
Poor Adherence to the Mediterranean Diet and Sleep Disturbances Are Associated with Migraine Chronification and Disability among an Adult Population in the Lazio Region, Italy
 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Evaluations of Demographic and Clinical Characteristics in the Migraine Patient Cohort
- -
- The Migraine Disability Assessment Scale (MIDAS) questionnaire, the most used disability instrument in migraine research based on five questions that focus on lost time in three domains: schoolwork or work for pay; household work or chores; and family, social, and leisure activities [14]. All questions ask about days of missed activity or days where productivity was at least halved. If productivity is reduced to 50% or below, the day is considered missed. The MIDAS score is derived as the sum of days missed due to a headache over a 3-month period in the three domains [14];
- -
- The Headache Impact Test-6 (HIT-6), a self-administered six-item questionnaire that measures the impact of headache on “usual daily activities”, including work, school, or social activities, assessing the severity of pain, fatigue, the desire to lie down, frustration, and difficulty concentrating. The HIT-6 questionnaire has good discriminative validity, internal consistency (Cronbach’s α of 0.79), and test–retest reliability (average Cronbach’s α of 0.78) [15];
- -
- The visual analogue scale (VAS) for the evaluation of pain intensity. It is presented graphically with a 10 cm line and endpoint adjective descriptors (“the worst imaginable pain” on one end and “no pain” on the other). The patient is asked to place a mark along the line to indicate their current level of pain. A difference of 13 mm between consecutive pain ratings is the minimum change in a clinically significant pain rating [16].
2.3. Evaluations of Lifestyle Habits and Diet Patterns in Migraine Patients and Controls
2.4. EMLF and EMHF+CM Groups
2.5. Statistical Analysis
3. Results
3.1. Cohort Characteristics
3.2. Migraine Patient Characteristics
3.3. Lifestyle Habits and Dietary Patterns in Migraine Patients and Controls
3.4. EMLF and EMHF+CM Subgroup Features
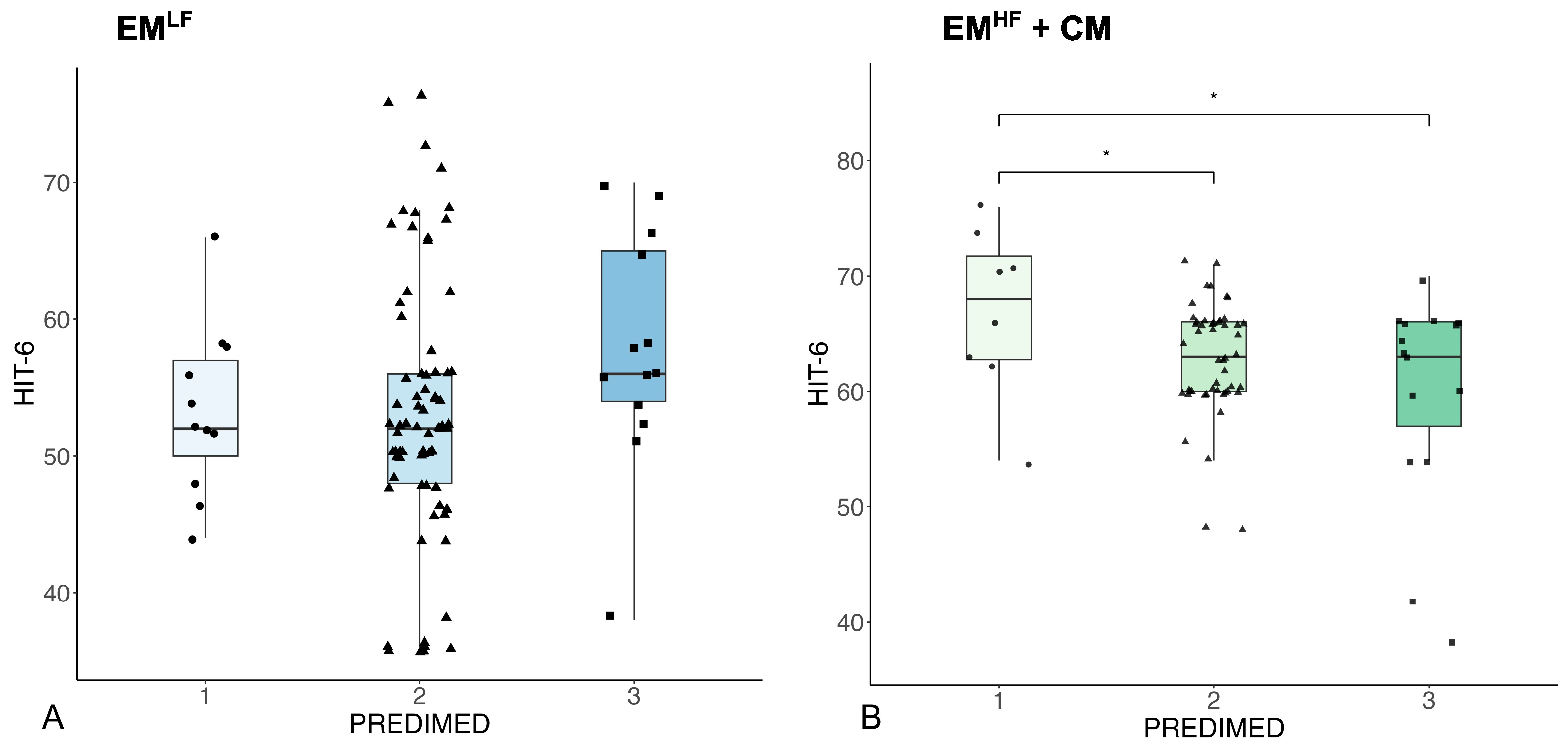
3.5. Relationships between Migraine Characteristics and Lifestyle Factors in the EMLF and EMHF+CM Subgroups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Olesen, J. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd Edition. Cephalalgia 2018, 38, 209–218. [Google Scholar] [CrossRef]
- Sacco, S.; Lampl, C.; Maassen van den Brink, A.; Caponnetto, V.; Braschinsky, M.; Ducros, A.; Little, P.; Pozo-Rosich, P.; Reuter, U.; Ruiz de la Torre, E.; et al. Burden and Attitude to Resistant and Refractory Migraine: A survey of the European Headache Federation with the endorsement of the European Migraine & Headache Alliance. J. Headache Pain 2021, 22, 1–10. [Google Scholar] [CrossRef]
- Tonini, M.C.; Fiorencis, A.; Iannacchero, R.; Zampolini, M.; Cappuccio, A.; Raddino, R.; Grillo, E.; Albanese, M.; Allais, G.; Bassano, M.A.; et al. Narrative Medicine to Integrate Patients’, Caregivers’ and Clinicians’ Migraine Experiences: The DRONE Multicentre Project. Neurol. Sci. 2021, 42, 5277–5288. [Google Scholar] [CrossRef] [PubMed]
- Scher, A.I.; Stewart, W.F.; Ricci, J.A.; Lipton, R.B. Factors Associated with the Onset and Remission of Chronic Daily Headache in a Population-Based Study. Pain 2003, 106, 81–89. [Google Scholar] [CrossRef]
- Di Lauro, M.; Guerriero, C.; Cornali, K.; Albanese, M.; Costacurta, M.; Mercuri, N.B.; Di Daniele, N.; Noce, A. Linking Migraine to Gut Dysbiosis and Chronic Non-Communicable Diseases. Nutrients 2023, 15, 4327. [Google Scholar] [CrossRef]
- Gazerani, P. A Bidirectional View of Migraine and Diet Relationship. Neuropsychiatr. Dis. Treat. 2021, 17, 435–451. [Google Scholar] [CrossRef] [PubMed]
- Tsigalou, C.; Konstantinidis, T.; Paraschaki, A.; Stavropoulou, E.; Voidarou, C.; Bezirtzoglou, E. Mediterranean Diet as a Tool to Combat Inflammation and Chronic Diseases. An Overview. Biomedicines 2020, 8, 201. [Google Scholar] [CrossRef]
- Martinelli, V.; Albanese, M.; Altieri, M.; Annovazzi, P.; Arabi, S.; Bucello, S.; Caleri, F.; Cerqua, R.; Costanzi, C.; Cottone, S.; et al. Gut-oriented interventions in patients with multiple sclerosis: Fact or fiction? Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 935–946. [Google Scholar] [CrossRef] [PubMed]
- Noce, A.; Marchetti, M.; Marrone, G.; Di Renzo, L.; Di Lauro, M.; Di Daniele, F.; Albanese, M.; Di Daniele, N.; De Lorenzo, A. Link between gut microbiota dysbiosis and chronic kidney disease. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 2057–2074. [Google Scholar] [CrossRef]
- Pietrucci, D.; Cerroni, R.; Unida, V.; Farcomeni, A.; Pierantozzi, M.; Mercuri, N.B.; Biocca, S.; Stefani, A.; Desideri, A. Dysbiosis of gut microbiota in a selected population of Parkinson’s patients. Parkinsonism Relat. Disord. 2019, 65, 124–130. [Google Scholar] [CrossRef]
- Arab, A.; Khorvash, F.; Karimi, E.; Hadi, A.; Askari, G. Associations between Adherence to Mediterranean Dietary Pattern and Frequency, Duration, and Severity of Migraine Headache: A Cross-Sectional Study. Nutr. Neurosci. 2023, 26, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Godos, J.; Ferri, R.; Lanza, G.; Caraci, F.; Vistorte, A.O.R.; Torres, V.Y.; Grosso, G.; Castellano, S. Mediterranean diet and sleep features: A systematic review of current evidence. Nutrients 2024, 16, 282. [Google Scholar] [CrossRef] [PubMed]
- Ruscheweyh, R.; Gossrau, G.; Dresler, T.; Freilinger, T.; Förderreuther, S.; Gaul, C.; Kraya, T.; Neeb, L.; Ruschil, V.; Straube, A.; et al. Triptan non-response in specialized headache care: Cross-sectional data from the DMKG Headache Registry. J. Headache Pain 2023, 24, 135. [Google Scholar] [CrossRef]
- Stewart, W.F.; Lipton, R.B.; Dowson, A.J.; Sawyer, J. Development and Testing of the Migraine Disability Assessment (MIDAS) Questionnaire to Assess Headache-Related Disability. Neurology 2001, 56, S20–S28. [Google Scholar] [CrossRef]
- Shin, H.E.; Park, J.W.; Kim, Y.I.; Lee, K.S. Headache Impact Test-6 (HIT-6) Scores for Migraine Patients: Their Relation to Disability as Measured from a Headache Diary. J. Clin. Neurol. 2008, 4, 158–163. [Google Scholar] [CrossRef]
- McCormack, H.M.; Horne, D.J.d.L.; Sheather, S. Clinical Applications of Visual Analogue Scales: A Critical Review. Psychol. Med. 1988, 18, 1007–1019. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-Item Mediterranean Diet Assessment Tool and Obesity Indexes among High-Risk Subjects: The PREDIMED Trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Serrano, D.; Lipton, R.B.; Scher, A.I.; Reed, M.L.; Stewart, W.B.F.; Adams, A.M.; Buse, D.C. Fluctuations in episodic and chronic migraine status over the course of 1 year: Implications for diagnosis, treatment and clinical trial design. J. Headache Pain 2017, 18, 1–12. [Google Scholar] [CrossRef]
- Agbetou, M.; Adoukonou, T. Lifestyle Modifications for Migraine Management. Front. Neurol. 2022, 13, 719467. [Google Scholar] [CrossRef] [PubMed]
- Di Lorenzo, C.; Ballerini, G.; Barbanti, P.; Bernardini, A.; D’arrigo, G.; Egeo, G.; Frediani, F.; Garbo, R.; Pierangeli, G.; Prudenzano, M.P.; et al. Applications of Ketogenic Diets in Patients with Headache: Clinical Recommendations. Nutrients 2021, 13, 2307. [Google Scholar] [CrossRef]
- Volpe, S.L. What Is the Mediterranean Diet? ACSM’S Heal. Fit. J. 2022, 26, 45–47. [Google Scholar] [CrossRef]
- Marrone, G.; Urciuoli, S.; Di Lauro, M.; Ruzzolini, J.; Ieri, F.; Vignolini, P.; Di Daniele, F.; Guerriero, C.; Nediani, C.; Di Daniele, N.; et al. Extra Virgin Olive Oil and Cardiovascular Protection in Chronic Kidney Disease. Nutrients 2022, 14, 4265. [Google Scholar] [CrossRef] [PubMed]
- Noce, A.; Marrone, G.; Urciuoli, S.; Di Daniele, F.; Di Lauro, M.; Pietroboni Zaitseva, A.; Di Daniele, N.; Romani, A. Usefulness of Extra Virgin Olive Oil Minor Polar Compounds in the Management of Chronic Kidney Disease Patients. Nutrients 2021, 13, 581. [Google Scholar] [CrossRef] [PubMed]
- Romani, A.; Bernini, R.; Noce, A.; Urciuoli, S.; Di Lauro, M.; Pietroboni Zaitseva, A.; Marrone, G.; Di Daniele, N. Potential Beneficial Effects of Extra Virgin Olive Oils Characterized by High Content in Minor Polar Compounds in Nephropathic Patients: A Pilot Study. Molecules 2020, 25, 4757. [Google Scholar] [CrossRef]
- De Lorenzo, A.; Noce, A.; Bigioni, M.; Calabrese, V.; Della Rocca, D.G.; Di Daniele, N.; Tozzo, C.; Di Renzo, L. The effects of Italian Mediterranean organic diet (IMOD) on health status. Curr. Pharm. Des. 2010, 16, 814–824. [Google Scholar] [CrossRef]
- Schirinzi, T.; Martella, G.; Imbriani, P.; Di Lazzaro, G.; Franco, D.; Colona, V.L.; Alwardat, M.; Salimei, P.S.; Mercuri, N.B.; Pierantozzi, M.; et al. Dietary Vitamin E as a Protective Factor for Parkinson’s Disease: Clinical and Experimental Evidence. Front. Neurol. 2019, 10, 148. [Google Scholar] [CrossRef] [PubMed]
- Noce, A.; Di Lauro, M.; Di Daniele, F.; Pietroboni Zaitseva, A.; Marrone, G.; Borboni, P.; Di Daniele, N. Natural Bioactive Compounds Useful in Clinical Management of Metabolic Syndrome. Nutrients 2021, 13, 630. [Google Scholar] [CrossRef]
- Tessari, S.; Casazza, M.; de Boni, G.; Bertoncello, C.; Fonzo, M.; di Pieri, M.; Russo, F. Promoting Health and Preventing Non-Communicable Diseases: Evaluation of the Adherence of the Italian Population to the Mediterranean Diet by Using the PREDIMED Questionnaire. Ann. Ig. Med. Prev. Comunità 2021, 33, 337–346. [Google Scholar] [CrossRef]
- Aureli, V.; Rossi, L. Nutrition Knowledge as a Driver of Adherence to the Mediterranean Diet in Italy. Front. Nutr. 2022, 9, 804865. [Google Scholar] [CrossRef] [PubMed]
- Katsarava, Z.; Buse, D.C.; Manack, A.N.; Lipton, R.B. Defining the Differences between Episodic Migraine and Chronic Migraine. Curr. Pain Headache Rep. 2012, 16, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Bigal, M.E.; Serrano, D.; Buse, D.; Scher, A.; Stewart, W.F.; Lipton, R.B. Acute Migraine Medications and Evolution from Episodic to Chronic Migraine: A Longitudinal Population-Based Study. Headache 2008, 48, 1157–1168. [Google Scholar] [CrossRef] [PubMed]
- Becker, W.J. Botulinum Toxin in the Treatment of Headache. Toxins 2020, 12, 803. [Google Scholar] [CrossRef]
- Altamura, C.; Brunelli, N.; Viticchi, G.; Salvemini, S.; Cecchi, G.; Marcosano, M.; Fofi, L.; Silvestrini, M.; Vernieri, F. Quantitative and Qualitative Pain Evaluation in Response to OnabotulinumtoxinA for Chronic Migraine: An Observational Real-Life Study. Toxins 2023, 15, 284. [Google Scholar] [CrossRef]
- Conti, M.; Bovenzi, R.; Palmieri, M.G.; Placidi, F.; Stefani, A.; Mercuri, N.B.; Albanese, M. Early effect of onabotulinumtoxinA on EEG-based functional connectivity in patients with chronic migraine: A pilot study. Headache 2024. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Morze, J.; Hoffmann, G. Mediterranean Diet and Health Status: Active Ingredients and Pharmacological Mechanisms. Br. J. Pharmacol. 2020, 177, 1241–1257. [Google Scholar] [CrossRef] [PubMed]
- Fila, M.; Pawłowska, E.; Blasiak, J. Mitochondria in Migraine Pathophysiology—Does Epigenetics Play a Role? Arch. Med Sci. 2019, 15, 944–956. [Google Scholar] [CrossRef]
- Albanese, M. Clinical Management of Migraine. J. Clin. Med. 2022, 11, 5225. [Google Scholar] [CrossRef]
- Canale, M.P.; Noce, A.; Di Lauro, M.; Marrone, G.; Cantelmo, M.; Cardillo, C.; Federici, M.; Di Daniele, N.; Tesauro, M. Gut Dysbiosis and Western Diet in the Pathogenesis of Essential Arterial Hypertension: A Narrative Review. Nutrients 2021, 13, 1162. [Google Scholar] [CrossRef]
- Di Daniele, N.; Noce, A.; Vidiri, M.F.; Moriconi, E.; Marrone, G.; Annicchiarico-Petruzzelli, M.; D’Urso, G.; Tesauro, M.; Rovella, V.; De Lorenzo, A. Impact of Mediterranean diet on metabolic syndrome, cancer and longevity. Oncotarget 2017, 8, 8947–8979. [Google Scholar] [CrossRef]
- Merra, G.; Noce, A.; Marrone, G.; Cintoni, M.; Tarsitano, M.G.; Capacci, A.; De Lorenzo, A. Influence of Mediterranean Diet on Human Gut Microbiota. Nutrients 2020, 13, 7. [Google Scholar] [CrossRef]
- Korabelnikova, E.A.; Danilov, A.B.; Danilov, A.B.; Vorobyeva, Y.D.; Latysheva, N.V.; Artemenko, A.R. Sleep Disorders and Headache: A Review of Correlation and Mutual Influence. Pain Ther. 2020, 9, 411–425. [Google Scholar] [CrossRef]
- Tiseo, C.; Vacca, A.; Felbush, A.; Filimonova, T.; Gai, A.; Glazyrina, T.; Hubalek, I.A.; Marchenko, Y.; Overeem, L.H.; Piroso, S.; et al. Migraine and Sleep Disorders: A Systematic Review. J. Headache Pain 2020, 21, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Petit, J.M.; Eren-Koçak, E.; Karatas, H.; Magistretti, P.; Dalkara, T. Brain Glycogen Metabolism: A Possible Link between Sleep Disturbances, Headache and Depression. Sleep. Med. Rev. 2021, 59, 101449. [Google Scholar] [CrossRef]
- Yi, T.; Gao, P.; Zhu, T.; Yin, H.; Jin, S. Glymphatic System Dysfunction: A Novel Mediator of Sleep Disorders and Headaches. Front. Neurol. 2022, 13, 885020. [Google Scholar] [CrossRef] [PubMed]
- Bond, D.S.; Roth, J.; Nash, J.M.; Wing, R.R. Migraine and Obesity: Epidemiology, Possible Mechanisms and the Potential Role of Weight Loss Treatment. Obes. Rev. 2011, 12, e362–e371. [Google Scholar] [CrossRef]
- Varkey, E.; Hagen, K.; Zwart, J.A.; Linde, M. Physical Activity and Headache: Results from the Nord-Trøndelag Health Study (HUNT). Cephalalgia 2008, 28, 1292–1297. [Google Scholar] [CrossRef] [PubMed]
- Amin, F.M.; Aristeidou, S.; Baraldi, C.; Czapinska-Ciepiela, E.K.; Ariadni, D.D.; Di Lenola, D.; Fenech, C.; Kampouris, K.; Karagiorgis, G.; Braschinsky, M.; et al. The Association between Migraine and Physical Exercise. J. Headache Pain 2018, 19, 83. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Migraine Patients (n = 170) | Controls (n = 100) | p-Value | |
|---|---|---|---|
| Gender (M/F) | 31/139 | 13/87 | NS |
| Age (years) | 44.4 ± 13.3 | 49.2 ± 15.7 | NS |
| BMI (kg/m2) | 23.6 ± 3.5 | 24.1 ± 4.2 | NS |
| IPAQ (1/2/3) | 65/65/40 | 38/18/7 | p = 0.007 * |
| PREDIMED (1/2/3) | 19/124/27 | 1/70/29 | p < 0.001 * |
| Sleep–wake disturbances (Y/N) | 110/60 | 63/37 | NS |
| Migraine features | |||
| Disease duration (years) | 22.4 ± 15.3 | / | / |
| MMDs | 8.2 ± 7.6 | / | / |
| Painkillers/month | 5.3 ± 7.3 | / | / |
| Mean duration of attacks (hours) | 34.9 ± 20.7 | / | / |
| VAS | 8.1 ± 1.8 | / | / |
| MIDAS | 18.8 ± 22.5 | / | / |
| HIT-6 | 57.6 ± 9.3 | / | / |
| Pain localization (1/2/3/4) | 50/19/18/82 | / | / |
| Pain type (1/2/3) | 79/3/88 | / | / |
| UASs (Y/N) | 19/151 | / | / |
| Preventive treatments (n) (0/1/2/3/4) | 41/87/31/7/4 | / | / |
| Response to triptans (0/1/2/3) | 6/26/75/63 | / | / |
| >3 failed previous preventive treatments (Y/N) | 12/158 | / | / |
| EMLF Patients (n = 98) | EMHF Patients + CM Patients (n = 72) | p-Value | |
|---|---|---|---|
| Gender (M/F) | 20/78 | 11/61 | NS |
| Age (years) | 43.1 ± 13.0 | 46.1 ± 13.6 | NS |
| Disease duration (years) | 23.3 ± 14.8 | 21.1 ± 15.1 | NS |
| BMI (kg/m2) | 23.7 ± 3.6 | 23.5 ± 3.4 | NS |
| MMDs | 3.3 ± 1.9 | 14.8 ± 12.9 | p < 0.001 * |
| Symptomatics/month | 2.4 ± 2.4 | 9.1 ± 9.6 | p < 0.001 * |
| Mean attack duration | 33.6 ± 21.1 | 36.6 ± 20.3 | NS |
| VAS | 7.7 ± 2.2 | 8.6 ± 1.1 | p = 0.009 * |
| MIDAS | 14.2 ± 19.1 | 25.0 ± 25.3 | p = 0.001 * |
| HIT-6 | 53.56 ± 9.3 | 63.0 ± 5.8 | p < 0.001 * |
| IPAQ (1/2/3) | 39/35/24 | 26/30/16 | NS |
| PREDIMED (1/2/3) | 11/74/13 | 8/50/14 | NS |
| Sleep–wake disturbances (Y/N) | 62/36 | 48/24 | NS |
| Pain localization (1/2/3/4) | 36/9/9/43 | 14/10/9/39 | NS |
| Pain type (1/2/3) | 38/2/52 | 27/1/36 | NS |
| UASs (Y/N) | 11/87 | 8/64 | NS |
| Preventive treatments (number) (0/1/2/3/4) | 31/47/16/4/0 | 10/40/15/3/4 | p = 0.019 * |
| Response to triptans (0/1/2/3) | 2/8/43/45 | 4/18/32/18 | p = 0.003 * |
| >3 failed previous preventive treatments (Y/N) | 7/91 | 5/67 | NS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bovenzi, R.; Noce, A.; Conti, M.; Di Lauro, M.; Chiaramonte, B.; Della Morte, D.; Stefani, A.; De Lorenzo, A.; Mercuri, N.B.; Albanese, M. Poor Adherence to the Mediterranean Diet and Sleep Disturbances Are Associated with Migraine Chronification and Disability among an Adult Population in the Lazio Region, Italy. Nutrients 2024, 16, 2169. https://doi.org/10.3390/nu16132169
Bovenzi R, Noce A, Conti M, Di Lauro M, Chiaramonte B, Della Morte D, Stefani A, De Lorenzo A, Mercuri NB, Albanese M. Poor Adherence to the Mediterranean Diet and Sleep Disturbances Are Associated with Migraine Chronification and Disability among an Adult Population in the Lazio Region, Italy. Nutrients. 2024; 16(13):2169. https://doi.org/10.3390/nu16132169
Chicago/Turabian StyleBovenzi, Roberta, Annalisa Noce, Matteo Conti, Manuela Di Lauro, Barbara Chiaramonte, David Della Morte, Alessandro Stefani, Antonino De Lorenzo, Nicola Biagio Mercuri, and Maria Albanese. 2024. "Poor Adherence to the Mediterranean Diet and Sleep Disturbances Are Associated with Migraine Chronification and Disability among an Adult Population in the Lazio Region, Italy" Nutrients 16, no. 13: 2169. https://doi.org/10.3390/nu16132169
APA StyleBovenzi, R., Noce, A., Conti, M., Di Lauro, M., Chiaramonte, B., Della Morte, D., Stefani, A., De Lorenzo, A., Mercuri, N. B., & Albanese, M. (2024). Poor Adherence to the Mediterranean Diet and Sleep Disturbances Are Associated with Migraine Chronification and Disability among an Adult Population in the Lazio Region, Italy. Nutrients, 16(13), 2169. https://doi.org/10.3390/nu16132169