
Effects of New Complementary Feeding Guidelines on Eating Behaviour, Food Consumption and Growth in Colombian Children: 6-Year Follow-Up of a Randomised Controlled Trial

Abstract
1. Introduction
2. Methods
2.1. Subjects and Study Design
2.1.1. Original Trial
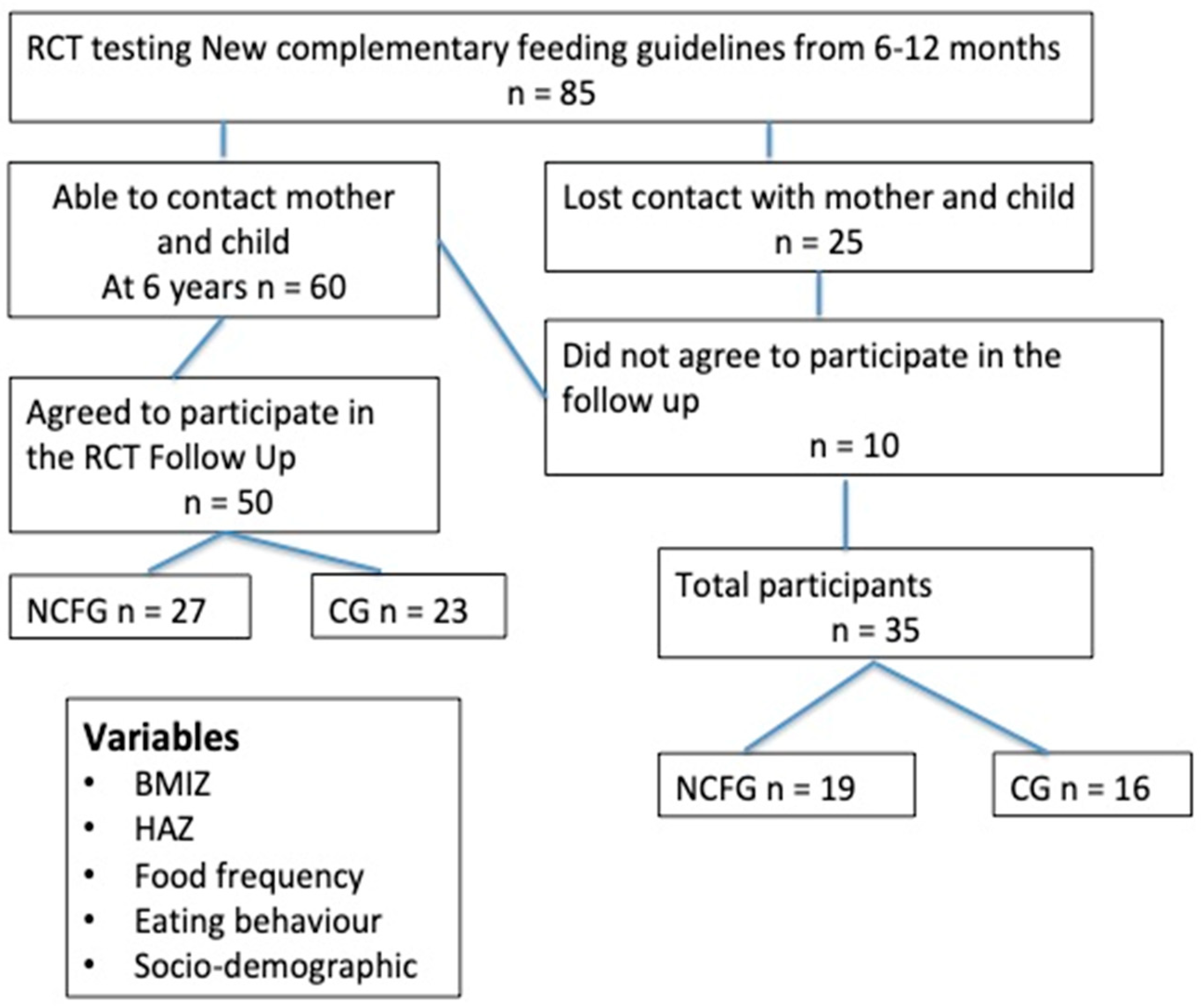
2.1.2. The 6-Year Follow-Up
2.2. Anthropometric Measurements at 6 Years of Age
2.3. Assessment of Frequency of Food Intake
2.4. Assessment of Eating Behaviour
3. Statistics
4. Results
4.1. Effects of NCFGs on Growth at 6 Years of Age
4.2. Food Intake
4.3. Eating Behaviour
4.4. Predictors of BMIZ at 6 Years of Age
4.5. Predictors of HAZ at 6 Years of Age
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Imai, C.M.; Gunnarsdottir, I.; Thorisdottir, B.; Halldorsson, T.I.; Thorsdottir, I. Associations between infant feeding practice prior to six months and body mass index at six years of age. Nutrients 2014, 6, 1608–1617. [Google Scholar] [CrossRef]
- Yang, Z.; Huffman, S.L. Nutrition in pregnancy and early childhood and associations with obesity in developing countries. Matern. Child Nutr. 2013, 9 (Suppl. 1), 105–119. [Google Scholar] [CrossRef] [PubMed]
- Pearce, J.; Langley-Evans, S.C. The types of food introduced during complementary feeding and risk of childhood obesity: A systematic review. Int. J. Obes. 2013, 37, 477–485. [Google Scholar] [CrossRef]
- Cattaneo, A.; Williams, C.; Pallás-Alonso, C.R.; Hernández-Aguilar, M.T.; Lasarte-Velillas, J.J.; Landa-Rivera, L.; Rouw, E.; Pina, M.; Volta, A.; Oudesluys-Murphy, A.M. ESPGHAN’s 2008 recommendation for early introduction of complementary foods: How good is the evidence? Matern. Child Nutr. 2011, 7, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Przyrembel, H. Timing of introduction of complementary food: Short- and long-term health consequences. Ann. Nutr. Metab. 2012, 60 (Suppl. 2), 8–20. [Google Scholar] [CrossRef] [PubMed]
- Qasem, W.; Fenton, T.; Friel, J. Age of introduction of first complementary feeding for infants: A systematic review. BMC Pediatr. 2015, 15, 107. [Google Scholar] [CrossRef] [PubMed]
- Habicht, J.P. Expert Consultation on the Optimal Duration of Exclusive Breastfeeding. In Protecting Infants through Human Milk; Advances in Experimental Medicine and Biology; Springer: Boston, MA, USA, 2004; pp. 79–87. [Google Scholar]
- Koletzko, B.; Von Kries, R.; Monasterolo, R.C.; Subías, J.E.; Scaglioni, S.; Giovannini, M.; Beyer, J.; Demmelmair, H.; Anton, B.; Gruszfeld, D.; et al. Can infant feeding choices modulate later obesity risk? Am. J. Clin. Nutr. 2009, 89, 1502S–1508S. [Google Scholar] [CrossRef]
- Patro-Gołab, B.; Zalewski, B.M.; Kouwenhoven, S.M.P.; Karaś, J.; Koletzko, B.; van Goudoever, J.B.; Szajewska, H. Protein concentration in milk formula, growth, and later risk of obesity: A systematic review. J. Nutr. 2016, 146, 551–564. [Google Scholar] [CrossRef]
- WHM; WHO. WHO|Facts and Figures on Childhood Obesity. 2017. Available online: https://www.who.int/end-childhood-obesity/facts/en/ (accessed on 21 February 2021).
- Keller, A.; Bucher Della Torre, S. Sugar-Sweetened Beverages and Obesity among Children and Adolescents: A Review of Systematic Literature Reviews. Child. Obes. 2015, 11, 338–346. [Google Scholar] [CrossRef]
- Sanigorski, A.M.; Bell, A.C.; Swinburn, B.A. Association of key foods and beverages with obesity in Australian schoolchildren. Public Health Nutr. 2007, 10, 152–157. [Google Scholar] [CrossRef]
- Olaya, G.A.; Lawson, M.; Fewtrell, M.S. Efficacy and safety of new complementary feeding guidelines with an emphasis on red meat consumption: A randomized trial in Bogota, Colombia. Am. J. Clin. Nutr. 2013, 98, 983–993. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Reference 2007: Growth Reference Data for 5–19 Years. 2007. Available online: http://www.who.int/growthref/en/ (accessed on 10 November 2020).
- Wardle, J.; Guthrie, C.A.; Sanderson, S.; Rapoport, L. Development of the children’s eating behaviour questionnaire. J. Child Psychol. Psychiatry 2001, 42, 963–970. [Google Scholar] [CrossRef]
- Fisk, C.M.; Crozier, S.R.; Inskip, H.M.; Godfrey, K.M.; Cooper, C.; Robinson, S.M. Influences on the quality of young children’s diets: The importance of maternal food choices. Br. J. Nutr. 2011, 105, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Warkentin, S.; Mais, L.A.; Latorre, M.D.R.D.D.O.; Carnell, S.; De Aguiar Carrazedotaddei, J.A. Relationships between parent feeding behaviors and parent and child characteristics in Brazilian preschoolers: A cross-sectional study. BMC Public Health 2018, 18, 704. [Google Scholar] [CrossRef] [PubMed]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors influencing children’s eating behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef] [PubMed]
- Llewellyn, C.H.; van Jaarsveld, C.H.M.; Johnson, L.; Carnell, S.; Wardle, J. Development and factor structure of the Baby Eating Behaviour Questionnaire in the Gemini birth cohort. Appetite 2011, 57, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Carnell, S.; Wardle, J. Appetitive traits in children. New evidence for associations with weight and a common, obesity-associated genetic variant. Appetite 2009, 53, 260–263. [Google Scholar] [CrossRef] [PubMed]
- Eagleton, S.G.; Shriver, L.H.; Buehler, C.; Wideman, L.; Leerkes, E.M. Bidirectional associations between maternal controlling feeding and food responsiveness during infancy. Front. Public Health 2022, 10, 975067. [Google Scholar] [CrossRef]
- Viana, V.; Sinde, S.; Saxton, J.C. Children’s Eating Behaviour Questionnaire: Associations with BMI in Portuguese children. Br. J. Nutr. 2008, 100, 445–450. [Google Scholar] [CrossRef]
- Sleddens, E.F.C.; Kremers, S.P.J.; Thijs, C. The Children’s Eating Behaviour Questionnaire: Factorial validity and association with Body Mass Index in Dutch children aged 6–7. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 49. [Google Scholar] [CrossRef]
- Boswell, N. Complementary feeding methods—A review of the benefits and risks. Int. J. Environ. Res. Public Health 2021, 18, 7165. [Google Scholar] [CrossRef] [PubMed]
- Webber, L.; Hill, C.; Saxton, J.; Van Jaarsveld, C.H.M.; Wardle, J. Eating behaviour and weight in children. Int. J. Obes. 2009, 33, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Bjørklund, O.; Wichstrøm, L.; Llewellyn, C.; Steinsbekk, S. The prospective relation between eating behaviors and BMI from middle childhood to adolescence: A 5-wave community study. Prev. Med. Rep. 2022, 27, 101795. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.M. Association of meat intake with overweight and obesity among school-aged children and adolescents. J. Obes. Metab. Syndr. 2017, 26, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Binnie, M.A.; Barlow, K.; Johnson, V.; Harrison, C. Red meats: Time for a paradigm shift in dietary advice. Meat Sci. 2014, 98, 445–451. [Google Scholar] [CrossRef]
- Daneshzad, E.; Askari, M.; Moradi, M.; Ghorabi, S.; Rouzitalab, T.; Heshmati, J.; Azadbakht, L. Red meat, overweight and obesity: A systematic review and meta-analysis of observational studies. Clin. Nutr. ESPEN 2021, 45, 66–74. [Google Scholar] [CrossRef]

{kind=link}
| Variable | Followed Up at 6 Years of Age (n = 50) | Not Followed Up (n = 35) | ||||
|---|---|---|---|---|---|---|
| NCFG Group (n = 23) | CG (n = 27) | Total n = 50 | NCFG Group (n = 19) | CG (n = 16) | Total (n = 35) | |
| Child’s age (mo) | 6.6 (±0.3) | 6.5 (±0.2) | 6.5 (±0.3) | 6.3 (±0.2) | 6.3 (±0.3) | 6.3 (±0.2) |
| Sex | ||||||
| Male, n (%) | 12 (52.2) | 13 (48.1) | 25 (50) | 8 (42.1) | 8 (50) | 16 (45.7) |
| Female, n (%) | 11 (47.8) | 14 (51.8) | 25 (50) | 11 (57.9) | 8 (50) | 19 (54.3) |
| Gestational age (wks) | ||||||
| Mean (SD) | 39.0 (±0.9) | 39.2 (±0.9) | 39.2 (±0.9) | 39.1 (±1.2) | 39.1 (±1.0) | 39.1 (±1.1) |
| Birth weight (g), mean (SD) | 2980 (±264) | 3134 (±379) | 3063 (±337) | 3133 (±286) | 3133 (±401) | 3133 (±338) |
| Birth length, mean (SD) | 49.2 (±1.7) | 50.4 (±1.9) | 49.8 (±1.8) | 50.3 (±1.4) | 50.2 (±1.9) | 50.3 (±1.6) |
| CF < 6 mo, n (%) | 10 (43.5) | 12 (44.4) | 21 (42.0) | 9 (47.4) | 9 (56.3) | 18 (51.4) |
| CF > 6 mo, n (%) | 13 (56.5) | 15 (55.6) | 29 (58) | 10 (52.6) | 7 (43.2) | 17 (48.6) |
| LAZ at 6 mo, mean (SD) | −1.11 (±1.0) | −0.71 (±1.0) | −0.89 (±1.1) | −0.68 (±1.2) | −0.65 (±0.8) | −0.66 (±1.0) |
| WLZ at 6 mo, mean (SD) | 0.22 (±0.9) | 0.83 (±1.0) | 0.55 (±1.0) | −0.05 (±0.7) | 0.4 (±1.1) | 0.15 (±0.9) |
| Mother’s age (y) | ||||||
| Mean (SD) | 32.4 (±7.3) | 32.7 (±9.7) | 32.6 (±8.7) | 23.5 (±6.8) | 22.1 (±6.5) | 22.9 (±6.6) |
| Marital status, n (%) | ||||||
| Single | 6 (26.1) | 4 (14.8) | 10 (20) | 5 (26.3) | 4 (25) | 9 (25.7) |
| Married | 4 (17.4) | 5 (18.5) | 9 (18) | 2 (10.5) | 0 (0) | 2 (5.7) |
| Living together | 12 (52.2) | 15 (55.6) | 27 (54) | 12 (63.2) | 12 (75) | 24 (68.6) |
| Mother’s education, n (%) | ||||||
| Primary | 1 (4.3) | 1 (3.7) | 2 (4) | 0 (0) | 2 (13.3) | 2 (5.9) |
| Mid-high school | 4 (17.4) | 2 (7.4) | 6 (12) | 8 (42,1) | 5 (33.3) | 13 (38.2) |
| Completed high school | 12 (52.2) | 12 (44.4) | 24 (48) | 7 (36.8) | 7 (46.7) | 14 (41.2) |
| Technician | 3 (33.3) | 9 (33.3) | 12 (24) | 3 (15.8) | 1 (6.7) | 4 (11.8) |
| Undergraduate | 1 (4.3) | 1 (3.7) | 2 (4) | 0 (0) | 0 (0) | 0 (0) |
| Family size, mean (SD) | 5.1 (±1.1) | 5.8 (±1.7) | 5.5 (±1.5) | 5.5 (±1.5) | 4.8 (±2.9) | 5.1 (±2.2) |
| House owner, n (%) | ||||||
| Yes | 7 (30.4) | 5 (18.5) | 3 (6) | 0 (0) | 0 (0) | 0 (0) |
| No | 16 (69.6) | 22 (81.5) | 47 (94) | 19 (100) | 16 (100) | 35 (100) |
| Variable | NCFG Group (n = 23) | CG (n = 27) | p-Value |
|---|---|---|---|
| Child’s age (years), mean (SD) | 6.6 (±0.3) | 6.5 (±0.2) | 0.27 |
| Sex | 0.50 | ||
| Male, n (%) | 12 (52.2) | 13 (48.1) | |
| Female, n (%) | 11 (47.8) | 14 (51.8) | |
| Months of EBF, mean (SD) | 5.6 (±0.6) | 5.3 (±0.8) | 0.22 |
| Months of TBF, mean (SD) | 25.4 (±12.9) | 20.2 (±8.8) | 0.10 |
| CF < 6 mo, n (%) | 10 (43.5) | 12 (44.4) | 0.58 |
| CF > 6 mo, n (%) | 13 (56.5) | 15 (53.6) | |
| LAZ at birth | −1.9 (±0.9) | 0.43 (±0.99) | 0.03 |
| LAZ at 12 mo, mean (SD) | −1.3 (±1.0) | −0.99 (±1.0) | 0.27 |
| WLZ at 12 mo, mean (SD) | 0.00 (±1.0) | 0.57 (±0.9) | 0.04 |
| BMIZ at 12 mo, mean (SD) | 0.17 (±0.97) | 0.72 (±0.9) | 0.05 |
| Mother’s stature (cm), mean (SD) | 154.8 (±7.4) | 158.3 (±5.4) | 0.08 |
| Mother’s BMI, mean (SD) | 24.9 (±3.0) | 25.5 (±4.7) | 0.61 |
| Socioeconomical status, n (%) | 0.49 | ||
| Level 1 | 1 (4.3) | 0 (0) | |
| Level 2 | 16 (69.6) | 18 (66.7) | |
| Level 3 | 6 (26.0) | 9 (33.3) |
| Variable | NCFG Group (n = 23) | CG (n = 27) | p-Value |
|---|---|---|---|
| Growth (mean (SD)) | |||
| BMI | 15.7 (±1.3) | 16.2 (±1.7) | 0.23 |
| BMIZ | 0.13 (±0.8) | 0.46 (±1.0) | 0.21 |
| HAZ | −0.74 (±0.8) | −0.14 (±0.9) | 0.02 |
| Change in BMIZ from 6 mo to 6 y | 0.08 (±1.2) | −0.33 (±1.2) | 0.29 |
| Change in BMIZ from 12 mo to 6 y | 0.003 (±1.3) | −0.24 (±1.2) | 0.55 |
| Change in HAZ from 6 mo to 6 y | 0.28 (±0.8) | 0.49 (±0.8) | 0.36 |
| Change in HAZ from 12 mo to 6 y | 0.48 (±0.8) | 0.77 (±0.9) | 0.24 |
| Overweight, n (%) | 3 (13) | 5 (18.5) | 0.54 |
| Obese, n (%) | 0 (0) | 1 (3.7) | |
| Mother’s weekly (number of times per week) food consumption (mean (SD)) | |||
| Red meat | 4.55 (±3.6) | 3.33 (±2.1) | 0.91 |
| Milk | 7.45 (±6.4) | 7.38 (±5.8) | 0.97 |
| Vegetables | 12.0 (±9.8) | 8.0 (±6.2) | 0.12 |
| Fruit | 11.8 (±6.0) | 11.6 (±14.6) | 0.95 |
| Processed food | 0.26 (±0.45) | 1.24 (±1.7) | 0.019 |
| Soft drinks | 1.4 (±3.2) | 3.4 (±4.9) | 0.049 |
| Sugary drinks | 0.21 (±0.5) | 1.05 (±1.7) | 0.045 |
| Chocolate drinks | 2.89 (±2.8) | 2.81 (±3.0) | 0.92 |
| Child’s weekly (number of times per week) food consumption (mean (SD)) | |||
| Red meat | 3.5 (±1.8) | 3.5 (±2.0) | 0.99 |
| Milk | 10.2 (±4.3) | 8.1 (±5.0) | 0.11 |
| Vegetables | 8.7 (±4.7) | 8.1 (±4.2) | 0.64 |
| Fruit | 14.9 (±5.3) | 13.5 (5.4) | 0.35 |
| Processed food | 3.0 (±2.6) | 2.9 (±2.4) | 0.78 |
| Soft drinks | 3.0 (±4.3) | 2.1 (±1.8) | 0.31 |
| Sugary drinks | 1.9 (±3.1) | 1.3 (±1.6) | 0.41 |
| Chocolate drinks | 3.5 (±2.4) | 5.9 (±5.1) | 0.048 |
| Eating Behaviour (mean (SD)) | |||
| Food responsiveness (FR) | 2.45 (±1.1) | 3.4 (±0.9) | 0.001 |
| Emotional overeating (EOE) | 2.6 (±0.7) | 2.8 (±0.9) | 0.30 |
| Enjoyment of food (EF) | 4.4 (±0.7) | 4.3 (±0.8) | 0.63 |
| Desire to drink (DD) | 4.5 (±0.8) | 4.6 (±0.6) | 0.64 |
| Satiety responsiveness (SR) | 3.5 (±0.8) | 3.1 (±0.9) | 0.20 |
| Slowness in eating (SE) | 3.4 (±0.9) | 3.2 (±0.8) | 0.42 |
| Emotional undereating (EUE) | 3.40 (±1.1) | 3.0 (±1.2) | 0.23 |
| Food fussiness (FF) | 3.5 (±0.6) | 3.7 (±0.5) | 0.17 |
| Food Consumption | Correlations Between Child’s and Mother’s Daily Food Consumption * | Correlations Between Child’s and Mother’s Weekly Food Consumption * |
|---|---|---|
| Milk | ||
| n | 41 | 41 |
| r | 0.539 | 0.341 |
| p | 0.0001 | 0.029 |
| Milk dairy | ||
| n | 41 | 41 |
| r | 0.417 | 0.413 |
| p | 0.007 | 0.007 |
| Vegetables | ||
| n | 40 | 40 |
| r | 0.528 | 0.465 |
| p | 0.0001 | 0.003 |
| Fruit | ||
| n | 40 | 40 |
| r | 0.398 | 0.408 |
| p | 0.011 | 0.009 |
| Red meat | ||
| n | 41 | 41 |
| r | 0.339 | 0.599 |
| p | 0.030 | 0.0001 |
| Variable | Standardised β Coefficient | 95% CI | p-Value |
|---|---|---|---|
| BMIZ at 6 years of age | |||
| Model 1 | |||
| Mother’s BMI | 0.084 | 0.011 to 0.158 | 0.025 |
| Model 2 | |||
| FR | 0.293 | 0.064 to 0.523 | 0.014 |
| Weekly red meat consumption at 12 mo | −0.169 | −0.310 to −0.028 | 0.020 |
| HAZ at 6 years of age | |||
| Model 1 | |||
| LAZ at 6 mo | 0.656 | 0.468 to 0.844 | 0.0001 |
| Model 2 | |||
| LAZ at 6 mo | 0.683 | 0.491 to 0.874 | 0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olaya Vega, G.; Fewtrell, M. Effects of New Complementary Feeding Guidelines on Eating Behaviour, Food Consumption and Growth in Colombian Children: 6-Year Follow-Up of a Randomised Controlled Trial. Nutrients 2024, 16, 2311. https://doi.org/10.3390/nu16142311
Olaya Vega G, Fewtrell M. Effects of New Complementary Feeding Guidelines on Eating Behaviour, Food Consumption and Growth in Colombian Children: 6-Year Follow-Up of a Randomised Controlled Trial. Nutrients. 2024; 16(14):2311. https://doi.org/10.3390/nu16142311
Chicago/Turabian StyleOlaya Vega, Gilma, and Mary Fewtrell. 2024. "Effects of New Complementary Feeding Guidelines on Eating Behaviour, Food Consumption and Growth in Colombian Children: 6-Year Follow-Up of a Randomised Controlled Trial" Nutrients 16, no. 14: 2311. https://doi.org/10.3390/nu16142311
APA StyleOlaya Vega, G., & Fewtrell, M. (2024). Effects of New Complementary Feeding Guidelines on Eating Behaviour, Food Consumption and Growth in Colombian Children: 6-Year Follow-Up of a Randomised Controlled Trial. Nutrients, 16(14), 2311. https://doi.org/10.3390/nu16142311