Abstract
Introduction: Type 1 Diabetes (T1D) affects over 9 million worldwide and necessitates meticulous self-management for blood glucose (BG) control. Utilizing BG prediction technology allows for increased BG control and a reduction in the diabetes burden caused by self-management requirements. This paper reviews BG prediction models in T1D, which include nutritional components. Method: A systematic search, utilizing the PRISMA guidelines, identified articles focusing on BG prediction algorithms for T1D that incorporate nutritional variables. Eligible studies were screened and analyzed for model type, inclusion of additional aspects in the model, prediction horizon, patient population, inputs, and accuracy. Results: The study categorizes 138 blood glucose prediction models into data-driven (54%), physiological (14%), and hybrid (33%) types. Prediction horizons of ≤30 min are used in 36% of models, 31–60 min in 34%, 61–90 min in 11%, 91–120 min in 10%, and >120 min in 9%. Neural networks are the most used data-driven technique (47%), and simple carbohydrate intake is commonly included in models (data-driven: 72%, physiological: 52%, hybrid: 67%). Real or free-living data are predominantly used (83%). Conclusion: The primary goal of blood glucose prediction in T1D is to enable informed decisions and maintain safe BG levels, considering the impact of all nutrients for meal planning and clinical relevance.
1. Introduction
Type 1 Diabetes (T1D) affects more than 9 million people worldwide, with its prevalence increasing by 5% annually [1]. This chronic auto-immune disease results in the inability to produce insulin, requiring self-monitoring and self-management to maintain blood glucose (BG) levels within the optimal range [2,3,4]. Effective BG management requires a balance of BG monitoring, precise exogenous insulin administration (both mealtime and long-acting), appropriate diet intake, and physical activity. Crucial to overall BG management is the management of the mealtime glucose response, the inadequate management of which contributes to a reduced time spent within the target blood glucose range of 3.9–10mmol/L (Time in Range; TIR), leading to an elevated HbA1C (a marker of overall glycemic control) [5,6,7].
BG prediction is a fundamental tool for managing BG levels, resulting in an improvement in the quality of life in people living with T1D (PwT1D) [8]. BG prediction proposes therapeutic solutions, which are critical to the artificial pancreas (AP) systems aiming to optimize BG levels and increase TIR [9]. BG prediction supports disease management through meal planning and insulin dosing suggestions based on BG levels and can be enhanced by including meal composition and volume, previous glycemic excursions, and guidance from the patient’s medical team [10].
Driven by the need to improve BG prediction accuracy and reduce patient burden, there has been extensive research in this field [11]. However, the modeling of the mealtime BG response is complex due to the non-linear nature and magnitude of confounding factors [12,13]. This paper reviews the available literature on the three main primary model strategies (physiological, data-driven, and hybrid models) for BG level prediction T1D, which include nutritional aspects in the prediction model. By analyzing commonly used techniques and the limitations within each of the strategies, the paper aims to provide recommendations for a clinically safe and effective blood glucose prediction model that minimizes user burden while enhancing prediction accuracy using nutritional inputs.
2. Related Literature
Work into predicting BG levels at pre-set prediction horizons (PH) [14] has evolved from using historical BG values [15], highlighting the crucial role played by other lifestyle factors, such as nutritional intake in BG dynamics [14,16]. To ensure clinical effectiveness, predictive algorithms must mimic the patient’s unique physiology while adjusting for external factors and be adaptable to the unpredictability of daily life [9,17].
Three approaches have been used to develop BG prediction models, namely, physiological, data-driven, and hybrid prediction models [9]. A prediction model with nutrition inputs at its core would offer an alternative to the three traditional model types. In this light, the authors focus on the role of nutritional factors in enhancing various BG prediction models.
2.1. Physiological Blood Glucose Prediction Models
Physiological BG prediction models mimic the glucose regulatory dynamics within various systems of the body [16]. To ensure accurate prediction outputs, the model needs to accurately set the physiological parameters based on a thorough understanding of insulin and glucose metabolism.
This approach necessitates prior knowledge of the underlying principles of action for the physiological and biological systems involved, specifically the glucose–insulin system [9,14,18]. This technique incorporates compartmental models to simulate human BG dynamics and includes additional aspects such as subcutaneous insulin absorption profiles, carbohydrate digestion and absorption, insulin action, and glucose kinetics [9,19].
Physiological BG prediction models are limited by the inherent assumption that the physiological processes controlling the glycemic response to food intake or lifestyle events are reproducible between individuals [12]. Factors that disturb the glucose balance, such as meal intake, are required to be announced for physiological models through self-reporting, which is another limiting aspect of this approach. The inter-patient variability in meal announcement can fluctuate by 30% in the interpretation of the composition of identical meals [20], increasing the need for calibration [21]. Further to the discrepancy in reporting, the inter-patient variability in physiological response makes personalization of physiological models difficult to achieve; in a non-diabetic population, it has been shown that 6% of the mealtime glycemic response variance is linked to person-specific factors [22,23].
2.2. Data-Driven Blood Glucose Prediction Models
Data-driven models facilitate BG predictions without prior knowledge, which is key to the physiological prediction models. These models can be based solely on Continuous Glucose Monitor (CGM) inputs, with optional additions of self-reported lifestyle information, such as food intake [24,25], which are the focus of this review. A wide range of data-driven techniques are presented in the literature, with varying core models and additional features utilized. Artificial neural networks (ANNs) have been shown as effective in health-aligned tasks [12] due to their large number of interconnected processing nodes, enabling pattern recognition in complex relationships. Feed-forward neural networks (FFNNs) make up 20% of the reports cited, depending on the features utilized [14].
Time series models rely on historical BG values and utilize linear functions to predict future readings [26]. Regression models utilize statistical algorithms to predict future BG levels based on historical BG values, insulin doses, and other factors, such as physical activity and meal composition. Decision trees, through the utilization of numerical and categorical data, are particularly useful for predicting BG levels based on categorical factors such as food intake, physical activity, and other lifestyle factors [14]. Support Vector Regression (SVR) techniques enable the isolation of patterns not discernible through human analysis, enabling BG prediction based on habitual patterns of human life [27]. The capacity of SVR to handle non-linear relationships makes SVR a promising technique in BG prediction and allows for the personalization of the models, which improves the accuracy of BG prediction. Data-driven models rely on non-physiological formulations to predict and are often built and validated on in silico data, which fail to account for the inter- and intra-subject variability in glucose dynamics at the detriment of physiological meaning [9,28,29]
2.3. Hybrid Blood Glucose Prediction Models
Hybrid models for BG prediction represent a fusion of physiological and data-driven methods, leveraging the strengths of both approaches to enhance accuracy. In these models, the physiological components of carbohydrate digestion and absorption, as well as insulin action and absorption profiles, are integrated into the pre-processing stage of the data-driven model [28]. The result is a personalized model that utilizes patient inputs, including self-reported information and mathematical equations, to optimize prediction accuracy [30]. Although this integration increases the complexity of the algorithm, it has the potential to provide more accurate predictions. However, it is important to note that hybrid models can be limited by biases in the training data and the clinical or demographic factors ingrained in the physiological model. Hybrid models utilize simple physiological models that require meal and/or insulin absorption profiles and then fit into a data-driven model to predict future BG values. However, it is important to note that hybrid models can be limited by biases in the training data and the clinical or demographic factors ingrained in the physiological model. These models require parameter tuning, which increases in complexity with multiple models that need to work effectively together to ensure accurate prediction.
3. Methodology
The present review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) [31] guidelines to establish a robust methodology. The search was restricted to studies that specifically incorporated nutritional variables as a prominent component in the BG prediction models, given the broad spectrum of input variables that have been utilized in existing prediction models.
3.1. Data Sources and Search Strategy
The initial identification of relevant literature was achieved by conducting a comprehensive search through digital libraries, including Google Scholar [32] and PubMed [33]. These platforms were selected as they encompass both the clinical and technical aspects of the inquiry. Specifically, Google Scholar was utilized due to its comprehensive coverage of technical conference papers.
The search criteria employed in this review included the following keywords: “Blood glucose prediction” AND Carbohydrate OR Nutrition OR “Nutritional Information” OR “Mixed Meals” AND “Type 1 Diabetes” OR T1DM.
3.2. Eligibility Criteria
The eligibility of articles was as follows:
- Publications written in English;
- Publications peer-reviewed and published by 1 May 2024;
- Publications focused on a Type 1 Diabetes population;
- Focused on blood glucose prediction algorithms without hyper/hypo-glycemia prevention;
- Prediction algorithms, including carbohydrate content or meal inputs;
- Conference papers or academic journal articles.
3.3. Study Selection
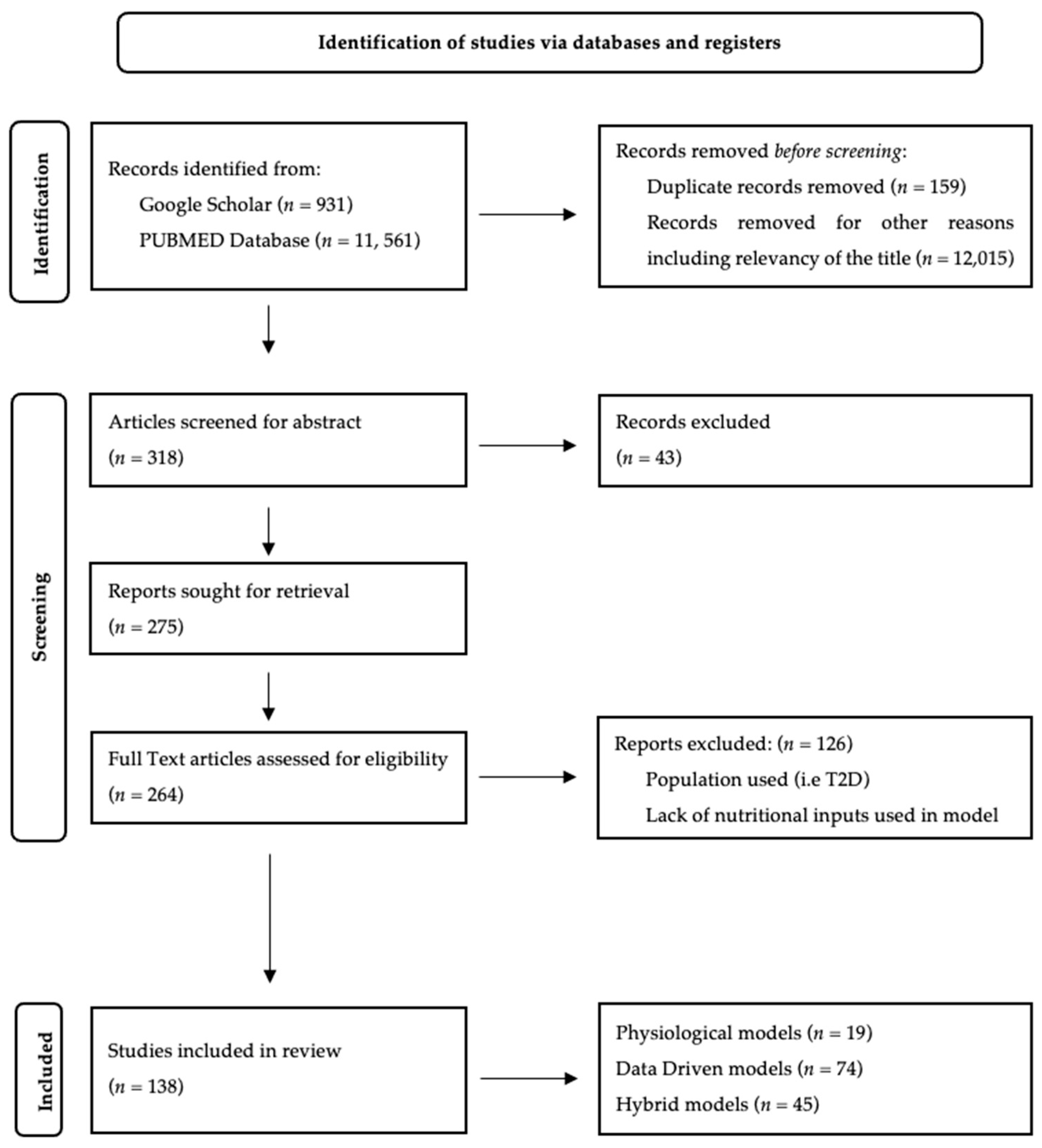
Once the databases had been queried/searched, Mendeley [34] reference manager was used to remove duplicates. The remaining references were evaluated for inclusion, and this was performed by screening for title and abstract, and finally, the full text was evaluated. The selection process is outlined in the PRISMA flow diagram (Figure 1). Using the framework outlined in Oviedo et al. [9], the features included in the summary tables are presented below. In cases where the information is not explicitly stated, the section is left blank.
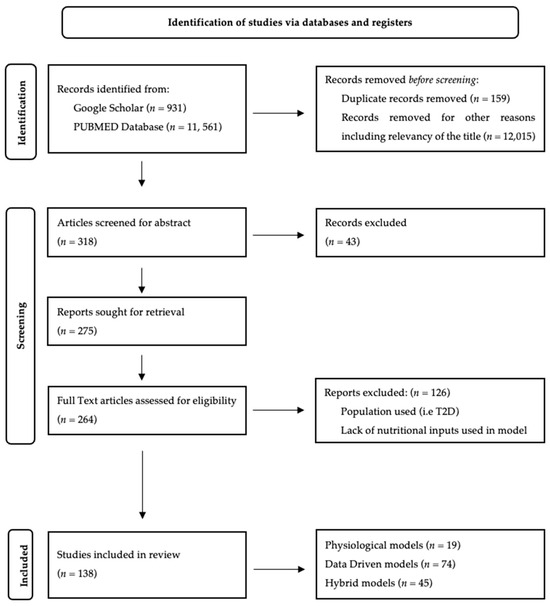
Figure 1.
Flow diagram for the identification of selected studies based on the PRISMA guidelines [31].
- Author: This includes the authors listed on the publication, the reference number, and the year of publication.
- Model Type: The core model used for the prediction is outlined; this includes previously published physiological models and data-driven prediction techniques.
- Additional Aspects: Any additional techniques used to supplement the core model used.
- Sub-Systems: This feature in the physiological and hybrid model summary tables highlights any absorption profiles included in the model and details the compartment models presented.
- Prediction Horizon: Highlights the time frame used in the prediction model.
- Patients: Here, the population included is outlined. The population is classified as “real” (where the model is validated using real-world data either in an in-patient setting or T1DM outpatients and/or their data) or simulated (where simulated patient data were used for validation).
- Inputs Used: Here, the checkmark indicates the use of GCM or BG data from self-monitoring blood glucose (SMBG) methods, insulin administration, carbohydrate intake, and/or mixed meals (carbohydrate/protein/fat/fiber).
- Additional Inputs: Any other included factors are presented here, such as physical activity, insulin-to-carbohydrate ratios, and sleep.
- Accuracy: Where reported, the models’ performance is indicated, and the metrics used are included along with the measurement used.
4. Results
As depicted in Figure 1, the identified unique prediction models (n = 138) can be broadly categorized into three types: data-driven blood glucose prediction models (n = 74), physiological blood glucose prediction models (n = 19), and hybrid blood glucose prediction models (n = 45).
A range of prediction horizons is proposed in the literature, with prediction horizons ≤30 min being used in 36% of blood glucose prediction models reported. Prediction horizons of 31–60 min were explored less frequently (34%) than prediction horizons 61–90 min (11%) and 91–120 min (10%) and >120 min (9%).
4.1. Physiological Blood Glucose Prediction Models
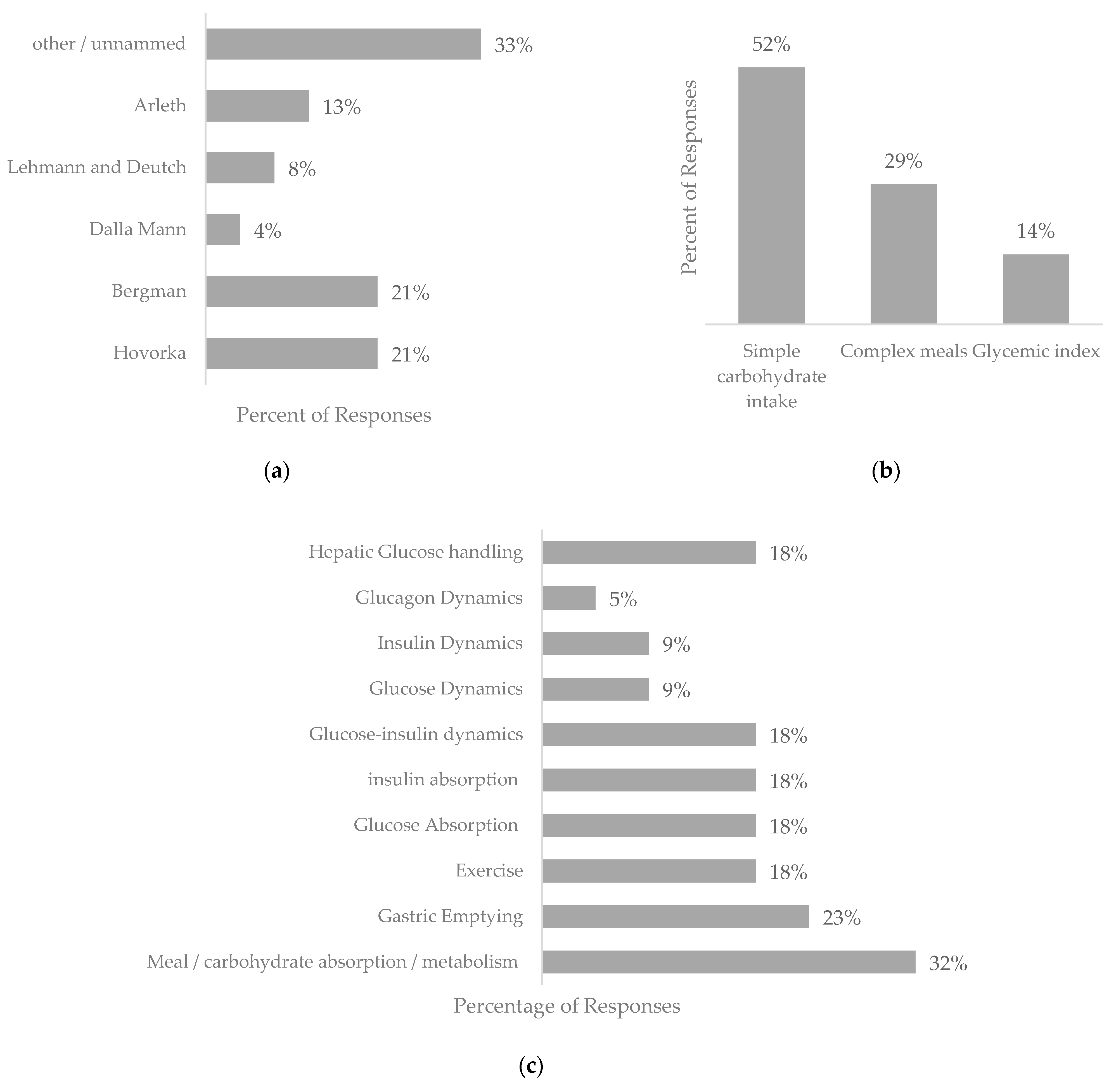
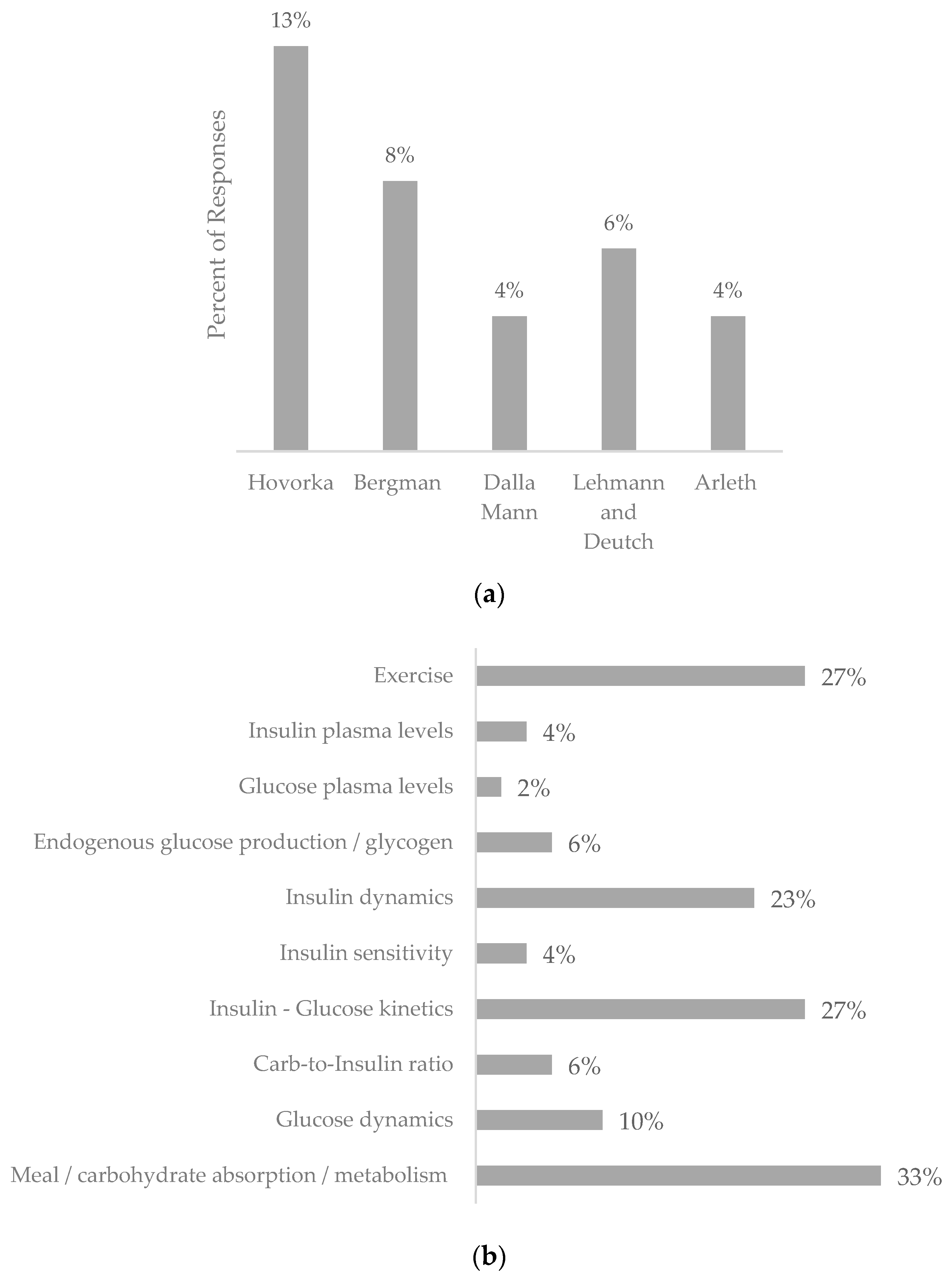
The review retrieved 19 pieces of work based on physiological models that explicitly used nutritional intakes in the model; a summary of these can be found in Table S1 (Supplementary Information). The physiological models presented comprise five cornerstone models, along with adaptations and novel approaches, as represented in Figure 2a–d.
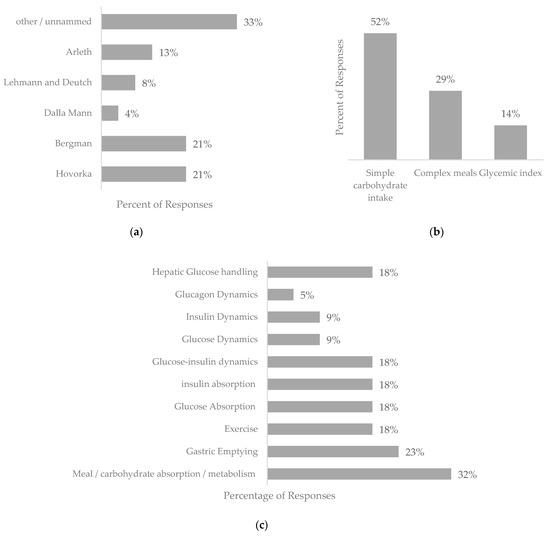
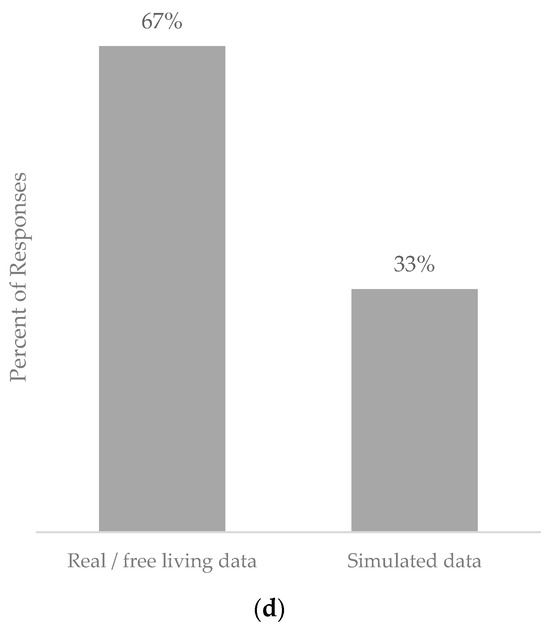
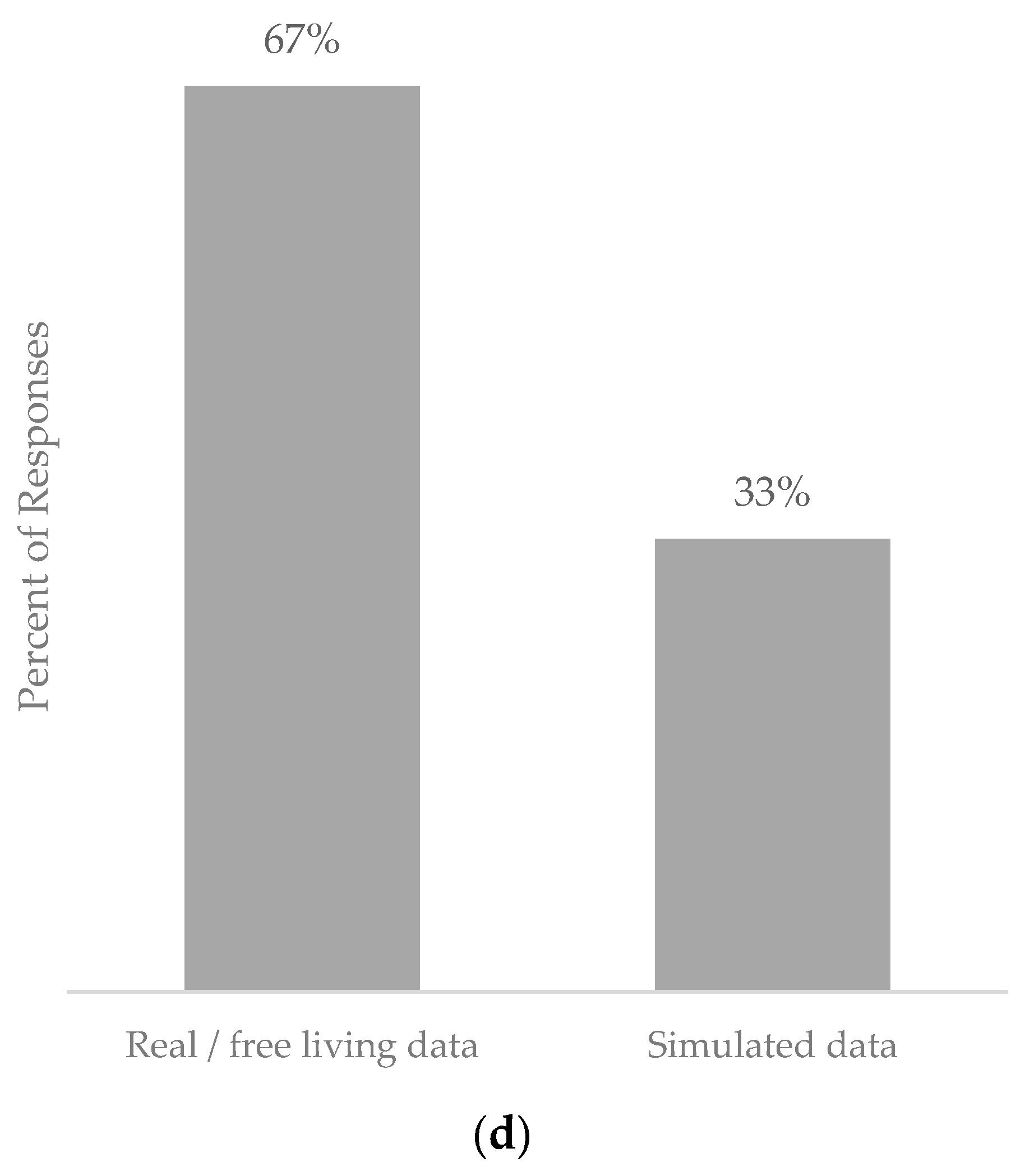
Figure 2.
Graphs depicting the features included within the physiological blood glucose prediction models returned in this systematic review. (a) Indication of the models represented within the physiological models presented. (b) Representation of nutritional input type in physiological models. (c) Representation of physiological aspects included in physiological models. (d) Representation of population type in physiological models.
Physiological BG prediction models can be classified into two types: “minimal models” and “comprehensive models”. “Minimal models” encompass glucose metabolism and insulin action, while “comprehensive models” incorporate a wide range of intricate physiological variables to mimic real-world scenarios. Figure 2c highlights the aspects included in the physiological models presented in this review.
The incorporation of the rate at which glucose enters the bloodstream is approached in different ways. Notably, the absorption profile of ingested food accounts for carbohydrate absorption at different points throughout the digestive system. Given the parameters of this review, all records incorporated nutritional intake in some regard. Simple carbohydrate intake was featured in 52%, while complex meals were considered in 29% of the reviews. However, other physiological factors that affect absorption profiles, such as glycemic index (14%) and gastric emptying rate (23%), which pertains to the pace at which food is expelled from the stomach into the small intestine, are infrequently integrated as independent features in the physiological models presented in the literature. An alternative rate of glucose appearance, stemming from endogenous glucose production or glycogen conversion, is featured in four of the physiological models identified in this study.
It is noteworthy that the prediction horizon was not explicitly stated in all the identified models. Of those models that specified a prediction horizon, short-term prediction horizons were the most frequently tested, with 31–60 min (29%) being the most common. Mid-term prediction horizons of 61–90 min (18%) and 91–120 min (18%) were also reported in some of the models. Frequently used prediction horizons include ≤30 min (6%) and ≥120 min (6%). Finally, prediction horizons of 24 h are used twice (12%), as is 6 h (12%).
4.2. Data-Driven Blood Glucose Prediction Models
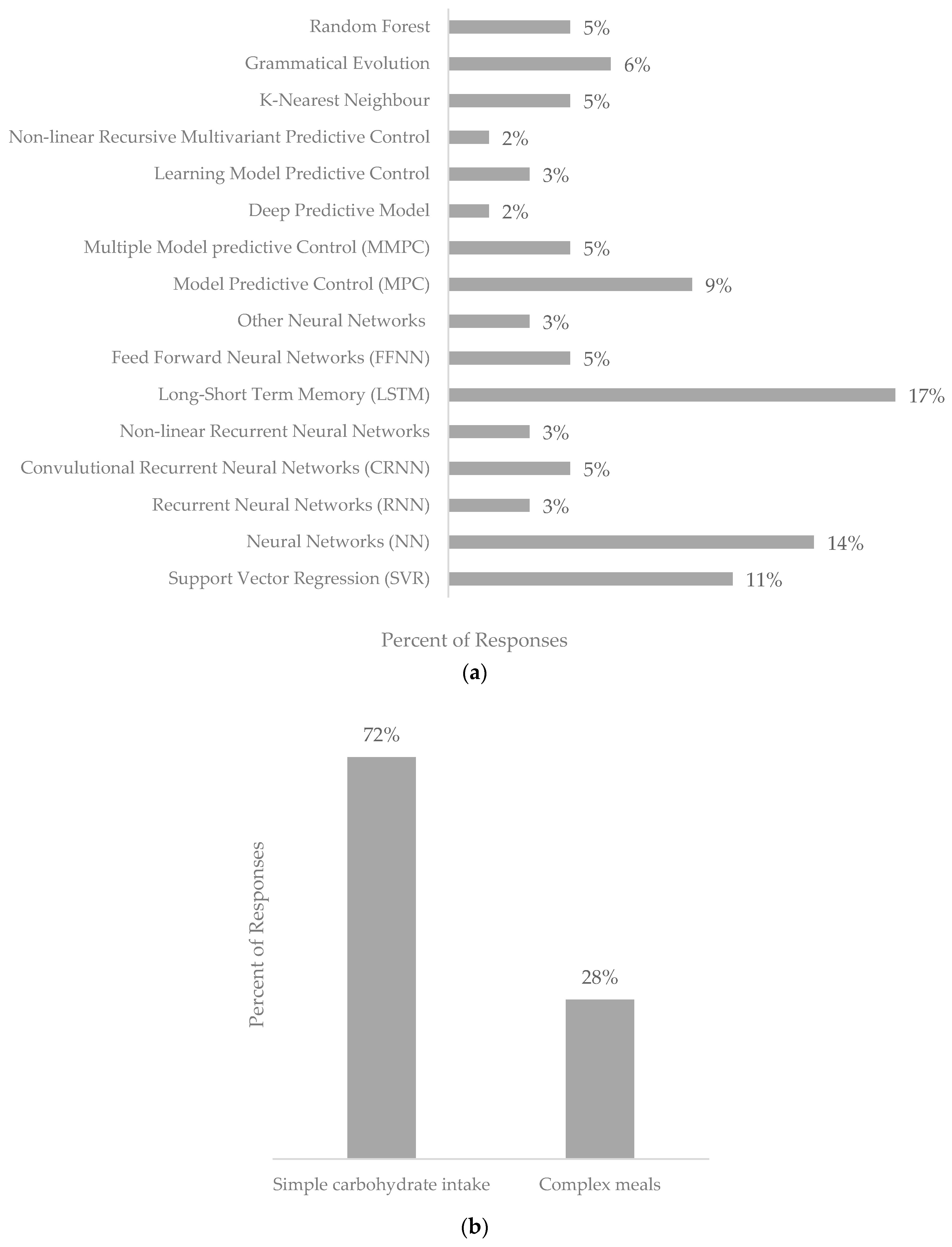
The search identified 74 unique records featuring data-driven BG prediction models, as shown in Table S2 (Supplementary Information). The features included in the returned data-driven blood glucose prediction models are highlighted in Figure 3a–c.
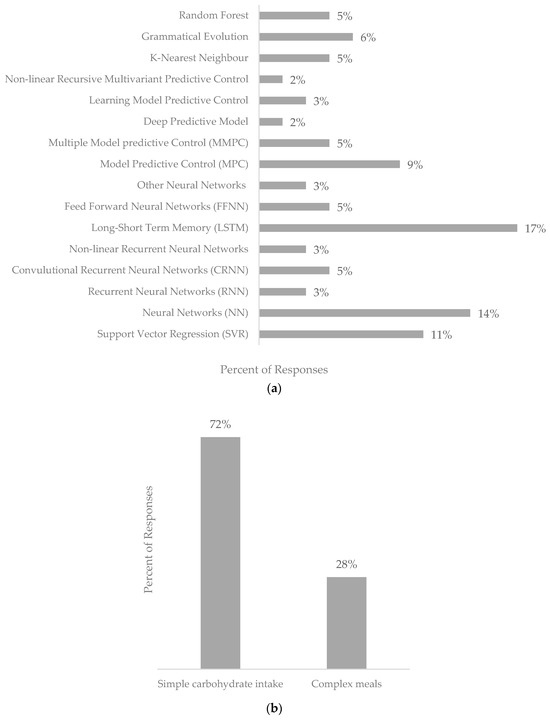
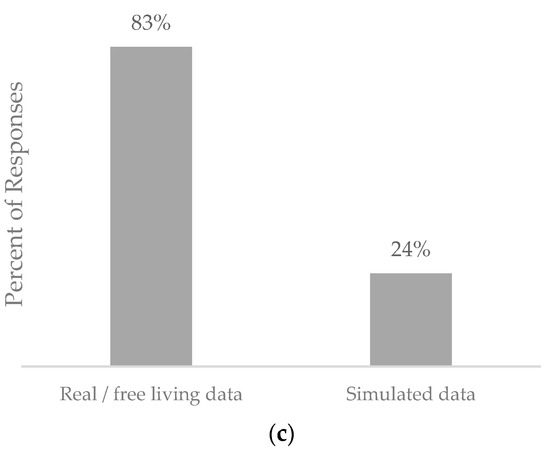
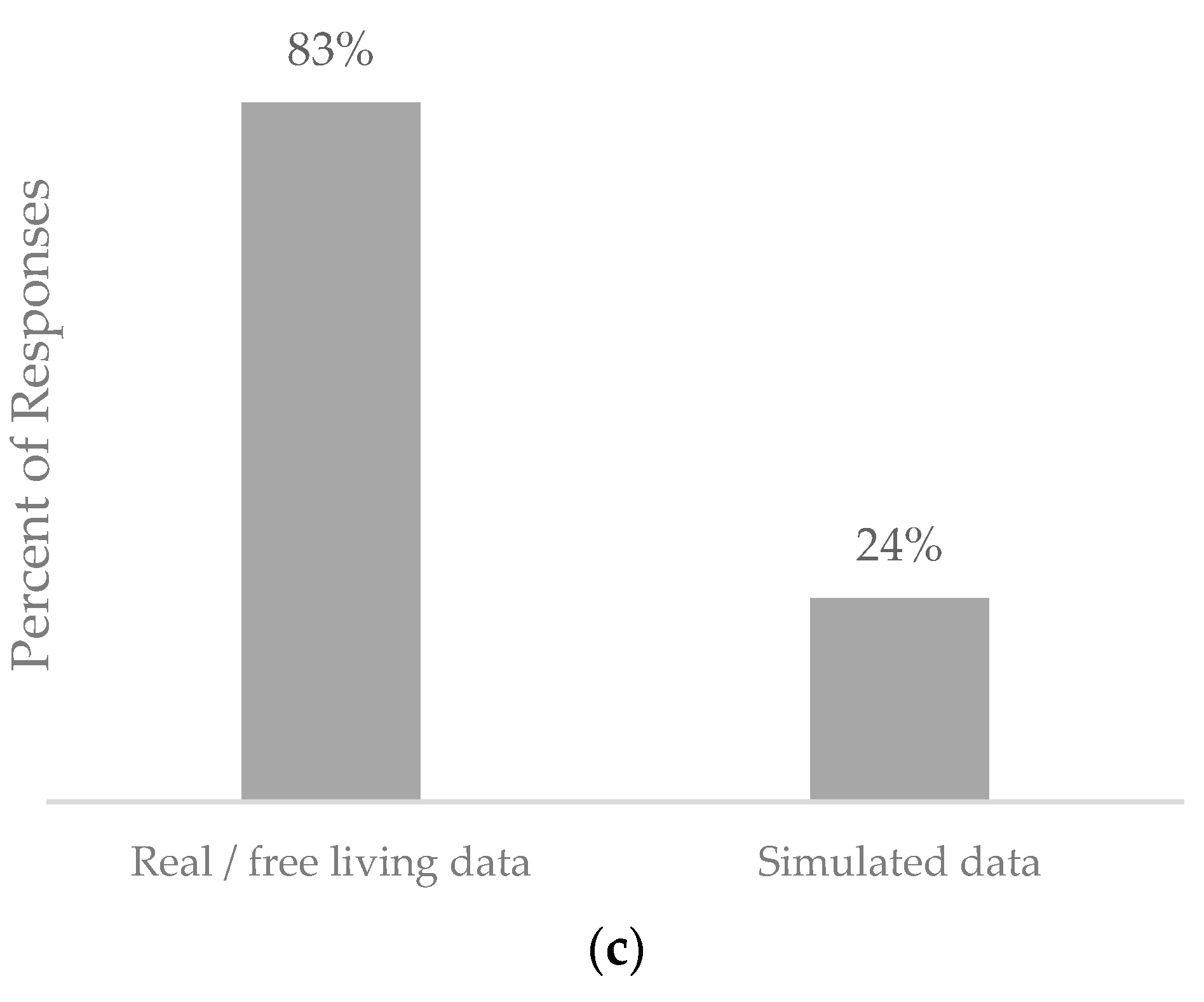
Figure 3.
Graphs depicting the features included within the data-driven blood glucose prediction models returned in this systematic review. (a) Representation of techniques used in data-driven blood glucose models. (b) Representation of nutritional inputs featured in data-driven blood glucose prediction models. (c) Representation of populations used in hybrid blood glucose prediction models.
While there is no clear preferred technique, neural networks (NNs) were the most used, with 47% of the prediction models using a form of neural network, followed by Support Vector Regression (SVR) used in 29% of the presented data-driven blood glucose prediction models. Other techniques were less frequently used, the distribution of which is shown in Figure 3a. Several neural network architectures are used in blood glucose prediction, with 25% of the neural networks presented being feedforward neural networks, recurrent neural networks (35%), and LSTM (25%) and convolution neural networks (16%). These algorithms can be trained utilizing various techniques, such as backpropagation, stochastic gradient descent, and other optimization algorithms.
In terms of nutritional inputs, simple carbohydrate intake was the most included variable (72%), with complex meals being used in 28% of the data-driven prediction models presented.
Regarding patient profiles, most studies (83%) used real or free-living data from individuals with diabetes, while simulated data were used in 24% of studies, raising potential issues regarding the generalizability of the results to real-world settings.
The prediction horizon used varied between ≤30 min (45%), 31–60 min (36%), 61–90 min (10%), 91–120 min (8%), and ≥121 min (2%).
4.3. Hybrid Prediction Models
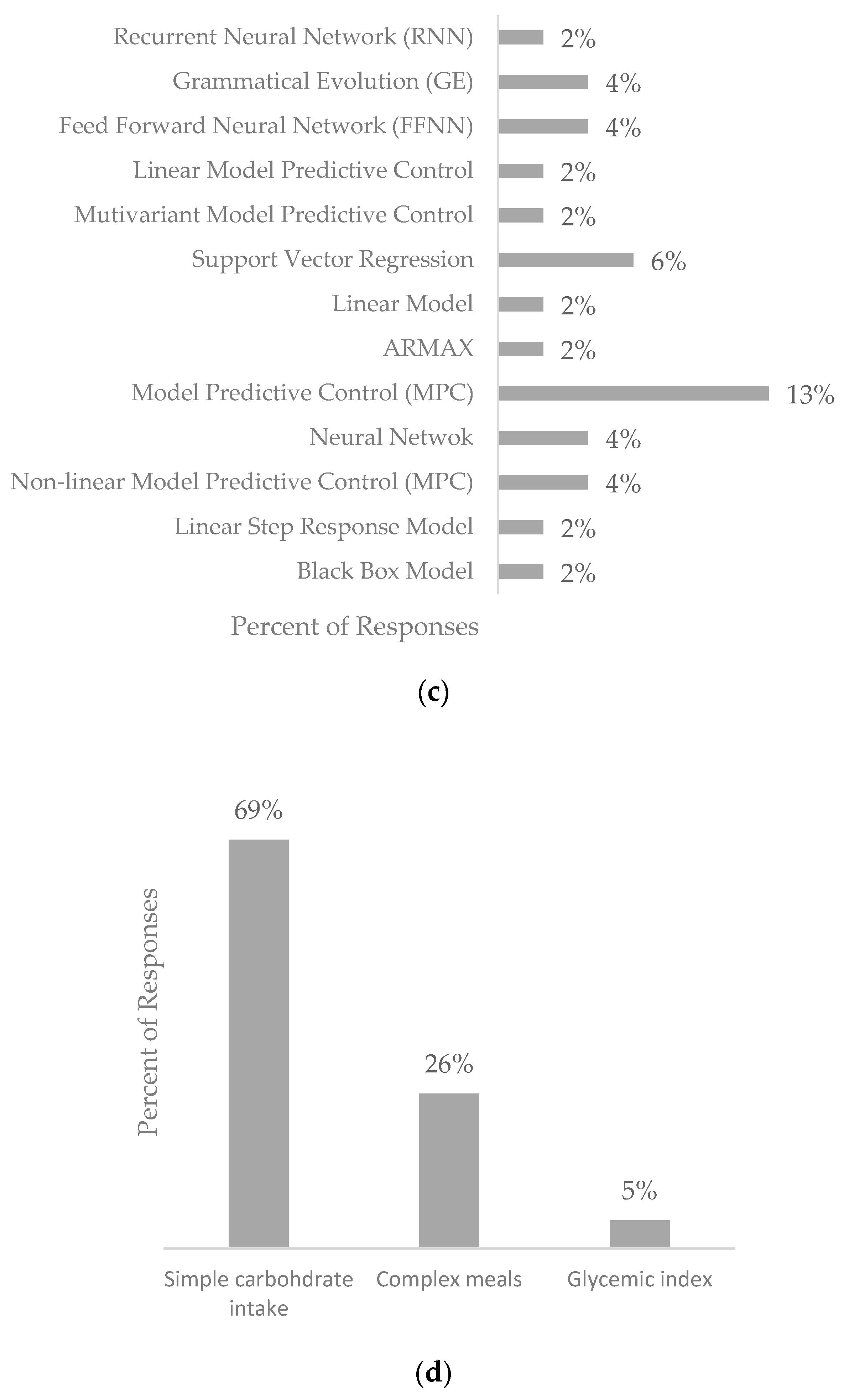
The review returned 45 pieces of work proposing hybrid blood glucose prediction models outlined in Table S3 (Supplementary Information). The physiological models and data-driven techniques utilized, along with nutritional inputs and physiological features proposed by the returned hybrid models, are shown in Figure 4a–d.
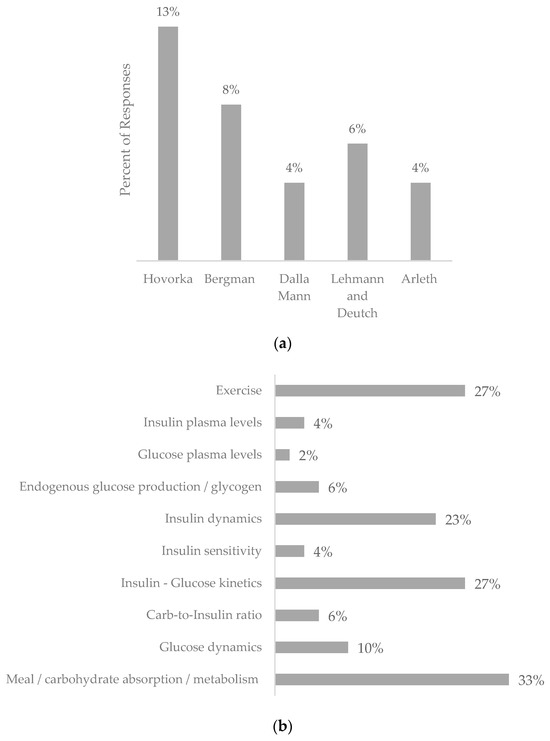
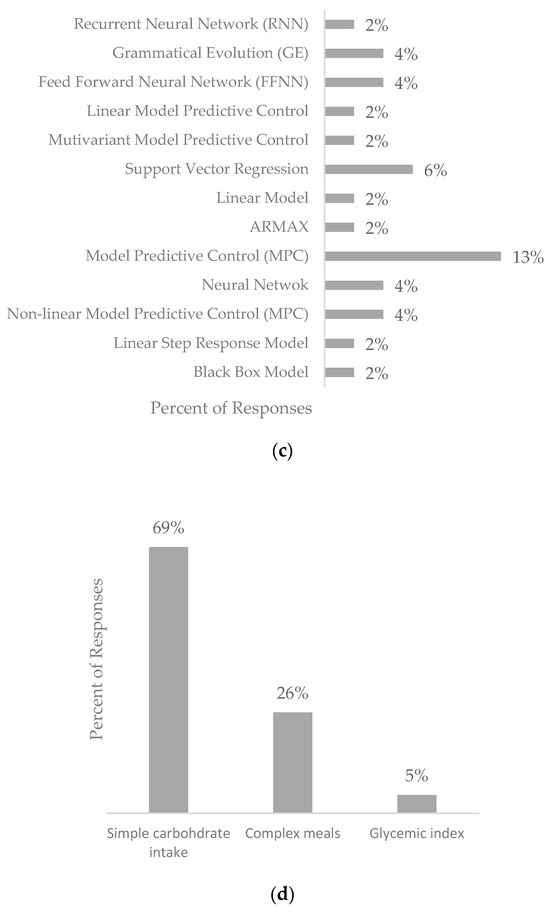
Figure 4.
Graphs depicting the features included within the hybrid blood glucose prediction models returned in this systematic review. (a). Representation of physiological models used in hybrid blood glucose prediction models. (b). Representation of physiological features used in hybrid blood glucose prediction models. (c). Representation of the data-driven models used in hybrid blood glucose prediction models. (d). Representation of nutritional inputs featured in hybrid blood glucose prediction models.
Filters were employed in 37.5% of the identified hybrid studies, with the Kalman filter being the most used filter, accounting for 15% of the studies. Bayesian and Gaussian distribution filters were also used in 6% of each study.
Regarding the detail of carbohydrates included, simple carbohydrate intake was the most included aspect (69%), followed by complex meals (26%) and glycemic index (5%). Finally, real/free-living data was the most used patient profile (60%), followed by simulated data (40%).
The prediction horizon used varied between <30 min (31%), 30–60 min (33%), 60–120 min (23%), and >120 min (13%).
5. Discussion
The complexity and non-linear nature of the human glucose regulatory system pose a challenge for BG prediction. To ensure an accurate BG prediction that is pragmatically valid, clinically observed trends in glucose metabolism should be considered and incorporated into the model framework [35].
Assessing the accuracy of BG prediction models can be limited by various factors, including the methodology employed, the variation in populations (real versus simulated), and the sample size. The Root Mean Square Error (RMSE) is the gold standard for assessing the accuracy of blood glucose prediction algorithms [36]; alternative assessment methods are also used, including the Clarke Error Grid, which quantifies clinical accuracy [37]. The use of multiple assessment methods allows for comparison between different prediction models [38], which would be otherwise unachievable without running the individual datasets through each presented model.
5.1. Validity of Different Model Types
The complexity of T1D and the non-linear nature of BG values present a challenge for accurate BG prediction in real-world settings. With at least 42 contributing factors to glucose dynamics, each model type presents a unique perspective on BG prediction. Physiological models, while perceived as time-consuming [9], allow for the absorption profiles of administered insulin and nutritional intake to be factored in, which are the main contributors to BG fluctuations. The Hovorka model incorporates the effects of meals, physical activity, and insulin doses tuned to the individual, enhancing the accuracy and clinical efficiency, which is potentially the reason it is a frequently used model in physiological and hybrid BG predictions with real-world clinical applications. The Bergman “minimal model” is often used in research and exploratory settings due to its simplicity and ease of use while capturing the essential elements of BG dynamics. Data-driven models, on the other hand, do not require clinical knowledge and allow for predictions to be made from historical information captured from BG sensor devices or manually entered by the user. Hybrid models, as the name suggests, use physiological aspects in the pre-processing stage and use the outputs for the data-driven models.
Given the large number of factors contributing to BG regulation, there needs to be a balance between the complexity of the prediction model and its reliability. The model must be complex enough to offer reliable results while being able to be personalized [10]. The different methods proposed in the literature each have challenges and benefits. There are more data-driven models presented due to the vast array of machine learning techniques available. Making a direct comparison between the techniques would have limited meaning due to the different datasets, prediction horizons, and models used [9].
Neural networks, the most frequently used data-driven technique (47% of returned manuscripts), are trained on extensive datasets encompassing information on meal composition, insulin levels, physical activity, and other physiological parameters, as well as corresponding BG levels. The neural network algorithm can then identify patterns and relationships among these variables and utilize this knowledge to predict future BG levels based on new input data. Additionally, neural networks can learn and adapt to new data over time, allowing for continual improvement of predictions as new data become available [39]. The benefits of using neural networks in BG prediction and one of the reasons for their popularity is their ability to model the complex non-linear nature of BG dynamics. RNNs and LSTMs are able to learn and adapt to new data, which is advantageous in the real world where PwT1D is continuously undertaking new experiences, eating different meals, and providing new data to the prediction model.
In the context of BG prediction, SVR prediction models, used in 22% of all the prediction models presented here and 11% of the hybrid models, work by identifying a hyperplane that best separates the input data into different regions based on their corresponding blood glucose levels. The hyperplane is chosen to maximize the distance between the support vectors, which are the data points closest to the hyperplane. This process, called margin maximization, ensures that the model generalizes well to new data. SVR is particularly useful in situations where the relationship between the input variables, such as historical BG values and nutritional intake, and the output variable, predicted BG levels, is non-linear and complex. SVR uses kernel methods to transform input data into a higher-dimensional space, where the relationship between the variables may be more linear. One advantage of SVR is that it is less susceptible to overfitting than other regression techniques because it uses a regularization parameter to control the complexity of the model. Overall, the use of SVR in BG prediction has shown promising results and is likely to become an increasingly important tool in the development of personalized blood glucose prediction models for individuals with diabetes or other metabolic conditions [40,41].
SVRs are often chosen for the simplicity of the model and the accuracy in smaller datasets, making them beneficial in cases where limited historical BG data are available. The risk of overfitting SVR models can be mitigated with the right choice of kernel and regulation parameters.
One limitation of data-driven models is the quality of the input data, as much of BG management in T1D is reliant on self-reported food intake. Studies have shown that the carbohydrate content of a meal is under-reported by as much as 30% and is frequently underreported at 62.7% of the time, suggesting that two out of three meals have underreported carbohydrate content [20].
One of the key advantages of employing the Kalman filter in BG prediction models is its capacity to handle incomplete or missing data. The recursive algorithm of the Kalman filter updates the state estimates of the system based on new data, even if some measurements are incomplete or missing. This feature can prove especially valuable in situations where CGM data are disrupted or missing due to technical or other factors. Several studies have employed the Kalman filter to enhance the precision of data-driven blood glucose prediction models. Utilizing a Kalman filter to estimate the BG levels of PwT1D by utilizing CGM data enhances the precision of the predictions compared to a standard linear regression model.
5.2. Prediction Horizons
In 70% of the studies that specified prediction horizons for all three classifications, the horizons were found to be below 60 min. However, a small percentage (9%) of studies allowed for a prediction horizon above 120 min. It is important to consider the time frames of meal absorption, as discussed in the section below, along with the insulin absorption profiles, in evaluating the clinical relevance of blood glucose predictions at both short- and mid-term horizons.
5.3. Impact of Nutritional Intake on Prediction Models
Although isolated carbohydrate intake is typically used as the primary input (71% of returned manuscripts across all prediction model types in this review), this approach neglects other essential factors such as glycemic index, protein, lipids, fiber, and total energy intake. Carbohydrate intake and insulin administration are the primary determinants of BG levels, and their timing and dosing are crucial for optimal BG regulation [42]. Relying solely on carbohydrate intake has its limitations in accurately determining mealtime glycemic response. The absorption time frame of food is determined by the rate of glucose absorption, which varies based on the overall meal composition and can impact the rise and fall of blood glucose levels. Several carbohydrate absorption models have been proposed in the literature, some of which were formulated for non-diabetic populations and adapted for PwT1D. A one-compartment model [43], based on the stomach, does not account for the glycemic index, fiber content, or other nutrients besides carbohydrates, while a two-compartment model [44] that includes intestinal absorption considers the timing of absorption. These compartmental models have been expanded to incorporate the breakdown of lipids, proteins, dietary fiber, and starch into monosaccharides, with five compartments: the stomach, intestine, starch breakdown, intestinal glucose absorption, and gastric emptying [7].
The concept of the glycemic index [4] allows for the quantification of physiological responses to different types of carbohydrates in mealtime conditions. Although not directly prescribed for the nutritional management of T1D, the glycemic index can impact the absorption profile of carbohydrates and the post-prandial glucose response. Foods with a lower glycemic index have been shown to have 15% higher bioavailability compared to those with a higher glycemic index, indicating that higher glycemic index meals are absorbed more quickly and have an impact on immediate post-prandial blood glucose levels [45]. High glycemic index meals are fully absorbed within five hours of consumption, highlighting the importance of considering glycemic index in predicting blood glucose levels and estimating remaining carbohydrates for subsequent meals [46,47].
The inclusion of complex meals as input in BG prediction models accounts for the dynamic and complex nature of BG regulation, influenced by multiple factors such as meal timing and composition, insulin levels, physical activity, and other physiological parameters.
Factoring in the need for nutritional information, the burden on users needs to be factored in. Although there is motivation to report nutritional intake when improved BG control is the outcome, nutrition reporting has been shown to cause stress, and continued retention is limited. Perhaps a BG model that factors in the natural detail of nutrition reporting [48], which reflects the entire meal composition (i.e., a one-word meal tag), could combat this burden and provide the necessary context for an accurate BG prediction.
5.4. Population Used
The majority of the studies across all the model types (71% of the returned prediction models) used real or free-living data from individuals with diabetes. Simulated data were also used in a substantial proportion of studies (29% of returned manuscripts), which may have implications for the generalizability of the results to real-world settings. Simulated populations, however, cannot fully mimic additional aspects of BG variations, such as mood and sleep patterns, which factor into the inter-patient variability. Consequently, simulated populations tend to offer smaller RMSE than models tested on real-world patients [7]. Many simulation models for T1D are constructed by amalgamating data from diverse clinical trials with varying participant characteristics, leading to inconsistencies in the data synthesis process. This can introduce biases and inaccuracies in the predictive capabilities of the models. These limitations impact the reliability, generalizability, and clinical applicability of BG prediction models modeled on simulated populations [49].
Overall, these results highlight the diverse range of physiological and data-driven models, filters, and carbohydrate inputs used in hybrid blood glucose prediction models, as well as the importance of considering the patient profile of the datasets used. Further research is needed to determine the optimal combinations of these elements for accurate and reliable blood glucose prediction in different patient populations and settings.
The dataset utilized is crucial to ensuring the generalizability of BG prediction models. Small datasets potentially lead to misleading trends and decreased generalizability. Different model types are more prone to over-fitting. However, because of individual physiological differences in BG regulation, a BG prediction model needs to be tailored to the individual. Even more important than the dataset itself is the amount of data or training time used to develop these models. Insufficient data or training can result in the model performing poorly in real-world or unforeseen situations.
6. Limitations and Future Work
While systematic reviews offer a powerful tool for synthesizing the available research in the area, there are limitations. There is inherent publication bias, where studies with positive and significant results tend to be published, leading to an unbalanced perspective of the research field. In addition, there is bias in the review process, including the selection of studies, data extraction, and the interpretation of the results. This review focused solely on blood glucose prediction models, which included nutritional inputs, limiting the generalizability of blood glucose predictions.
7. Conclusions
The primary goal of blood glucose prediction in the context of T1D is to enable individuals to make informed decisions and maintain a safe BG level, particularly during the period between meals. Given that individuals consume food rather than individual macronutrients, it is crucial to consider the impact of other nutrients on BG levels both in the immediate timeframe and in nutrients on board at the next meal. In real-world scenarios, where individuals consume food every three to four hours, the ability to provide longer prediction horizons can facilitate future meal planning and have clinical relevance in an outpatient setting.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/nu16142214/s1. Table S1: Summary of Physiological Blood Glucose Prediction Model Approaches. Table S2: Summary of Data-Driven Blood Glucose Prediction Model Approaches. Table S3: Summary of Hybrid Blood Glucose Prediction Model Approaches. Refs [7,19,24,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156,157,158] are cited in Supplementary Materials.
Author Contributions
Conceptualization, N.L., H.T., P.W.N. and S.H.; Formal analysis, N.L.; Methodology, N.L., H.T., P.W.N. and S.H.; Supervision, H.T., P.W.N. and S.H.; Writing—original draft, N.L.; Writing—review and editing, N.L., H.T., P.W.N. and S.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
No ethical considerations.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- JDRF: Type 1 Diabetes Facts and Figures. Available online: https://jdrf.org.uk/information-support/about-type-1-diabetes/facts-and-figures/ (accessed on 6 October 2022).
- Atkinson, M.A.; Eisenbarth, G.S.; Michels, A.W. Type 1 Diabetes. Lancet 2014, 383, 69–82. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Diabetes (Type 1 and Type 2) in Children and Young People: Diagnosis and Management; National Institute for Health and Care Excellence: London, UK, 2015; p. 55. [Google Scholar]
- Jenkins, D.; Wolever, T.; Taylor, R.; Barker, H.; Fielden, H.; Baldwin, J.; Bowling, A.; Newman, H.; Jenkins, A.; Goff, D. Glycemic Index of Foods: A Physiological Basis for Carbohydrate Exchange. Am. J. Clin. Nutr. 1981, 34, 362–366. [Google Scholar] [CrossRef]
- Gabbay, M.A.L.; Rodacki, M.; Calliari, L.E.; Vianna, A.G.D.; Krakauer, M.; Pinto, M.S.; Reis, J.S.; Puñales, M.; Miranda, L.G.; Ramalho, A.C.; et al. Time in Range: A New Parameter to Evaluate Blood Glucose Control in Patients with Diabetes. Diabetol. Metab. Syndr. 2020, 12, 22. [Google Scholar] [CrossRef]
- Battelino, T.; Danne, T.; Bergenstal, R.M.; Amiel, S.A.; Beck, R.; Biester, T.; Bosi, E.; Buckingham, B.A.; Cefalu, W.T.; Close, K.L.; et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations from the International Consensus on Time in Range. Diabetes Care 2019, 42, 1593–1603. [Google Scholar] [CrossRef] [PubMed]
- Karim, R.A.H.; Vassányi, I.; Kósa, I. After-Meal Blood Glucose Level Prediction Using an Absorption Model for Neural Network Training. Comput. Biol. Med. 2020, 125, 103956. [Google Scholar] [CrossRef] [PubMed]
- Saiti, K.; Macaš, M.; Lhotská, L.; Štechová, K.; Pithová, P. Ensemble Methods in Combination with Compartment Models for Blood Glucose Level Prediction in Type 1 Diabetes Mellitus. Comput. Methods Programs Biomed. 2020, 196, 105628. [Google Scholar] [CrossRef] [PubMed]
- Oviedo, S.; Vehí, J.; Calm, R.; Armengol, J. A Review of Personalized Blood Glucose Prediction Strategies for T1DM Patients: Personalized Blood Glucose Prediction Strategies for T1D Patients. Int. J. Numer. Meth. Biomed. Engng. 2017, 33, e2833. [Google Scholar] [CrossRef] [PubMed]
- Karim, R.A.H.; Vassányi, I.; Kósa, I. Improved Methods for Mid-Term Blood Glucose Level Prediction Using Dietary and Insulin Logs. Medicina 2021, 57, 676. [Google Scholar] [CrossRef] [PubMed]
- Moreira, T.R.; Negreiros, F.D.D.S.; Aquino, M.D.J.N.D.; Silva, L.M.S.D.; Moreira, T.M.M.; Torres, R.A.M. Digital Technology and Its Effects on Knowledge Improvement for Diabetes Management: An Integrative Review. Int. J. Nurs. Pract. 2023, 29, e13029. [Google Scholar] [CrossRef] [PubMed]
- Annuzzi, G.; Apicella, A.; Arpaia, P.; Bozzetto, L.; Criscuolo, S.; Benedetto, E.D.; Pesola, M.; Prevete, R.; Vallefuoco, E. Impact of Nutritional Factors in Blood Glucose Prediction in Type 1 Diabetes through Machine Learning. IEEE Access 2023, 11, 17104–17115. [Google Scholar] [CrossRef]
- Butt, H.; Khosa, I.; Iftikhar, M.A. Feature Transformation for Efficient Blood Glucose Prediction in Type 1 Diabetes Mellitus Patients. Diagnostics 2023, 13, 340. [Google Scholar] [CrossRef] [PubMed]
- Woldaregay, A.Z.; Årsand, E.; Walderhaug, S.; Albers, D.; Mamykina, L.; Botsis, T.; Hartvigsen, G. Data-Driven Modeling and Prediction of Blood Glucose Dynamics: Machine Learning Applications in Type 1 Diabetes. Artif. Intell. Med. 2019, 98, 109–134. [Google Scholar] [CrossRef] [PubMed]
- Bremer, T.; Gough, D.A. Is Blood Glucose Predictable from Previous Values? A Solicitation for Data. Diabetes 1999, 48, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Munoz-Organero, M. Deep Physiological Model for Blood Glucose Prediction in T1DM Patients. Sensors 2020, 20, 3896. [Google Scholar] [CrossRef] [PubMed]
- Borle, N.C.; Ryan, E.A.; Greiner, R. The Challenge of Predicting Blood Glucose Concentration Changes in Patients with Type I Diabetes. Health Inform. J. 2021, 27, 146045822097758. [Google Scholar] [CrossRef]
- Georga, E.I.; Protopappas, V.C.; Polyzos, D.; Fotiadis, D.I. Online prediction of glucose concentration in type 1 diabetes using extreme learning machines. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2015, 2015, 3262–3265. [Google Scholar] [CrossRef] [PubMed]
- Calm, R.; García-Jaramillo, M.; Bondia, J.; Sainz, M.A.; Vehí, J. Comparison of Interval and Monte Carlo Simulation for the Prediction of Postprandial Glucose under Uncertainty in Type 1 Diabetes Mellitus. Comput. Methods Programs Biomed. 2011, 104, 325–332. [Google Scholar] [CrossRef]
- Brazeau, A.S.; Mircescu, H.; Desjardins, K.; Leroux, C.; Strychar, I.; Ekoé, J.M.; Rabasa-Lhoret, R. Carbohydrate Counting Accuracy and Blood Glucose Variability in Adults with Type 1 Diabetes. Diabetes Res. Clin. Pract. 2013, 99, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Aliberti, A.; Pupillo, I.; Terna, S.; Macii, E.; Di Cataldo, S.; Patti, E.; Acquaviva, A. A Multi-Patient Data-Driven Approach to Blood Glucose Prediction. IEEE Access 2019, 7, 69311–69325. [Google Scholar] [CrossRef]
- Berry, S.E.; Valdes, A.M.; Drew, D.A.; Asnicar, F.; Mazidi, M.; Wolf, J.; Capdevila, J.; Hadjigeorgiou, G.; Davies, R.; Al Khatib, H.; et al. Human Postprandial Responses to Food and Potential for Precision Nutrition. Nat. Med. 2020, 26, 964–973. [Google Scholar] [CrossRef] [PubMed]
- Zeevi, D.; Korem, T.; Zmora, N.; Israeli, D.; Rothschild, D.; Weinberger, A.; Ben-Yacov, O.; Lador, D.; Avnit-Sagi, T.; Lotan-Pompan, M.; et al. Personalized Nutrition by Prediction of Glycemic Responses. Cell 2015, 163, 1079–1094. [Google Scholar] [CrossRef]
- Georga, E.I.; Protopappas, V.C.; Ardigo, D.; Marina, M.; Zavaroni, I.; Polyzos, D.; Fotiadis, D.I. Multivariate Prediction of Subcutaneous Glucose Concentration in Type 1 Diabetes Patients Based on Support Vector Regression. IEEE J. Biomed. Health Inform. 2013, 17, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Balakrishnan, N.P.; Samavedham, L.; Rangaiah, G.P. Personalized Mechanistic Models for Exercise, Meal and Insulin Interventions in Children and Adolescents with Type 1 Diabetes. J. Theor. Biol. 2014, 357, 62–73. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rodríguez, I.; Chatzigiannakis, I.; Rodríguez, J.-V.; Maranghi, M.; Gentili, M.; Zamora-Izquierdo, M.-Á. Utility of Big Data in Predicting Short-Term Blood Glucose Levels in Type 1 Diabetes Mellitus through Machine Learning Techniques. Sensors 2019, 19, 4482. [Google Scholar] [CrossRef] [PubMed]
- Bunescu, R.; Struble, N.; Marling, C.; Shubrook, J.; Schwartz, F. Blood Glucose Level Prediction Using Physiological Models and Support Vector Regression. In Proceedings of the 2013 12th International Conference on Machine Learning and Applications, Miami, FL, USA, 4–7 December 2013; pp. 135–140. [Google Scholar]
- Contreras, I.; Oviedo, S.; Vettoretti, M.; Visentin, R.; Vehí, J. Personalized Blood Glucose Prediction: A Hybrid Approach Using Grammatical Evolution and Physiological Models. PLoS ONE 2017, 12, e0187754. [Google Scholar] [CrossRef]
- Felizardo, V.; Garcia, N.M.; Pombo, N.; Megdiche, I. Data-Based Algorithms and Models Using Diabetics Real Data for Blood Glucose and Hypoglycaemia Prediction–A Systematic Literature Review. Artif. Intell. Med. 2021, 118, 102120. [Google Scholar] [CrossRef] [PubMed]
- Pereira, J.P.A.; Brandão, A.A.F.; Da Silva Bevilacqua, J.; Correa Giannella, M.L.C. A Hybrid Model to Predict Glucose Oscillation for Patients with Type 1 Diabetes and Suggest Customized Recommendations. In Intelligent Systems and Applications; Bi, Y., Bhatia, R., Kapoor, S., Eds.; Advances in Intelligent Systems and Computing; Springer International Publishing: Cham, Switzerland, 2020; Volume 1038, pp. 790–801. ISBN 978-3-030-29512-7. [Google Scholar]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Google Scholar. Available online: https://scholar.google.com/#d=gs_hdr_drw&t=1714405788098 (accessed on 1 June 2022).
- PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov (accessed on 1 July 2022).
- Mendeley Reference Management Software 2024. Available online: www.mendeley.com (accessed on 1 June 2023).
- Asad, M.; Khan, Y.; Qamar, U.; Bashir, S. Blood Glucose Level Prediction Using Optimized Neural Network for Virtual Patients. In Intelligent Systems and Applications; Bi, Y., Bhatia, R., Kapoor, S., Eds.; Advances in Intelligent Systems and Computing; Springer International Publishing: Cham, Switzerland, 2020; Volume 1038, pp. 671–683. ISBN 978-3-030-29512-7. [Google Scholar]
- Willmott, C.; Matsuura, K. Advantages of the Mean Absolute Error (MAE) over the Root Mean Square Error (RMSE) in Assessing Average Model Performance. Clim. Res. 2005, 30, 79–82. [Google Scholar] [CrossRef]
- Mondal, H.; Mondal, S. Clarke Error Grid Analysis on Graph Paper and Microsoft Excel. J. Diabetes Sci. Technol. 2020, 14, 499. [Google Scholar] [CrossRef] [PubMed]
- Pustozerov, E.A.; Tkachuk, A.S.; Vasukova, E.A.; Anopova, A.D.; Kokina, M.A.; Gorelova, I.V.; Pervunina, T.M.; Grineva, E.N.; Popova, P.V. Machine Learning Approach for Postprandial Blood Glucose Prediction in Gestational Diabetes Mellitus. IEEE Access 2020, 8, 219308–219321. [Google Scholar] [CrossRef]
- Zecchin, C.; Facchinetti, A.; Sparacino, G.; Cobelli, C. Jump Neural Network for Online Short-Time Prediction of Blood Glucose from Continuous Monitoring Sensors and Meal Information. Comput. Methods Programs Biomed. 2014, 113, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhang, Y. Blood Glucose Prediction Using Support Vector Regression with Particle Swarm Optimization. J. Healthc. Eng. 2018, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Wang, Y.; Zhang, X. Blood Glucose Prediction Based on Support Vector Regression. J. Healthc. Eng. 2019, 1–9. [Google Scholar]
- Martínez-Delgado, L.; Munoz-Organero, M.; Queipo-Alvarez, P. Using Absorption Models for Insulin and Carbohydrates and Deep Leaning to Improve Glucose Level Predictions. Sensors 2021, 21, 5273. [Google Scholar] [CrossRef] [PubMed]
- Hejlesen, O.K.; Andreasseen, S.; Hovorka, R.; Cavan, D.A. DIAS-the Diabetes Advisory System: Technical and Physiological Aspects of the System and Evaluation Results Obtained so Far. Comput. Methods Programs Biomed. 1997, 54, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Arleth, T.; Andreassen, S.; Orsini-Federici, M.; Timi, A.; Massi-Benedetti, M. A Model of Glucose Absorption from Mixed Meals. IFAC Proc. Vol. 2000, 33, 307–312. [Google Scholar] [CrossRef]
- O’Keefe, J.H.; Gheewala, N.M.; O’Keefe, J.O. Dietary Strategies for Improving Post-Prandial Glucose, Lipids, Inflammation, and Cardiovascular Health. J. Am. Coll. Cardiol. 2008, 51, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Elleri, D.; Allen, J.M.; Harris, J.; Kumareswaran, K.; Nodale, M.; Leelarathna, L.; Acerini, C.L.; Haidar, A.; Wilinska, M.E.; Jackson, N.; et al. Absorption Patterns of Meals Containing Complex Carbohydrates in Type 1 Diabetes. Diabetologia 2013, 56, 1108–1117. [Google Scholar] [CrossRef]
- Cunningham, K.M.; Read, N.W. The Effect of Incorporating Fat into Different Components of a Meal on Gastric Emptying and Postprandial Blood Glucose and Insulin Responses. Br. J. Nutr. 1989, 61, 285–290. [Google Scholar] [CrossRef]
- Lubasinski, N.; Thabit, H.; Nutter, P.W.; Harper, S. What Is the Tech Missing? Nutrition Reporting in Type 1 Diabetes. Nutrients 2024, 16, 1690. [Google Scholar] [CrossRef]
- Campos-Náñez, E.; Layne, J.E.; Zisser, H.C. In Silico Modeling of Minimal Effective Insulin Doses Using the UVA/PADOVA Type 1 Diabetes Simulator. J. Diabetes Sci. Technol. 2018, 12, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Bergman, R.N.; Ider, Y.Z.; Bowden, C.R.; Cobelli, C. Quantitative estimation of insulin sensitivity. Am. J. Physiol.-Endocrinol. Metab. 1979, 236, E667. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, E.D.; Deutsch, T. A physiological model of glucose-insulin interaction in type 1 diabetes mellitus. J. Biomed. Eng. 1992, 14, 235–242. [Google Scholar] [CrossRef]
- Andreassena, S.; Hejlesena, O.K.; Hovorkab, R.; Cavan, D.A. The Diabetes Advisory System-an IT approach to the management of insulin dependent diabetes. In Medical Informatics Europe’96; IOS Press: Amsterdam, The Netherlands, 1996. [Google Scholar]
- Höfig, B.; Kistner, A.; Seibold, A.; Böhm, B. Extended physiological models for the simulation of the glucose metabolism. Math. Model. Syst. 1996, 2, 41–54. [Google Scholar] [CrossRef]
- Dalla Man, C.; Raimondo, D.M.; Rizza, R.A.; Cobelli, C. GIM, Simulation Software of Meal Glucose—Insulin Model. J. Diabetes Sci Technol 2007, 1, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Islam, S.; Leech, J.; Lin, C.C.Y.; Chrostowski, L. Peak Blood Glucose Prediction Algorithm Following a Meal Intake. In 2007 Canadian Conference on Electrical and Computer Engineering; IEEE: Vancouver, BC, Canada, 2007; pp. 579–582. [Google Scholar] [CrossRef]
- Bock, A.; François, G.; Gillet, D. A therapy parameter-based model for predicting blood glucose concentrations in patients with type 1 diabetes. Comput. Methods Programs Biomed. 2015, 118, 107–123. [Google Scholar] [CrossRef]
- Magdelaine, N.; Chaillous, L.; Guilhem, I.; Poirier, J.Y.; Krempf, M.; Moog, C.; Carpentier, E.L. A Long-Term Model of the Glucose–Insulin Dynamics of Type 1 Diabetes. IEEE Trans. Biomed. Eng. 2015, 62, 1546–1552. [Google Scholar] [CrossRef]
- Hovorka, R.; Canonico, V.; Chassin, L.J.; Haueter, U.; Massi-Benedetti, M.; Federici, M.O.; Pieber, T.R.; Schaller, H.C.; Schaupp, L.; Vering, T.; et al. Nonlinear model predictive control of glucose concentration in subjects with type 1 diabetes. Physiol. Meas. 2004, 25, 905–920. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Vehi, J.; Oliver, N.; Georgiou, P.; Herrero, P. Enhancing Blood Glucose Prediction with Meal Absorption and Physical Exercise Information. arXiv 2018, arXiv:1901.07467. [Google Scholar]
- Rozendaal, Y.J.; Maas, A.H.; van Pul, C.; Cottaar, E.J.; Haak, H.R.; Hilbers, P.A.; van Reil, N.A. Model-based analysis of postprandial glycemic response dynamics for different types of food. Clin. Nutr. Exp. 2018, 19, 32–45. [Google Scholar] [CrossRef]
- Gyuk, P.; Vassányi, I.; Kósa, I. Blood Glucose Level Prediction for Diabetics Based on Nutrition and Insulin Administration Logs Using Personalized Mathematical Models. J. Healthc. Eng. 2019, 2019, 8605206. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Zhang, G.; Yu, L.; Xu, B.; Jin, H. Improved Generalized Predictive Control Algorithm for Blood Glucose Control of Type 1 Diabetes. Artif. Organs 2019, 43, 386–398. [Google Scholar] [CrossRef]
- Tresp, V.; Briegel, T. A Solution for Missing Data in Recurrent Neural Networks with an Application to Blood Glucose Prediction. Available online: https://proceedings.neurips.cc/paper_files/paper/1997/file/c73dfe6c630edb4c1692db67c510f65c-Paper.pdf (accessed on 8 June 2023).
- Sandham, W.; Nikoletou, D.; Hamilton, D.J.; Paterson, K.; Japp, A.; Macgregor, C. Blood glucose prediction for diabetes therapy using a recurrent artificial neural network. In Proceedings of the 9th European Signal Processing Conference (EUSIPCO 1998), Rhodes, Greece, 8–11 September 1998. [Google Scholar]
- Ståhl, F.; Johansson, R.; Renard, E. Post-prandial plasma glucose prediction in type I diabetes based on Impulse Response Models. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; pp. 1324–1327. [Google Scholar] [CrossRef]
- Cescon, M.; Renard, E. Adaptive subspace-based prediction of T1DM glycemia. In Proceedings of the IEEE Conference on Decision and Control and European Control Conference, Orlando, FL, USA, 12–15 December 2011; pp. 5164–5169. [Google Scholar] [CrossRef]
- Pappada, S.M.; Cameron, B.D.; Rosman, P.M.; Bourey, R.E.; Papadimos, T.J.; Olorunto, W.; Borst, M.J. Neural Network-Based Real-Time Prediction of Glucose in Patients with Insulin-Dependent Diabetes. Diabetes Technol. Ther. 2011, 13, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Pappada, S.M.; Cameron, B.D.; Rosman, P.M. Development of a Neural Network for Prediction of Glucose Concentration in Type 1 Diabetes Patients. J. Diabetes Sci. Technol. 2008, 2, 792–801. [Google Scholar] [CrossRef] [PubMed]
- Robertson, G.; Lehmann, E.D.; Sandham, W.; Hamilton, D. Blood Glucose Prediction Using Artificial Neural Networks Trained with the AIDA Diabetes Simulator: A Proof-of-Concept Pilot Study. J. Electr. Comput. Eng. 2011, 2011, 681786. [Google Scholar] [CrossRef]
- Daskalaki, E.; Prountzou, A.; Diem, P.; Mougiakakou, S.G. Real-Time Adaptive Models for the Personalized Prediction of Glycemic Profile in Type 1 Diabetes Patients. Diabetes Technol. Ther. 2012, 14, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Pappada, S.M.; Cameron, B.D. Neural Network Modeling Approaches for Patient Specific Glycemic Forecasting. In Patient-Specific Modeling in Tomorrow’s Medicine; Gefen, A., Ed.; Springer: Berlin/Heidelberg, Germany, 2011; Volume 9, pp. 505–529. [Google Scholar]
- Van Heusden, K.; Dassau, E.; Zisser, H.C.; Seborg, D.E.; Doyle, F.J. Control-Relevant Models for Glucose Control Using a Priori Patient Characteristics. IEEE Trans. Biomed. Eng. 2012, 59, 1839–1849. [Google Scholar] [CrossRef] [PubMed]
- Steil, G.M. Algorithms for a Closed-Loop Artificial Pancreas: The Case for Proportional-Integral-Derivative Control. J. Diabetes Sci. Technol. 2013, 7, 1621–1631. [Google Scholar] [CrossRef]
- Toffanin, C.; Messori, M.; Di Palma, F.; De Nicolao, G.; Cobelli, C.; Magni, L. Artificial Pancreas: Model Predictive Control Design from Clinical Experience. J. Diabetes Sci. Technol. 2013, 7, 1470–1483. [Google Scholar] [CrossRef] [PubMed]
- Cameron, F.; Niemeyer, G.; Wilson, D.M.; Bequette, B.W.; Benassi, K.S.; Clinton, P.; Buckingham, B.A. Inpatient Trial of an Artificial Pancreas Based on Multiple Model Probabilistic Predictive Control with Repeated Large Unannounced Meals. Diabetes Technol. Ther. 2014, 16, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Del Favero, S.; Bruttomesso, D.; Di Palma, F.; Lanzola, G.; Visentin, R.; Filippi, A.; Scotton, R.; Toffanin, C.; Messori, M.; Scarpellini, S.; et al. First Use of Model Predictive Control in Outpatient Wearable Artificial Pancreas. Diabetes Care 2014, 37, 1212–1215. [Google Scholar] [CrossRef] [PubMed]
- Efendic, H.; Kirchsteiger, H.; Freckmann, G.; del Re, L. Short-term prediction of blood glucose concentration using interval probabilistic models. In Proceedings of the 22nd Mediterranean Conference on Control and Automation, Palermo, Italy, 16–19 June 2014; pp. 1494–1499. [Google Scholar] [CrossRef]
- Kirchsteiger, H.; Johansson, R.; Renard, E.; Re, L.D. Continuous-time interval model identification of blood glucose dynamics for type 1 diabetes. Int. J. Control 2014, 87, 1454–1466. [Google Scholar] [CrossRef]
- Oviedo, S.; Contreras, I.; Vehí, J.; Visentin, R.; Vettoretti, M. Mid-term blood glucose prediction: A hybrid approach using grammatical evolution and physiological models. Training 2017, 19, 15–62. [Google Scholar]
- Plis, K.; Bunescu, R.; Marling, C.; Shubrook, J.; Schwartz, F. A Machine Learning Approach to Predicting Blood Glucose Levels for Diabetes Management. Available online: https://citeseerx.ist.psu.edu/document?repid=rep1&type=pdf&doi=7e0ad22e8314dbb89695021e505bf3d043ad255a (accessed on 8 June 2023).
- Ståhl, F.; Johansson, R.; Renard, E. Ensemble Glucose Prediction in Insulin-Dependent Diabetes. In Data-Driven Modeling for Diabetes; Marmarelis, V., Mitsis, G., Eds.; Springer: Berlin/Heidelberg, Germany, 2014; pp. 37–71. [Google Scholar] [CrossRef]
- Wang, Y.; Wu, X.; Mo, X. A Novel Adaptive-Weighted-Average Framework for Blood Glucose Prediction. Diabetes Technol. Ther. 2013, 15, 792–801. [Google Scholar] [CrossRef] [PubMed]
- Georga, E.I.; Protopappas, V.C.; Polyzos, D.; Fotiadis, D.I. Evaluation of short-term predictors of glucose concentration in type 1 diabetes combining feature ranking with regression models. Med. Biol. Eng. Comput. 2015, 53, 1305–1318. [Google Scholar] [CrossRef]
- Bazaev, N.A.; Pozhar, K.V. Blood Glucose Prediction for “Artificial Pancreas” System. In Gluconeogenesis; Zhang, W., Ed.; InTech: 2017. Available online: https://www.intechopen.com/chapters/53941 (accessed on 8 June 2023). [CrossRef]
- Hidalgo, J.I.; Colmenar, J.M.; Kronberger, G.; Winkler, S.M.; Garnica, O.; Lanchares, J. Data Based Prediction of Blood Glucose Concentrations Using Evolutionary Methods. J. Med. Syst. 2017, 41, 142. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, M.V.; Mosimann, S.; Bally, L.; Stettler, C.; Mougiakakou, S. Deep prediction model: The case of online adaptive prediction of subcutaneous glucose. In Proceedings of the 2016 13th Symposium on Neural Networks and Applications (NEUREL), Belgrade, Serbia, 22–24 November 2016. [Google Scholar] [CrossRef]
- Zecchin, C.; Facchinetti, A.; Sparacino, G.; Cobelli, C. How Much Is Short-Term Glucose Prediction in Type 1 Diabetes Improved by Adding Insulin Delivery and Meal Content Information to CGM Data? A Proof-of-Concept Study. J. Diabetes Sci. Technol. 2016, 10, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Reiter, M.; Reiterer, F.; Del Re, L. A probabilistic framework for blood glucose control in diabetes. In Proceedings of the 2017 American Control Conference (ACC), Seattle, WA, USA, 24–26 May 2017; pp. 1450–1455. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, J.; Zeng, F.; Wang, N.; Chen, X.; Zhang, B.; Zhao, D.; Yang, W.; Cobelli, C. “Learning” Can Improve the Blood Glucose Control Performance for Type 1 Diabetes Mellitus. Diabetes Technol. Ther. 2017, 19, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Acedo, L.; Botella, M.; Cortés, J.C.; Hidalgo, J.I.; Maqueda, E.; Villanueva, R.J. Swarm hybrid optimization for a piecewise model fitting applied to a glucose model. J. Syst. Inf. Technol. 2018, 20, 404–416. [Google Scholar] [CrossRef]
- Buckingham, B.A.; Christiansen, M.P.; Forlenza, G.P.; Wadwa, R.P.; Peyser, T.A.; Lee, J.B.; O’Connor, J.; Dassau, E.; Huyett, L.M.; Layne, J.E.; et al. Performance of the Omnipod Personalized Model Predictive Control Algorithm with Meal Bolus Challenges in Adults with Type 1 Diabetes. Diabetes Technol. Ther. 2018, 20, 585–595. [Google Scholar] [CrossRef] [PubMed]
- Vahedi, M.R.; MacBride, K.B.; Wunsik, W.; Kim, Y. Predicting Glucose Levels in Patients with Type1 Diabetes Based on Physiological and Activity Data. In Proceedings of the 8th ACM MobiHoc 2018 Workshop on Pervasive Wireless Healthcare Workshop; ACM: Los Angeles, CA, USA, 2018; pp. 1–5. [Google Scholar] [CrossRef]
- Akbari, M.; Chunara, R. Using Contextual Information to Improve Blood Glucose Prediction. Available online: http://proceedings.mlr.press/v106/akbari19a/akbari19a.pdf (accessed on 8 June 2023).
- Borle, N.C.; Ryan, E.A.; Greiner, R. The Challenge of Predicting Meal-to-meal Blood Glucose Concentrations for Patients with Type I Diabetes. arXiv 2019, arXiv:1903.12347. [Google Scholar]
- Griva, L.O.; Martinez, R.; Basualdo, M.S. Combining short and long-term models for predicting blood glucose concentrations on diabetic patients. In Proceedings of the 2019 XVIII Workshop on Information Processing and Control (RPIC), Salvador, Brazil, 18–20 September 2019; IEEE: Bahía Blanca, Argentina, 2019; pp. 123–128. [Google Scholar] [CrossRef]
- Georga, E.I.; Príncipe, J.C.; Fotiadis, D.I. Short-term prediction of glucose in type 1 diabetes using kernel adaptive filters. Med. Biol. Eng. Comput. 2019, 57, 27–46. [Google Scholar] [CrossRef] [PubMed]
- Litinskaia, E.L.; Rudenko, P.A.; Pozhar, K.V.; Bazaev, N.A. Validation of Short-Term Blood Glucose Prediction Algorithms. Int. J. Pharma Med. Biol. Sci. 2019, 8, 34–39. [Google Scholar] [CrossRef]
- Padmapritha, T. Prediction of Blood Glucose Level by using an LSTM based Recurrent Neural networks. In Proceedings of the 2019 IEEE International Conference on Clean Energy and Energy Efficient Electronics Circuit for Sustainable Development (INCCES), Krishnankoil, India, 18–20 December 2019; pp. 1–4. [Google Scholar] [CrossRef]
- Saiti, K.; Macaš, M.; Štechová, K.; Pit’hová, P.; Lhotská, L. A Combined-Predictor Approach to Glycaemia Prediction for Type 1 Diabetes. In World Congress on Medical Physics and Biomedical Engineering 2018; IFMBE Proceedings; Lhotska, L., Sukupova, L., Lacković, I., Ibbott, G., Eds.; Springer: Singapore, 2019; Volume 68/3. [Google Scholar] [CrossRef]
- Alqudah, A.; Younes, A.; Alqudah, A. Towards Modeling Human Body Responsiveness to Glucose Intake and Insulin Injection based on Artificial Neural Networks. J. Comput. Inf. Technol. 2020, 6. [Google Scholar] [CrossRef]
- Amar, Y.; Shilo, S.; Oron, T.; Amar, E.; Phillip, M.; Segal, E. Clinically Accurate Prediction of Glucose Levels in Patients with Type 1 Diabetes. Diabetes Technol. Ther. 2020, 22, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Balasooriya, K.; Nanayakkara, N.D. Predicting Short-Term Changing Blood Glucose Level of Diabetes Patients using Noninvasive Data. In Proceedings of the 2020 IEEE Region 10 Conference (Tencon), Osaka, Japan, 16–19 November 2020; pp. 31–36. [Google Scholar] [CrossRef]
- Camerlingo, N.; Vettoretti, M.; Del Favero, S.; Facchinetti, A.; Sparacino, G. Mathematical Models of Meal Amount and Timing Variability with Implementation in the Type-1 Diabetes Patient Decision Simulator. J. Diabetes Sci. Technol. 2021, 15, 346–359. [Google Scholar] [CrossRef] [PubMed]
- Contador, S.; Colmenar, J.M.; Garnica, O.; Hidalgo, J.I. Short and Medium Term Blood Glucose Prediction Using Multi-objective Grammatical Evolution. In Applications of Evolutionary Computation; Castillo, P.A., Jiménez Laredo, J.L., Fernández De Vega, F., Eds.; Springer International Publishing: Cham, Switzerland, 2020; Volume 12104, pp. 494–509. [Google Scholar]
- Hidalgo, J.I.; Botella, M.; Velasco, J.M.; Garnica, O.; Cervigón, C.; Martínez, R.; Aramendi, A.; Maqueda, E.; Lanchares, J. Glucose forecasting combining Markov chain based enrichment of data, random grammatical evolution and Bagging. Appl. Soft Comput. 2020, 88, 105923. [Google Scholar] [CrossRef]
- Kriventsov, S.; Lindsey, A.; Hayeri, A. The Diabits App for Smartphone-Assisted Predictive Monitoring of Glycemia in Patients with Diabetes: Retrospective Observational Study. JMIR Diabetes 2020, 5, e18660. [Google Scholar] [CrossRef]
- Pavan, J.; Prendin, F.; Meneghetti, L.; Cappon, G.; Sparaconi, G.; Facchinetti, A.; Del Favero, S. Personalized Machine Learning Algorithm Based on Shallow Network and Error Imputation Module for an Improved Blood Glucose Prediction. Available online: https://ceur-ws.org/Vol-2675/paper16.pdf (accessed on 8 June 2023).
- Song, L.; Liu, C.; Yang, W.; Zhang, J.; Kong, X.; Zhang, B.; Chen, X.; Wang, N.; Shen, D.; Li, Z.; et al. Glucose outcomes of a learning-type artificial pancreas with an unannounced meal in type 1 diabetes. Comput. Methods Programs Biomed. 2020, 191, 105416. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Rashid, M.; Sevil, M.; Hobbs, N.; Brandt, R.; Askari, M.R.; Shahidehpour, A.; Cinar, A. Prediction of Blood Glucose Levels for People with Type 1 Diabetes Using Latent-Variable-Based Model. Available online: https://ceur-ws.org/Vol-2675/paper20.pdf (accessed on 8 June 2023).
- Zhu, T.; Yao, X.; Li, K.; Herrero, P.; Georgiou, P. Blood Glucose Prediction for Type 1 Diabetes Using Generative Adversarial Networks. In CEUR Workshop Proceedings; 2020. Available online: https://ceur-ws.org/Vol-2675/paper15.pdf (accessed on 8 June 2023).
- Alvarado, J.; Velasco, J.M.; Chavez, F.; Hidalgo, J.I.; De Vega, F.F. Blood Glucose Prediction Using a Two Phase TSK Fuzzy Rule Based System. In Proceedings of the 2021 IEEE Congress on Evolutionary Computation (CEC), Kraków, Poland, 28 June–1 July 2021; pp. 712–719. [Google Scholar] [CrossRef]
- Beauchamp, J.; Bunescu, R.; Marling, C.; Li, Z.; Liu, C. LSTMs and Deep Residual Networks for Carbohydrate and Bolus Recommendations in Type 1 Diabetes Management. Sensors 2021, 21, 3303. [Google Scholar] [CrossRef] [PubMed]
- Bhargav, S.; Kaushik, S.; Dutt, V.; Choudhury, A. Development of a weighted ensemble approach for prediction of blood glucose levels. Manch. J. Artif. Intell. Appl. Sci. 2022, 3, 6. [Google Scholar]
- Cui, R.; Hettiarachchi, C.; Nolan, C.J.; Daskalaki, E.; Suominen, H. Personalised Short-Term Glucose Prediction via Recurrent Self-Attention Network. In Proceedings of the 2021 IEEE 34th International Symposium on Computer-Based Medical Systems (CBMS), Aveiro, Portugal, 7–9 June 2021; pp. 154–159. [Google Scholar] [CrossRef]
- De Bois, M.; El-Yacoubi, M.A.; Ammi, M. Integration of clinical criteria into the training of deep models: Application to glucose prediction for diabetic people. Smart Health 2021, 21, 100193. [Google Scholar] [CrossRef]
- De Falco, I.; Cioppa, A.D.; Koutny, T.; Scafuri, U.; Tarantino, E.; Ubi, M. Grammatical Evolution-Based Approach for Extracting Interpretable Glucose-Dynamics Models. In Proceedings of the 2021 IEEE Symposium on Computers and Communications (ISCC), Athens, Greece, 5–8 September 2021; pp. 1–6. [Google Scholar] [CrossRef]
- Rabby, M.F.; Tu, Y.; Hossen, M.I.; Maida, A.S.; Hei, X. Stacked LSTM based deep recurrent neural network with kalman smoothing for blood glucose prediction. BMC Med. Inf. Decis. Mak. 2021, 21, 101. [Google Scholar] [CrossRef] [PubMed]
- Shahid, S.; Hussain, S.; Khan, W.A. Predicting continuous blood glucose level using deep learning. In Proceedings of the 14th IEEE/ACM International Conference on Utility and Cloud Computing Companion, Leicester UK, 6–9 December 2021; pp. 1–5. [Google Scholar] [CrossRef]
- Wang, Y. A Comparison of Machine Learning Algorithms in Blood Glucose Prediction for People with Type 1 Diabetes. In Proceedings of the 2nd International Symposium on Artificial Intelligence for Medicine Sciences, Beijing China, 29–31 October 2021; pp. 351–360. [Google Scholar] [CrossRef]
- Zaidi, S.M.A.; Chandola, V.; Ibrahim, M.; Romanski, B.; Mastrandrea, L.D.; Singh, T. Multi-step ahead predictive model for blood glucose concentrations of type-1 diabetic patients. Sci. Rep. 2021, 11, 24332. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Flores, K.B.; Tran, H.T. Deep learning and regression approaches to forecasting blood glucose levels for type 1 diabetes. Biomed. Signal Process. Control 2021, 69, 102923. [Google Scholar] [CrossRef]
- Aashima Bhargav, S.; Kaushik, S.; Dutt, V. A Combination of Decision Trees with Machine Learning Ensembles for Blood Glucose Level Predictions. In Proceedings of International Conference on Data Science and Applications; Saraswat, M., Roy, S., Chowdhury, C., Gandomi, A.H., Eds.; Springer: Singapore, 2022; Volume 287, pp. 533–548. [Google Scholar]
- Daniels, J.; Herrero, P.; Georgiou, P. A Multitask Learning Approach to Personalized Blood Glucose Prediction. IEEE J. Biomed. Health Inform. 2022, 26, 436–445. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Yu, X.; Ma, N.; Wu, R.; Li, H. An autonomous channel deep learning framework for blood glucose prediction. Appl. Soft Comput. 2022, 120, 108636. [Google Scholar] [CrossRef]
- Mordvanyuk, N.; Torrent-Fontbona, F.; Pez, B.L. Prediction of Glucose Level Conditions from Sequential Data. Available online: http://eia.udg.es/~nmordvanyuk/papers/Prediction-of-Glucose-Level-Conditions-from%20Sequential-DataCCIA2017.pdf (accessed on 8 June 2023).
- Jaloli, M.; Cescon, M. Long-Term Prediction of Blood Glucose Levels in Type 1 Diabetes Using a CNN-LSTM-Based Deep Neural Network. J. Diabetes Sci. Technol. 2023, 17, 1590–1601. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Rashid, M.; Askari, M.R.; Cinar, A. Adaptive personalized prior-knowledge-informed model predictive control for type 1 diabetes. Control Eng. Pract. 2023, 131, 105386. [Google Scholar] [CrossRef] [PubMed]
- Cui, R.; Nolan, C.J.; Daskalaki, E.; Suominen, H. Jointly Predicting Postprandial Hypoglycemia and Hyperglycemia Using Continuous Glucose Monitoring Data in Type 1 Diabetes. In Proceedings of the 2023 45th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Sydney, Australia, 24–27 July 2023; pp. 1–7. [Google Scholar] [CrossRef]
- Langarica, S.; Rodriguez-Fernandez, M.; Doyle Iii, F.J.; Núñez, F. A Probabilistic Approach to Blood Glucose Prediction in Type 1 Diabetes Under Meal Uncertainties. IEEE J. Biomed. Health Inform. 2023, 27, 5054–5065. [Google Scholar] [CrossRef]
- Langarica, S.; de la Vega, D.; Cariman, N.; Miranda, M.; Andrade, D.C.; Núñez, F.; Rodriguez-Fernandez, M. Deep Learning-Based Glucose Prediction Models: A Guide for Practitioners and a Curated Dataset for Improved Diabetes Management. IEEE Open J. Eng. Med. Biol. 2024, 5, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Aiello, E.M.; Jaloli, M.; Cescon, M. Model Predictive Control (MPC) of an artificial pancreas with data-driven learning of multi-step-ahead blood glucose predictors. Control Eng. Pract. 2024, 144, 105810. [Google Scholar] [CrossRef]
- Hutten, H. A multicompartment model for open-loop control of glucose in insulin-dependent diabetics. Comput. Methods Programs Biomed. 1990, 32, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Parker, R.S.; Doyle, F.J.; Peppas, N.A. A model-based algorithm for blood glucose control in Type I diabetic patients. IEEE Trans. Biomed. Eng. 1999, 46, 148–157. [Google Scholar] [CrossRef] [PubMed]
- Mougiakakou, S.G.; Prountzou, K.; Nikita, K.S. A Real Time Simulation Model of Glucose-Insulin Metabolism for Type 1 Diabetes Patients. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2006; pp. 298–301. [Google Scholar] [CrossRef]
- Roy, A.; Parker, R.S. Dynamic Modeling of Free Fatty Acid, Glucose, and Insulin: An Extended ‘Minimal Model’. Diabetes Technol. Ther. 2006, 8, 617–626. [Google Scholar] [CrossRef] [PubMed]
- Schlotthauer, G.; Gamero, L.G.; Torres, M.E.; Nicolini, G.A. Modeling, identification and nonlinear model predictive control of type I diabetic patient. Med. Eng. Phys. 2006, 28, 240–250. [Google Scholar] [CrossRef]
- Kildegaard, J.; Randløv, J.; Poulsen, J.U.; Hejlesen, O. A Study of Trained Clinicians’ Blood Glucose Predictions Based on Diaries of People with Type 1 Diabetes. Methods Inf. Med. 2007, 46, 553–557. [Google Scholar]
- Markakis, M.G.; Mitsis, G.D.; Papavassilopoulos, G.P.; Marmarelis, V.Z. Model Predictive Control of blood glucose in Type 1 diabetes: The Principal Dynamic Modes approach. In Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008; pp. 5466–5469. [Google Scholar] [CrossRef]
- Stahl, F.; Johansson, R. Short-term diabetes blood glucose prediction based on blood glucose measurements. In Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008; pp. 291–294. [Google Scholar] [CrossRef]
- Estrada, G.C.; Kirchsteiger, H.; Del Re, L.; Renard, E. Innovative approach for online prediction of blood glucose profile in type 1 diabetes patients. In Proceedings of the 2010 American Control Conference 2015–2020, Baltimore, MD, USA, 30 June–2 July 2010. [Google Scholar] [CrossRef]
- Georga, E.I.; Protopappas, V.C.; Fotiadis, D.I. Predictive Metabolic Modeling for Type 1 Diabetes Using Free-Living Data on Mobile Devices. In Wireless Mobile Communication and Healthcare; Lin, J.C., Nikita, K.S., Eds.; Springer: Berlin, Heidelberg, 2011; Volume 55, pp. 187–193. [Google Scholar]
- Percival, M.W.; Wang, Y.; Grosman, B.; Dassau, E.; Zisser, H.; Jovanovič, L.; Doyle, F.J. Development of a multi-parametric model predictive control algorithm for insulin delivery in type 1 diabetes mellitus using clinical parameters. J. Process Control 2011, 21, 391–404. [Google Scholar] [CrossRef]
- De Pereda, D.; Romero-Vivo, S.; Ricarte, B.; Bondia, J. On the prediction of glucose concentration under intra-patient variability in type 1 diabetes: A monotone systems approach. Comput. Methods Programs Biomed. 2012, 108, 993–1001. [Google Scholar] [CrossRef] [PubMed]
- Gondhalekar, R.; Dassau, E.; Zisser, H.C.; Doyle, F.J. Periodic-Zone Model Predictive Control for Diurnal Closed-Loop Operation of an Artificial Pancreas. J. Diabetes Sci. Technol. 2013, 7, 1446–1460. [Google Scholar] [CrossRef] [PubMed]
- Cescon, M.; Johansson, R.; Renard, E. Subspace-based linear multi-step predictors in type 1 diabetes mellitus. Biomed. Signal Process. Control 2015, 22, 99–110. [Google Scholar] [CrossRef]
- Mirshekarian, S.; Bunescu, R.; Marling, C.; Schwartz, F. Using LSTMs to learn physiological models of blood glucose behavior. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Seogwipo, Republic of Korea, 11–15 July 2017; pp. 2887–2891. [Google Scholar] [CrossRef]
- Bertachi, A.; Biagi, L.; Contreras, I.; Luo, N.; Vehı, J. Prediction of blood glucose levels and nocturnal hypoglycemia using physiological models and artificial neural networks. KDH@ IJCAI 2018, 85–90. [Google Scholar]
- Contreras, I.; Bertachi, A.; Biagi, L.; Oviedo, S.; Vehı, J. Using Grammatical Evolution to Generate Short-Term Blood Glucose Prediction models. KDH@ IJCAI 2018, 91–96. [Google Scholar]
- Hajizadeh, I.; Rashid, M.; Turksoy, K.; Samadi, S.; Feng, J.; Sevil, M.; Hobbs, N.; Lazaro, C.; Maloney, Z.; Littlejohn, E.; et al. Incorporating Unannounced Meals and Exercise in Adaptive Learning of Personalized Models for Multivariable Artificial Pancreas Systems. J. Diabetes Sci. Technol. 2018, 12, 953–966. [Google Scholar] [CrossRef] [PubMed]
- De Falco, I.; Della Cioppa, A.; Giugliano, A.; Marcelli, A.; Koutny, T.; Krcma, M.; Scafuri, U.; Tarantino, E. A genetic programming-based regression for extrapolating a blood glucose-dynamics model from interstitial glucose measurements and their first derivatives. Appl. Soft Comput. 2019, 77, 316–328. [Google Scholar] [CrossRef]
- Hajizadeh, I.; Rashid, M.; Cinar, A. Plasma-insulin-cognizant adaptive model predictive control for artificial pancreas systems. J. Process Control 2019, 77, 97–113. [Google Scholar] [CrossRef]
- Knopp, J.L.; Signal, M.; Harris, D.L.; Marics, G.; Weston, P.; Harding, J.; Tóth-Heyn, P.; Hómlok, J.; Benyó, B.; Chase, J.G. Modelling intestinal glucose absorption in premature infants using continuous glucose monitoring data. Comput. Methods Programs Biomed. 2019, 171, 41–51. [Google Scholar] [CrossRef]
- Dias, C.C.; Kamath, S.; Vidyasagar, S. Design of dual hormone blood glucose therapy and comparison with single hormone using MPC algorithm. IET Syst. Biol. 2020, 14, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Aydas, B.; Ghazaleh, H.; Rajasekharan, S. CarbMetSim: A discrete-event simulator for carbohydrate metabolism in humans. PLoS ONE 2020, 15, e0209725. [Google Scholar] [CrossRef]
- Montaser, E.; Diez, J.E.; Rossetti, P.; Rashid, M.; Cinar, A.; Bondia, J. Seasonal Local Models for Glucose Prediction in Type 1 Diabetes. IEEE J. Biomed. Health Inform. 2020, 24, 2064–2072. [Google Scholar] [CrossRef] [PubMed]
- Adelberger, D.; Reiterer, F.; Schrangl, P.; Ringemann, C.H.; Huschto, T.; del Re, L. Prediction of postprandial glucose excursions in type 1 diabetes using control-oriented process models. IFAC-Pap. 2021, 54, 466–471. [Google Scholar] [CrossRef]
- Cervigon, C.; Velasco, J.M.; Burgos-Simon, C.; Villanueva, R.J.; Hidalgo, J.I. Probabilistic Fitting of Glucose Models with Real-Coded Genetic Algorithms. In Proceedings of the 2021 IEEE Congress on Evolutionary Computation (CEC), Kraków, Poland, 28 June–1 July 2021; pp. 736–743. [Google Scholar] [CrossRef]
- Tavarez, J.R.; Sanchez, I.Y.; Maldonado, V.A.; Montes, M.; Ortiz, R.A. Stochastic Identification and Kalman Filter for Blood Glucose Estimation. In Recent Trends in Sustainable Engineering; Flores Rodríguez, K.L., Ramos Alvarado, R., Barati, M., Segovia Tagle, V., Velázquez González, R.S., Eds.; Springer International Publishing: Cham, Switzerland, 2022; Volume 297, pp. 117–130. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).