Abstract
This review summarizes the relationship between diet, the gut microbiome, and migraine. Key findings reveal that certain dietary factors, such as caffeine and alcohol, can trigger migraine, while nutrients like magnesium and riboflavin may help alleviate migraine symptoms. The gut microbiome, through its influence on neuroinflammation (e.g., vagus nerve and cytokines), gut–brain signaling (e.g., gamma-aminobutyric acid), and metabolic function (e.g., short-chain fatty acids), plays a crucial role in migraine susceptibility. Migraine can also alter eating behaviors, leading to poor nutritional choices and further exacerbating the condition. Individual variability in diet and microbiome composition highlights the need for personalized dietary and prebiotic interventions. Epidemiological and clinical data support the effectiveness of tailored nutritional approaches, such as elimination diets and the inclusion of beneficial nutrients, in managing migraine. More work is needed to confirm the role of prebiotics, probiotics, and potentially fecal microbiome translation in the management of migraine. Future research should focus on large-scale studies to elucidate the underlying mechanisms of bidirectional interaction between diet and migraine and develop evidence-based clinical guidelines. Integrating dietary management, gut health optimization, and lifestyle modifications can potentially offer a holistic approach to reducing migraine frequency and severity, ultimately improving patient outcomes and quality of life.
1. Introduction
Migraine is a prevalent and debilitating neurological disorder characterized by recurrent episodes of severe headache [1], often accompanied by nausea, vomiting, and higher sensitivity to light and sound [2]. Affecting both children and adults, migraine represents a significant public health challenge due to its impact on quality of life and productivity [3,4]. Emerging evidence suggests that migraine is not solely a neurological condition but also involves complex metabolic processes [5,6]. This review focuses on the contribution of metabolic, microbiome–gut–brain (MGB) axis, and dietary aspects in the multifaceted nature of migraine, emphasizing environmental and lifestyle factors.
The significance of exploring the interplay between the brain, eating habits, and the gut microbiome in migraine pathogenesis cannot be overstated [7]. Recent research indicates that dietary habits and gut health may play crucial roles in the onset and severity of migraine attacks [8]. The MGB axis is an active field of investigation that offers new insights into how dietary components and the gut microbiome can influence migraine [9,10].
The purpose of this review is to present current findings on the relationship between diet, the gut microbiome, and migraine, providing an overview of how these factors interact to influence migraine development and severity. By integrating evidence, this review aims to highlight potential targets and lifestyle modifications that could mitigate migraine frequency and severity, ultimately contributing to more effective management strategies for this complex disorder. The viewpoint here also considers the bidirectional relationship between migraine and dietary choices and their consequences.
2. Trigeminovascular System and Migraine Pathogenesis
There is consensus that the activation followed by sensitization of meningeal nociceptors within trigeminal ophthalmic and upper cervical nerves generates headaches in both migraine with and without aura [11]. Consistent with this anatomical arrangement, meningeal nociception refers to pain in the skin of the forehead and occipital regions, a pattern typical for visceral pain (e.g., heartache). Animal studies demonstrate that prolonged activation of trigeminocervical nociceptors prompts the release of vasoactive mediators such as calcitonin gene-related peptide (CGRP), pituitary adenylate cyclase-activating polypeptide (PACAP), substance P, and neurokinin-A from their nerve endings [12,13]. These peptides initiate a sterile neurogenic inflammation characterized by meningeal vasodilatation, plasma protein extravasation, the activation of meningeal inflammatory dendritic cells and macrophages, and the degranulation of dural mast cells [12,14]. A connection in the brain stem between the second-order central nociceptive neurons located in the trigeminal nucleus caudalis (TNC) and the parasympathetic superior salivary nucleus causes the release of acetylcholine, nitric oxide, vasointestinal peptide (VIP), and PACAP from parasympathetic fibers around dural blood vessels [11,15]. This trigeminoparasympathetic reflex contributes to meningeal vasodilation induced by the peptides released from nociceptors [16,17]. Of note, vascular dilation and permeability increase do not directly cause headaches, but the sensitization of Aδ fibers triggered by CGRP seems to play a primary role [12,18]. Inflammatory mediators such as prostaglandins, histamine, and tryptase released from mast cells located near dural sensory fibers can also contribute to nociceptor activation and sensitization [19]. Sensitized perivascular nociceptors responding to mechanical stimuli start firing with vascular pulsations or head motion, giving a headache a throbbing nature and leading to sensations like “my heart is beating inside my head” or “my brain is being pushed out of my eyeballs” [20]. Clinical success with largely blood–brain barrier (BBB)-impermeable triptans, which inhibit CGRP release, and the anti-CGRP antibodies suggest that CGRP has a more prominent role in meningeal neurogenic inflammation in humans [21,22]. This also supports the idea that migraine headache is initiated in the meninges because central nociceptive pathways in CNS are located behind the BBB.
The cell bodies of C-type unmyelinated and lightly myelinated A∂-type fibers reside in the trigeminal ganglion (TG) [23]. CGRP is released from activated C-type nociceptors and binds to its receptors on neighboring Aδ neurons that do not express CGRP [24,25]. This interaction may lead to signal amplification within the TG. Additionally, CGRP stimulates the satellite glia cells in the ganglion, triggering the release of nitric oxide, which in turn creates a positive feedback amplification loop by increasing CGRP release from C-type fibers [25,26]. Similar to the meninges, the trigeminal ganglion is accessible by triptans and anti-CGRP antibodies due to the lack of a BBB. The central processes of trigeminal and cervical nociceptive neurons enter the CNS and synapse on the second-order sensory neurons in the TNC extending from the upper cervical medulla spinalis segments to the medulla oblongata. Central terminals of C-fibers also release CGRP, as do their meningeal nerve endings. CGRP stimulates its receptors on TNC neurons as well as on the presynaptic terminals of A∂-fibers, promoting glutamate release [27]. Consequently, activity in the first-order TG neurons is transmitted to the second-order neurons, priming them to be excited with lower-intensity synaptic inputs than normal [20,28]. The sensitization of the TNC results in allodynia, the painful perception of non-nociceptive stimuli like touching the head [28]. TNC activity is further transmitted to the ventral posteromedial thalamic nucleus, somatosensory cortex, insula, limbic structures, and hypothalamus, leading to pain perception, as well as emotional (like mood changes), hypothalamic (like malaise), and autonomic symptoms (like pale skin) [28]. Over time, thalamic synapses may also sensitize, resulting in whole-body (extracephalic) allodynia such as the noxious perception of the touch of bracelets on the wrist. The convergence of nociceptive and visual stimuli in some thalamic neurons likely underlies photophobia, another typical migraine symptom [28,29].
The mechanisms that episodically activate the trigeminocervicovascular system in migraine within an otherwise healthy brain are not entirely clear. The occurrence of migraine prodrome often preceding the headache suggests that the loss of homeostasis begins intrinsically in the brain parenchyma in most cases. Consistent with this perspective, prodromal symptoms are anatomically associated with cortical and subcortical structures [30]. Experimental animal studies support the notion that cortical spreading depolarization (CSD), the putative cause of migraine aura, can induce headache by initiating a parenchymal inflammatory signaling cascade that progresses to the meninges by way of astrocytes [31,32]. Notably, mutations identified in familial migraine increase susceptibility to CSD in animal models [33]. Furthermore, clinical investigations using a highly sensitive PET ligand have revealed an inflammatory process encompassing both the cerebral parenchyma and adjacent meninges in patients experiencing frequent migraine with aura attacks [34,35].
However, there are distinct examples that seem to involve mainly meningeal activation without a primary parenchymal component, thus triggering migraine headaches. For instance, the Umbellularia California plant, known as the “headache tree”, can induce a migraine episode in susceptible individuals through inhalation of the volatile compound umbellullone emitted by its leaves. This is believed to occur via direct activation of meningeal nociceptive afferents by opening TRPA1 channels on nociceptors, subsequently leading to CGRP release [36]. Some volatile irritants known to trigger migraine headaches may also act through a similar mechanism. Additionally, GTN or CGRP infusion has been suggested to trigger migraine attacks in migraineurs, likely through peripheral mechanisms [22,37]. Allergy-triggered migraine attacks may involve mast cell degranulation and subsequent dural inflammation [38]. The throbbing headache accompanying fever during systemic infections may also result from the activation and sensitization of meningeal nociceptors by circulating pro-inflammatory cytokines. The absence of the BBB at the level of dural nociceptors, as well as at the trigeminal and dorsal root ganglia, provides a common platform for several circulating pro-inflammatory mediators and molecules to trigger migraine headaches. Similar genetic predispositions (e.g., TRES potassium channel mutations [39]) and hormonal factors (e.g., estrogen [38]) can prime both parenchymal and meningeal mechanisms for migraine attacks, with parenchymal disturbances likely associated with auras and prodromal symptoms. Additionally, synaptic metabolic stress caused by transcriptional changes induced by hunger or lack of sleep has been proposed to initiate parenchymal inflammatory signaling resulting in headache [40,41]. Although relatively underexplored, migraine triggers may also modulate nociception and dural neurogenic inflammation, predisposing people to headache generation, as proposed for estrogen and stress [38].
3. Microbiome Contribution to Migraine
3.1. Overview of the Microbiome–Gut–Brain Axis
As more attention has been paid to the human microbiome since the initiation of the Human Microbiome Project in 2007 [42,43], the microbiome–gut–brain (MGB) axis, a bidirectional communication network between the gut and the brain [44], has been a central focus in understanding the mechanisms of neurocognitive and psychological effects of gut–brain communication. As a complex communication network, the MGB axis includes the gastrointestinal (GI)-related immune system, enteric neuroendocrine system, enteric nervous system (ENS), central nervous system (CNS), and the gut microbiome [45]. The gut microbiome is defined as the collection of all genomes of microbes (e.g., bacteria, fungi, and viruses) and their functional products (e.g., metabolites) in the GI tract [46]. The human gut hosts tens of trillions of microbial cells, indicating more than 500 bacterial species on average [47]. The community of the gut microbiome plays an important role in human health and disease [48]. For example, the bidirectional MGB axis was significantly linked with GI-associated disorders, such as inflammatory bowel disease (IBD) [49] and irritable bowel syndromes (IBS) [50,51]. Recently, the MGB axis was identified to play a critical role in a wide range of neuropsychiatric disorders, including emotional disorders (e.g., acute and chronic stress and depression), developmental disorders (e.g., autism spectrum disorder), and neurodegenerative disorders (e.g., Parkinson’s disease and Alzheimer’s disease) [52,53,54].
Rapidly evolving sequencing methods and analytical tools promote our understanding of the gut microbiome and its function in human health and diseases [55]. A dysbiotic gut microbiome (i.e., loss of keystone taxa, loss of diversity, shifts in metabolic capacity, or blooms of pathogens [56,57]) has been characterized in various diseases and conditions [48,58,59]. Specifically, a dysbiotic gut microbiome could influence the brain and neurological health through multiple pathways: regulating the production of pro-inflammatory cytokines and immune activity; adjusting the production of neurotransmitters (e.g., gamma-aminobutyric acid [GABA] and serotonin); modulating the formation of bacterial metabolites (e.g., short-chain fatty acids [SCFAs]) and tryptophan/kynurenine pathway metabolites (e.g., indoles); and disturbing the neuronal pathways (e.g., afferent vagus nerve and spinal sensory neurons) [60,61]. The systems biological view of the MGB axis provides an innovative and dynamic model to study the pathophysiology of brain and neuropsychiatric disorders, in which pathophysiological processes were previously hypothesized to be limited to the brain. The MGB axis has opened newer opportunities to target the gut microbiome as a treatment for both GI disorders (e.g., IBD and IBS) and neuropsychiatric disorders (e.g., depression, Alzheimer’s disease, Parkinson’s disease, and autism spectrum disorder).
Although the connection between the GI tract and the CNS has been hypothesized as a mechanism for a wide range of human diseases and conditions, recent work proposes that the axis serves as a highway—enabling bidirectional signals that can influence peripheral and central pain [62,63,64]. In the CNS, the gut microbiome-derived or activated mediators regulate neuroinflammation via the activation of microglia, astrocytes, and immune cells to modulate the central sensitization, subsequently being linked with chronic pain [62,65,66] and pain attacks (e.g., migraine) [62,67]. Additionally, the gut microbiome-derived signaling molecules, such as metabolites, neurotransmitters, and neuromodulators, serve as critical regulators for peripheral sensitization, directly or indirectly regulating the excitability of primary nociceptive neurons and pain experiences [63,68]. Considering that the gut microbiome may regulate pain in the peripheral and central nervous system, targeting the gut microbiome by pharmacological and non-pharmacological (e.g., diet) interventions may represent a new therapeutic strategy for the management of chronic pain and other chronic diseases or conditions. Regarding migraine, studies suggest that certain foods may be migraine triggers and promote these painful events. However, food triggers do not create a clear linear reaction and can be challenging for patients and clinicians to identify. In addition to potential food triggers, patients with migraine have disproportional GI symptoms, including nausea, vomiting, and bowel disturbances prior to and throughout the migraine episode as compared to healthy controls without migraine [69]. A recent study [7] suggests that patients with gut dysbiosis are more likely to report migraine symptoms. This evidence suggests an area of further investigation to determine the best treatment approaches to migraine.
3.2. Role of the Gut Microbiome in Neurological Function and Dysfunction and Potential Mechanisms
Both animal and human studies indicate that the gut microbiome plays a role in maintaining homeostasis and regulating almost every major body system, including the CNS [52,70]. According to the MGB axis as mentioned above, biological pathways through which the gut influences neurological function (i.e., the brain), or vice versa, include altered gut microbiome composition and its functional metabolome, lack of balance of “beneficial” and “detrimental” bacteria in the lumen, and activated neuro-immune signaling pathways [71]. Specifically, associations between the gut microbiome and neurological function have been primarily conducted in animal models [72,73,74,75,76]. Germ-free mice (i.e., those lacking the gut microbiome) showed exaggerated responses in inflammatory pain [74], anxiety [76,77,78], and cognitive dysfunction as compared with specific pathogen-free mice [76]. However, mice infected with pathogenic Citrobacter rodentium received daily probiotics (Lactobacillus rhamnosus + Lactobacillus helveticus) and then showed a reversed memory dysfunction [76]. Although limited, a similar role of the gut microbiome in neurological function has been reported among human studies, including the effects of the gut microbiome on pain, anxiety, depression, and cognitive dysfunction [52,70]. Additionally, the metabolites produced or activated by the gut microbiome, such as SCFAs [79,80] and tryptophan (for kynurenine pathway metabolism) [81], may influence the relationship between the gut microbiome and neurological function [82]. Alterations in SCFAs might underpin disturbances in the CNS from neurodevelopmental disorders (e.g., mood disorders) [83]. Similarly, tryptophan metabolism via the kynurenine pathway regulates neuronal function [84] and can modulate various neuropsychiatric disorders, including depression and cognitive dysfunction [85,86,87,88].
Considering the potentially similar biological pathways underlying neurological disorders, multiple intensive reviews [52,70,89] have reviewed and summarized the role of the gut microbiome in brain function in the context of neurological disorders. Particularly, the MGB axis has been implicated in understanding the pathophysiology of a group of neurological disorders, including autism spectrum disorder, Alzheimer’s disease, multiple sclerosis, and Parkinson’s disease [52,70,89,90]. Common themes have emerged from these studies, including (1) alterations in the composition of the microbiome [91,92,93,94]; (2) involvement of the MGB axis pathways, such as α-synuclein signaling to the brain via the vagus nerve [95,96,97], pro-inflammatory cytokines and neuroinflammation [98,99,100], and functional metabolomic molecules (e.g., SCFAs) [101,102,103]; and (3) prebiotic (e.g., galacto-oligosaccharide) and probiotic (e.g., Lactobacillus acidophilus, Lactobacillus casei, Bifidobacterium bifidum, and Lactobacillus fermentum) interventions with promising results to improve GI and brain-related symptoms and behaviors [104,105,106,107]. Considering the limitations of these studies, such as primarily cross-sectional designs, participant selection bias, inconsistent sampling, and sequencing protocols [70], the findings of the MGB axis in neurological disorders need to be cautiously interpreted. However, these studies provide promising examples to further uncover the role of the MGB axis in neurological disorders, including migraine.
3.3. Microbiome–Gut–Brain Axis in Migraine Pathogenesis
Migraine is a complex neurological disorder that involves both the sensory afferent nerves in the face, head, and neck, intra- and extracranial vessels, and central brain structures. Migraine was once thought to be a vascular phenomenon and drugs were created to target this pathway; however, this theory is less likely to be the cause of migraine. Subsequent studies demonstrated minimal vascular change during a migraine attack [108,109]. However, the drugs that target this pathway have neural effects in addition to their vasoconstrictive effects. Triptans most likely reduce migraine symptoms through these neural effects [110].
The neural theory suggests that migraine begins in the central brain areas and if treated early, worsening migraine symptoms could be prevented. Nitric oxide (NO) can trigger migraine symptoms. NO synthase inhibition has been studied as a potential treatment option and was not an overall useful strategy as there are significant cardiovascular adverse effects associated with inhibition of NO. However, experimental migraine attacks triggered with NO are a response to triptan treatment [111]. Furthermore, migraine attacks triggered by increased levels of NO suggest a potential cause due to interplay with CGRP. Increased levels of CGRP are thought to promote migraine attacks and have been associated with higher levels of NO. This aligns with the neural theory of migraine [111]. The pathway of NO in migraine supported that nitrate-, nitrite-, and nitric oxide-reducing oral microbes (e.g., Streptococcus and Pseudomonas) play significant roles in migraine development [112].
Recently, multiple observational studies have reported the promising role of the MGB axis in migraine as well as possible targets for treatment interventions. Qu and colleagues [113] recently showed that Lachnospiraceae UCG001 was associated with an increased risk of migraine, while Eubacterium and Bacteroides fragilis may be associated with a lower migraine risk. The functional pathways of these bacteria, including Methionine synthesis and hydrocinnamate, were associated with lower migraine risk [113]. Additionally, children with migraine showed a lower alpha diversity and dissimilar beta diversity compared to children without migraine [114]. Considering the limited literature using the observational research design primarily, future work is required to examine the role of the MGB axis in migraine among different populations.
3.4. Therapeutic Interventions Targeting the Gut Microbiome for Migraine Management
3.4.1. Prebiotics and Probiotics
Prebiotics are found in certain foods and are the fuel for the human microbiome, whereas probiotics can be consumed either in food or supplements that contain live microorganisms or helpful bacteria. Dysbiosis has been suggested to be associated with migraine headaches [114]. The increased association between dysbiosis and migraine is thought to be related to a disproportional number of bacteria found in migraine patients’ guts that produce NO. The elevation of NO is thought to increase levels of CGRP, suggesting a potential trigger for a migraine attack [111]. Various studies, including a systematic review [115,116,117], have evaluated the usefulness of probiotics (Bifidobacterium, Lactobacillus, Lactococcus, and Streptococcus) in the prevention of migraine attacks in migraine patients. Due to methodological differences, there is no consensus on whether supplementation is helpful to migraine patients. Probiotics may have a positive influence on migraine by decreasing both the frequency and severity of attacks; however, further studies are needed to better understand the usefulness of these therapies in migraine patients [117].
3.4.2. Lifestyle Interventions
Lifestyle modification is essential to migraine care and should be incorporated into the patient treatment plan. Evidence-based lifestyle modifications include SEEDS, which stands for Sleep, Exercise, Eating, Diary, and Stress Reduction [118]. Patients with migraine should aim to get seven hours of sleep per night. Patients who get poor sleep are at increased risk of migraine [119]. Consider asking patients to take 400–600 mg of magnesium prior to bed. Magnesium can prevent migraine and can help patients relax and initiate sleep. Magnesium is also thought to have a positive effect on the microbiome [7]. Patients with migraine should aim for 150 min of exercise per week or 30 min of exercise five times per week. There is no specific recommendation regarding what type of exercise patients should perform—the key is to encourage them to choose something fun and accessible, so exercise becomes a sustainable part of their life. While exercise can be helpful to prevent migraine, it may not be best for patients to exercise during an acute attack. To date, there is not a lot of evidence suggesting that one diet is more effective at preventing migraine compared to another. However, we do know that skipping meals is a migraine trigger [118]. The patient should aim to eat at least three meals a day and consider adding a morning or afternoon snack to decrease the risk of a migraine occurring between meals. Furthermore, caffeine consumption should be limited to 200 mg of caffeine per day or less [120].
Migraine is a complex neurological condition that in addition to causing pain through widespread sensory activation can also activate the limbic system [30]. For patients, this means that migraine pain will have an emotional component, which can make it difficult to keep track of attacks without a migraine diary. Encouraging patients to keep a diary not only helps to define the frequency and severity of attacks but also helps to determine the effectiveness of treatments and evaluate potential migraine triggers.
3.4.3. Fecal Microbiome Transplantation (FMT)
FMT has been used successfully in the treatment of patients with depression [7,121]. The procedure involves transplanting a healthy fecal microbiome into a person with an unhealthy microbiome. Many patients note the unpleasantness of the procedure as a limitation. Additionally, there is a risk of infection, which can be mitigated through appropriate screening. While several studies have demonstrated the effectiveness of FMT in several chronic conditions, the exact mechanism of action is not fully known. To date, there have been no FMT clinical trials in migraine patients.
4. Diet and Migraine
4.1. A Bidirectional Relationship between Diet and Migraine: Dietary Factors That Trigger or Subside Migraine
Individual dietary factors (e.g., foods, beverages, and habits) trigger the onset and increased severity of migraine via proposed vascular, neuropeptide, neuroinflammation, insulin, and oxidant–antioxidant pathways [122,123,124]. Common triggers include chocolate, nuts, citrus, cheese, and other dairy products [125,126,127]. Alcohol has also been identified as a common dietary factor associated with migraine, with 17.5% to 35.6% of individuals reporting the beverage as a potential trigger [125,126,127]. When compared to other types of alcoholic beverages, red wine is the most commonly reported trigger by individuals suffering from migraine [127]. Caffeinated beverages, such as coffee, energy drinks, teas, and sodas, are also potential triggers, yet findings are inconsistent. Some studies have demonstrated a positive association between caffeine consumption and migraine onset [128,129]. However, Mostofsky et al. [130] found that one to two servings of caffeine were not associated with migraine, whereas consuming three or more servings demonstrated significantly higher odds of developing a migraine within the same day. With this finding in mind, a daily intake of 200 mg per day of caffeine has been recommended, with the abrupt cessation of caffeine being inadvisable due to withdrawal also being associated with migraine onset [131]. While a healthy balance of caffeine is recommended to prevent migraine, it has also been proposed as a potential treatment due to its initiation of cerebral vasoconstriction. There is insufficient evidence to support universal guidelines for the use of dietary and medicinal caffeine in headache disorders. A sensible approach, based on available evidence, is to limit dietary caffeine intake to moderate amounts with consistent timing before noon and to use caffeine-containing combination analgesics infrequently for milder headaches [132]. One dietary intervention that improves migraine outcomes through the removal of these common migraine triggers from the daily diet is elimination diets [125]. Numerous randomized control trials (RCTs) have demonstrated the positive effects of elimination diets on reducing the frequency and severity of migraine, especially when the removed items are associated with Immunoglobulin G (IgG)-mediated immune responses [133,134,135].
While specific foods and beverages are linked to migraine onset, dietary habits also play a crucial role. For example, fasting due to dietary preferences or religious practices has been found to trigger migraine. During the Holy month of Ramadan, daily fasting caused a significant increase in migraine frequency and severity in practicing Muslims when compared to previous months [136,137,138]. Conversely, a study examining the onset of migraine in 34 individuals following their typical dietary habits over six weeks demonstrated that consuming meals or snacks late at night reduced the odds of experiencing a headache within the consecutive 24 h [139]. The dehydration and hypoglycemia often associated with fasting or extended timeframes between meals are some hypothesized underlying mechanisms for migraine onset due to increased vasopressin secretion, upregulation of the sympathetic nervous system, and alteration of the serotonergic system.
Nutraceuticals have been reported as effective and safe alternatives for individuals with migraine and include vitamins such as B and D; minerals; supplements, such as riboflavin, antioxidants, L-Carnitine, and Omega-3; and phytomedicines such as feverfew (Tanacetum parthenium), butterbur (Petasites hybridus), cannabis, St. John’s Wort (Hypericum perforatum), and ginkgo (Ginkgo biloba) [140]. The most commonly used nutraceuticals with evidence for migraine prevention include riboflavin (vitamin B2), coenzyme Q10 (CoQ10), magnesium, butterbur root extract, feverfew, ginkgolide B, and, recently, phycocyanins [141]. While vitamins have strong evidence, dietary therapies offer broader health benefits. With increasing cannabis legalization, providers should note its limited evidence in migraine treatment. Future research should explore traditional medicines and larger human trials for current and new nutraceutical treatments.
Isolated nutrients have also been found to influence migraine outcomes. For example, the increased consumption of B vitamins (e.g., vitamin B6, folate, thiamine, and riboflavin) and magnesium has been shown to reduce or prevent migraine [142]. A study examining the effect of dietary vitamin B6 and folate on migraine outcomes using the National Health and Nutrition Examination Survey found that a vitamin B6 intake of > 2.39 mg per day and a folate intake of > 502.01 mg per day demonstrated significantly lower odds of developing migraine [142]. Similarly, studies have demonstrated an inverse relationship between the increased consumption of dietary thiamine or riboflavin and decreased migraine onset [143,144]. Hypomagnesemia has also been observed in individuals who experience migraine. One cross-sectional study of 905 individuals experiencing migraine demonstrated that they consumed significantly less magnesium (mean = 290.2 mg/day; standard error [SE] = 5.7) when compared to 2721 healthy controls (mean = 327.6 mg/day; SE = 4.7) [145]. Additionally, individuals who attained the recommended dietary allowance of magnesium (310–420 mg/day) through dietary or supplementary methods were at significantly lower odds of migraine onset. While B vitamins play a crucial role in migraine pathogenesis due to their association with mitochondrial energy metabolism [127,143,144], magnesium blocks N-methyl-D-aspartate (NMDA) receptors, which prevents glutamate from binding to the NMDA receptor and causes hyperexcitability in the brain [145]. Dietary changes are one method to improve migraine by increasing the consumption of these essential nutrients. For example, the Mediterranean diet consists of eating primarily legumes, fish, whole grains, olive oil, vegetables, fruits, and nuts, which have high levels of B vitamins and magnesium. Previous studies confirm the effectiveness of this diet, demonstrating significant associations between consuming foods frequently found in the Mediterranean diet and decreased frequency, duration, and severity of migraine [146,147].
Therefore, the relationship between diet and migraine is complex and bidirectional, encompassing how dietary factors can trigger or alleviate migraine and how migraine can influence dietary habits [148]. Identifying and avoiding specific dietary triggers, while incorporating beneficial nutrients, can be a crucial part of migraine management. Migraine can significantly influence an individual’s eating habits. During migraine attacks, symptoms like nausea and vomiting may lead to reduced food intake and the avoidance of certain foods. Post-migraine fatigue can also alter eating patterns, often leading to irregular meal timings and poor nutritional choices. Chronic migraine can lead to long-term changes in dietary habits and nutritional status. Moreover, the stress and pain associated with chronic migraine can lead to emotional eating or appetite suppression, further complicating nutritional status. It is important to state that there is considerable individual variability in how diet affects migraine, influenced by genetic, environmental, and lifestyle factors. The gut microbiome, which plays a key role in digestion and overall health, also varies significantly among individuals and can influence both diet and migraine susceptibility. Understanding these individual differences is therefore essential for personalized dietary recommendations. Behavioral strategies, such as mindful eating and stress management techniques, can also help reduce migraine incidence. Tailoring dietary recommendations to the individual, considering their unique triggers, preferences, and lifestyle, is crucial for effective migraine management.
4.2. Dietary Interventions
Certain dietary factors are linked to migraine occurrence and aggravation. A low intake of zinc [149], iron (and low ferritin levels) [150], and potassium [151] is associated with higher migraine prevalence, according to population-based studies. These studies, however, relied on self-reported severe headaches or migraine. The ketogenic diet (KD) is a diet with strong evidence for migraine prevention [152]. The KD, a high-fat, high-protein, low-carbohydrate diet, induces ketosis, which provides alternative energy sources for the brain and reduces cerebral reactivity [153,154]. Studies, including case reports, series, and randomized controlled trials (RCTs), have shown that the KD can significantly reduce migraine frequency, severity, and the need for rescue medication, though it may cause gastrointestinal issues, muscle cramps, fatigue, and increased cholesterol [155]. Since 2021, additional trials have supported the KD’s benefits, showing up to 60% of patients with a ≥50% reduction in monthly headache frequency, even for those with chronic migraine [156]. However, results for low-glycemic-index diets (LGIDs) are mixed [157,158], with some studies finding them less effective than the KD and others finding them equally effective. The optimal diet protocol, including the best lipid/carbohydrate and protein ratios, remains unclear and perhaps continues to do so as the individual needs must be taken into consideration for adjustments and fine-tuning. Neri et al. [159] have systematically reviewed the available literature on migraine and ketosis and recommended the evaluation of ketosis in future interventions. Adverse effects of the KD are generally mild, but long-term adherence is challenging, requiring a multidisciplinary approach [160]. An alternative to the KD is exogenous ketone supplementation to increase ketone bodies in the blood and brain. While this approach is easier to follow than the KD, it has shown no significant clinical improvement over a placebo in recent trials, except for a subgroup of patients with specific metabolic and inflammatory markers [161,162].
Moderate-quality evidence suggests that besides the KD, Dietary Approaches to Stop Hypertension (DASHs) can also reduce the frequency, duration, and severity of migraine in adults [8]. The DASH diet, designed to combat hypertension, emphasizes fruits, vegetables, and whole grains while limiting sodium, sweets, and saturated fats. It has been shown to decrease migraine frequency and severity, reduce headache duration, and lower the Migraine Headache Index Score. Other researched diets include the Mediterranean and MIND diets. The Mediterranean diet, rich in vegetables, legumes, fruits, nuts, olive oil, and limited meat, yields similar benefits comparable to the DASH diet [124,146]. The MIND Diet, created to prevent Alzheimer’s, has shown minimal effects on migraine pain in women [163].
The benefits of omega-3 and omega-6 fatty acids and balancing these acids have been proposed for migraine prevention and treatment [164], where reducing omega-6 and increasing omega-3 intake have been suggested to help reduce migraine attacks [165]. Maintaining stable blood sugar levels seems to benefit individuals with migraine. A 2018 experiment showed that a low-glycemic-index diet decreased attack frequency within the first month of starting the low-glycemic-index diet [166]. Epigenetic diets have been proposed to influence cellular structures and molecules, like mitochondria and DNA, through specific dietary ingredients. This concept, introduced by Hardy and Tollefsboll [167], suggests that dietary components can affect the epigenetic system and potentially prevent diseases, but there are discussions around its applicability [168]. Folate plays a role in DNA methylation, and abnormal mitochondrial DNA methylation has been observed in migraine patients [169]. Future studies may focus on DNA methylation and histone modification, i.e., epigenetic mechanisms influenced by diet. In migraine prevention, folate (vitamin B9) and riboflavin (vitamin B2) are found to be promising compounds [170,171].
Tryptophan-rich foods (e.g., flaxseed, salami, lentils, turkey, nuts, and eggs) may reduce migraine attacks due to their role in serotonin and kynurenine production [172]. Migraine patients often have lower serotonin and tryptophan levels between attacks and higher levels during attacks. Abnormal kynurenine levels have been linked to chronic migraine, suggesting that tryptophan-rich diets might help in prevention and treatment. However, further research is needed as the effects of tryptophan intake have shown mixed results [10].
Various other types of diets have also been tested and interested readers are referred to excellent reviews available, for example, the review by Jibril et al. [173]. Plant-based foods have also attracted attention for their potential beneficial effects on migraine [174,175]. The LIFE diet (Low Inflammatory Foods Everyday), which is a nutrient-dense, dark green leafy vegetable-rich, and whole food plant-based diet, has improved chronic migraine in a case [176].
Researchers worldwide are striving to define “a healthy plate” [177], which is a challenging task considering global differences in resources and practical issues related to sustainability and affordability according to the EAT-Lancet Commission on healthy diets from sustainable food systems [178]. Accordingly, a healthy plate and its relation to migraine have been the subject of various studies and it seems to continue attracting the interest of patients, nutritionists, and headache specialists. For example, an interventional study with a Healthy Eating Plate (HEP) for migraine has been conducted [179], where it was demonstrated that following HEP advice, especially reducing carbs and red and processed meat, migraine frequency and associated disability subsided [179]. This study shows that education and promoting healthy eating habits can be beneficial in migraine.
It is crucial to consider lifestyle factors, age, sex, and individual needs when creating dietary plans or defining a healthy plate for migraine. So far, no certain “migraine diet” exists, and researchers tend to emphasize that dietary recommendation for migraine is a better term to highlight the need for individualization based on patients’ needs and responses to a planned diet. In this line, it seems rational to also take into account diet quality [180] and dietary adherence [181] together with providing evidence for the mechanism-based [182] effectiveness of selected diets, including the potential role of neuroendocrine signaling [183] and the possible contribution of microbiota [184] followed by delineating recommendations for clinical implications [105], for example, the use of pre- or probiotics. Parohan et al. [185] performed a meta-analysis of randomized controlled trials and concluded that probiotic supplementation did not significantly alter the frequency or severity of episodic migraine attacks. However, only three randomized controlled trials (179 patients) were included for analysis and the significant heterogeneity among the studies [185] calls for a cautious interpretation of data and the need for further studies.
Overall, dietary interventions or recommendations may aid in the immediate control, slow progression, or prevention of migraine. Applying a patient-centric model, considering patients’ preferences, comorbidities, and a broader lifestyle modification, including sleep hygiene, stress management, regular exercise, or smoking cessation, seems logical. Accordingly, the effect of migraine or its evolution over age and among the genders on dietary choices must be taken into consideration with dietary patterns, quality, and the amount and the dynamicity of migraine–diet cross-talk [8,69,186,187].
5. The Interplay between Diet, Gut Microbiome, and Migraine: Current Evidence
While the impact of dietary factors and the gut microbiome on migraine outcomes have been independently examined, limited studies have explored the interplay between these factors via the hypothesized MGB axis. One RCT examining the influence of symbiotic supplementation on gut microbial by-products and migraine outcomes in women demonstrated a reduction in the frequency of migraine and the use of painkillers in individuals who received the symbiotic treatment [188]. Gut microbial by-products, specifically C-reactive protein and zonulin, also decreased in the treatment group, suggesting a reduction in inflammation and intestinal permeability. However, the direct influence of symbiotic supplementation on the diversity and composition of the gut microbiome was not explored. A murine model investigated how the gut microbiome’s composition and nitroglycerin-induced migraine are influenced by sodium butyrate (SB) and sodium propionate (SP), two SCFAs that are found in the diet [189]. SB and SP administration was associated with a higher Firmicutes-to-Bacteroidetes ratio, demonstrating an increase in healthy bacteria commonly found in the gut microbiome of mice and humans. High levels of SB (30 mg/kg) and SP (100 mg/kg) treatments reduced pain following the injection of nitroglycerin, which was used to induce migraine-like symptoms. Another RCT that examined how the adoption of a gluten-free Mediterranean diet influenced the gut microbiome and migraine outcomes corroborated the influence of dietary factors on migraine outcomes in humans diagnosed with gastrointestinal disorders [190]. Individuals who maintained a gluten-free diet demonstrated a significant reduction in migraine frequency over the previous three months. While there were no significant differences in bacterial and fungal diversity (alpha and beta) within the gut microbiome when comparing the gluten-free participants to controls (receiving 8 g of gluten daily), the gluten-free participants demonstrated a significant reduction in the abundance of the fungus Dothideomycetes, whereas the controls experienced a decrease in the fungus Tremellomycetes. These preliminary results highlight the importance of future research examining the interplay between dietary factors, the gut microbiome, and migraine via the proposed MGB axis to develop a deeper understanding of the pathogenesis of migraine. The insights that derive from this future work can foster the development of novel migraine dietary treatments or potentially provide a biomarker from which targeted and individualized dietary interventions can be formulated [191]. Figure 1 depicts this proposed interplay.
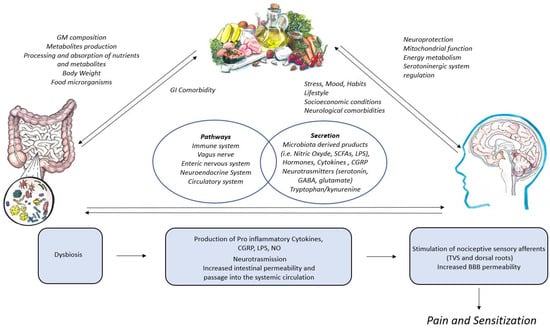
Figure 1.
The interplay between diet, gut microbiome, and brain in the pathogenesis of migraine.
Different dietary components can affect the composition of the gut microbiome. The diversity of the gut microbiome, its ecosystem, and the production of metabolites are influenced by the metabolism of nutrients entering the intestine from the diet. The microbiome–gut–brain axis is interconnected by the immune system, vagus nerve, enteric nervous system, neuroendocrine system, and metabolomic system. This communication occurs through sensory nervous pathways and also involves the release of numerous gut microbiome products into the systemic circulation. Similarly, the brain can communicate with the intestine directly by releasing neuroactive substances or changing the gut microbiome. The interaction between the gut microbiome, brain, and diet is not one-way but rather multidirectional. The intake of specific foods can be impacted by gastrointestinal disorders. Diet has a direct impact on brain functions through mechanisms that include neuroprotection, energy metabolism, and the regulation of mitochondrial and serotonergic functions. Finally, neurological or neuropsychiatric conditions, lifestyle, and socioeconomic factors can be important determinants of eating habits. Dysbiosis at the intestinal level could be favored by certain dietary habits, which alter the production of metabolites and establish a pro-inflammatory biochemical structure in the intestine. Chemical stimuli possess the ability to directly stimulate sensory fibers in the gut, which are then able to transmit messages to the brain. Furthermore, the proinflammatory environment can lead to an increase in intestinal permeability and passage into the systemic circulation of inflammatory molecules, which can stimulate the trigeminovascular system and spinal sensory afferents with the facilitation of the triggering of pain and also sensitization phenomena.
6. Conclusions
This review has elucidated the intricate and multidirectional relationship between diet, the gut microbiome, and migraine. Key findings highlight that dietary habits and gut health significantly influence migraine pathogenesis, while migraine can alter eating behaviors and nutritional status. The literature provides evidence that certain foods and beverages can act as migraine triggers, while nutrients like magnesium and riboflavin may help reduce migraine frequency and severity. The composition of the gut microbiome plays a crucial role in modulating migraine susceptibility through mechanisms, such as neuroinflammation, gut–brain signaling, and metabolic function. Migraine can also lead to altered eating patterns, including reduced food intake during attacks and poor nutritional choices, which can exacerbate the condition and affect overall health. There is significant individual variability in how diet affects migraine, influenced by genetic, environmental, and lifestyle factors, including the unique composition of each individual’s gut microbiome. Therefore, personalized dietary interventions, such as elimination diets and the inclusion of beneficial nutrients, show promise in managing migraine symptoms and improving quality of life. Advanced digital tools can aid in continuous monitoring, offer tailored educational content, support adherence to dietary plans, and enhance personalized care. Considering the complex interactions of lifestyle factors, as well as the influence of age and sex, is essential in creating effective dietary plans that meet patients’ needs at different life stages. The relationship between diet and migraine is dynamic and bidirectional, requiring careful monitoring and individualized dietary choices to achieve the best outcomes and minimize potential risks.
This review offers implications for future research and clinical practice. Future research should focus on large-scale, long-term studies to better understand the mechanisms underlying the diet–gut–migraine relationship and identify precise dietary recommendations. Advances in understanding individual variability in diet and gut microbiome composition will pave the way for personalized migraine management strategies, tailored to the unique needs of each patient. From this perspective, it should be considered that the microbiome is a true metabolic system made up not only of microorganisms but also of their metabolites. Metabolomic and metaproteomic studies can help understand which dietary styles in migraineurs can create a more beneficial microbiome ecosystem.
Developing evidence-based clinical guidelines for dietary and lifestyle interventions in migraine management will be crucial for healthcare providers, offering clear and actionable recommendations for patients. Integrating dietary management, gut health optimization, and lifestyle modifications into a holistic approach to migraine treatment can potentially reduce the frequency and severity of migraine, improving patient outcomes and quality of life. By continuing to explore the complex interactions between gut microbiome and dietary choices and their implications, we can move towards more effective and individualized approaches to managing migraine, ultimately reducing the burden of this debilitating condition.
Author Contributions
All authors have contributed substantially to this review. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
Thanks to Eleonora Cuzzola (cuzzola.eleonora@gmail.com) for creating the figure.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Robbins, M.S. Diagnosis and Management of Headache: A Review. JAMA 2021, 325, 1874–1885. [Google Scholar] [CrossRef]
- Hervias, T. An update on migraine: Current and new treatment options. JAAPA 2024, 37, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Estave, P.M.; Beeghly, S.; Anderson, R.; Margol, C.; Shakir, M.; George, G.; Berger, A.; O’Connell, N.; Burch, R.; Haas, N.; et al. Learning the full impact of migraine through patient voices: A qualitative study. Headache 2021, 61, 1004–1020. [Google Scholar] [CrossRef]
- Steiner, T.J.; Stovner, L.J.; Jensen, R.; Uluduz, D.; Katsarava, Z.; on Behalf of Lifting The Burden: The Global Campaign against Headache. Migraine remains second among the world’s causes of disability, and first among young women: Findings from GBD2019. J. Headache Pain 2020, 21, 137. [Google Scholar] [CrossRef] [PubMed]
- Khan, J.; Asoom, L.I.A.; Sunni, A.A.; Rafique, N.; Latif, R.; Saif, S.A.; Almandil, N.B.; Almohazey, D.; AbdulAzeez, S.; Borgio, J.F. Genetics, pathophysiology, diagnosis, treatment, management, and prevention of migraine. Biomed. Pharmacother. 2021, 139, 111557. [Google Scholar] [CrossRef] [PubMed]
- Del Moro, L.; Rota, E.; Pirovano, E.; Rainero, I. Migraine, Brain Glucose Metabolism and the “Neuroenergetic” Hypothesis: A Scoping Review. J. Pain 2022, 23, 1294–1317. [Google Scholar] [CrossRef] [PubMed]
- Kappéter, Á.; Sipos, D.; Varga, A.; Vigvári, S.; Halda-Kiss, B.; Péterfi, Z. Migraine as a Disease Associated with Dysbiosis and Possible Therapy with Fecal Microbiota Transplantation. Microorganisms 2023, 11, 2083. [Google Scholar] [CrossRef]
- Gazerani, P. Diet and migraine: What is proven? Curr. Opin. Neurol. 2023, 36, 615–621. [Google Scholar] [CrossRef]
- Crawford, J.; Liu, S.; Tao, F. Gut microbiota and migraine. Neurobiol. Pain 2022, 11, 100090. [Google Scholar] [CrossRef]
- Spekker, E.; Nagy-Grócz, G. All Roads Lead to the Gut: The Importance of the Microbiota and Diet in Migraine. Neurol. Int. 2023, 15, 1174–1190. [Google Scholar] [CrossRef]
- Ashina, M.; Hansen, J.M.; Do, T.P.; Melo-Carrillo, A.; Burstein, R.; Moskowitz, M.A. Migraine and the trigeminovascular system—40 years and counting. Lancet Neurol. 2019, 18, 795–804. [Google Scholar] [CrossRef]
- Levy, D.; Moskowitz, M.A. Meningeal Mechanisms and the Migraine Connection. Annu. Rev. Neurosci. 2023, 46, 39–58. [Google Scholar] [CrossRef]
- Moskowitz, M.A. Neurogenic inflammation in the pathophysiology and treatment of migraine. Neurology 1993, 43, S16–S20. [Google Scholar] [PubMed]
- Schain, A.J.; Melo-Carrillo, A.; Borsook, D.; Grutzendler, J.; Strassman, A.M.; Burstein, R. Activation of pial and dural macrophages and dendritic cells by cortical spreading depression. Ann. Neurol. 2018, 83, 508–521. [Google Scholar] [CrossRef] [PubMed]
- Waschek, J.A.; Baca, S.M.; Akerman, S. PACAP and migraine headache: Immunomodulation of neural circuits in autonomic ganglia and brain parenchyma. J. Headache Pain 2018, 19, 23. [Google Scholar] [CrossRef]
- Bolay, H.; Reuter, U.; Dunn, A.K.; Huang, Z.; Boas, D.A.; Moskowitz, M.A. Intrinsic brain activity triggers trigeminal meningeal afferents in a migraine model. Nat. Med. 2002, 8, 136–142. [Google Scholar] [CrossRef]
- Schain, A.J.; Melo-Carrillo, A.; Stratton, J.; Strassman, A.M.; Burstein, R. CSD-Induced Arterial Dilatation and Plasma Protein Extravasation Are Unaffected by Fremanezumab: Implications for CGRP’s Role in Migraine with Aura. J. Neurosci. 2019, 39, 6001–6011. [Google Scholar] [CrossRef]
- De Logu, F.; Nassini, R.; Hegron, A.; Landini, L.; Jensen, D.D.; Latorre, R.; Ding, J.; Marini, M.; Souza Monteiro de Araujo, D.; Ramírez-Garcia, P.; et al. Schwann cell endosome CGRP signals elicit periorbital mechanical allodynia in mice. Nat. Commun. 2022, 13, 646. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.C.; Strassman, A.M.; Burstein, R.; Levy, D. Sensitization and activation of intracranial meningeal nociceptors by mast cell mediators. J. Pharmacol. Exp. Ther. 2007, 322, 806–812. [Google Scholar] [CrossRef] [PubMed]
- Burstein, R. Deconstructing migraine headache into peripheral and central sensitization. Pain 2001, 89, 107–110. [Google Scholar] [CrossRef]
- Goadsby, P.J.; Edvinsson, L.; Ekman, R. Vasoactive peptide release in the extracerebral circulation of humans during migraine headache. Ann. Neurol. 1990, 28, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Hansen, J.M.; Hauge, A.W.; Olesen, J.; Ashina, M. Calcitonin gene-related peptide triggers migraine-like attacks in patients with migraine with aura. Cephalalgia 2010, 30, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Edvinsson, L.; Haanes, K.A. Identifying New Antimigraine Targets: Lessons from Molecular Biology. Trends Pharmacol. Sci. 2021, 42, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Eftekhari, S.; Salvatore, C.A.; Calamari, A.; Kane, S.A.; Tajti, J.; Edvinsson, L. Differential distribution of calcitonin gene-related peptide and its receptor components in the human trigeminal ganglion. Neuroscience 2010, 169, 683–696. [Google Scholar] [CrossRef] [PubMed]
- Messlinger, K.; Russo, A.F. Current understanding of trigeminal ganglion structure and function in headache. Cephalalgia 2019, 39, 1661–1674. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Vause, C.V.; Durham, P.L. Calcitonin gene-related peptide stimulation of nitric oxide synthesis and release from trigeminal ganglion glial cells. Brain Res. 2008, 1196, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Messlinger, K. The big CGRP flood—Sources, sinks and signalling sites in the trigeminovascular system. J. Headache Pain 2018, 19, 22. [Google Scholar] [CrossRef] [PubMed]
- Noseda, R.; Burstein, R. Migraine pathophysiology: Anatomy of the trigeminovascular pathway and associated neurological symptoms, CSD, sensitization and modulation of pain. Pain 2013, 154 (Suppl. S1), S44–S53. [Google Scholar] [CrossRef]
- Noseda, R.; Kainz, V.; Jakubowski, M.; Gooley, J.J.; Saper, C.B.; Digre, K.; Burstein, R. A neural mechanism for exacerbation of headache by light. Nat. Neurosci. 2010, 13, 239–245. [Google Scholar] [CrossRef]
- Karsan, N.; Goadsby, P.J. Biological insights from the premonitory symptoms of migraine. Nat. Rev. Neurol. 2018, 14, 699–710. [Google Scholar] [CrossRef]
- Erdener, Ş.E.; Kaya, Z.; Dalkara, T. Parenchymal neuroinflammatory signaling and dural neurogenic inflammation in migraine. J. Headache Pain 2021, 22, 138. [Google Scholar] [CrossRef] [PubMed]
- Karatas, H.; Erdener, S.E.; Gursoy-Ozdemir, Y.; Lule, S.; Eren-Koçak, E.; Sen, Z.D.; Dalkara, T. Spreading depression triggers headache by activating neuronal Panx1 channels. Science 2013, 339, 1092–1095. [Google Scholar] [CrossRef] [PubMed]
- Eren-Koçak, E.; Dalkara, T. Ion Channel Dysfunction and Neuroinflammation in Migraine and Depression. Front. Pharmacol. 2021, 12, 777607. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, D.S.; Mainero, C.; Ichijo, E.; Ward, N.; Granziera, C.; Zürcher, N.R.; Akeju, O.; Bonnier, G.; Price, J.; Hooker, J.M.; et al. Imaging of neuroinflammation in migraine with aura: A [(11)C]PBR28 PET/MRI study. Neurology 2019, 92, e2038–e2050. [Google Scholar] [CrossRef] [PubMed]
- Hadjikhani, N.; Albrecht, D.S.; Mainero, C.; Ichijo, E.; Ward, N.; Granziera, C.; Zürcher, N.R.; Akeju, O.; Bonnier, G.; Price, J.; et al. Extra-Axial Inflammatory Signal in Parameninges in Migraine with Visual Aura. Ann. Neurol. 2020, 87, 939–949. [Google Scholar] [CrossRef] [PubMed]
- Nassini, R.; Materazzi, S.; Vriens, J.; Prenen, J.; Benemei, S.; De Siena, G.; la Marca, G.; Andrè, E.; Preti, D.; Avonto, C.; et al. The ‘’’headache tree’ via umbellulone and TRPA1 activates the trigeminovascular system. Brain 2012, 135, 376–390. [Google Scholar] [CrossRef] [PubMed]
- Reuter, U.; Bolay, H.; Jansen-Olesen, I.; Chiarugi, A.; Sanchez del Rio, M.; Letourneau, R.; Theoharides, T.C.; Waeber, C.; Moskowitz, M.A. Delayed inflammation in rat meninges: Implications for migraine pathophysiology. Brain 2001, 124, 2490–2502. [Google Scholar] [CrossRef] [PubMed]
- Levy, D. Migraine pain, meningeal inflammation, and mast cells. Curr. Pain Headache Rep. 2009, 13, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Reyes, R.; Duprat, F.; Lesage, F.; Fink, M.; Salinas, M.; Farman, N.; Lazdunski, M. Cloning and expression of a novel pH-sensitive two pore domain K+ channel from human kidney. J. Biol. Chem. 1998, 273, 30863–30869. [Google Scholar] [CrossRef]
- Kilic, K.; Karatas, H.; Dönmez-Demir, B.; Eren-Kocak, E.; Gursoy-Ozdemir, Y.; Can, A.; Petit, J.M.; Magistretti, P.J.; Dalkara, T. Inadequate brain glycogen or sleep increases spreading depression susceptibility. Ann. Neurol. 2018, 83, 61–73. [Google Scholar] [CrossRef]
- Petit, J.M.; Eren-Koçak, E.; Karatas, H.; Magistretti, P.; Dalkara, T. Brain glycogen metabolism: A possible link between sleep disturbances, headache and depression. Sleep. Med. Rev. 2021, 59, 101449. [Google Scholar] [CrossRef] [PubMed]
- Turnbaugh, P.J.; Ley, R.E.; Hamady, M.; Fraser-Liggett, C.M.; Knight, R.; Gordon, J.I. The human microbiome project. Nature 2007, 449, 804–810. [Google Scholar] [CrossRef] [PubMed]
- The Integrative HMP (iHMP) Research Network Consortium. The Integrative Human Microbiome Project. Nature 2019, 569, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Rhee, S.H.; Pothoulakis, C.; Mayer, E.A. Principles and clinical implications of the brain-gut-enteric microbiota axis. Nat. Rev. Gastroenterol. Hepatol. 2009, 6, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Mayer, E.A.; Nance, K.; Chen, S. The Gut-Brain Axis. Annu. Rev. Med. 2022, 73, 439–453. [Google Scholar] [CrossRef] [PubMed]
- Cryan, J.F.; Dinan, T.G. Mind-altering microorganisms: The impact of the gut microbiota on brain and behaviour. Nat. Rev. Neurosci. 2012, 13, 701–712. [Google Scholar] [CrossRef] [PubMed]
- Savage, D.C. Microbial ecology of the gastrointestinal tract. Annu. Rev. Microbiol. 1977, 31, 107–133. [Google Scholar] [CrossRef] [PubMed]
- Lynch, S.V.; Pedersen, O. The Human Intestinal Microbiome in Health and Disease. N Engl. J. Med. 2016, 375, 2369–2379. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, C.N. The Brain-Gut Axis and Stress in Inflammatory Bowel Disease. Gastroenterol. Clin. North Am. 2017, 46, 839–846. [Google Scholar] [CrossRef]
- Collins, S.M.; Surette, M.; Bercik, P. The interplay between the intestinal microbiota and the brain. Nat. Rev. Microbiol. 2012, 10, 735–742. [Google Scholar] [CrossRef]
- Mayer, E.A. Gut feelings: The emerging biology of gut-brain communication. Nat. Rev. Neurosci. 2011, 12, 453–466. [Google Scholar] [CrossRef] [PubMed]
- Ullah, H.; Arbab, S.; Tian, Y.; Liu, C.Q.; Chen, Y.; Qijie, L.; Khan, M.I.U.; Hassan, I.U.; Li, K. The gut microbiota-brain axis in neurological disorder. Front. Neurosci. 2023, 17, 1225875. [Google Scholar] [CrossRef] [PubMed]
- Suganya, K.; Koo, B.S. Gut-Brain Axis: Role of Gut Microbiota on Neurological Disorders and How Probiotics/Prebiotics Beneficially Modulate Microbial and Immune Pathways to Improve Brain Functions. Int. J. Mol. Sci. 2020, 21, 7551. [Google Scholar] [CrossRef] [PubMed]
- Naveed, M.; Zhou, Q.G.; Xu, C.; Taleb, A.; Meng, F.; Ahmed, B.; Zhang, Y.; Fukunaga, K.; Han, F. Gut-brain axis: A matter of concern in neuropsychiatric disorders…! Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 104, 110051. [Google Scholar] [CrossRef] [PubMed]
- Ursell, L.K.; Metcalf, J.L.; Parfrey, L.W.; Knight, R. Defining the human microbiome. Nutr. Rev. 2012, 70 (Suppl. 1), S38–S44. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.; Kolodziejczyk, A.A.; Thaiss, C.A.; Elinav, E. Dysbiosis and the immune system. Nat. Rev. Immunol. 2017, 17, 219–232. [Google Scholar] [CrossRef] [PubMed]
- Vangay, P.; Ward, T.; Gerber, J.S.; Knights, D. Antibiotics, pediatric dysbiosis, and disease. Cell Host Microbe 2015, 17, 553–564. [Google Scholar] [CrossRef] [PubMed]
- de Vos, W.M.; Tilg, H.; Van Hul, M.; Cani, P.D. Gut microbiome and health: Mechanistic insights. Gut 2022, 71, 1020–1032. [Google Scholar] [CrossRef]
- Cani, P.D. Human gut microbiome: Hopes, threats and promises. Gut 2018, 67, 1716–1725. [Google Scholar] [CrossRef] [PubMed]
- Montiel-Castro, A.J.; González-Cervantes, R.M.; Bravo-Ruiseco, G.; Pacheco-López, G. The microbiota-gut-brain axis: Neurobehavioral correlates, health and sociality. Front. Integr. Neurosci. 2013, 7, 70. [Google Scholar] [CrossRef]
- Strasser, B.; Becker, K.; Fuchs, D.; Gostner, J.M. Kynurenine pathway metabolism and immune activation: Peripheral measurements in psychiatric and co-morbid conditions. Neuropharmacology 2017, 112, 286–296. [Google Scholar] [CrossRef] [PubMed]
- Ustianowska, K.; Ustianowski, Ł.; Machaj, F.; Gorący, A.; Rosik, J.; Szostak, B.; Szostak, J.; Pawlik, A. The Role of the Human Microbiome in the Pathogenesis of Pain. Int. J. Mol. Sci. 2022, 23, 13267. [Google Scholar] [CrossRef] [PubMed]
- Guo, R.; Chen, L.H.; Xing, C.; Liu, T. Pain regulation by gut microbiota: Molecular mechanisms and therapeutic potential. Br. J. Anaesth. 2019, 123, 637–654. [Google Scholar] [CrossRef] [PubMed]
- Morreale, C.; Bresesti, I.; Bosi, A.; Baj, A.; Giaroni, C.; Agosti, M.; Salvatore, S. Microbiota and Pain: Save Your Gut Feeling. Cells 2022, 11, 971. [Google Scholar] [CrossRef] [PubMed]
- Shoskes, D.A.; Wang, H.; Polackwich, A.S.; Tucky, B.; Altemus, J.; Eng, C. Analysis of Gut Microbiome Reveals Significant Differences between Men with Chronic Prostatitis/Chronic Pelvic Pain Syndrome and Controls. J. Urol. 2016, 196, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Du, H.X.; Yue, S.Y.; Niu, D.; Liu, C.; Zhang, L.G.; Chen, J.; Chen, Y.; Guan, Y.; Hua, X.L.; Li, C.; et al. Gut Microflora Modulates Th17/Treg Cell Differentiation in Experimental Autoimmune Prostatitis via the Short-Chain Fatty Acid Propionate. Front. Immunol. 2022, 13, 915218. [Google Scholar] [CrossRef] [PubMed]
- Arzani, M.; Jahromi, S.R.; Ghorbani, Z.; Vahabizad, F.; Martelletti, P.; Ghaemi, A.; Sacco, S.; Togha, M. Gut-brain Axis and migraine headache: A comprehensive review. J. Headache Pain 2020, 21, 15. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.; Wang, Y.; Zhang, P.; Yuan, Y.; Zhang, Y.; Chen, G. Gut microbiota regulates neuropathic pain: Potential mechanisms and therapeutic strategy. J. Headache Pain 2020, 21, 103. [Google Scholar] [CrossRef]
- Gazerani, P. Migraine and Diet. Nutrients 2020, 12, 1658. [Google Scholar] [CrossRef]
- Cryan, J.F.; O’Riordan, K.J.; Sandhu, K.; Peterson, V.; Dinan, T.G. The gut microbiome in neurological disorders. Lancet Neurol. 2020, 19, 179–194. [Google Scholar] [CrossRef]
- Bajic, J.E.; Johnston, I.N.; Howarth, G.S.; Hutchinson, M.R. From the Bottom-Up: Chemotherapy and Gut-Brain Axis Dysregulation. Front. Behav. Neurosci. 2018, 12, 104. [Google Scholar] [CrossRef]
- Stringer, A.M.; Al-Dasooqi, N.; Bowen, J.M.; Tan, T.H.; Radzuan, M.; Logan, R.M.; Mayo, B.; Keefe, D.M.; Gibson, R.J. Biomarkers of chemotherapy-induced diarrhoea: A clinical study of intestinal microbiome alterations, inflammation and circulating matrix metalloproteinases. Support. Care Cancer 2013, 21, 1843–1852. [Google Scholar] [CrossRef]
- Galloway-Peña, J.R.; Smith, D.P.; Sahasrabhojane, P.; Ajami, N.J.; Wadsworth, W.D.; Daver, N.G.; Chemaly, R.F.; Marsh, L.; Ghantoji, S.S.; Pemmaraju, N.; et al. The role of the gastrointestinal microbiome in infectious complications during induction chemotherapy for acute myeloid leukemia. Cancer 2016, 122, 2186–2196. [Google Scholar] [CrossRef]
- Amaral, F.A.; Sachs, D.; Costa, V.V.; Fagundes, C.T.; Cisalpino, D.; Cunha, T.M.; Ferreira, S.H.; Cunha, F.Q.; Silva, T.A.; Nicoli, J.R.; et al. Commensal microbiota is fundamental for the development of inflammatory pain. Proc. Natl. Acad. Sci. USA 2008, 105, 2193–2197. [Google Scholar] [CrossRef]
- Foster, J.A.; McVey Neufeld, K.A. Gut-brain axis: How the microbiome influences anxiety and depression. Trends Neurosci. 2013, 36, 305–312. [Google Scholar] [CrossRef]
- Gareau, M.G.; Wine, E.; Rodrigues, D.M.; Cho, J.H.; Whary, M.T.; Philpott, D.J.; Macqueen, G.; Sherman, P.M. Bacterial infection causes stress-induced memory dysfunction in mice. Gut 2011, 60, 307–317. [Google Scholar] [CrossRef]
- Sudo, N.; Chida, Y.; Aiba, Y.; Sonoda, J.; Oyama, N.; Yu, X.N.; Kubo, C.; Koga, Y. Postnatal microbial colonization programs the hypothalamic-pituitary-adrenal system for stress response in mice. J. Physiol. 2004, 558, 263–275. [Google Scholar] [CrossRef]
- Neufeld, K.M.; Kang, N.; Bienenstock, J.; Foster, J.A. Reduced anxiety-like behavior and central neurochemical change in germ-free mice. Neurogastroenterol. Motil. 2011, 23, 255-e119. [Google Scholar] [CrossRef]
- van de Wouw, M.; Boehme, M.; Lyte, J.M.; Wiley, N.; Strain, C.; O’Sullivan, O.; Clarke, G.; Stanton, C.; Dinan, T.G.; Cryan, J.F. Short-chain fatty acids: Microbial metabolites that alleviate stress-induced brain-gut axis alterations. J. Physiol. 2018, 596, 4923–4944. [Google Scholar] [CrossRef]
- Russo, R.; Cristiano, C.; Avagliano, C.; De Caro, C.; La Rana, G.; Raso, G.M.; Canani, R.B.; Meli, R.; Calignano, A. Gut-brain Axis: Role of Lipids in the Regulation of Inflammation, Pain and CNS Diseases. Curr. Med. Chem. 2018, 25, 3930–3952. [Google Scholar] [CrossRef]
- Kennedy, P.J.; Cryan, J.F.; Dinan, T.G.; Clarke, G. Kynurenine pathway metabolism and the microbiota-gut-brain axis. Neuropharmacology 2017, 112, 399–412. [Google Scholar] [CrossRef]
- Martinez, K.B.; Leone, V.; Chang, E.B. Microbial metabolites in health and disease: Navigating the unknown in search of function. J. Biol. Chem. 2017, 292, 8553–8559. [Google Scholar] [CrossRef]
- Silva, Y.P.; Bernardi, A.; Frozza, R.L. The Role of Short-Chain Fatty Acids From Gut Microbiota in Gut-Brain Communication. Front. Endocrinol. 2020, 11, 25. [Google Scholar] [CrossRef]
- Platten, M.; Nollen, E.A.A.; Röhrig, U.F.; Fallarino, F.; Opitz, C.A. Tryptophan metabolism as a common therapeutic target in cancer, neurodegeneration and beyond. Nat. Rev. Drug. Discov. 2019, 18, 379–401. [Google Scholar] [CrossRef]
- Berger, M.; Gray, J.A.; Roth, B.L. The expanded biology of serotonin. Annu. Rev. Med. 2009, 60, 355–366. [Google Scholar] [CrossRef]
- O’Mahony, S.M.; Clarke, G.; Borre, Y.E.; Dinan, T.G.; Cryan, J.F. Serotonin, tryptophan metabolism and the brain-gut-microbiome axis. Behav. Brain Res. 2015, 277, 32–48. [Google Scholar] [CrossRef]
- Müller, C.P.; Homberg, J.R. Serotonin revisited. Behav. Brain Res. 2015, 277, 1–2. [Google Scholar] [CrossRef]
- Jenkins, T.A.; Nguyen, J.C.; Polglaze, K.E.; Bertrand, P.P. Influence of Tryptophan and Serotonin on Mood and Cognition with a Possible Role of the Gut-Brain Axis. Nutrients 2016, 8, 56. [Google Scholar] [CrossRef]
- Loh, J.S.; Mak, W.Q.; Tan, L.K.S.; Ng, C.X.; Chan, H.H.; Yeow, S.H.; Foo, J.B.; Ong, Y.S.; How, C.W.; Khaw, K.Y. Microbiota-gut-brain axis and its therapeutic applications in neurodegenerative diseases. Signal Transduct. Target. Ther. 2024, 9, 37. [Google Scholar] [CrossRef] [PubMed]
- Preethy, S.; Ranganathan, N.; Raghavan, K.; Dedeepiya, V.D.; Ikewaki, N.; Abraham, S.J.K. Integrating the Synergy of the Gut Microbiome into Regenerative Medicine: Relevance to Neurological Disorders. J. Alzheimers Dis. 2022, 87, 1451–1460. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wang, Y.; Xiayu, X.; Shi, C.; Chen, W.; Song, N.; Fu, X.; Zhou, R.; Xu, Y.F.; Huang, L.; et al. Altered Gut Microbiota in a Mouse Model of ’Alzheimer’s Disease. J. Alzheimers Dis. 2017, 60, 1241–1257. [Google Scholar] [CrossRef]
- Kang, D.W.; Adams, J.B.; Gregory, A.C.; Borody, T.; Chittick, L.; Fasano, A.; Khoruts, A.; Geis, E.; Maldonado, J.; McDonough-Means, S.; et al. Microbiota Transfer Therapy alters gut ecosystem and improves gastrointestinal and autism symptoms: An open-label study. Microbiome 2017, 5, 10. [Google Scholar] [CrossRef]
- Liu, S.; Li, E.; Sun, Z.; Fu, D.; Duan, G.; Jiang, M.; Yu, Y.; Mei, L.; Yang, P.; Tang, Y.; et al. Altered gut microbiota and short chain fatty acids in Chinese children with autism spectrum disorder. Sci. Rep. 2019, 9, 287. [Google Scholar] [CrossRef]
- Scheperjans, F.; Aho, V.; Pereira, P.A.; Koskinen, K.; Paulin, L.; Pekkonen, E.; Haapaniemi, E.; Kaakkola, S.; Eerola-Rautio, J.; Pohja, M.; et al. Gut microbiota are related to ’Parkinson’s disease and clinical phenotype. Mov. Disord. 2015, 30, 350–358. [Google Scholar] [CrossRef]
- Felice, V.D.; Quigley, E.M.; Sullivan, A.M.; O’Keeffe, G.W.; O’Mahony, S.M. Microbiota-gut-brain signalling in ’Parkinson’s disease: Implications for non-motor symptoms. Park. Relat. Disord. 2016, 27, 1–8. [Google Scholar] [CrossRef]
- Braak, H.; de Vos, R.A.; Bohl, J.; Del Tredici, K. Gastric alpha-synuclein immunoreactive inclusions in ’Meissner’s and ’Auerbach’s plexuses in cases staged for ’Parkinson’s disease-related brain pathology. Neurosci. Lett. 2006, 396, 67–72. [Google Scholar] [CrossRef]
- Holmqvist, S.; Chutna, O.; Bousset, L.; Aldrin-Kirk, P.; Li, W.; Björklund, T.; Wang, Z.Y.; Roybon, L.; Melki, R.; Li, J.Y. Direct evidence of Parkinson pathology spread from the gastrointestinal tract to the brain in rats. Acta Neuropathol. 2014, 128, 805–820. [Google Scholar] [CrossRef]
- Cattaneo, A.; Cattane, N.; Galluzzi, S.; Provasi, S.; Lopizzo, N.; Festari, C.; Ferrari, C.; Guerra, U.P.; Paghera, B.; Muscio, C.; et al. Association of brain amyloidosis with pro-inflammatory gut bacterial taxa and peripheral inflammation markers in cognitively impaired elderly. Neurobiol. Aging 2017, 49, 60–68. [Google Scholar] [CrossRef]
- Quigley, E.M.M. Microbiota-Brain-Gut Axis and Neurodegenerative Diseases. Curr. Neurol. Neurosci. Rep. 2017, 17, 94. [Google Scholar] [CrossRef] [PubMed]
- Romano, S.; Savva, G.M.; Bedarf, J.R.; Charles, I.G.; Hildebrand, F.; Narbad, A. Meta-analysis of the ’Parkinson’s disease gut microbiome suggests alterations linked to intestinal inflammation. NPJ Park. Dis. 2021, 7, 27. [Google Scholar] [CrossRef] [PubMed]
- Sampson, T.R.; Debelius, J.W.; Thron, T.; Janssen, S.; Shastri, G.G.; Ilhan, Z.E.; Challis, C.; Schretter, C.E.; Rocha, S.; Gradinaru, V.; et al. Gut Microbiota Regulate Motor Deficits and Neuroinflammation in a Model of ’Parkinson’s Disease. Cell 2016, 167, 1469–1480.e2. [Google Scholar] [CrossRef]
- Qian, X.H.; Xie, R.Y.; Liu, X.L.; Chen, S.D.; Tang, H.D. Mechanisms of Short-Chain Fatty Acids Derived from Gut Microbiota in ’Alzheimer’s Disease. Aging Dis. 2022, 13, 1252–1266. [Google Scholar] [CrossRef]
- Colombo, A.V.; Sadler, R.K.; Llovera, G.; Singh, V.; Roth, S.; Heindl, S.; Sebastian Monasor, L.; Verhoeven, A.; Peters, F.; Parhizkar, S.; et al. Microbiota-derived short chain fatty acids modulate microglia and promote Aβ plaque deposition. eLife 2021, 10, e59826. [Google Scholar] [CrossRef]
- Cavanaugh, G.; Bai, J.; Tartar, J.L.; Lin, J.; Nunn, T.; Sangwan, N.; Patel, D.; Stanis, S.; Patel, R.K.; Rrukiqi, D.; et al. Enteric Dysbiosis in Children With Autism Spectrum Disorder and Associated Response to Stress. Cureus 2024, 16, e53305. [Google Scholar] [CrossRef]
- Di Lorenzo, C.; Ballerini, G.; Barbanti, P.; Bernardini, A.; D’Arrigo, G.; Egeo, G.; Frediani, F.; Garbo, R.; Pierangeli, G.; Prudenzano, M.P.; et al. Applications of Ketogenic Diets in Patients with Headache: Clinical Recommendations. Nutrients 2021, 13, 2307. [Google Scholar] [CrossRef]
- Barichella, M.; Pacchetti, C.; Bolliri, C.; Cassani, E.; Iorio, L.; Pusani, C.; Pinelli, G.; Privitera, G.; Cesari, I.; Faierman, S.A.; et al. Probiotics and prebiotic fiber for constipation associated with Parkinson disease: An RCT. Neurology 2016, 87, 1274–1280. [Google Scholar] [CrossRef]
- Grimaldi, R.; Gibson, G.R.; Vulevic, J.; Giallourou, N.; Castro-Mejía, J.L.; Hansen, L.H.; Leigh Gibson, E.; Nielsen, D.S.; Costabile, A. A prebiotic intervention study in children with autism spectrum disorders (ASDs). Microbiome 2018, 6, 133. [Google Scholar] [CrossRef]
- Schoonman, G.G.; van der Grond, J.; Kortmann, C.; van der Geest, R.J.; Terwindt, G.M.; Ferrari, M.D. Migraine headache is not associated with cerebral or meningeal vasodilatation—A 3T magnetic resonance angiography study. Brain 2008, 131, 2192–2200. [Google Scholar] [CrossRef]
- Amin, F.M.; Asghar, M.S.; Hougaard, A.; Hansen, A.E.; Larsen, V.A.; de Koning, P.J.; Larsson, H.B.; Olesen, J.; Ashina, M. Magnetic resonance angiography of intracranial and extracranial arteries in patients with spontaneous migraine without aura: A cross-sectional study. Lancet Neurol. 2013, 12, 454–461. [Google Scholar] [CrossRef]
- Moskowitz, M.A. Neurogenic versus vascular mechanisms of sumatriptan and ergot alkaloids in migraine. Trends Pharmacol. Sci. 1992, 13, 307–311. [Google Scholar] [CrossRef]
- Bagdy, G.; Riba, P.; Kecskeméti, V.; Chase, D.; Juhász, G. Headache-type adverse effects of NO donors: Vasodilation and beyond. Br. J. Pharmacol. 2010, 160, 20–35. [Google Scholar] [CrossRef]
- Gonzalez, A.; Hyde, E.; Sangwan, N.; Gilbert, J.A.; Viirre, E.; Knight, R. Migraines Are Correlated with Higher Levels of Nitrate-, Nitrite-, and Nitric Oxide-Reducing Oral Microbes in the American Gut Project Cohort. mSystems 2016, 1, e00105-16. [Google Scholar] [CrossRef]
- Qu, K.; Li, M.X.; Gan, L.; Cui, Z.T.; Li, J.J.; Yang, R.; Dong, M. To analyze the relationship between gut microbiota, metabolites and migraine: A two-sample Mendelian randomization study. Front. Microbiol. 2024, 15, 1325047. [Google Scholar] [CrossRef]
- Bai, J.; Shen, N.; Liu, Y. Associations between the Gut Microbiome and Migraines in Children Aged 7–18 Years: An Analysis of the American Gut Project Cohort. Pain Manag. Nurs. 2023, 24, 35–43. [Google Scholar] [CrossRef]
- de Roos, N.M.; van Hemert, S.; Rovers, J.M.P.; Smits, M.G.; Witteman, B.J.M. The effects of a multispecies probiotic on migraine and markers of intestinal permeability-results of a randomized placebo-controlled study. Eur. J. Clin. Nutr. 2017, 71, 1455–1462. [Google Scholar] [CrossRef]
- Martami, F.; Togha, M.; Seifishahpar, M.; Ghorbani, Z.; Ansari, H.; Karimi, T.; Jahromi, S.R. The effects of a multispecies probiotic supplement on inflammatory markers and episodic and chronic migraine characteristics: A randomized double-blind controlled trial. Cephalalgia 2019, 39, 841–853. [Google Scholar] [CrossRef]
- Naghibi, M.M.; Day, R.; Stone, S.; Harper, A. Probiotics for the Prophylaxis of Migraine: A Systematic Review of Randomized Placebo Controlled Trials. J. Clin. Med. 2019, 8, 1441. [Google Scholar] [CrossRef]
- Robblee, J.; Starling, A.J. SEEDS for success: Lifestyle management in migraine. Clevel. Clin. J. Med. 2019, 86, 741–749. [Google Scholar] [CrossRef]
- Houle, T.T.; Butschek, R.A.; Turner, D.P.; Smitherman, T.A.; Rains, J.C.; Penzien, D.B. Stress and sleep duration predict headache severity in chronic headache sufferers. Pain 2012, 153, 2432–2440. [Google Scholar] [CrossRef]
- Martin, V.T.; Vij, B. Diet and Headache: Part 1. Headache 2016, 56, 1543–1552. [Google Scholar] [CrossRef]
- Kurokawa, S.; Kishimoto, T.; Mizuno, S.; Masaoka, T.; Naganuma, M.; Liang, K.C.; Kitazawa, M.; Nakashima, M.; Shindo, C.; Suda, W.; et al. The effect of fecal microbiota transplantation on psychiatric symptoms among patients with irritable bowel syndrome, functional diarrhea and functional constipation: An open-label observational study. J. Affect. Disord. 2018, 235, 506–512. [Google Scholar] [CrossRef]
- Lelleck, V.V.; Schulz, F.; Witt, O.; Kühn, G.; Klein, D.; Gendolla, A.; Evers, S.; Gaul, C.; Thaçi, D.; Sina, C.; et al. A Digital Therapeutic Allowing a Personalized Low-Glycemic Nutrition for the Prophylaxis of Migraine: Real World Data from Two Prospective Studies. Nutrients 2022, 14, 2927. [Google Scholar] [CrossRef]
- Fila, M.; Chojnacki, J.; Pawlowska, E.; Sobczuk, P.; Chojnacki, C.; Blasiak, J. The Ketogenic Diet in the Prevention of Migraines in the Elderly. Nutrients 2023, 15, 4998. [Google Scholar] [CrossRef]
- Arab, A.; Khorvash, F.; Karimi, E.; Heidari, Z.; Askari, G. The effects of the dietary approaches to stop hypertension (DASH) diet on oxidative stress and clinical indices of migraine patients: A randomized controlled trial. Nutr. Neurosci. 2022, 25, 2259–2268. [Google Scholar] [CrossRef]
- Hindiyeh, N.A.; Zhang, N.; Farrar, M.; Banerjee, P.; Lombard, L.; Aurora, S.K. The Role of Diet and Nutrition in Migraine Triggers and Treatment: A Systematic Literature Review. Headache 2020, 60, 1300–1316. [Google Scholar] [CrossRef]
- Hauge, A.W.; Kirchmann, M.; Olesen, J. Characterization of consistent triggers of migraine with aura. Cephalalgia 2011, 31, 416–438. [Google Scholar] [CrossRef]
- Onderwater, G.L.J.; van Oosterhout, W.P.J.; Schoonman, G.G.; Ferrari, M.D.; Terwindt, G.M. Alcoholic beverages as trigger factor and the effect on alcohol consumption behavior in patients with migraine. Eur. J. Neurol. 2019, 26, 588–595. [Google Scholar] [CrossRef]
- Tai, M.S.; Yap, J.F.; Goh, C.B. Dietary trigger factors of migraine and tension-type headache in a South East Asian country. J. Pain. Res. 2018, 11, 1255–1261. [Google Scholar] [CrossRef]
- Takeshima, T.; Ishizaki, K.; Fukuhara, Y.; Ijiri, T.; Kusumi, M.; Wakutani, Y.; Mori, M.; Kawashima, M.; Kowa, H.; Adachi, Y.; et al. Population-based door-to-door survey of migraine in Japan: The Daisen study. Headache 2004, 44, 8–19. [Google Scholar] [CrossRef]
- Mostofsky, E.; Mittleman, M.A.; Buettner, C.; Li, W.; Bertisch, S.M. Prospective Cohort Study of Caffeinated Beverage Intake as a Potential Trigger of Headaches among Migraineurs. Am. J. Med. 2019, 132, 984–991. [Google Scholar] [CrossRef]
- Nowaczewska, M.; Wiciński, M.; Kaźmierczak, W. The Ambiguous Role of Caffeine in Migraine Headache: From Trigger to Treatment. Nutrients 2020, 12, 2259. [Google Scholar] [CrossRef]
- Charles, A. The role of caffeine in headache disorders. Curr. Opin. Neurol. 2024, 37, 289–294. [Google Scholar] [CrossRef]
- Xie, Y.; Zhou, G.; Xu, Y.; He, B.; Wang, Y.; Ma, R.; Chang, Y.; He, D.; Xu, C.; Xiao, Z. Effects of Diet Based on IgG Elimination Combined with Probiotics on Migraine Plus Irritable Bowel Syndrome. Pain. Res. Manag. 2019, 2019, 7890461. [Google Scholar] [CrossRef]
- Aydinlar, E.I.; Dikmen, P.Y.; Tiftikci, A.; Saruc, M.; Aksu, M.; Gunsoy, H.G.; Tozun, N. IgG-based elimination diet in migraine plus irritable bowel syndrome. Headache 2013, 53, 514–525. [Google Scholar] [CrossRef]
- Alpay, K.; Ertas, M.; Orhan, E.K.; Ustay, D.K.; Lieners, C.; Baykan, B. Diet restriction in migraine, based on IgG against foods: A clinical double-blind, randomised, cross-over trial. Cephalalgia 2010, 30, 829–837. [Google Scholar] [CrossRef]
- Al-Hashel, J.Y.; Abokalawa, F.; Toma, R.; Algubari, A.; Ahmed, S.F. Worsening of migraine headache with fasting Ramadan. Clin. Neurol. Neurosurg. 2021, 209, 106899. [Google Scholar] [CrossRef]
- Ragab, A.H.; Kishk, N.A.; Hassan, A.; Yacoub, O.; El Ghoneimy, L.; Elmazny, A.; Elsawy, E.H.; Mekkawy, D.; Othman, A.S.; Rizk, H.I.; et al. Changes in migraine characteristics over 30 days of Ramadan fasting: A prospective study. Headache 2021, 61, 1493–1498. [Google Scholar] [CrossRef] [PubMed]
- Abu-Salameh, I.; Plakht, Y.; Ifergane, G. Migraine exacerbation during Ramadan fasting. J. Headache Pain. 2010, 11, 513–517. [Google Scholar] [CrossRef]
- Turner, D.P.; Smitherman, T.A.; Penzien, D.B.; Porter, J.A.; Martin, V.T.; Houle, T.T. Nighttime snacking, stress, and migraine activity. J. Clin. Neurosci. 2014, 21, 638–643. [Google Scholar] [CrossRef]
- Rajapakse, T.; Gantenbein, A.R. Nutraceuticals in migraine. Handb. Clin. Neurol. 2024, 199, 125–144. [Google Scholar] [CrossRef]
- Quintana, S.; Russo, M.; Torelli, P. Nutraceuticals and migraine: Further strategy for the treatment of specific conditions. Neurol. Sci. 2022, 43, 6565–6567. [Google Scholar] [CrossRef] [PubMed]
- Tian, S.; Yu, X.; Wu, L.; Zheng, H.; Zhong, X.; Xie, Y.; Wu, W. Vitamin B(6) and folate intake are associated with lower risk of severe headache or migraine in adults: An analysis based on NHANES 1999-2004. Nutr. Res. 2024, 121, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Guo, Y.; Xia, M.; Zhang, J.; Zang, W. Dietary intake of thiamine and riboflavin in relation to severe headache or migraine: A cross-sectional survey. Headache 2022, 62, 1133–1142. [Google Scholar] [CrossRef] [PubMed]
- Thompson, D.F.; Saluja, H.S. Prophylaxis of migraine headaches with riboflavin: A systematic review. J. Clin. Pharm. Ther. 2017, 42, 394–403. [Google Scholar] [CrossRef] [PubMed]
- Slavin, M.; Li, H.; Khatri, M.; Frankenfeld, C. Dietary magnesium and migraine in adults: A cross-sectional analysis of the National Health and Nutrition Examination Survey 2001–2004. Headache 2021, 61, 276–286. [Google Scholar] [CrossRef] [PubMed]
- Arab, A.; Khorvash, F.; Karimi, E.; Hadi, A.; Askari, G. Associations between adherence to Mediterranean dietary pattern and frequency, duration, and severity of migraine headache: A cross-sectional study. Nutr. Neurosci. 2023, 26, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bakırhan, H.; Yıldıran, H.; Uyar Cankay, T. Associations between diet quality, DASH and Mediterranean dietary patterns and migraine characteristics. Nutr. Neurosci. 2022, 25, 2324–2334. [Google Scholar] [CrossRef] [PubMed]
- Ocal, R.; Karakurum-Goksel, B.; Van, M.; Coskun, O.; Karaaslan, C.; Ucler, S.; Gokcay, F.; Celebisoy, N.; Sirin, H.; Kisabay Ak, A.; et al. Eating attitudes of migraine patients in Turkey: A prospective multi-center study. BMC Neurol. 2024, 24, 180. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.; Tian, S.; Wu, L.; Zhong, X.; Liu, M.; Yu, X.; Xie, Y.; Wu, W. Dietary zinc intake in relation to migraine among adults: A cross sectional study of NHANES 1999-2004. Nutr. Neurosci. 2024, 27, 667–676. [Google Scholar] [CrossRef]
- Meng, S.H.; Zhou, H.B.; Li, X.; Wang, M.X.; Kang, L.X.; Fu, J.M.; Li, X.; Li, X.T.; Zhao, Y.S. Association Between Dietary Iron Intake and Serum Ferritin and Severe Headache or Migraine. Front. Nutr. 2021, 8, 685564. [Google Scholar] [CrossRef]
- Xu, L.; Zhang, C.; Liu, Y.; Shang, X.; Huang, D. Association between dietary potassium intake and severe headache or migraine in US adults: A population-based analysis. Front. Nutr. 2023, 10, 1255468. [Google Scholar] [CrossRef]
- Valente, M.; Garbo, R.; Filippi, F.; Antonutti, A.; Ceccarini, V.; Tereshko, Y.; Di Lorenzo, C.; Gigli, G.L. Migraine Prevention through Ketogenic Diet: More than Body Mass Composition Changes. J. Clin. Med. 2022, 11, 4946. [Google Scholar] [CrossRef] [PubMed]
- Barbanti, P.; Fofi, L.; Aurilia, C.; Egeo, G.; Caprio, M. Ketogenic diet in migraine: Rationale, findings and perspectives. Neurol. Sci. 2017, 38, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Boison, D. New insights into the mechanisms of the ketogenic diet. Curr. Opin. Neurol. 2017, 30, 187–192. [Google Scholar] [CrossRef]
- Caminha, M.C.; Moreira, A.B.; Matheus, F.C.; Rieger, D.K.; Moreira, J.D.; Dalmarco, E.M.; Demarchi, I.G.; Lin, K. Efficacy and tolerability of the ketogenic diet and its variations for preventing migraine in adolescents and adults: A systematic review. Nutr. Rev. 2022, 80, 1634–1647. [Google Scholar] [CrossRef] [PubMed]
- Haslam, R.L.; Bezzina, A.; Herbert, J.; Spratt, N.; Rollo, M.E.; Collins, C.E. Can Ketogenic Diet Therapy Improve Migraine Frequency, Severity and Duration? Healthcare 2021, 9, 1105. [Google Scholar] [CrossRef]
- Lovati, C.; d’Alessandro, C.M.; Ventura, S.D.; Muzio, F.; Pantoni, L. Ketogenic diet in refractory migraine: Possible efficacy and role of ketone bodies-a pilot experience. Neurol. Sci. 2022, 43, 6479–6485. [Google Scholar] [CrossRef] [PubMed]
- Tereshko, Y.; Dal Bello, S.; Di Lorenzo, C.; Pez, S.; Pittino, A.; Sartor, R.; Filippi, F.; Lettieri, C.; Belgrado, E.; Garbo, R.; et al. 2:1 ketogenic diet and low-glycemic-index diet for the treatment of chronic and episodic migraine: A single-center real-life retrospective study. J. Headache Pain 2023, 24, 95. [Google Scholar] [CrossRef]
- Neri, L.C.L.; Ferraris, C.; Catalano, G.; Guglielmetti, M.; Pasca, L.; Pezzotti, E.; Carpani, A.; Tagliabue, A. Ketosis and migraine: A systematic review of the literature and meta-analysis. Front. Nutr. 2023, 10, 1204700. [Google Scholar] [CrossRef]
- Batch, J.T.; Lamsal, S.P.; Adkins, M.; Sultan, S.; Ramirez, M.N. Advantages and Disadvantages of the Ketogenic Diet: A Review Article. Cureus 2020, 12, e9639. [Google Scholar] [CrossRef]
- Putananickal, N.; Gross, E.C.; Orsini, A.L.; Schmidt, S.; Hafner, P.; Gocheva, V.; Nagy, S.; Henzi, B.C.; Rubino, D.; Vogt, D.R.; et al. Efficacy and safety of exogenous beta-hydroxybutyrate for preventive treatment in episodic migraine: A single-centred, randomised, placebo-controlled, double-blind crossover trial. Cephalalgia 2022, 42, 302–311. [Google Scholar] [CrossRef]
- Gross, E.C.; Putananickal, N.; Orsini, A.-L.; Schoenen, J.; Fischer, D.; Soto-Mota, A. Defining metabolic migraine with a distinct subgroup of patients with suboptimal inflammatory and metabolic markers. Sci. Rep. 2023, 13, 3787. [Google Scholar] [CrossRef] [PubMed]
- Askarpour, M.; Yarizadeh, H.; Sheikhi, A.; Khorsha, F.; Mirzaei, K. Associations between adherence to MIND diet and severity, duration and frequency of migraine headaches among migraine patients. BMC Res. Notes 2020, 13, 341. [Google Scholar] [CrossRef]
- Chen, T.B.; Yang, C.C.; Tsai, I.J.; Yang, H.W.; Hsu, Y.C.; Chang, C.M.; Yang, C.P. Neuroimmunological effects of omega-3 fatty acids on migraine: A review. Front. Neurol. 2024, 15, 1366372. [Google Scholar] [CrossRef]
- Ramsden, C.E.; Zamora, D.; Faurot, K.R.; MacIntosh, B.; Horowitz, M.; Keyes, G.S.; Yuan, Z.-X.; Miller, V.; Lynch, C.; Honvoh, G.; et al. Dietary alteration of n-3 and n-6 fatty acids for headache reduction in adults with migraine: Randomized controlled trial. BMJ 2021, 374, n1448. [Google Scholar] [CrossRef] [PubMed]
- Evcili, G.; Utku, U.; Öğün, M.N.; Özdemir, G. Early and long period follow-up results of low glycemic index diet for migraine prophylaxis. Agri 2018, 30, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Hardy, T.M.; Tollefsbol, T.O. Epigenetic diet: Impact on the epigenome and cancer. Epigenomics 2011, 3, 503–518. [Google Scholar] [CrossRef]
- Fila, M.; Chojnacki, C.; Chojnacki, J.; Blasiak, J. Is an “Epigenetic Diet” for Migraines Justified? The Case of Folate and DNA Methylation. Nutrients 2019, 11, 2763. [Google Scholar] [CrossRef]
- Fila, M.; Pawłowska, E.; Blasiak, J. Mitochondria in migraine pathophysiology–does epigenetics play a role? Arch. Med. Sci. 2019, 15, 944–956. [Google Scholar] [CrossRef]
- Daniel, O.; Mauskop, A. Nutraceuticals in acute and prophylactic treatment of migraine. Curr. Treat. Options Neurol. 2016, 18, 14. [Google Scholar] [CrossRef]
- Bahrampour, N.; Mirzababaei, A.; Yarizadeh, H.; Barekzai, A.M.; Khorsha, F.; Clark, C.C.T.; Mirzaei, K. The relationship between dietary nutrients patterns and intensity and duration of migraine headaches. Br. J. Nutr. 2023, 129, 947–954. [Google Scholar] [CrossRef] [PubMed]
- Razeghi Jahromi, S.; Togha, M.; Ghorbani, Z.; Hekmatdoost, A.; Khorsha, F.; Rafiee, P.; Shirani, P.; Nourmohammadi, M.; Ansari, H. The association between dietary tryptophan intake and migraine. Neurol. Sci. 2019, 40, 2349–2355. [Google Scholar] [CrossRef] [PubMed]
- Jibril, A.T.; Shab-Bidar, S.; Djafarian, K.; Iddrisu, M.; Kwartemaah, I.S.O.; Yelarge, A. Effect of Major Dietary Interventions on Migraine: A Systematic Review of Randomized Control Trials. SN Compr. Clin. Med. 2022, 4, 185. [Google Scholar] [CrossRef]
- Karimi, E.; Tirani, S.A.; Azimi, E.S.; Askari, G.; As’habi, A.; Arab, A. Is there an association between a plant-based eating pattern and clinical findings of a migraine headache? Front. Nutr. 2023, 10, 1117740. [Google Scholar] [CrossRef] [PubMed]
- Morton, O.; Shehata, M.; Gabbitas, N.; Kassam, S. A Whole Food Plant-Based Approach for Migraine; A Case Series. Am. J. Lifestyle Med. 2022. [Google Scholar] [CrossRef]
- Perzia, B.M.; Dunaief, J.L.; Dunaief, D.M. Chronic migraine reversal and prevention with the LIFE diet: A nutrient dense whole food plant-based diet (WFPBD). BMJ Case Rep. 2021, 14, e243987. [Google Scholar] [CrossRef] [PubMed]
- Vaidyanathan, G. What humanity should eat to stay healthy and save the planet. Nature 2021, 600, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef] [PubMed]
- Altamura, C.; Cecchi, G.; Bravo, M.; Brunelli, N.; Laudisio, A.; Caprio, P.D.; Botti, G.; Paolucci, M.; Khazrai, Y.M.; Vernieri, F. The Healthy Eating Plate Advice for Migraine Prevention: An Interventional Study. Nutrients 2020, 12, 1579. [Google Scholar] [CrossRef]
- Balali, A.; Karimi, E.; Kazemi, M.; Hadi, A.; Askari, G.; Khorvash, F.; Arab, A. Associations between diet quality and migraine headaches: A cross-sectional study. Nutr. Neurosci. 2024, 27, 677–687. [Google Scholar] [CrossRef]
- Khalili, P.; Mirzababaei, A.; Abaj, F.; Ansari, S.; Harsini, A.R.; Hajmir, M.M.; Clark, C.C.T.; Mirzaei, K. The association between adherence to alternative healthy Diet Index (AHEI) and severity, disability, duration, and frequency of migraine headache among women: A cross-sectional study. Nutr. J. 2023, 22, 41. [Google Scholar] [CrossRef]
- Zhu, H.; Bi, D.; Zhang, Y.; Kong, C.; Du, J.; Wu, X.; Wei, Q.; Qin, H. Ketogenic diet for human diseases: The underlying mechanisms and potential for clinical implementations. Signal Transduct. Target. Ther. 2022, 7, 11. [Google Scholar] [CrossRef]
- Martins-Oliveira, M.; Akerman, S.; Holland, P.R.; Hoffmann, J.R.; Tavares, I.; Goadsby, P.J. Neuroendocrine signaling modulates specific neural networks relevant to migraine. Neurobiol. Dis. 2017, 101, 16–26. [Google Scholar] [CrossRef]
- He, Q.; Wang, W.; Xiong, Y.; Tao, C.; Ma, L.; Ma, J.; You, C.; Anttila, V.; Artto, V.; Belin, A.C.; et al. A causal effects of gut microbiota in the development of migraine. J. Headache Pain 2023, 24, 90. [Google Scholar] [CrossRef]
- Parohan, M.; Djalali, M.; Sarraf, P.; Yaghoubi, S.; Seraj, A.; Foroushani, A.R.; Ranji-Burachaloo, S.; Javanbakht, M.H. Effect of probiotic supplementation on migraine prophylaxis: A systematic review and meta-analysis of randomized controlled trials. Nutr. Neurosci. 2022, 25, 511–518. [Google Scholar] [CrossRef]
- Khorsha, F.; Mirzababaei, A.; Togha, M.; Mirzaei, K. Association of dietary diversity score (DDS) and migraine headache severity among women. Neurol. Sci. 2021, 42, 3403–3410. [Google Scholar] [CrossRef]
- Gazerani, P. A Bidirectional View of Migraine and Diet Relationship. Neuropsychiatr. Dis. Treat. 2021, 17, 435–451. [Google Scholar] [CrossRef]
- Ghavami, A.; Khorvash, F.; Heidari, Z.; Khalesi, S.; Askari, G. Effect of synbiotic supplementation on migraine characteristics and inflammatory biomarkers in women with migraine: Results of a randomized controlled trial. Pharmacol. Res. 2021, 169, 105668. [Google Scholar] [CrossRef]
- Lanza, M.; Filippone, A.; Casili, G.; Giuffrè, L.; Scuderi, S.A.; Paterniti, I.; Campolo, M.; Cuzzocrea, S.; Esposito, E. Supplementation with SCFAs Re-Establishes Microbiota Composition and Attenuates Hyperalgesia and Pain in a Mouse Model of NTG-Induced Migraine. Int. J. Mol. Sci. 2022, 23, 4847. [Google Scholar] [CrossRef]
- San Mauro Martín, I.; López Oliva, S.; Garicano Vilar, E.; Sánchez Niño, G.M.; Penadés, B.F.; Terrén Lora, A.; Sanz Rojo, S.; Collado Yurrita, L. Effects of Gluten on Gut Microbiota in Patients with Gastrointestinal Disorders, Migraine, and Dermatitis. Nutrients 2024, 16, 1228. [Google Scholar] [CrossRef]
- Slavin, M.; Li, H.A.; Frankenfeld, C.; Cheskin, L.J. What is Needed for Evidence-Based Dietary Recommendations for Migraine: A Call to Action for Nutrition and Microbiome Research. Headache 2019, 59, 1566–1581. [Google Scholar] [CrossRef]
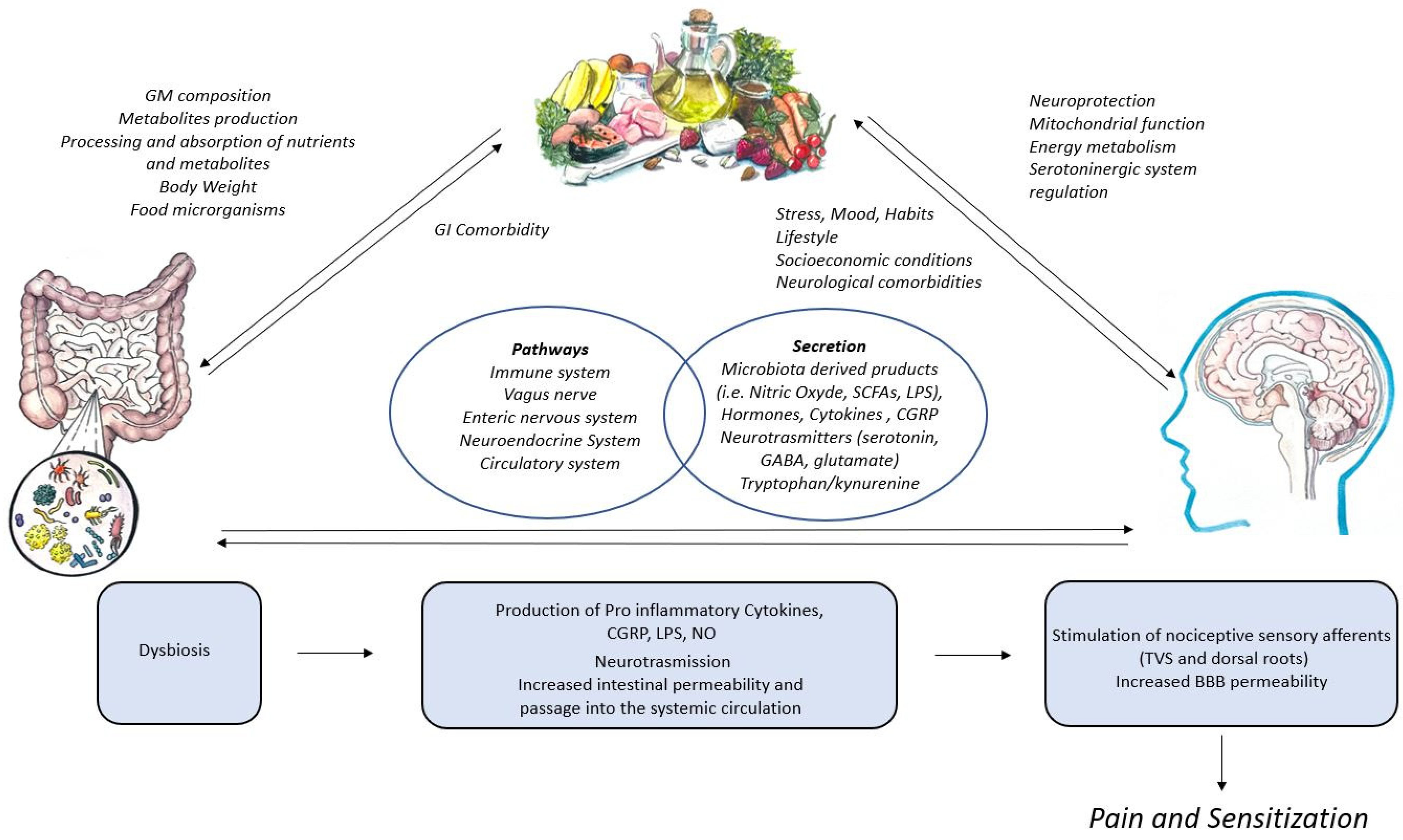
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).