6) |
| Some college | 916 (31.1) | 966 (31.6) | 994 (31.3) | 1144 (34.2) | 4016 (32.1) |
| ≥College | 913 (31.0) | 928 (30.3) | 953 (30.1) | 928 (27.8) | 3731 (29.7) |
| Poverty income ratio | |||||
| <130% | 828 (30.6) | 793 (27.9) | 735 (26.1) | 683 (23.6) | 3039 (27.0) |
| 130–350% | 889 (32.8) | 984 (34.7) | 1140 (40.5) | 1197 (41.3) | 4210 (37.4) |
| >350% | 990 (36.6) | 1062 (37.4) | 938 (33.3) | 1016 (35.1) | 4006 (35.6) |
| Quantity of Supplement Taken Daily | Days Any Supplement Taken in the Past 30 Days | Days Any Supplement Has Been Taken | ||||
|---|---|---|---|---|---|---|
| Median [IQR] | p-Value | Median [IQR] | p-Value | Median [IQR] | p-Value | |
| Sex | ||||||
| Men | 2.00 [1.00, 4.00] | Reference | 30 [15, 30] | Reference | 1095 [365, 3650] | Reference |
| Women | 2.00 [1.00, 4.25] | <0.001 | 30 [16.25, 30] | <0.001 | 1095 [274, 3650] | 0.453 |
| Race/ethnicity | ||||||
| Non-Hispanic White | 2.00 [1.00, 4.00] | Reference | 30 [20, 30] | Reference | 1825 [547, 4745] | Reference |
| Hispanic | 3.00 [1.00, 5.00] | <0.001 | 30 [15, 30] | <0.001 | 547 [91, 1825] | <0.001 |
| Non-Hispanic Black | 2.00 [1.00, 3.00] | 0.30473 | 30 [15, 30] | <0.001 | 730 [182, 2190] | <0.001 |
| Non-Hispanic Asian | 2.00 [1.00, 4.00] | 0.73291 | 30 [15, 30] | 0.0405 | 730 [182, 1825] | <0.001 |
| Other Races | 2.00 [1.00, 5.00] | 0.00211 | 30 [12, 30] | 0.0372 | 1095 [365, 3650] | 0.0316 |
| Age, y | ||||||
| 20–39 | 2.00 [1.00, 4.00] | Reference | 20 [7, 30] | Reference | 365 [91, 1460] | Reference |
| 40–64 | 2.00 [1.00, 4.00] | <0.001 | 30 [15, 30] | <0.001 | 1095 [365, 3650] | <0.001 |
| 65–79 | 3.00 [1.00, 5.00] | <0.001 | 30 [30, 30] | <0.001 | 1825 [730, 5475] | <0.001 |
| ≥80 | 3.00 [1.00, 5.00] | <0.001 | 30 [30, 30] | <0.001 | 3650 [730, 7300] | <0.001 |
| Education level | ||||||
| Less than high school | 2.00 [1.00, 3.00] | Reference | 30 [15, 30] | Reference | 730 [122, 2190] | Reference |
| High school | 2.00 [1.00, 4.00] | <0.001 | 30 [15, 30] | 0.684 | 1095 [274, 3650] | <0.001 |
| Some college | 2.00 [1.00, 4.00] | <0.001 | 30 [15, 30] | 0.975 | 1095 [365, 3650] | <0.001 |
| ≥College | 2.38 [1.00, 5.00] | <0.001 | 30 [15, 30] | 0.335 | 1460 [365, 3650] | <0.001 |
| Poverty income ratio | ||||||
| <130% | 2.00 [1.00, 3.00] | Reference | 30 [14, 30] | Reference | 365 [91, 1825] | Reference |
| 130–350% | 2.00 [1.00, 4.00] | <0.001 | 30 [15, 30] | 0.00125 | 730 [182, 2555] | <0.001 |
| >350% | 2.00 [1.00, 4.00] | <0.001 | 30 [15, 30] | <0.001 | 1095 [365, 3650] | <0.001 |
| % (SE) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Reason | Improve Overall Health | Maintain Health | Bone Health | Supplement the Diet | Enhanced Energy | Prevent Health Problems | Boost Immune System | Heart Health | Joint Health | Skin, Hair, and Nail |
| Overall | 37.3 (0.7) | 34.7 (0.8) | 21.4 (0.6) | 20.3 (0.6) | 18.1 (0.5) | 16.7 (0.7) | 16.3 (0.6) | 14.2 (0.5) | 10.5 (0.5) | 9.4 (0.5) |
| Sex | ||||||||||
| Men | 38.5 (1.0) | 36.2 (1.2) | 12.4 (0.8) | 19.4 (0.7) | 16.6 (0.7) | 17.3 (0.9) | 17.2 (0.8) | 14.4 (0.7) | 9.7 (0.8) | 4.2 (0.4) |
| Women | 36.3 (0.7) | 33.6 (1.1) | 28.4 (0.8) | 21.1 (0.8) | 19.2 (0.6) | 16.1 (0.7) | 15.6 (0.7) | 14.1 (0.6) | 13.5 (0.8) | 11.1 (0.6) |
| Age range, y | ||||||||||
| 20–39 | 35.3 (1.2) | 34.1 (1.4) | 9.1 (0.7) | 20.4 (0.9) | 20.7 (0.8) | 15.5 (0.8) | 17.8 (1.0) | 5.7 (0.5) | 6.9 (0.5) | 11.2 (0.7) |
| 40–64 | 37.3 (1.0) | 34.2 (1.1) | 20.8 (0.9) | 20.3 (0.9) | 18.0 (0.7) | 16.6 (1.0) | 16.4 (0.8) | 14.9 (0.7) | 10.5 (0.7) | 9.2 (0.7) |
| 65–79 | 40.3 (1.4) | 36.8 (1.7) | 35.9 (1.7) | 20.6 (1.3) | 16.2 (1.0) | 19.4 (1.3) | 16.0 (1.0) | 23.9 (1.4) | 14.9 (1.2) | 8.9 (1.0) |
| ≥80 | 36.3 (1.5) | 35.1 (1.5) | 35.1 (1.6) | 19.3 (1.8) | 13.0 (1.4) | 13.8 (1.6) | 10.3 (1.2) | 16.4 (1.5) | 12.6 (1) | 5.1 (0.7) |
| Race/ethnicity | ||||||||||
| Non-Hispanic White | 39.2 (0.8) | 36.0 (1.0) | 21.7 (0.7) | 21.1 (0.7) | 16.2 (0.6) | 17.5 (0.9) | 16.3 (0.8) | 15 (0.7) | 10.8 (0.7) | 8.7 (0.6) |
| Non-Hispanic Black | 34.6 (1.0) | 31.2 (1.3) | 19.1 (1.1) | 18.4 (1.2) | 27.0 (1.1) | 15.1 (1) | 17.5 (0.8) | 12.1 (0.7) | 9.2 (0.7) | 12.6 (0.9) |
| Hispanic | 29.4 (1.2) | 28.3 (1.1) | 20.3 (0.9) | 16.4 (0.9) | 24.6 (1.0) | 13.6 (1.0) | 15.0 (1) | 10.5 (0.9) | 8.8 (0.6) | 11.4 (0.8) |
| Asian | 35.3 (1.5) | 37.4 (1.0) | 22.9 (1.4) | 20.9 (1.3) | 12.7 (0.9) | 13.4 (0.9) | 12.5 (0.9) | 14 (0.9) | 10.4 (0.9) | 10.1 (0.9) |
| Other races | 33.1 (2.8) | 35.1 (3.5) | 22.8 (3.4) | 21.7 (2.6) | 20.8 (2.5) | 17.6 (2.6) | 24.3 (3.5) | 16.5 (2.3) | 12.2 (1.8) | 9.2 (1.6) |
| Education | ||||||||||
| <High school | 25.3 (1.4) | 25.4 (1.6) | 22.1 (1.1) | 14.4 (0.9) | 20.3 (1.2) | 11.4 (1.2) | 11.5 (1.3) | 11.4 (1.3) | 8.5 (0.7) | 6.6 (0.6) |
| High school | 36.2 (1.3) | 30.0 (1.4) | 22.3 (1.3) | 17.4 (1) | 19.4 (1.0) | 13.4 (0.9) | 14.0 (1.3) | 15.3 (1.2) | 10.1 (1.0) | 9.2 (1.2) |
| Some college | 39.1 (1.2) | 33.8 (1.2) | 19.7 (0.8) | 20.1 (1) | 19.1 (0.8) | 16.7 (0.9) | 17.5 (0.9) | 14.3 (0.7) | 11.4 (0.8) | 10.5 (0.7) |
| ≥College | 39.6 (1.1) | 40.9 (1.1) | 22.2 (1.0) | 23.8 (0.9) | 15.9 (0.9) | 20 (1.0) | 17.9 (1) | 14.4 (0.8) | 10.5 (0.8) | 9.3 (0.6) |
| Poverty income ratio | ||||||||||
| <130% | 31.2 (1.4) | 26.2 (1.4) | 19.6 (1.0) | 17.3 (1) | 20.5 (1.1) | 12.4 (1.0) | 14.2 (0.9) | 11.5 (1) | 8.7 (0.8) | 10.3 (0.8) |
| 130–350% | 38 (1.2) | 33.5 (0.9) | 21.1 (0.8) | 18.7 (0.9) | 20.4 (0.9) | 16.9 (1) | 18 (1.0) | 15.3 (0.7) | 10 (0.6) | 9.2 (0.8) |
| >350% | 39.8 (1.0) | 38.8 (1.1) | 22 (1.1) | 23 (1) | 16 (0.8) | 18.6 (0.9) | 16.9 (0.9) | 15 (0.8) | 11.8 (0.9) | 9.1 (0.7) |
| % (SE) | ||||||
|---|---|---|---|---|---|---|
| Self-Initiated Decision | Doctors’ Recommendation | |||||
| Overall | Male | Female | Overall | Male | Female | |
| To prevent health problems | 20.7 (0.8) | 21.1 (1) | 20.3 (1) | 18.1 (1) a | 20.4 (1.6) | 16.9 (1.1) c |
| To improve overall health | 46.6 (0.8) | 47.8 (1.1) | 45.5 (1) | 37.7 (0.9) a | 39.9 (1.8) | 36.6 (1.1) |
| To supplement diet | 23.5 (0.8) | 22.6 (1) | 24.2 (1) | 24.8 (1) | 23.9 (1.5) | 25.2 (1.2) |
| To maintain health | 43.4 (0.8) | 45.3 (1.4) | 41.8 (1.1) | 36.1 (1.4) a | 39.5 (1.7) | 34.4 (1.7) c |
| boost immune system | 21.7 (0.8) | 22.3 (1) | 21.1 (1) | 14.6 (0.6) a | 16.2 (1.3) | 13.8 (0.8) |
| For heart health, cholesterol | 16.8 (0.6) | 16.7 (0.9) | 16.9 (0.8) | 22.2 (0.9) a | 24.8 (1.7) | 20.9 (1) c |
| For healthy joints, arthritis | 13.5 (0.7) | 12.7 (0.9) | 14.2 (0.7) | 13.6 (0.9) | 12.5 (1.4) | 14.2 (1) |
| For healthy skin, hair, and nails | 12.5 (0.7) | 5.5 (0.5) | 18.3 (1) b | 10.4 (0.7) a | 4.1 (0.6) | 13.5 (1) c |
| For bone health | 22.8 (0.7) | 13.6 (0.9) | 30.5 (1) b | 35.4 (1.1) a | 20.5 (1.6) | 42.9 (1.3) c |
| To get more energy | 23.2 (0.7) | 21.3 (0.9) | 24.8 (0.8) b | 16.5 (0.9) a | 14.3 (1.3) | 17.7 (1.0) c |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, L.; Tao, H.; Xu, J.; Liu, L.; Nahata, M.C. Quantity, Duration, Adherence, and Reasons for Dietary Supplement Use among Adults: Results from NHANES 2011–2018. Nutrients 2024, 16, 1830. https://doi.org/10.3390/nu16121830
Liu L, Tao H, Xu J, Liu L, Nahata MC. Quantity, Duration, Adherence, and Reasons for Dietary Supplement Use among Adults: Results from NHANES 2011–2018. Nutrients. 2024; 16(12):1830. https://doi.org/10.3390/nu16121830
Chicago/Turabian StyleLiu, Ligang, Heqing Tao, Jinyu Xu, Lijun Liu, and Milap C. Nahata. 2024. "Quantity, Duration, Adherence, and Reasons for Dietary Supplement Use among Adults: Results from NHANES 2011–2018" Nutrients 16, no. 12: 1830. https://doi.org/10.3390/nu16121830
APA StyleLiu, L., Tao, H., Xu, J., Liu, L., & Nahata, M. C. (2024). Quantity, Duration, Adherence, and Reasons for Dietary Supplement Use among Adults: Results from NHANES 2011–2018. Nutrients, 16(12), 1830. https://doi.org/10.3390/nu16121830