
Blood Lead Mediates the Relationship between Biological Aging and Hypertension: Based on the NHANES Database

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. PhenoAge and PhenoAgeAccel Assessments
2.3. Blood Pressure Measurement and Definitions
2.4. Heavy Metals Assessments
2.5. Study Covariates
2.6. Statistical Analyses
3. Result
3.1. Baseline Characteristic
3.2. Association between PhenoAgeAccel and Hypertension, SBP, and DBP
3.3. Association between Co-Exposure of Blood Metals and Hypertension, SBP, and DBP
3.4. Blood Lead and Hypertension, SBP, and DBP in the Logistic Regression Model
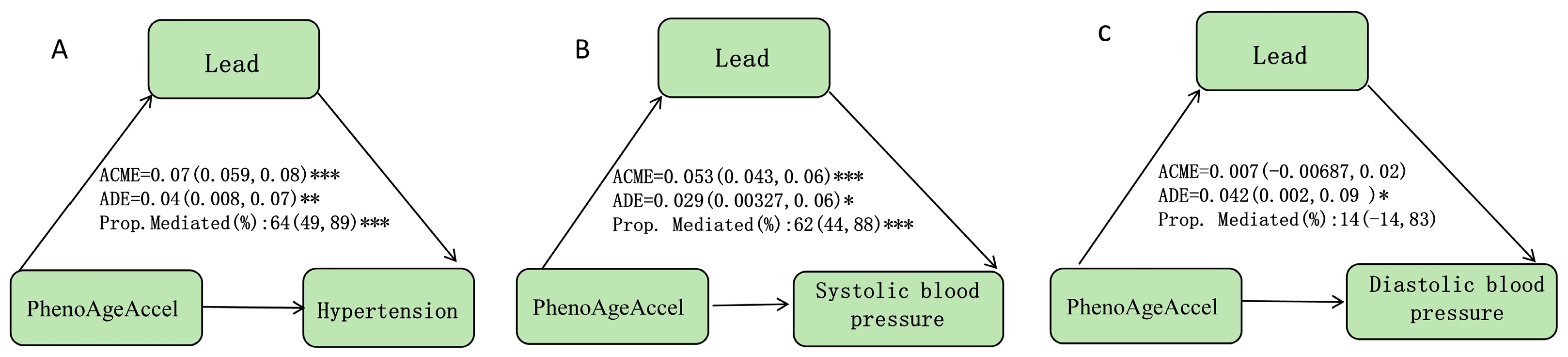
3.5. The Mediation Effects of Blood Lead in the Relationships of PhenoAgeAccel with Hypertension, SBP, and DBP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Heaton, J.; Alshami, A.; Imburgio, S.; Mararenko, A.; Schoenfeld, M.; Sealove, B.; Asif, A.; Almendral, J. Current Trends in Hypertension Identification and Management: Insights from the National Health and Nutrition Examination Survey (NHANES) Following the 2017 ACC/AHA High Blood Pressure Guidelines. J. Am. Heart Assoc. 2024, 13, e034322. [Google Scholar] [CrossRef] [PubMed]
- Muntner, P.; Carey, R.M.; Gidding, S.; Jones, D.W.; Taler, S.J.; Wright, J.T.; Whelton, P.K. Potential U.S. Population Impact of the 2017 ACC/AHA High Blood Pressure Guideline. J. Am. Coll. Cardiol. 2018, 71, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Perel, P.; Mensah, G.A.; Ezzati, M. Global epidemiology, health burden and effective interventions for elevated blood pressure and hypertension. Nat. Rev. Cardiol. 2021, 18, 785–802. [Google Scholar] [CrossRef] [PubMed]
- Oliveros, E.; Patel, H.; Kyung, S.; Fugar, S.; Goldberg, A.; Madan, N.; Williams, K.A. Hypertension in older adults: Assessment, management, and challenges. Clin. Cardiol. 2019, 43, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Börjesson, M.; Onerup, A.; Lundqvist, S.; Dahlöf, B. Physical activity and exercise lower blood pressure in individuals with hypertension: Narrative review of 27 RCTs. Br. J. Sports Med. 2016, 50, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Zhang, Y.; Yao, M.; Wu, G.; Duan, Z.; Zhao, X.; Zhang, J. Long-term effects of ambient PM2.5 on hypertension in multi-ethnic population from Sichuan province, China: A study based on 2013 and 2018 health service surveys. Environ. Sci. Pollut. Res. 2020, 28, 5991–6004. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.; Steven Xu, X.; Yang, Y.; Zhu, Z.; Zhu, Z.; Tao, F.; Yuan, M. Stratification of population in NHANES 2009–2014 based on exposure pattern of lead, cadmium, mercury, and arsenic and their association with cardiovascular, renal and respiratory outcomes. Environ. Int. 2021, 149, 106410. [Google Scholar] [CrossRef] [PubMed]
- Dodig, S.; Čepelak, I.; Pavić, I. Hallmarks of senescence and aging. Biochem. Medica 2019, 29, 483–497. [Google Scholar] [CrossRef] [PubMed]
- López-Otín, C.; Blasco, M.A.; Partridge, L.; Serrano, M.; Kroemer, G. Hallmarks of aging: An expanding universe. Cell 2023, 186, 243–278. [Google Scholar] [CrossRef] [PubMed]
- Odden, M.C.; Beilby, P.R.; Peralta, C.A. Blood Pressure in Older Adults: The Importance of Frailty. Curr. Hypertens. Rep. 2015, 17, 55. [Google Scholar] [CrossRef] [PubMed]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics—2022 Update: A Report From the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [CrossRef] [PubMed]
- Lanphear, B.P.; Rauch, S.; Auinger, P.; Allen, R.W.; Hornung, R.W. Low-level lead exposure and mortality in US adults: A population-based cohort study. Lancet Public Health 2018, 3, e177–e184. [Google Scholar] [CrossRef] [PubMed]
- Tellez-Plaza, M.; Navas-Acien, A.; Menke, A.; Crainiceanu, C.M.; Pastor-Barriuso, R.; Guallar, E. Cadmium Exposure and All-Cause and Cardiovascular Mortality in the U.S. General Population. Environ. Health Perspect. 2012, 120, 1017–1022. [Google Scholar] [CrossRef] [PubMed]
- Genchi, G.; Sinicropi, M.; Carocci, A.; Lauria, G.; Catalano, A. Mercury Exposure and Heart Diseases. Int. J. Environ. Res. Public Health 2017, 14, 74. [Google Scholar] [CrossRef] [PubMed]
- Zeng, A.; Li, S.; Zhou, Y.; Sun, D. Association Between Low-Level Blood Cadmium Exposure and Hyperuricemia in the American General Population: A Cross-sectional Study. Biol. Trace Elem. Res. 2021, 200, 560–567. [Google Scholar] [CrossRef] [PubMed]
- Scinicariello, F.; Abadin, H.G.; Edward Murray, H. Association of low-level blood lead and blood pressure in NHANES 1999–2006. Environ. Res. 2011, 111, 1249–1257. [Google Scholar] [CrossRef] [PubMed]
- Almeida Lopes, A.C.B.d.; Silbergeld, E.K.; Navas-Acien, A.; Zamoiski, R.; Martins, A.d.C.; Camargo, A.E.I.; Urbano, M.R.; Mesas, A.E.; Paoliello, M.M.B. Association between blood lead and blood pressure: A population-based study in Brazilian adults. Environ. Health 2017, 16, 27. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.A.; Kim, B.; Kim, E.; Kwon, K. Interaction between blood cadmium and lead concentration and physical activity on hypertension from the Korean national health and nutrition examination survey in 2008–2013. BMC Public Health 2023, 23, 703. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-q.; He, G.-d.; Feng, Y.-q. The association of lead exposure with blood pressure and hypertension: A mediation analyses of estimated glomerular filtration rate. Environ. Sci. Pollut. Res. 2023, 30, 59689–59700. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.D.; Rouzier, V.; Pierre, J.L.; Lee, M.H.; Muntner, P.; Parsons, P.J.; Apollon, A.; St-Preux, S.; Malebranche, R.; Pierre, G.; et al. High Lead Exposure Associated With Higher Blood Pressure in Haiti: A Warning Sign for Low-Income Countries. Hypertension 2022, 79, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.-Y.; Efremov, L.; Mujaj, B.; Zhang, Z.-Y.; Wei, F.-F.; Huang, Q.-F.; Thijs, L.; Vanassche, T.; Nawrot, T.S.; Staessen, J.A. Association of office and ambulatory blood pressure with blood lead in workers before occupational exposure. J. Am. Soc. Hypertens. 2018, 12, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Hara, A.; Thijs, L.; Asayama, K.; Gu, Y.-M.; Jacobs, L.; Zhang, Z.-Y.; Liu, Y.-P.; Nawrot, T.S.; Staessen, J.A. Blood Pressure in Relation to Environmental Lead Exposure in the National Health and Nutrition Examination Survey 2003 to 2010. Hypertension 2015, 65, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Den Hond, E.; Nawrot, T.; Staessen, J.A. The relationship between blood pressure and blood lead in NHANES III. J. Hum. Hypertens. 2002, 16, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Levine, M.E.; Lu, A.T.; Quach, A.; Chen, B.H.; Assimes, T.L.; Bandinelli, S.; Hou, L.; Baccarelli, A.A.; Stewart, J.D.; Li, Y.; et al. An epigenetic biomarker of aging for lifespan and healthspan. Aging 2018, 10, 573–591. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Liu, M.; Zhang, Y.; Wu, J.; Gao, M.; Huang, F.; Chen, H.; Zhu, Z. Serum HDL partially mediates the association between exposure to volatile organic compounds and kidney stones: A nationally representative cross-sectional study from NHANES. Sci. Total Environ. 2024, 907, 167915. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.heart.org/en/health-topics/high-blood-pressure/understanding-blood-pressure-readings (accessed on 5 June 2024).
- Chen, Y.; Pan, Z.; Shen, J.; Wu, Y.; Fang, L.; Xu, S.; Ma, Y.; Zhao, H.; Pan, F. Associations of exposure to blood and urinary heavy metal mixtures with psoriasis risk among U.S. adults: A cross-sectional study. Sci. Total Environ. 2023, 887, 164133. [Google Scholar] [CrossRef] [PubMed]
- Zheng, L.; Jing, X.; Zhang, X.; Zhong, C.; Qiu, D.; Yan, Q.; Gao, Z. Mediation analysis of urinary metals and stroke risk by inflammatory markers. Chemosphere 2023, 341, 140084. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.W.; Kim, H.C.; Nam, C.; Lee, H.-Y.; Ahn, S.V.; Oh, Y.A.; Suh, I. Age-differential association between serum uric acid and incident hypertension. Hypertens. Res. 2018, 42, 428–437. [Google Scholar] [CrossRef] [PubMed]
- Abete, P.; Parikh, J.D.; Hollingsworth, K.G.; Wallace, D.; Blamire, A.M.; MacGowan, G.A. Left ventricular functional, structural and energetic effects of normal aging: Comparison with hypertension. PLoS ONE 2017, 12, e0177404. [Google Scholar] [CrossRef]
- Casso, A.G.; VanDongen, N.S.; Gioscia-Ryan, R.A.; Clayton, Z.S.; Greenberg, N.T.; Ziemba, B.P.; Hutton, D.A.; Neilson, A.P.; Davy, K.P.; Seals, D.R.; et al. Initiation of 3,3-dimethyl-1-butanol at midlife prevents endothelial dysfunction and attenuates in vivo aortic stiffening with ageing in mice. J. Physiol. 2022, 600, 4633–4651. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zhao, L.; Zhou, X.; Meng, X.; Zhou, X. Role of inflammation, immunity, and oxidative stress in hypertension: New insights and potential therapeutic targets. Front. Immunol. 2023, 13, 1098725. [Google Scholar] [CrossRef] [PubMed]
- Charkiewicz, A.E.; Backstrand, J.R. Lead Toxicity and Pollution in Poland. Int. J. Environ. Res. Public Health 2020, 17, 4385. [Google Scholar] [CrossRef] [PubMed]
- Schneider, J.L.; Rowe, J.H.; Garcia-de-Alba, C.; Kim, C.F.; Sharpe, A.H.; Haigis, M.C. The aging lung: Physiology, disease, and immunity. Cell 2021, 184, 1990–2019. [Google Scholar] [CrossRef] [PubMed]
- Funk, M.C.; Zhou, J.; Boutros, M. Ageing, metabolism and the intestine. EMBO Rep. 2020, 21, e50047. [Google Scholar] [CrossRef] [PubMed]
- Ravipati, E.S.; Mahajan, N.N.; Sharma, S.; Hatware, K.V.; Patil, K. The toxicological effects of lead and its analytical trends: An update from 2000 to 2018. Crit. Rev. Anal. Chem. 2019, 51, 87–102. [Google Scholar] [CrossRef] [PubMed]
- Glassock, R.J.; Rule, A.D. Aging and the Kidneys: Anatomy, Physiology and Consequences for Defining Chronic Kidney Disease. Nephron 2016, 134, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Zheng, K.; Zeng, Z.; Tian, Q.; Huang, J.; Zhong, Q.; Huo, X. Epidemiological evidence for the effect of environmental heavy metal exposure on the immune system in children. Sci. Total Environ. 2023, 868, 161691. [Google Scholar] [CrossRef] [PubMed]
- Aramjoo, H.; Arab-Zozani, M.; Feyzi, A.; Naghizadeh, A.; Aschner, M.; Naimabadi, A.; Farkhondeh, T.; Samarghandian, S. The association between environmental cadmium exposure, blood pressure, and hypertension: A systematic review and meta-analysis. Environ. Sci. Pollut. Res. 2022, 29, 35682–35706. [Google Scholar] [CrossRef] [PubMed]
- Martins, A.C.; Almeida Lopes, A.C.B.; Urbano, M.R.; Carvalho, M.d.F.H.; Silva, A.M.R.; Tinkov, A.A.; Aschner, M.; Mesas, A.E.; Silbergeld, E.K.; Paoliello, M.M.B. An updated systematic review on the association between Cd exposure, blood pressure and hypertension. Ecotoxicol. Environ. Saf. 2021, 208, 111636. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Zou, Y.; Leng, X.; Huang, F.; Huang, R.; Wijayabahu, A.; Chen, X.; Xu, Y. Associations of blood lead, cadmium, and mercury with resistant hypertension among adults in NHANES, 1999–2018. Environ. Health Prev. Med. 2023, 28, 66. [Google Scholar] [CrossRef] [PubMed]
- He, P.; Yang, C.; He, D.; Zhao, S.; Xie, Y.; Wang, H.; Ma, J. Blood Lead, Systemic Inflammation, and Blood Pressure: Exploring Associations and Mediation Effects in Workers Exposed to Lead. Biol. Trace Elem. Res. 2020, 199, 2573–2581. [Google Scholar] [CrossRef] [PubMed]
- Jomova, K.; Valko, M. Advances in metal-induced oxidative stress and human disease. Toxicology 2011, 283, 65–87. [Google Scholar] [CrossRef] [PubMed]
- Jiao, J.; Wang, M.; Wang, Y.; Sun, N.; Li, C. Lead exposure increases blood pressure by increasing angiotensinogen expression. J. Environ. Sci. Health Part A 2016, 51, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Franco, C.; Sciatti, E.; Favero, G.; Bonomini, F.; Vizzardi, E.; Rezzani, R. Essential Hypertension and Oxidative Stress: Novel Future Perspectives. Int. J. Mol. Sci. 2022, 23, 14489. [Google Scholar] [CrossRef]
- Partridge, L.; Deelen, J.; Slagboom, P.E. Facing up to the global challenges of ageing. Nature 2018, 561, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Levin, R.; Zilli Vieira, C.L.; Rosenbaum, M.H.; Bischoff, K.; Mordarski, D.C.; Brown, M.J. The urban lead (Pb) burden in humans, animals and the natural environment. Environ. Res. 2021, 193, 110377. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n (%) | p Value | ||
|---|---|---|---|---|
| Hypertension | DBP | SBP | ||
| Sex | ||||
| male | 2247 (50.2) | 0.104 | <0.001 | <0.001 |
| female | 2226 (49.8) | |||
| Diabetes | ||||
| No | 3705 (82.8) | <0.001 | 0.093 | <0.001 |
| Yes | 768 (17.2) | |||
| Drinking status | ||||
| No | 806 (18.0) | 0.824 | <0.001 | 0.388 |
| Yes | 3667 (82.0) | |||
| Age | ||||
| 18–39 | 1490 (33.3) | <0.001 | <0.001 | <0.001 |
| 40–59 | 1492 (33.4) | |||
| ≥60 | 1491 (33.3) | |||
| Race | ||||
| White | 1669 (37.3) | 0.27 | <0.001 | 0.454 |
| Black and others | 2804 (62.7) | |||
| Education level | ||||
| Below high school | 809 (18.1) | 0.006 | 0.162 | <0.001 |
| High school | 1033 (23.1) | |||
| Above high school | 2631 (58.8) | |||
| Marital status | ||||
| Single/divorced/widowed/separated | 1762 (39.4) | 0.158 | 0.263 | 0.233 |
| Married/cohabited | 2711 (60.6) | |||
| PIR | ||||
| <2 | 2047 (45.8) | 0.313 | 0.616 | 0.907 |
| ≥2 | 2426 (54.2) | |||
| CHD | ||||
| No | 4296 (96.0) | <0.001 | 0.015 | <0.001 |
| Yes | 177 (4.0) | |||
| Stroke | ||||
| No | 4296 (96.0) | <0.001 | 0.218 | <0.001 |
| Yes | 177 (4.0) | |||
| Smoking status | ||||
| No | 2492 (55.7) | <0.001 | 0.897 | <0.001 |
| Yes | 1981 (44.3) | |||
| BMI (kg/m2) | ||||
| <25 | 1158 (25.9) | <0.001 | 0.001 | <0.001 |
| 25–30 | 1410 (31.5) | |||
| ≥30 | 1905 (42.6) | |||
| InPb | ||||
| Q1 | 1141 (25.5) | <0.001 | <0.001 | <0.001 |
| Q2 | 1101 (24.6) | |||
| Q3 | 1130 (25.3) | |||
| Q4 | 1101 (24.6) | |||
| InCd | ||||
| Q1 | 1121 (25.1) | <0.001 | 0.167 | 0.024 |
| Q2 | 1121 (25.1) | |||
| Q3 | 1121 (25.1) | |||
| Q4 | 1110 (24.8) | |||
| InHg | ||||
| Q1 | 1137 (25.4) | 0.204 | 0.962 | 0.044 |
| Q2 | 1112 (24.9) | |||
| Q3 | 1111 (24.8) | |||
| Q4 | 1113 (24.9) | |||
| InMn | ||||
| Q1 | 1122 (25.1) | <0.001 | 0.526 | <0.001 |
| Q2 | 1120 (25.0) | |||
| Q3 | 1114 (24.9) | |||
| Q4 | 1117 (25.0) | |||
| InSe | ||||
| Q1 | 1119 (25.0) | 0.191 | <0.001 | 0.352 |
| Q2 | 1118 (25.0) | |||
| Q3 | 1119 (25.0) | |||
| Q4 | 1117 (25.0) | |||
| PhenoAgeAccel | ||||
| No | 2661 (59.5) | <0.001 | 0.056 | <0.001 |
| Yes | 1812 (40.5) | |||
| Method | Hypertension | SBP | DBP | |||
|---|---|---|---|---|---|---|
| OR (95% Cl) | p-Value | OR (95% Cl) | p-Value | OR (95% Cl) | p-Value | |
| WQS | ||||||
| Crude model | 1.37 (1.27, 1.48) | <0.001 | 1.59 (1.46, 1.73) | <0.001 | 1.29 (1.15, 1.46) | <0.001 |
| Adjusted model | 1.35 (1.24, 1.48) | <0.001 | 1.53 (1.39, 1.68) | <0.001 | 1.28 (1.13, 1.46) | <0.001 |
| QGC | ||||||
| Crude model | 1.317 (1.178, 1.474) | <0.001 | 1.323 (1.18, 1.483) | <0.001 | 1.255 (1.105, 1.425) | <0.001 |
| Adjusted model | 1.385 (1.226, 1.565) | <0.001 | 1.352 (1.2, 1.524) | <0.001 | 1.288 (1.128, 1.471) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, C.; Su, J.; Li, J.; Wei, W.; Yuan, Z.; Chen, R.; Wei, W.; Huang, Y.; Ye, L.; Liang, H.; et al. Blood Lead Mediates the Relationship between Biological Aging and Hypertension: Based on the NHANES Database. Nutrients 2024, 16, 2144. https://doi.org/10.3390/nu16132144
Wang C, Su J, Li J, Wei W, Yuan Z, Chen R, Wei W, Huang Y, Ye L, Liang H, et al. Blood Lead Mediates the Relationship between Biological Aging and Hypertension: Based on the NHANES Database. Nutrients. 2024; 16(13):2144. https://doi.org/10.3390/nu16132144
Chicago/Turabian StyleWang, Cuixiao, Jinming Su, Jinmiao Li, Wenfei Wei, Zongxiang Yuan, Rongfeng Chen, Wudi Wei, Youjin Huang, Li Ye, Hao Liang, and et al. 2024. "Blood Lead Mediates the Relationship between Biological Aging and Hypertension: Based on the NHANES Database" Nutrients 16, no. 13: 2144. https://doi.org/10.3390/nu16132144