
The Relationship between Low-Sodium Salt Intake and Both Blood Pressure Level and Hypertension in Chinese Residents

Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Measurement of Low-Sodium Salt Intake
2.3. Definition of Hypertension
2.4. Covariates
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics of the Study Populations
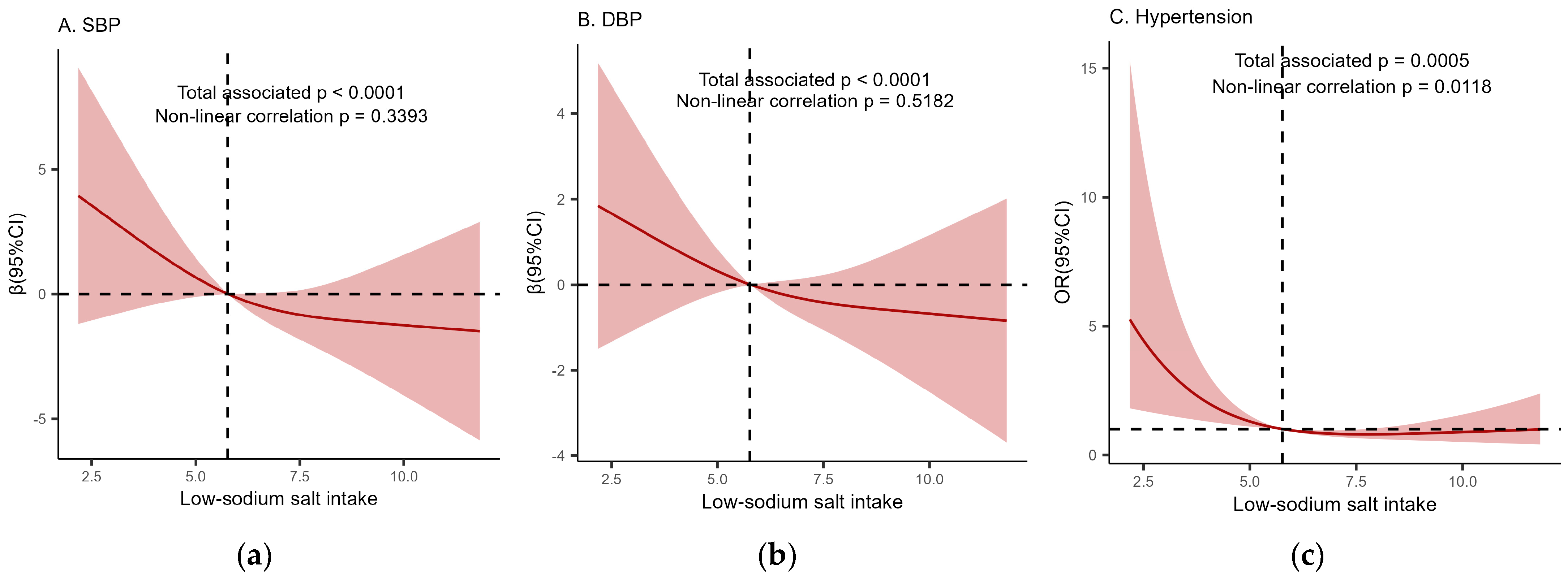
3.2. The Relationship between Low-Sodium Salt Intake and Both SBP and DBP
3.3. The Relationship between Low-Sodium Salt Intake and Hypertension
3.4. Exploratory Subgroup Analyses
3.5. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization Hypertension. Available online: https://www.who.int/news-room/fact-sheets/detail/hypertension (accessed on 2 May 2024).
- Global Report on Hypertension: The Race Against a Silent Killer. Available online: https://www.who.int/publications-detail-redirect/9789240081062 (accessed on 2 May 2024).
- GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Wang, Z.; Fan, J.; Hu, S. Epidemiology and Management of Hypertension in China: An Analysis Using Data from the Annual Report on Cardiovascular Health and Diseases in China (2021). Zhongguo Quan Ke Yi Xue 2022, 25, 3715–3720. [Google Scholar]
- Wang, Z.; Chen, Z.; Zhang, L.; Wang, X.; Hao, G.; Zhang, Z.; Shao, L.; Tian, Y.; Dong, Y.; Zheng, C.; et al. Status of Hypertension in China: Results From the China Hypertension Survey, 2012–2015. Circulation 2018, 137, 2344–2356. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1859–1922. [Google Scholar] [CrossRef]
- Joint Committee for Guideline Revision. 2018 Chinese Guidelines for Prevention and Treatment of Hypertension-A report of the Revision Committee of Chinese Guidelines for Prevention and Treatment of Hypertension. J. Geriatr. Cardiol. 2019, 16, 182–241. [Google Scholar] [CrossRef]
- Xu, A.; Ma, J.; Guo, X.; Wang, L.; Wu, J.; Zhang, J.; Bai, Y.; Xu, J.; Lu, Z.; Xu, Z.; et al. Association of a Province-Wide Intervention With Salt Intake and Hypertension in Shandong Province, China, 2011–2016. JAMA Intern. Med. 2020, 180, 877–886. [Google Scholar] [CrossRef] [PubMed]
- Sacks, F.M.; Svetkey, L.P.; Vollmer, W.M.; Appel, L.J.; Bray, G.A.; Harsha, D.; Obarzanek, E.; Conlin, P.R.; Miller, E.R.; Simons-Morton, D.G.; et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N. Engl. J. Med. 2001, 344, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Moran, A.E.; Liu, J.; Qi, Y.; Xie, W.; Tzong, K.; Zhao, D. A Meta-Analysis of Effect of Dietary Salt Restriction on Blood Pressure in Chinese Adults. Glob. Heart 2015, 10, 291–299.e6. [Google Scholar] [CrossRef]
- Elliott, P.; Stamler, J.; Nichols, R.; Dyer, A.R.; Stamler, R.; Kesteloot, H.; Marmot, M. Intersalt revisited: Further analyses of 24 hour sodium excretion and blood pressure within and across populations. Intersalt Cooperative Research Group. BMJ 1996, 312, 1249–1253. [Google Scholar] [CrossRef]
- Emamian, M.H.; Ebrahimi, H.; Hashemi, H.; Fotouhi, A. Salt intake and blood pressure in Iranian children and adolescents: A population-based study. BMC Cardiovasc. Disord. 2021, 21, 62. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Li, J.; Macgregor, G.A. Effect of longer term modest salt reduction on blood pressure: Cochrane systematic review and meta-analysis of randomised trials. BMJ 2013, 346, f1325. [Google Scholar] [CrossRef] [PubMed]
- Yin, X.; Liu, H.; Webster, J.; Trieu, K.; Huffman, M.D.; Miranda, J.J.; Marklund, M.; Wu, J.H.Y.; Cobb, L.K.; Li, K.C.; et al. Availability, Formulation, Labeling, and Price of Low-sodium Salt Worldwide: Environmental Scan. JMIR Public Health Surveill. 2021, 7, e27423. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Jin, A.; Neal, B.; Feng, X.; Qiao, Q.; Wang, H.; Zhang, R.; Li, J.; Duan, P.; Cao, L.; et al. Salt substitution and salt-supply restriction for lowering blood pressure in elderly care facilities: A cluster-randomized trial. Nat. Med. 2023, 29, 973–981. [Google Scholar] [CrossRef] [PubMed]
- China Salt Substitute Study Collaborative Group. Salt substitution: A low-cost strategy for blood pressure control among rural Chinese. A randomized, controlled trial. J. Hypertens. 2007, 25, 2011–2018. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Bai, Y.; Lu, Z.; Zhang, X.; Yin, Z.; Zuo, H.; Xu, C.; Xu, J.; Guo, X.; Ma, J. The influencing of reducing salt intervention on condiment salt intake in self-reported adult hypertension patients (18–69 years old) of Shandong Province. Zhongguo Man Xing Bing Yu Fang Yu Kong Zhi 2020, 28, 570–573. [Google Scholar] [CrossRef]
- Lu, Z.; Zhang, X.; Li, J.; Zhang, J.; Zhao, W.; Ma, J.; Guo, X.; Yan, L.; Chu, J.; Xu, A. [Dietary sodium intakes and resources among residents in Shandong province]. Zhonghua Yu Fang Yi Xue Za Zhi 2014, 48, 7–11. [Google Scholar] [PubMed]
- Joint Committee on the Development of Guidelines for the Prevention and Treatment of Dyslipidemia in Adults in China. Chinese guidelines for the prevention and treatment of dyslipidemia in adults. Zhonghua Xin Xue Guan Bing Za Zhi 2007, 35, 390–419. [Google Scholar]
- Chinese Medical Association Diabetes Section. Guideline for the Prevention and Treatment of Type 2 Diabetes Mellitus in China (2020 Edition). Zhonghua Tang Niao Bing Za Zhi 2021, 13, 315–409. [Google Scholar]
- Chinese Nutrition Society Obesity Prevention and Control Section; Chinese Nutrition Society Clinical Nutrition Section; Chinese Preventive Medicine Association Behavioral Health Section; Chinese Preventive Medicine Association Sports and Health Section. [Expert Consensus on Obesity Prevention and Treatment in China]. Zhonghua Liu Xing Bing Xue Za Zhi 2022, 43, 609–626. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Cogswell, M.E.; Gillespie, C.; Fang, J.; Loustalot, F.; Dai, S.; Carriquiry, A.L.; Kuklina, E.V.; Hong, Y.; Merritt, R.; et al. Association between usual sodium and potassium intake and blood pressure and hypertension among U.S. adults: NHANES 2005–2010. PLoS ONE 2013, 8, e75289. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.; Chen, Y.; Gong, R.; Wang, L. Dietary Sodium and Potassium Intake and Hypertension. Sheng Li Ke Xue Jin Zhan 2023, 54, 235–239. [Google Scholar] [CrossRef]
- Liu, M.; Xu, J.W.; Li, Y.; Zhang, P.H.; Bai, Y.M.; Ji, N.; Wang, S.Q.; Wu, J. 24 hours urinary sodium and potassium excretion and association with blood pressure among people aged 18-75 years old in six Chinese provinces. Zhonghua Yu Fang Yi Xue Za Zhi 2021, 55, 1299–1304. [Google Scholar] [CrossRef] [PubMed]
- Nomura, N.; Shoda, W.; Uchida, S. Clinical importance of potassium intake and molecular mechanism of potassium regulation. Clin. Exp. Nephrol. 2019, 23, 1175–1180. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Tian, M.; Yu, J.; Li, Q.; Liu, Y.; Yin, X.; Wu, J.H.; Marklund, M.; Wu, Y.; Li, N.; et al. Interim effects of salt substitution on urinary electrolytes and blood pressure in the China Salt Substitute and Stroke Study (SSaSS). Am. Heart J. 2020, 221, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Wang, H.-L.; Wang, W.-L.; Wu, X.-M.; Fu, L.-Y.; Shi, J.-P. Long-term effects of salt substitution on blood pressure in a rural north Chinese population. J. Hum. Hypertens. 2013, 27, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Liu, J.-X.; Shi, R.; Yang, N.; Song, D.-L.; Pang, W.; Li, Y.-M. Compound ion salt, a novel low-sodium salt substitute: From animal study to community-based population trial. Am. J. Hypertens. 2009, 22, 934–942. [Google Scholar] [CrossRef] [PubMed]
- Barros, C.L.d.A.; Sousa, A.L.L.; Chinem, B.M.; Rodrigues, R.B.; Jardim, T.S.V.; Carneiro, S.B.; Souza, W.K.S.B.d.; Jardim, P.C.B.V. Impact of light salt substitution for regular salt on blood pressure of hypertensive patients. Arq. Bras. Cardiol. 2015, 104, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Yin, X.; Li, X.; Yan, L.L.; Lam, C.T.; Li, S.; He, F.; Xie, W.; Sang, B.; Luobu, G.; et al. Using a low-sodium, high-potassium salt substitute to reduce blood pressure among Tibetans with high blood pressure: A patient-blinded randomized controlled trial. PLoS ONE 2014, 9, e110131. [Google Scholar] [CrossRef] [PubMed]
- Graudal, N.; Hubeck-Graudal, T.; Jürgens, G.; Taylor, R.S. Dose-response relation between dietary sodium and blood pressure: A meta-regression analysis of 133 randomized controlled trials. Am. J. Clin. Nutr. 2019, 109, 1273–1278. [Google Scholar] [CrossRef]
- Schiffrin, E.L. How Structure, Mechanics, and Function of the Vasculature Contribute to Blood Pressure Elevation in Hypertension. Can. J. Cardiol. 2020, 36, 648–658. [Google Scholar] [CrossRef] [PubMed]
- Li, S.C.; Wang, Q.H.; Chen, L.F.; Feng, S.Y.; Wu, Y.X.; Yan, X.W. High Sodium Intake Impairs Small Artery Vasoreactivity in vivo in Dahl Salt-Sensitive Rats. J. Vasc. Res. 2019, 56, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Geleijnse, J.M.; Witteman, J.C.; Bak, A.A.; den Breeijen, J.H.; Grobbee, D.E. Reduction in blood pressure with a low sodium, high potassium, high magnesium salt in older subjects with mild to moderate hypertension. BMJ 1994, 309, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Frisoli, T.M.; Schmieder, R.E.; Grodzicki, T.; Messerli, F.H. Salt and hypertension: Is salt dietary reduction worth the effort? Am. J. Med. 2012, 125, 433–439. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; MacGregor, G.A. Effect of modest salt reduction on blood pressure: A meta-analysis of randomized trials. Implications for public health. J. Hum. Hypertens. 2002, 16, 761–770. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Zhao, L.; Thompson, B.; Zhang, Y.; Wu, Y. Effects of salt substitute on home blood pressure differs according to age and degree of blood pressure in hypertensive patients and their families. Clin. Exp. Hypertens. 2018, 40, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Webster, J.; Fu, L.-Y.; Wang, H.-L.; Wu, X.-M.; Wang, W.-L.; Shi, J.-P. Intake of low sodium salt substitute for 3years attenuates the increase in blood pressure in a rural population of North China—A randomized controlled trial. Int. J. Cardiol. 2016, 215, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Kim, K.; Shin, M.-H.; Shin, D.H.; Lee, Y.-H.; Chun, B.-Y.; Choi, B.Y. The relationship of dietary sodium, potassium, fruits, and vegetables intake with blood pressure among Korean adults aged 40 and older. Nutr. Res. Pract. 2014, 8, 453–462. [Google Scholar] [CrossRef] [PubMed]
- Stolarz-Skrzypek, K.; Bednarski, A.; Czarnecka, D.; Kawecka-Jaszcz, K.; Staessen, J.A. Sodium and potassium and the pathogenesis of hypertension. Curr. Hypertens. Rep. 2013, 15, 122–130. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | Low-Sodium Salt Intake | p-Value 1 | |||
|---|---|---|---|---|---|
| Total Cases | Q1 (<4.72 g/d) | Q2 (4.72–6.88 g/d) | Q3 (≥6.88 g/d) | ||
| Number of participants, N | 350 | 116 | 114 | 120 | |
| Salt intake (mean (SD)) | 8.67 (4.24) | 5.62 (2.42) | 8.13 (2.33) | 12.15 (4.51) | <0.001 |
| Low-sodium salt intake (mean (SD)) | 6.16 (2.92) | 3.47 (0.83) | 5.77 (0.61) | 9.14 (2.79) | <0.001 |
| SBP (mean (SD)) | 119.76 (17.77) | 121.99 (22.44) | 120.01 (17.04) | 117.37 (12.38) | 0.134 |
| DBP (mean (SD)) | 76.43 (11.76) | 78.34 (14.17) | 76.07 (11.62) | 74.93 (8.82) | 0.078 |
| Hypertension, N% | |||||
| No | 302 (86.3) | 92 (79.3) | 97 (85.1) | 113 (94.2) | 0.004 |
| Yes | 48 (13.7) | 24 (20.7) | 17 (14.9) | 7 (5.8) | |
| Age (mean (SD)) | 40.85 (12.49) | 40.80 (11.69) | 41.24 (12.65) | 40.52 (13.15) | 0.907 |
| Age groups, N% | |||||
| 17–44 years old | 206 (58.9) | 68 (58.6) | 64 (56.1) | 74 (61.7) | 0.690 |
| 45–70 years old | 144 (41.1) | 48 (41.4) | 50 (43.9) | 46 (38.3) | |
| Gender, N% | |||||
| Female | 171 (48.9) | 68 (58.6) | 55 (48.2) | 48 (40.0) | 0.016 |
| Male | 179 (51.1) | 48 (41.4) | 59 (51.8) | 72 (60.0) | |
| Region, N% | |||||
| Urban | 133 (38.0) | 49 (42.2) | 44 (38.6) | 40 (33.3) | 0.366 |
| Rural | 217 (62.0) | 67 (57.8) | 70 (61.4) | 80 (66.7) | |
| Marital status, N% | |||||
| Unmarried 2 | 42 (12.0) | 16 (13.8) | 9 (7.9) | 17 (14.2) | 0.258 |
| Married | 308 (88.0) | 100 (86.2) | 105 (92.1) | 103 (85.8) | |
| Educational level, N% | |||||
| Primary and below | 105 (30.0) | 32 (27.6) | 33 (28.9) | 40 (33.3) | 0.829 |
| Junior high school | 153 (43.7) | 51 (44.0) | 53 (46.5) | 49 (40.8) | |
| High school and above | 92 (26.3) | 33 (28.4) | 28 (24.6) | 31 (25.8) | |
| Income 3, N% | |||||
| ≥¥0, ≤¥5000 | 102 (30.0) | 30 (26.3) | 38 (34.5) | 34 (29.3) | 0.678 |
| >¥5000, ≤¥10,000 | 101 (29.7) | 35 (30.7) | 29 (26.4) | 37 (31.9) | |
| >¥10,000, ≤¥15,000 | 59 (17.4) | 19 (16.7) | 17 (15.5) | 23 (19.8) | |
| >¥15,000 | 78 (22.9) | 30 (26.3) | 26 (23.6) | 22 (19.0) | |
| BMI (mean (SD)) | 24.76 (4.08) | 25.32 (4.10) | 24.88 (4.43) | 24.11 (3.63) | 0.071 |
| BMI groups, N% | |||||
| <24 kg/m2 | 156 (44.6) | 48 (41.4) | 50 (43.9) | 58 (48.3) | 0.407 |
| ≥24 kg/m2, <28 kg/m2 | 128 (36.6) | 40 (34.5) | 43 (37.7) | 45 (37.5) | |
| ≥28 kg/m2 | 66 (18.9) | 28 (24.1) | 21 (18.4) | 17 (14.2) | |
| Smoking status, N% | |||||
| No | 252 (72.0) | 92 (79.3) | 85 (74.6) | 75 (62.5) | 0.012 |
| Yes | 98 (28.0) | 24 (20.7) | 29 (25.4) | 45 (37.5) | |
| Drinking status, N% | |||||
| No | 217 (62.0) | 82 (70.7) | 66 (57.9) | 69 (57.5) | 0.062 |
| Yes | 133 (38.0) | 34 (29.3) | 48 (42.1) | 51 (42.5) | |
| Physical exercise, N% | |||||
| No | 243 (69.4) | 75 (64.7) | 88 (77.2) | 80 (66.7) | 0.086 |
| Yes | 107 (30.6) | 41 (35.3) | 26 (22.8) | 40 (33.3) | |
| Dyslipidemia, N% | |||||
| No | 239 (68.3) | 77 (66.4) | 73 (64.0) | 89 (74.2) | 0.216 |
| Yes | 111 (31.7) | 39 (33.6) | 41 (36.0) | 31 (25.8) | |
| Diabetes, N% | |||||
| No | 331 (94.6) | 110 (94.8) | 106 (93.0) | 115 (95.8) | 0.623 |
| Yes | 19 (5.4) | 6 (5.2) | 8 (7.0) | 5 (4.2) | |
| Center obesity, N% | |||||
| No | 203 (58.0) | 60 (51.7) | 67 (58.8) | 76 (63.3) | 0.192 |
| Yes | 147 (42.0) | 56 (48.3) | 47 (41.2) | 44 (36.7) | |
| Outcome | Low-Sodium Salt | p-Value for 1 g Increment | |||
|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Per 1 g Increment | ||
| SBP | |||||
| Model 1 | Ref | −1.980 (−6.576, 2.616) | −4.616 (−9.154, −0.079) | −0.517 (−1.157, 0.123) | 0.113 |
| Model 2 | Ref | −3.476 (−7.941, 0.989) | −6.884 (−11.329, −2.439) | −0.739 (−1.359, −0.120) | 0.020 |
| Model 3 | Ref | −2.829 (−7.036, 1.379) | −5.051 (−9.244, −0.858) | −0.488 (−1.072, 0.096) | 0.101 |
| Model 4 | Ref | −3.112 (−7.282, 1.058) | −4.997 (−9.136, −0.858) | −0.460 (−1.037, 0.116) | 0.117 |
| DBP | |||||
| Model 1 | Ref | −2.263 (−5.301, 0.775) | −3.406 (−6.405, −0.407) | −0.377 (−0.801, 0.046) | 0.081 |
| Model 2 | Ref | −3.124 (−6.166, −0.083) | −4.412 (−7.439, −1.384) | −0.472 (−0.894, −0.050) | 0.028 |
| Model 3 | Ref | −2.755 (−5.485, −0.025) | −2.755 (−5.476, −0.035) | −0.252 (−0.631, 0.127) | 0.192 |
| Model 4 | Ref | −2.843 (−5.552, −0.133) | −2.683 (−5.372, 0.006) | −0.233 (−0.608, 0.142) | 0.222 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.; Lu, Z.; Zhang, J.; Chen, X.; Xu, J.; Zhang, B.; Dong, J.; Ren, J.; Xu, C.; Gao, C.; et al. The Relationship between Low-Sodium Salt Intake and Both Blood Pressure Level and Hypertension in Chinese Residents. Nutrients 2024, 16, 1909. https://doi.org/10.3390/nu16121909
Wang C, Lu Z, Zhang J, Chen X, Xu J, Zhang B, Dong J, Ren J, Xu C, Gao C, et al. The Relationship between Low-Sodium Salt Intake and Both Blood Pressure Level and Hypertension in Chinese Residents. Nutrients. 2024; 16(12):1909. https://doi.org/10.3390/nu16121909
Chicago/Turabian StyleWang, Cuicui, Zilong Lu, Jiyu Zhang, Xiaorong Chen, Jianwei Xu, Bingyin Zhang, Jing Dong, Jie Ren, Chunxiao Xu, Congcong Gao, and et al. 2024. "The Relationship between Low-Sodium Salt Intake and Both Blood Pressure Level and Hypertension in Chinese Residents" Nutrients 16, no. 12: 1909. https://doi.org/10.3390/nu16121909
APA StyleWang, C., Lu, Z., Zhang, J., Chen, X., Xu, J., Zhang, B., Dong, J., Ren, J., Xu, C., Gao, C., Guo, X., Wu, J., & Ma, J. (2024). The Relationship between Low-Sodium Salt Intake and Both Blood Pressure Level and Hypertension in Chinese Residents. Nutrients, 16(12), 1909. https://doi.org/10.3390/nu16121909