
Functional Foods and Adapted Physical Activity as New Adjuvant Therapy for Chronic Kidney Disease Patients

 ,
,  , , ,
, , ,  , , , ,
, , , ,  , , and
, , and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
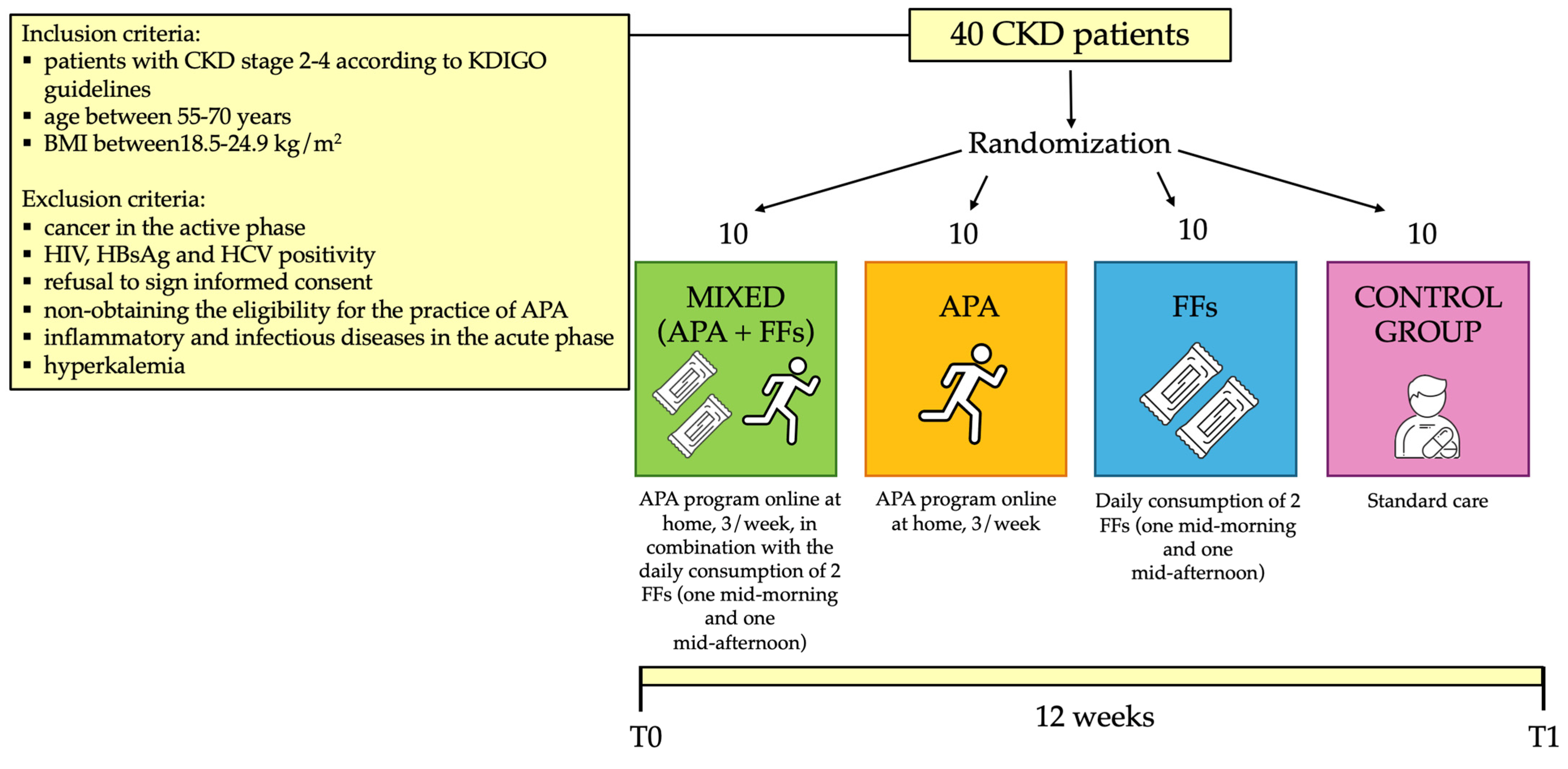
4.1. Patients
4.2. Laboratory Parameters and Biomarkers of Inflammation and Oxidative Stress
4.3. Questionnaires
4.4. Measurement of Anthropometric Parameters and Body Composition Assessment
4.5. Ultrasonographic Evaluation
4.6. Evaluation of Muscle Strength, Physical Performance and Flexibility
- (a)
- Muscle strength was evaluated through the hand grip ST, a dynamometer that evaluates the handgrip force (Jamar Plus, Performance Health (Warrenville, IL, USA). The seated patients were asked to squeeze the dynamometer as hard as possible with the elbow of the working hand at 90◦ close to the hip. The test was performed three times with both limbs, alternately, and the average value was considered. The cut-offs of hand grip ST are <30 kg for men and <20 kg for women [6].
- (b)
- The SPPB includes the gait speed (4 m walking), power (five-times chair sit to stand), and balance (tandem test). Each test is scored up to 4 points, and their sum indicates the level of performance. A sum of 12 points is the best score.
- The SCPT analyses the power of the lower limbs. Patients have to climb 10 steps as fast as possible, without running or jumping. The time required to complete the task was recorded.
- The SMWT evaluates the functional capacity. Patients have to walk, without running, for 6 min on 30 m of flat corridor. At the end of the test, the researchers recorded both the walking distance and the fatigue sensation through the BORG Scale (0–10) [71].
- (c)
- For flexibility, the following tests were conducted:
- The sit and reach test was used to evaluate the flexibility of the lower back and hamstring muscles. Patients were asked to sit on the floor with the feet placed against a box and to stretch, maintaining the legs straight. After two trials, the measurement of the third trial was recorded [72].
- The back scratch test was used to assess upper limb mobility. The shoulder range of motion was measured by this test in standing position. The upper limb that is brought up performs a combined movement of flexion, extra-rotation ad abduction, while the other one that is brought down performs a combined movement of extension, extra-rotation and adduction. The distance between the 2 punches behind the back for both arms is recorded in centimeters [73].
4.7. Composition of the Functional Food Bars
4.8. Physical Exercise Protocol
4.9. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Paniagua-Sierra, J.R.; Galvan-Plata, M.E. Chronic kidney disease. Rev. Med. Inst. Mex. Seguro Soc. 2017, 55, S116–S117. [Google Scholar] [PubMed]
- Kovesdy, C.P. Epidemiology of chronic kidney disease: An update 2022. Kidney Int. Suppl. 2022, 12, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Noce, A.; Marrone, G.; Ottaviani, E.; Guerriero, C.; Di Daniele, F.; Pietroboni Zaitseva, A.; Di Daniele, N. Uremic Sarcopenia and Its Possible Nutritional Approach. Nutrients 2021, 13, 147. [Google Scholar] [CrossRef] [PubMed]
- Molfino, A.; Chiappini, M.G.; Laviano, A.; Ammann, T.; Bollea, M.R.; Alegiani, F.; Rossi Fanelli, F.; Muscaritoli, M. Effect of intensive nutritional counseling and support on clinical outcomes of hemodialysis patients. Nutrition 2012, 28, 1012–1015. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, A.; Sanchez-Nino, M.D. Sarcopenia in CKD: A roadmap from basic pathogenetic mechanisms to clinical trials. Clin. Kidney J. 2019, 12, 110–112. [Google Scholar] [CrossRef] [PubMed]
- Van Ancum, J.M.; Alcazar, J.; Meskers, C.G.M.; Nielsen, B.R.; Suetta, C.; Maier, A.B. Impact of using the updated EWGSOP2 definition in diagnosing sarcopenia: A clinical perspective. Arch. Gerontol. Geriatr. 2020, 90, 104125. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef]
- Hu, L.; Napoletano, A.; Provenzano, M.; Garofalo, C.; Bini, C.; Comai, G.; La Manna, G. Mineral Bone Disorders in Kidney Disease Patients: The Ever-Current Topic. Int. J. Mol. Sci. 2022, 23, 2223. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Landi, F.; Topinkova, E.; Michel, J.P. Understanding sarcopenia as a geriatric syndrome. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 1–7. [Google Scholar] [CrossRef]
- Janssen, I.; Baumgartner, R.N.; Ross, R.; Rosenberg, I.H.; Roubenoff, R. Skeletal muscle cutpoints associated with elevated physical disability risk in older men and women. Am. J. Epidemiol. 2004, 159, 413–421. [Google Scholar] [CrossRef]
- Doherty, T.J. Invited review: Aging and sarcopenia. J. Appl. Physiol. 2003, 95, 1717–1727. [Google Scholar] [CrossRef] [PubMed]
- Wilund, K.R.; Thompson, S.; Viana, J.L.; Wang, A.Y. Physical Activity and Health in Chronic Kidney Disease. Contrib. Nephrol. 2021, 199, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Grazioli, E.; Tranchita, E.; Marrone, G.; Urciuoli, S.; Di Lauro, M.; Cerulli, C.; Piacentini, N.; Murri, A.; Celotto, R.; Romani, A.; et al. The Impact of Functional Bars and Adapted Physical Activity on Quality of Life in Chronic Kidney Disease: A Pilot Study. Int. J. Environ. Res. Public. Health 2022, 19, 3281. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Han, Z.; Granato, D. Polyphenols in foods: Classification, methods of identification, and nutritional aspects in human health. Adv. Food Nutr. Res. 2021, 98, 1–33. [Google Scholar] [CrossRef] [PubMed]
- Durazzo, A.; Lucarini, M.; Souto, E.B.; Cicala, C.; Caiazzo, E.; Izzo, A.A.; Novellino, E.; Santini, A. Polyphenols: A concise overview on the chemistry, occurrence, and human health. Phytother. Res. 2019, 33, 2221–2243. [Google Scholar] [CrossRef] [PubMed]
- Calderón-Oliver, M.; Ponce-Alquicira, E. Chapter 7—Fruits: A Source of Polyphenols and Health Benefits. In Natural and Artificial Flavoring Agents and Food Dyes; Grumezescu, A.M., Holban, A.M., Eds.; Academic Press: Cambridge, MA, USA, 2018; pp. 189–228. [Google Scholar] [CrossRef]
- Zekrumah, M.; Begua, P.; Razak, A.; Wahab, J.; Moffo, N.; Ivane, A.; Oman, M.; Elrashied, H.; Zou, X.; Zhang, D. Role of dietary polyphenols in non-communicable chronic disease prevention, and interactions in food systems: An overview. Nutrition 2023, 112, 112034. [Google Scholar] [CrossRef] [PubMed]
- Marrone, G.; Urciuoli, S.; Di Lauro, M.; Ruzzolini, J.; Ieri, F.; Vignolini, P.; Di Daniele, F.; Guerriero, C.; Nediani, C.; Di Daniele, N.; et al. Extra Virgin Olive Oil and Cardiovascular Protection in Chronic Kidney Disease. Nutrients 2022, 14, 4265. [Google Scholar] [CrossRef] [PubMed]
- Marrone, G.; Di Lauro, M.; Izzo, F.; Cornali, K.; Masci, C.; Vita, C.; Occhiuto, F.; Di Daniele, N.; De Lorenzo, A.; Noce, A. Possible Beneficial Effects of Hydrolyzable Tannins Deriving from Castanea sativa L. in Internal Medicine. Nutrients 2023, 16, 45. [Google Scholar] [CrossRef]
- Noce, A.; Di Lauro, M.; Di Daniele, F.; Pietroboni Zaitseva, A.; Marrone, G.; Borboni, P.; Di Daniele, N. Natural Bioactive Compounds Useful in Clinical Management of Metabolic Syndrome. Nutrients 2021, 13, 630. [Google Scholar] [CrossRef]
- Gothai, S.; Ganesan, P.; Park, S.Y.; Fakurazi, S.; Choi, D.K.; Arulselvan, P. Natural Phyto-Bioactive Compounds for the Treatment of Type 2 Diabetes: Inflammation as a Target. Nutrients 2016, 8, 461. [Google Scholar] [CrossRef]
- Benameur, T.; Porro, C.; Twfieg, M.E.; Benameur, N.; Panaro, M.A.; Filannino, F.M.; Hasan, A. Emerging Paradigms in Inflammatory Disease Management: Exploring Bioactive Compounds and the Gut Microbiota. Brain Sci. 2023, 13, 1226. [Google Scholar] [CrossRef]
- Bawa, S. The significance of soy protein and soy bioactive compounds in the prophylaxis and treatment of osteoporosis. J. Osteoporos. 2010, 2010, 891058. [Google Scholar] [CrossRef] [PubMed]
- Yuan, M.; Zhang, G.; Bai, W.; Han, X.; Li, C.; Bian, S. The Role of Bioactive Compounds in Natural Products Extracted from Plants in Cancer Treatment and Their Mechanisms Related to Anticancer Effects. Oxidative Med. Cell. Longev. 2022, 2022, 1429869. [Google Scholar] [CrossRef] [PubMed]
- Nicikowski, J.; Regula, J. Selected bioactive compounds in food of plant origin as natural immunomodulators in asthma and chronic obstructive pulmonary disease. Acta Sci. Pol. Technol. Aliment. 2021, 20, 383–397. [Google Scholar] [CrossRef]
- Grosso, G. Dietary Antioxidants and Prevention of Non-Communicable Diseases. Antioxidants 2018, 7, 94. [Google Scholar] [CrossRef] [PubMed]
- Marrone, G.; Urciuoli, S.; Candi, E.; Bernini, R.; Vanni, G.; Masci, C.; Guerriero, C.; Mancini, M.; De Lorenzo, A.; Vignolini, P.; et al. Biological Activities of Molecules Derived from Olea europaea L. Tested In Vitro. Life 2023, 14, 49. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Zhang, L.; Li, S. Advances in nutritional supplementation for sarcopenia management. Front. Nutr. 2023, 10, 1189522. [Google Scholar] [CrossRef] [PubMed]
- Noce, A.; Marrone, G.; Urciuoli, S.; Di Daniele, F.; Di Lauro, M.; Pietroboni Zaitseva, A.; Di Daniele, N.; Romani, A. Usefulness of Extra Virgin Olive Oil Minor Polar Compounds in the Management of Chronic Kidney Disease Patients. Nutrients 2021, 13, 581. [Google Scholar] [CrossRef]
- Romani, A.; Bernini, R.; Noce, A.; Urciuoli, S.; Di Lauro, M.; Pietroboni Zaitseva, A.; Marrone, G.; Di Daniele, N. Potential Beneficial Effects of Extra Virgin Olive Oils Characterized by High Content in Minor Polar Compounds in Nephropathic Patients: A Pilot Study. Molecules 2020, 25, 4757. [Google Scholar] [CrossRef]
- Romani, A.; Ieri, F.; Urciuoli, S.; Noce, A.; Marrone, G.; Nediani, C.; Bernini, R. Health Effects of Phenolic Compounds Found in Extra-Virgin Olive Oil, By-Products, and Leaf of Olea europaea L. Nutrients 2019, 11, 1776. [Google Scholar] [CrossRef]
- Romani, A.; Campo, M.; Urciuoli, S.; Marrone, G.; Noce, A.; Bernini, R. An Industrial and Sustainable Platform for the Production of Bioactive Micronized Powders and Extracts Enriched in Polyphenols From Olea europaea L. and Vitis vinifera L. Wastes. Front. Nutr. 2020, 7, 120. [Google Scholar] [CrossRef] [PubMed]
- Acar-Tek, N.; Agagunduz, D. Olive Leaf (Olea europaea L. folium): Potential Effects on Glycemia and Lipidemia. Ann. Nutr. Metab. 2020, 76, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.F.; Zhang, H. Phytochemical Constituents, Health Benefits, and Industrial Applications of Grape Seeds: A Mini-Review. Antioxidants 2017, 6, 71. [Google Scholar] [CrossRef] [PubMed]
- Cupisti, A.; D’Alessandro, C.; Fumagalli, G.; Vigo, V.; Meola, M.; Cianchi, C.; Egidi, M.F. Nutrition and physical activity in CKD patients. Kidney Blood Press. Res. 2014, 39, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Smart, N.A.; Williams, A.D.; Levinger, I.; Selig, S.; Howden, E.; Coombes, J.S.; Fassett, R.G. Exercise & Sports Science Australia (ESSA) position statement on exercise and chronic kidney disease. J. Sci. Med. Sport 2013, 16, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Senthil Kumar, T.G.; Soundararajan, P.; Maiya, A.G.; Ravi, A. Effects of graded exercise training on functional capacity, muscle strength, and fatigue after renal transplantation: A randomized controlled trial. Saudi J. Kidney Dis. Transplant. 2020, 31, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.P.; Burris, D.D.; Lucas, F.L.; Crocker, G.A.; Wasserman, J.C. Effects of a renal rehabilitation exercise program in patients with CKD: A randomized, controlled trial. Clin. J. Am. Soc. Nephrol. 2014, 9, 2052–2058. [Google Scholar] [CrossRef]
- Beto, J.A.; Schury, K.A.; Bansal, V.K. Strategies to promote adherence to nutritional advice in patients with chronic kidney disease: A narrative review and commentary. Int. J. Nephrol. Renovasc. Dis. 2016, 9, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Bossola, M.; Pellu, V.; Di Stasio, E.; Tazza, L.; Giungi, S.; Nebiolo, P.E. Self-reported physical activity in patients on chronic hemodialysis: Correlates and barriers. Blood Purif. 2014, 38, 24–29. [Google Scholar] [CrossRef]
- Schrauben, S.J.; Apple, B.J.; Chang, A.R. Modifiable Lifestyle Behaviors and CKD Progression: A Narrative Review. Kidney360 2022, 3, 752–778. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2024, 105, S117–S314. [Google Scholar] [CrossRef]
- Jha, V.; Al-Ghamdi, S.M.G.; Li, G.; Wu, M.S.; Stafylas, P.; Retat, L.; Card-Gowers, J.; Barone, S.; Cabrera, C.; Garcia Sanchez, J.J. Global Economic Burden Associated with Chronic Kidney Disease: A Pragmatic Review of Medical Costs for the Inside CKD Research Programme. Adv. Ther. 2023, 40, 4405–4420. [Google Scholar] [CrossRef]
- United Nations-Department of Economic and Social Affairs-Sustainable Development. Available online: https://sustainabledevelopment.un.org/content/documents/21252030 (accessed on 23 April 2024).
- Mapanga, R.F.; Tufts, M.A.; Shode, F.O.; Musabayane, C.T. Renal effects of plant-derived oleanolic acid in streptozotocin-induced diabetic rats. Ren. Fail. 2009, 31, 481–491. [Google Scholar] [CrossRef]
- Kim, H.J.; Vaziri, N.D.; Norris, K.; An, W.S.; Quiroz, Y.; Rodriguez-Iturbe, B. High-calorie diet with moderate protein restriction prevents cachexia and ameliorates oxidative stress, inflammation and proteinuria in experimental chronic kidney disease. Clin. Exp. Nephrol. 2010, 14, 536–547. [Google Scholar] [CrossRef]
- Albarrati, A.M.; Alghamdi, M.S.M.; Nazer, R.I.; Alkorashy, M.M.; Alshowier, N.; Gale, N. Effectiveness of Low to Moderate Physical Exercise Training on the Level of Low-Density Lipoproteins: A Systematic Review. Biomed. Res. Int. 2018, 2018, 5982980. [Google Scholar] [CrossRef]
- Avesani, C.M.; Kamimura, M.A.; Cuppari, L. Energy expenditure in chronic kidney disease patients. J. Ren. Nutr. 2011, 21, 27–30. [Google Scholar] [CrossRef]
- Xu, X.; Yang, Z.; Ma, T.; Li, Z.; Chen, Y.; Zheng, Y.; Dong, J. Novel equation for estimating resting energy expenditure in patients with chronic kidney disease. Am. J. Clin. Nutr. 2021, 113, 1647–1656. [Google Scholar] [CrossRef]
- Beavers, K.M.; Brinkley, T.E.; Nicklas, B.J. Effect of exercise training on chronic inflammation. Clin. Chim. Acta 2010, 411, 785–793. [Google Scholar] [CrossRef]
- Fedewa, M.V.; Hathaway, E.D.; Ward-Ritacco, C.L. Effect of exercise training on C reactive protein: A systematic review and meta-analysis of randomised and non-randomised controlled trials. Br. J. Sports Med. 2017, 51, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Salucci, S.; Bartoletti-Stella, A.; Bavelloni, A.; Aramini, B.; Blalock, W.L.; Fabbri, F.; Vannini, I.; Sambri, V.; Stella, F.; Faenza, I. Extra Virgin Olive Oil (EVOO), a Mediterranean Diet Component, in the Management of Muscle Mass and Function Preservation. Nutrients 2022, 14, 3567. [Google Scholar] [CrossRef] [PubMed]
- Noce, A.; Marrone, G.; Rovella, V.; Cusumano, A.; Di Daniele, N.; Casasco, M. Beneficial effects of physical activity on uremic sarcopenia. Med. Dello Sport 2018, 71, 370–392. [Google Scholar] [CrossRef]
- Grazioli, E.; Romani, A.; Marrone, G.; Di Lauro, M.; Cerulli, C.; Urciuoli, S.; Murri, A.; Guerriero, C.; Tranchita, E.; Tesauro, M.; et al. Impact of Physical Activity and Natural Bioactive Compounds on Endothelial Dysfunction in Chronic Kidney Disease. Life 2021, 11, 841. [Google Scholar] [CrossRef]
- Marrone, G.; Grazioli, E.; Tranchita, E.; Parisi, A.; Cerulli, C.; Murri, A.; Minganti, C.; Di Lauro, M.; Piacentini, N.; Galiuto, L.; et al. Effect of Online Home-Based Training on Functional Capacity and Strength in Two CKD Patients: A Case Study. Healthcare 2022, 10, 572. [Google Scholar] [CrossRef]
- Parkinson, L.; Keast, R. Oleocanthal, a phenolic derived from virgin olive oil: A review of the beneficial effects on inflammatory disease. Int. J. Mol. Sci. 2014, 15, 12323–12334. [Google Scholar] [CrossRef]
- Beauchamp, G.K.; Keast, R.S.; Morel, D.; Lin, J.; Pika, J.; Han, Q.; Lee, C.H.; Smith, A.B.; Breslin, P.A. Phytochemistry: Ibuprofen-like activity in extra-virgin olive oil. Nature 2005, 437, 45–46. [Google Scholar] [CrossRef]
- Ekramzadeh, M.; Santoro, D.; Kopple, J.D. The Effect of Nutrition and Exercise on Body Composition, Exercise Capacity, and Physical Functioning in Advanced CKD Patients. Nutrients 2022, 14, 2129. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Isaka, Y. Optimal Protein Intake in Pre-Dialysis Chronic Kidney Disease Patients with Sarcopenia: An Overview. Nutrients 2021, 13, 1205. [Google Scholar] [CrossRef]
- Evans, M.; Lewis, R.D.; Morgan, A.R.; Whyte, M.B.; Hanif, W.; Bain, S.C.; Davies, S.; Dashora, U.; Yousef, Z.; Patel, D.C.; et al. A Narrative Review of Chronic Kidney Disease in Clinical Practice: Current Challenges and Future Perspectives. Adv. Ther. 2022, 39, 33–43. [Google Scholar] [CrossRef]
- Kanbay, M.; Copur, S.; Yildiz, A.B.; Tanriover, C.; Mallamaci, F.; Zoccali, C. Physical exercise in kidney disease: A commonly undervalued treatment modality. Eur. J. Clin. Investig. 2024, 54, e14105. [Google Scholar] [CrossRef]
- Grazioli, E.; Cerulli, C.; Dimauro, I.; Moretti, E.; Murri, A.; Parisi, A. New Strategy of Home-Based Exercise during Pandemic COVID-19 in Breast Cancer Patients: A Case Study. Sustainability 2020, 12, 6940. [Google Scholar] [CrossRef]
- Pavlatou, M.G.; Papastamataki, M.; Apostolakou, F.; Papassotiriou, I.; Tentolouris, N. FORT and FORD: Two simple and rapid assays in the evaluation of oxidative stress in patients with type 2 diabetes mellitus. Metabolism 2009, 58, 1657–1662. [Google Scholar] [CrossRef] [PubMed]
- Guasch-Ferre, M.; Salas-Salvado, J.; Ros, E.; Estruch, R.; Corella, D.; Fito, M.; Martinez-Gonzalez, M.A.; Investigators, P. The PREDIMED trial, Mediterranean diet and health outcomes: How strong is the evidence? Nutr. Metab. Cardiovasc. Dis. 2017, 27, 624–632. [Google Scholar] [CrossRef] [PubMed]
- Lins, L.; Carvalho, F.M. SF-36 total score as a single measure of health-related quality of life: Scoping review. SAGE Open Med. 2016, 4, 2050312116671725. [Google Scholar] [CrossRef]
- Sabatino, A.; Regolisti, G.; Delsante, M.; Di Motta, T.; Cantarelli, C.; Pioli, S.; Grassi, G.; Batini, V.; Gregorini, M.; Fiaccadori, E. Noninvasive evaluation of muscle mass by ultrasonography of quadriceps femoris muscle in End-Stage Renal Disease patients on hemodialysis. Clin. Nutr. 2019, 38, 1232–1239. [Google Scholar] [CrossRef] [PubMed]
- Sabatino, A.; Regolisti, G.; Bozzoli, L.; Fani, F.; Antoniotti, R.; Maggiore, U.; Fiaccadori, E. Reliability of bedside ultrasound for measurement of quadriceps muscle thickness in critically ill patients with acute kidney injury. Clin. Nutr. 2017, 36, 1710–1715. [Google Scholar] [CrossRef]
- Treacy, D.; Hassett, L. The Short Physical Performance Battery. J. Physiother. 2018, 64, 61. [Google Scholar] [CrossRef] [PubMed]
- Agarwala, P.; Salzman, S.H. Six-Minute Walk Test: Clinical Role, Technique, Coding, and Reimbursement. Chest 2020, 157, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Alvi, Z.B.; Shukla, M.P. Evaluation of Functional Capacity and Rate of Perceived Exertion through Six-minute Walk Test in Pre and Post-haemodialysis Patients with Chronic Kidney Disease: A Prospective Cohort Study. J. Clin. Diagn. Res. 2023, 17, YC01–YC05. [Google Scholar] [CrossRef]
- Wells, K.; Dillon, E. The Sit and Reach—A Test of Back and Leg Flexibility. Res. Q. Am. Assoc. Health Phys. Educ. Recreat. 2013, 23, 115–118. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Development and validation of criterion-referenced clinically relevant fitness standards for maintaining physical independence in later years. Gerontologist 2013, 53, 255–267. [Google Scholar] [CrossRef] [PubMed]
- Campos, M.; Miguel, H. Elastic resistance training: Resistance exercise alternative in the home environment during COVID-19 pandemic. Int. Am. J. Med. Health 2020, 3. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Parameters | Mixed | APA | FFs | Controls | |
|---|---|---|---|---|---|
| Age (years) | N | 10 | 10 | 10 | 10 |
| T0 | 58.00 ± 8.25 a | 58.44 ± 8.28 a | 63.66 ± 4.61 a | 65.50 ± 4.43 a | |
| Gender (F/M) | N | 10 | 10 | 10 | 10 |
| T0 | 2/8 | 3/7 | 5/5 | 3/7 | |
| Weight (kg) | N | 10 | 10 | 10 | 10 |
| T0 | 84.72± 12.03 a | 75.98 ± 13.04 a | 75.20 ± 12.05 a | 71.73 ± 10.40 a | |
| BMI (kg/m2) | N | 10 | 10 | 10 | 10 |
| T0 | 28.72 ± 4.02 a | 27.40 ± 4.29 a | 26.93 ± 3.48 a | 26.64 ± 3.62 a |
| Laboratory Parameters | Mixed | APA | FFs | Controls | |
|---|---|---|---|---|---|
| Hemoglobin (g/dL) | T0 | 14.05 ± 1.79 a | 14.14 ± 1.62 a | 13.42±1.66 a | 13.75 ± 1.86 a |
| T1 | 13.98 ± 1.79 a | 13.91 ± 1.55 a | 13.25 ± 1.70 a | 13.79 ± 1.78 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| Creatinine (mg/dL) | T0 | 1.41 ± 0.46 a | 1.50 ± 0.32 a | 1.72 ± 0.65 a | 1.51 ± 0.45 a |
| T1 | 1.57 ± 0.57 a | 1.66 ± 0.36 a | 1.80 ± 0.63 a | 1.57 ± 0.46 a | |
| p | 0.0144 b | 0.0009 b | n.s. b | n.s. b | |
| e-GFR (mL/min/1.73 m2) e | T0 | 56.85 ± 20.97 a | 46.41 ± 10.83 a | 40.95 ± 15.03 a | 51.03 ± 18.29 a |
| T1 | 48.85 ± 15.22 a | 41.55 ± 10.32 a | 38.30 ± 13.44 a | 46.02 ± 12.98 a | |
| p | n.s. b | 0.0003 b | 0.0350 b | n.s. b | |
| Azotemia (mg/dL) | T0 | 59.11 ± 15.02 a | 47.44 ± 21.01 a | 57.00 ± 14.40 a | 61.22 ± 20.65 a |
| T1 | 54.00 ± 14.15 a | 50.78 ± 26.32 a | 52.00 ± 12.07 a | 67.32 ± 29.16 a | |
| p | 0.0272 b | n.s. b | n.s. b | n.s. b | |
| Sodium (mEq/L) | T0 | 139.5 ± 3.75 a | 141.11 ± 2.09 a | 141.00 ± 1.41 a | 140.56 ± 2.19 a |
| T1 | 140.4 ± 1.71 a | 141.00 ± 1.66 a | 141.00 ± 1.50 a | 140.44 ± 3.78 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| Potassium (mEq/L) | T0 | 4.39 ± 0.32 a | 4.06 ± 0.43 a | 4.34 ± 0.36 a | 4.54 ± 0.28 a |
| T1 | 4.31 ± 0.46 a | 4.01 ± 0.52 a | 4.33 ± 0.35 a | 4.71 ± 0.62 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| Calcium (mg/dL) | T0 | 9.32 ± 0.33 a | 9.40 ± 0.50 a | 9.38 ± 0.43 a | 9.32 ± 0.44 a |
| T1 | 9.24 ± 0.33 a | 9.29 ± 0.63 a | 18.74 ± 27.48 a | 9.36 ± 0.59 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| Phosphorus (mg/dL) | T0 | 3.24 ± 0.46 a | 3.12 ± 0.58 a | 3.12 ± 0.44 a | 3.35 ± 0.71 a |
| T1 | 3.27 ± 0.29 a | 3.13 ± 0.60 a | 3.28 ± 0.56 a | 3.45 ± 0.71 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| TC (mg/dL) | T0 | 196 (170–240) c | 239 (85–333) c | 185 (126–229) c | 189.5 (136–221) c |
| T1 | 187.5 (153–240) c | 200 (69–282) c | 159 (133–196) c | 177.5 (115–222) c | |
| p | n.s. d | 0.0039 d | n.s. d | n.s. d | |
| HDL-C (mg/dL) | T0 | 46 (35–73) c | 56.5 (37–75) c | 37 (27–67) c | 51 (35–63) c |
| T1 | 45 (32–66) c | 50.5 (31–73) c | 43 (27–67) c | 48 (34–64) c | |
| p | n.s. d | 0.0156 d | n.s. d | n.s. d | |
| LDL-C (mg/dL) | T0 | 125.11 ± 29.87 a | 135.62 ± 60.36 a | 99.50 ± 26.11 a | 121.5 ± 28.82 a |
| T1 | 123.22 ± 21.69 a | 124.75 ± 57.76 a | 100.12 ± 17.68 a | 113.87 ± 36.92 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| Triglycerides (mg/dL) | T0 | 129.9 ± 73.01 a | 176.75 ± 121.85 a | 142.44 ± 59.19 a | 112.78 ± 35.89 a |
| T1 | 140.44 ± 101.43 a | 172.12 ± 160.58 a | 124.67 ± 53.02 a | 98.00 ± 35.46 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| Albuminemia (gr/dL) | T0 | 4.74 ± 0.11 a | 4.61 ± 0.34 a | 4.70 ± 0.31 a | 4.58 ± 0.23 a |
| T1 | 4.59 ± 0.20 a | 4.56 ± 0.40 a | 4.65 ± 0.39 a | 4.67 ± 0.40 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| Albuminuria (mg/gr) f | T0 | 100.45 ± 119.95 a | 206.06 ± 412.21 a | 171.16 ± 253.04 a | 80.60 ± 66.23 a |
| T1 | 71.05 ± 103.97 a | 103.07 ± 174.35 a | 156.62 ± 235.89 a | 67.86 ± 51.39 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| Uricemia (mg/dL) | T0 | 6.30 ± 1.15 a | 6.59 ± 1.10 a | 5.82 ± 0.84 a | 5.97 ± 1.40 a |
| T1 | 6.36 ± 1.07 a | 6.64 ± 2.14 a | 6.05 ± 0.89 a | 5.64 ± 1.79 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b |
| Arterial Blood Pressure Parameters | Mixed | APA | FFs | Controls | |
|---|---|---|---|---|---|
| Systolic Pressure (mmHg) | T0 | 135.60 ± 22.32 a | 132.89 ± 13.18 a | 140.89 ± 12.78 a | 137.80 ± 17.13 a |
| T1 | 129.30 ± 14.97 a | 129.22 ± 18.80 a | 136.78 ± 10.71 a | 139.40 ± 16.17 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| Diastolic Pressure (mmHg) | T0 | 88.50 ± 15.28 a | 82.00 ± 12.84 a | 84.78 ± 9.35 a | 78.30 ± 9.57 a |
| T1 | 78.00 ± 9.77 a | 75.78 ± 9.36 a | 80.56 ± 5.17 a | 78.50 ± 8.83 a | |
| p | 0.0169 b | n.s. b | n.s. b | n.s. b |
| Biomarkers of Inflammation and Oxidative Stress | Mixed | APA | FFs | Controls | |
|---|---|---|---|---|---|
| FORT (U) | T0 | 271.40 ± 147.93 a | 311.78 ± 150.41 a | 287.22 ± 112.15 a | 347.33 ± 140.07 a |
| T1 | 336.70 ± 202.38 a | 312.33 ± 185.63 a | 283.00 ± 182.67 a | 254.33 ± 145.11 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| FORD (mmol/L Trolox equivalents) | T0 | 1.41 ± 0.47 a | 1.38 ± 0.68 a | 1.19 ± 0.29 a | 1.18 ± 0.56 a |
| T1 | 1.89 ± 0.54 a | 1.22 ± 0.55 a | 0.86 ± 0.48 a | 1.26 ± 0.35 a | |
| p | 0.0203 b | n.s. b | n.s. b | n.s. b | |
| CRP (mg/L) | T0 | 3.8 (0.4–9.5) c | 1.55 (1–5.1) c | 2.5 (0.4–7.9) c | 1.1 (0.5–5) c |
| T1 | 1.9 (0.4–5) c | 1.65 (0.8–5.6) c | 1.7 (0.6–8) c | 1.0 (0.5–7.5) c | |
| p | 0.0313 d | n.s. d | n.s. d | n.s. d | |
| ESR (mm/h) | T0 | 26.67 ± 16.72 a | 38.00 ± 18.48 a | 29.20 ± 33.57 a | 33.89 ± 25.14 a |
| T1 | 27.22 ± 15.31 a | 37.33 ± 18.12 a | 26.80 ± 27.64 a | 34.55 ± 23.20 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b |
| Anthropometric Body Composition and Ultrasonographic Evaluation Parameters | Mixed | APA | FFs | Controls | |
|---|---|---|---|---|---|
| Weight (kg) | T0 | 84.72 ± 12.03 a | 75.98 ± 13.04 a | 75.20 ± 12.05 a | 71.73 ± 10.40 a |
| T1 | 84.08 ± 11.85 a | 75.37 ± 12.98 a | 75.49 ± 11.51 a | 72.20 ± 10.52 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| BMI (kg/m2) | T0 | 28.72 ± 4.02 a | 27.40 ± 4.29 a | 26.93 ± 3.48 a | 26.64 ± 3.62 a |
| T1 | 28.68 ± 4.14 a | 27.23 ± 4.54 a | 27.04 ± 3.39 a | 26.84 ± 3.84 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| Resistance (Ω) | T0 | 464.5 ± 60.29 a | 518.78 ± 74.71 a | 517.62 ± 62.66 a | 490.90 ± 107.24 a |
| T1 | 466.40 ± 60.07 a | 479.00 ± 47.22 a | 517.87 ± 92.06 a | 490.90 ± 96.41 a | |
| p | n.s. b | 0.0491 b | n.s. b | n.s. b | |
| Reactance (Ω) | T0 | 39.80 ± 5.67 a | 49.89 ± 8.15 a | 45.22 ± 6.73 a | 41.5 ± 6.45 a |
| T1 | 45.40 ± 8.03 a | 52.00 ± 9.38 a | 47.75 ± 10.46 a | 44.9 ± 6.19 a | |
| p | 0.0232 b | n.s. b | n.s. b | n.s. b | |
| Phase angle (°) | T0 | 5.56 ± 0.81 a | 5.73 ± 0.85 a | 4.92 ± 0.73 a | 4.99 ± 1.00 a |
| T1 | 5.06 ± 0.89 a | 5.63 ± 0.40 a | 5.60 ± 1.08 a | 5.33 ± 0.94 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| TBW (%) | T0 | 53.89 ± 4.82 a | 52.60 ± 5.43 a | 53.31 ± 5.96 a | 56.47 ± 7.86 a |
| T1 | 53.99 ± 4.65 a | 54.20 ± 5.61 a | 54.71 ± 7.50 a | 56.17 ± 6.42 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| ECW (%) | T0 | 50.86 ± 4.44 a | 47.14 ± 3.61 a | 50.94 ± 4.35 a | 51.59 ± 6.73 a |
| T1 | 47.87 ± 4.68 a | 45.81 ± 2.10 a | 49.51 ± 3.86 a | 49.39 ± 5.21 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| FM (%) | T0 | 27.00 ± 6.32 a | 29.01 ± 7.37 a | 27.84 ± 8.50 a | 24.22 ± 11.68 a |
| T1 | 25.92 ± 5.66 a | 25.77 ± 6.55 a | 27.36 ± 10.03 a | 28.02 ± 17.09 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| FFM (%) | T0 | 69.36 ± 7.27 a | 72.02 ± 7.08 a | 72.16 ± 8.50 a | 75.78 ± 11.68 a |
| T1 | 74.14 ± 5.55 a | 73.41 ± 7.14 a | 72.63 ± 10.03 a | 75.94 ± 9.02 a | |
| p | 0.0258 b | n.s. b | n.s. b | n.s. b | |
| BCM (%) | T0 | 48.51 ± 4.48 a | 51.34 ± 1.91 a | 48.17 ± 4.59 a | 47.48 ± 7.11 a |
| T1 | 50.90 ± 5.26 a | 54.27 ± 3.69 a | 49.70 ± 4.10 a | 49.82 ± 5.52 a | |
| p | n.s. b | 0.0270 b | n.s. b | n.s. b | |
| QRFT left 1/2 (cm) | T0 | 1.36 ± 0.38 a | 1.58 ± 0.15 a | 1.47 ± 0.47 a | 1.64 ± 0.34 a |
| T1 | 1.47 ± 0.61 a | 1.77 ± 0.25 a | 1.48 ± 0.49 a | 1.54 ± 0.40 a | |
| p | n.s. b | 0.0465 b | n.s. b | n.s. b | |
| QRFT right 1/2 (cm) | T0 | 1.33 ± 0.40 a | 1.46 ± 0.32 a | 1.33 ± 0.38 a | 1.47 ± 0.31 a |
| T1 | 1.49 ± 0.64 a | 1.76 ± 0.48 a | 1.38 ± 0.39 a | 1.54 ± 0.31 a | |
| p | n.s. b | 0.0255 b | n.s. b | n.s. b | |
| QRFT left 2/3 (cm) | T0 | 1.21 ± 0.58 a | 1.59 ± 0.30 a | 1.27 ± 0.43 a | 1.51 ± 0.40 a |
| T1 | 1.33 ± 0.54 a | 1.79 ± 0.34 a | 1.25 ± 0.43 a | 1.43 ± 0.35 a | |
| p | n.s. b | 0.0480 b | n.s. b | n.s. b | |
| QRFT right 2/3 (cm) | T0 | 1.23 ± 0.59 a | 1.48 ± 0.38 a | 1.24 ± 0.49 a | 1.57 ± 0.44 a |
| T1 | 1.37 ± 0.55 a | 1.66 ± 0.45 a | 1.32 ± 0.41 a | 1.41 ± 0.43 a | |
| p | n.s. b | n.s. b | n.s. b | 0.0435 b |
| Evaluation of Physical Performance and Muscle Strength | Mixed | APA | FFs | Controls | |
|---|---|---|---|---|---|
| SPPB (points) | T0 | 11.70 ± 0.95 a | 11.56 ± 0.73 a | 9.89 ± 1.83 a | 10.80 ± 1.40 a |
| T1 | 12.00 ± 0.00 a | 11.89 ± 0.33 a | 11.33 ± 0.87 a | 10.50 ± 2.07 a | |
| p | n.s. b | n.s. b | 0.0316 b | n.s. b | |
| SMWT (m) | T0 | 572.00 ± 75.98 a | 603.75 ± 107.03 a | 473.61 ± 152.27 a | 504.00 ± 145.37 a |
| T1 | 624.50 ± 89.15 a | 636.87 ± 97.13 a | 502.67 ± 108.16 a | 505.50 ± 151.30 a | |
| p | 0.0002 b | 0.0070 b | n.s. b | n.s. b | |
| SMWT BORG (points) | T0 | 2.50 ± 1.33 a | 3.22 ± 1.20 a | 2.56 ± 1.01 a | 2.90 ± 1.20 a |
| T1 | 3.10 ± 1.33 a | 2.94 ± 1.01 a | 2.50 ± 0.87 a | 2.70 ± 1.51 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| SCPT (W) | T0 | 357.20 ± 113.04 a | 371. 21 ± 128.80 a | 192.70 ± 97.57 a | 258.40 ± 81.59 a |
| T1 | 363.04 ± 77.61 a | 345.43 ± 85.75 a | 227.53 ± 109.02 a | 270.80 ± 69.95 a | |
| p | n.s. b | n.s. b | 0.0280 b | n.s. b | |
| HGST right (kg) | T0 | 41.84 ± 13.14 a | 40.01 ± 12.48 a | 31.98 ± 13.99 a | 32.50 ± 10.21 a |
| T1 | 43.53 ± 14.98 a | 43.03 ± 14.70 a | 34.47 ± 11.96 a | 31.60 ± 11.35 a | |
| p | n.s. b | n.s. b | 0.0500 b | n.s. b | |
| HGST left (kg) | T0 | 38.83 ± 13.68 a | 36.85 ± 11.18 a | 28.84 ± 11.05 a | 29.65 ± 10.70 a |
| T1 | 41.25 ± 13.79 a | 39.30 ± 12.47 a | 29.43 ± 10.09 a | 30.30 ± 12.30 a | |
| p | 0.0491 b | n.s. b | n.s. b | n.s. b | |
| Scratch test right (cm) | T0 | 29.90 ± 9.05 a | 23.56 ± 10.27 a | 39.89 ± 10.86 a | 38.10 ± 10.64 a |
| T1 | 30.40 ± 6.20 a | 22.72 ± 9.50 a | 33.89 ± 8.12 a | 34.00 ± 6.25 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| Scratch test left (cm) | T0 | 27.50 ± 6.19 a | 28.00 ± 8.65 a | 43.28 ± 9.69 a | 41.80 ± 11.64 a |
| T1 | 27.90 ± 6.85 a | 27.44 ± 8.14 a | 36.78 ± 9.54 a | 37.90 ± 6.37 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b | |
| Sit and reach (cm) | T0 | −6.15 ± 12.05 a | −6.56 ± 6.82 a | −14.00 ± 11.48 a | −10.90 ± 8.16 a |
| T1 | −2.75 ± 5.98 a | −2.67 ± 4.76 a | −11.37 ± 13.00 a | −10.60 ± 8.14 a | |
| p | n.s. b | n.s. b | n.s. b | n.s. b |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marrone, G.; Murri, A.; Urciuoli, S.; Di Lauro, M.; Grazioli, E.; Vignolini, P.; Cornali, K.; Tranchita, E.; Masci, C.; Cerulli, C.; et al. Functional Foods and Adapted Physical Activity as New Adjuvant Therapy for Chronic Kidney Disease Patients. Nutrients 2024, 16, 2325. https://doi.org/10.3390/nu16142325
Marrone G, Murri A, Urciuoli S, Di Lauro M, Grazioli E, Vignolini P, Cornali K, Tranchita E, Masci C, Cerulli C, et al. Functional Foods and Adapted Physical Activity as New Adjuvant Therapy for Chronic Kidney Disease Patients. Nutrients. 2024; 16(14):2325. https://doi.org/10.3390/nu16142325
Chicago/Turabian StyleMarrone, Giulia, Arianna Murri, Silvia Urciuoli, Manuela Di Lauro, Elisa Grazioli, Pamela Vignolini, Kevin Cornali, Eliana Tranchita, Claudia Masci, Claudia Cerulli, and et al. 2024. "Functional Foods and Adapted Physical Activity as New Adjuvant Therapy for Chronic Kidney Disease Patients" Nutrients 16, no. 14: 2325. https://doi.org/10.3390/nu16142325