

Sourdough Bread with Different Fermentation Times: A Randomized Clinical Trial in Subjects with Metabolic Syndrome
 , , , , ,
, , , , ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Ethical Aspects
2.3. Bread Composition and Fermentation Process
2.4. General and Lifestyle Data
2.5. Anthropometric and Exploration Data
2.6. Laboratory Analysis
2.7. Intestinal Microbiota Analysis
2.8. Bioinformatic Analysis
2.9. Sample Size
2.10. Statistical Analysis
3. Results
3.1. Study Population
3.2. Dietetic Assessment
3.3. Clinical Parameters, Inflammatory Biomarkers, and Satiety-Related Hormones
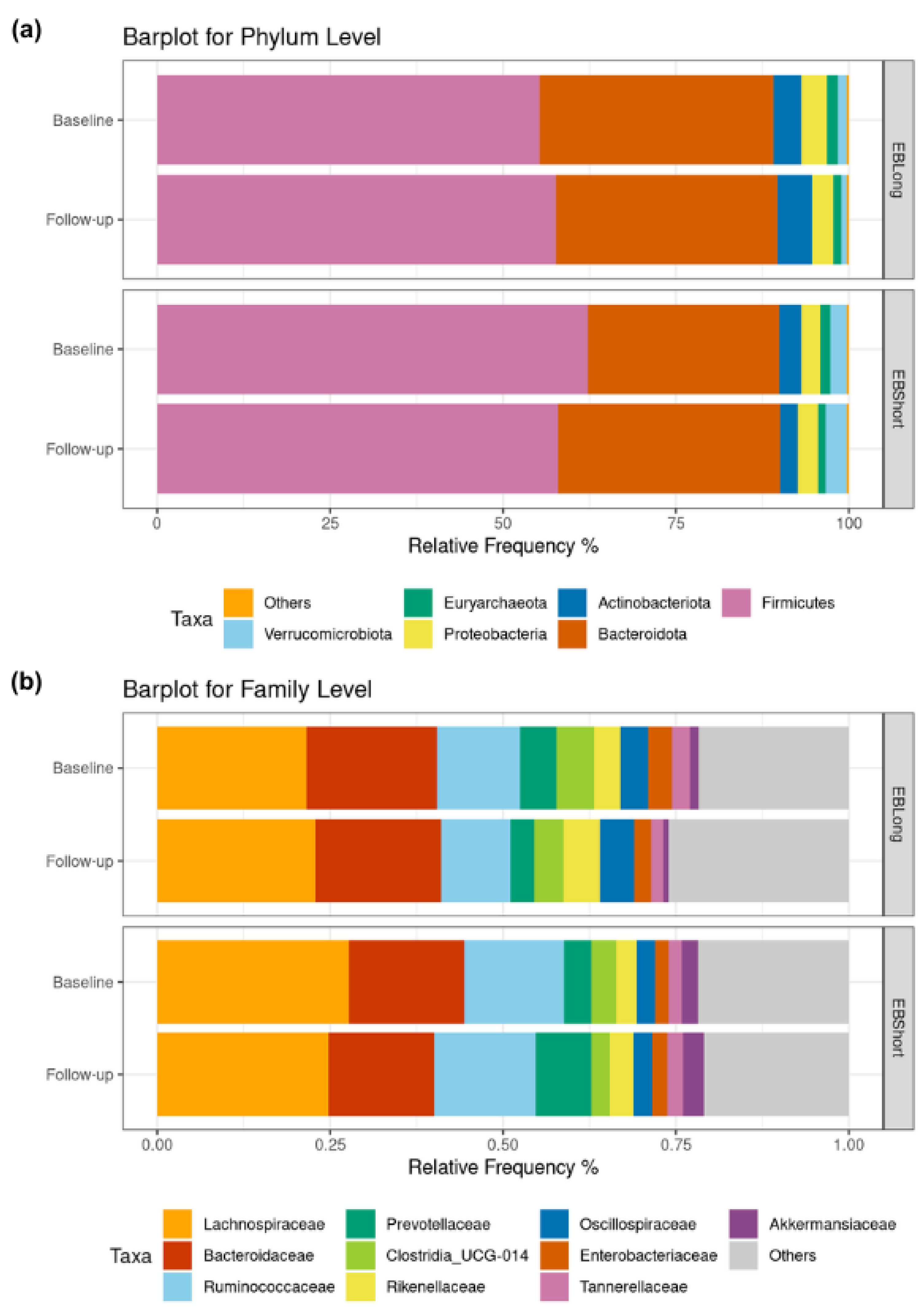
3.4. Microbiota Characterization
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shin, J.A.; Lee, J.H.; Lim, S.Y.; Ha, H.S.; Kwon, H.S.; Park, Y.M.; Lee, W.C.; Kang, M.I.; Yim, H.W.; Yoon, K.H.; et al. Metabolic Syndrome as a Predictor of Type 2 Diabetes, and Its Clinical Interpretations and Usefulness. J. Diabetes Investig. 2013, 4, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Galassi, A.; Reynolds, K.; He, J. Metabolic Syndrome and Risk of Cardiovascular Disease: A Meta-Analysis. Am. J. Med. 2006, 119, 812–819. [Google Scholar] [CrossRef]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the Metabolic Syndrome: A Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; And International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed]
- Rippe, J.M. Lifestyle Strategies for Risk Factor Reduction, Prevention, and Treatment of Cardiovascular Disease. Am. J. Lifestyle Med. 2019, 13, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Capurso, A. The Mediterranean Diet: A Historical Perspective. Aging Clin. Exp. Res. 2024, 36, 78. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Kastorini, C.M.; Panagiotakos, D.B.; Giugliano, D. Mediterranean Diet and Metabolic Syndrome: An Updated Systematic Review. Rev. Endocr. Metab. Disord. 2013, 14, 255–263. [Google Scholar] [CrossRef]
- Capurso, A.; Capurso, C. The Mediterranean Way: Why Elderly People Should Eat Wholewheat Sourdough Bread—A Little Known Component of the Mediterranean Diet and Healthy Food for Elderly Adults. Aging Clin. Exp. Res. 2020, 32, 1–5. [Google Scholar] [CrossRef]
- Arendt, E.K.; Ryan, L.A.M.; Dal Bello, F. Impact of Sourdough on the Texture of Bread. Food Microbiol. 2007, 24, 165–174. [Google Scholar] [CrossRef]
- Olagnero, G.; Abad, A.; Bendersky, S.; Genevois, C.; Granzella, L.; Montonati, M. Alimentos Funcionales: Fibra, Prebióticos, Probióticos y Simbióticos. Diaeta 2007, 25, 20–33. [Google Scholar]
- Akamine, I.T.; Mansoldo, F.R.P.; Vermelho, A.B. Probiotics in the Sourdough Bread Fermentation: Current Status. Fermentation 2023, 9, 90. [Google Scholar] [CrossRef]
- Lau, S.W.; Chong, A.Q.; Chin, N.L.; Talib, R.A.; Basha, R.K. Sourdough Microbiome Comparison and Benefits. Microorganisms 2021, 9, 1355. [Google Scholar] [CrossRef]
- Canesin, M.R.; Cazarin, C.B.B. Nutritional Quality and Nutrient Bioaccessibility in Sourdough Bread. Curr. Opin. Food Sci. 2021, 40, 81–86. [Google Scholar] [CrossRef]
- Chavan, R.S.; Chavan, S.R. Sourdough Technology-A Traditional Way for Wholesome Foods: A Review. Compr. Rev. Food Sci. Food Saf. 2011, 10, 169–182. [Google Scholar] [CrossRef]
- Gänzle, M.G.; Qiao, N.; Bechtner, J. The Quest for the Perfect Loaf of Sourdough Bread Continues: Novel Developments for Selection of Sourdough Starter Cultures. Int. J. Food Microbiol. 2023, 407, 110421. [Google Scholar] [CrossRef] [PubMed]
- Lluansí, A.; Llirós, M.; Oliver, L.; Bahí, A.; Elias-Masiques, N.; Gonzalez, M.; Benejam, P.; Cueva, E.; Termes, M.; Ramió-Pujol, S.; et al. In Vitro Prebiotic Effect of Bread-Making Process in Inflammatory Bowel Disease Microbiome. Front. Microbiol. 2021, 12, 716307. [Google Scholar] [CrossRef]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A Short Screener Is Valid for Assessing Mediterranean Diet Adherence among Older Spanish Men and Women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [PubMed]
- Cantós López, D.; Farran, A.; Palma Linares, I. Programa de Càlcul Nutricional Professional (PCN Pro), version 1.0, Universitat de Barcelona, 2013. Available online: http://www.ub.edu/campusalimentacio/ca/pcnpro/index.htm (accessed on 20 July 2023).
- Molina, L.; Sarmiento, M.; Peñafiel, J.; Donaire, D.; Garcia-Aymerich, J.; Gomez, M.; Ble, M.; Ruiz, S.; Frances, A.; Schröder, H.; et al. Validation of the Regicor Short Physical Activity Questionnaire for the Adult Population. PLoS ONE 2017, 12, e0168148. [Google Scholar] [CrossRef]
- Klindworth, A.; Pruesse, E.; Schweer, T.; Peplies, J.; Quast, C.; Horn, M.; Glöckner, F.O. Evaluation of General 16S Ribosomal RNA Gene PCR Primers for Classical and Next-Generation Sequencing-Based Diversity Studies. Nucleic Acids Res. 2013, 41, e1. [Google Scholar] [CrossRef]
- Bolyen, E.; Rideout, J.R.; Dillon, M.R.; Bokulich, N.A.; Abnet, C.C.; Al-Ghalith, G.A.; Alexander, H.; Alm, E.J.; Arumugam, M.; Asnicar, F.; et al. Reproducible, Interactive, Scalable and Extensible Microbiome Data Science Using QIIME 2. Nat. Biotechnol. 2019, 37, 852–857. [Google Scholar] [CrossRef]
- Callahan, B.J.; McMurdie, P.J.; Rosen, M.J.; Han, A.W.; Johnson, A.J.A.; Holmes, S.P. DADA2: High-Resolution Sample Inference from Illumina Amplicon Data. Nat. Methods 2016, 13, 581–583. [Google Scholar] [CrossRef] [PubMed]
- Katoh, K.; Standley, D.M. MAFFT Multiple Sequence Alignment Software Version 7: Improvements in Performance and Usability. Mol. Biol. Evol. 2013, 30, 772–780. [Google Scholar] [CrossRef] [PubMed]
- Price, M.N.; Dehal, P.S.; Arkin, A.P. FastTree 2—Approximately Maximum-Likelihood Trees for Large Alignments. PLoS ONE 2010, 5, e9490. [Google Scholar] [CrossRef] [PubMed]
- Lozupone, C.; Lladser, M.E.; Knights, D.; Stombaugh, J.; Knight, R. UniFrac: An Effective Distance Metric for Microbial Community Comparison. ISME J. 2011, 5, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Garrity, G.M.; Tiedje, J.M.; Cole, J.R. Naïve Bayesian Classifier for Rapid Assignment of RRNA Sequences into the New Bacterial Taxonomy. Appl. Environ. Microbiol. 2007, 73, 5261–5267. [Google Scholar] [CrossRef] [PubMed]
- Pruesse, E.; Quast, C.; Knittel, K.; Fuchs, B.M.; Ludwig, W.; Peplies, J.; Glöckner, F.O. SILVA: A Comprehensive Online Resource for Quality Checked and Aligned Ribosomal RNA Sequence Data Compatible with ARB. Nucleic Acids Res. 2007, 35, 7188–7196. [Google Scholar] [CrossRef]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-Learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Dinno, A. Exploring the Sensitivity of Horn’s Parallel Analysis to the Distributional Form of Random Data. Multivar. Behav. Res. 2009, 44, 362–388. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing, Version 4.3.1, R Foundation for Statistical Computing, Vienna, 2021. Available online: https://www.R-project.org (accessed on 18 July 2024).
- Zhang, X.; Yi, N. NBZIMM: Negative Binomial and Zero-Inflated Mixed Models, with Application to Microbiome/Metagenomics Data Analysis. BMC Bioinform. 2020, 21, 488. [Google Scholar] [CrossRef]
- Cribari-Neto, F.; Zeileis, A. Beta Regression in R. J. Stat. Softw. 2010, 34, 1–24. [Google Scholar] [CrossRef]
- Silveira Rossi, J.L.; Barbalho, S.M.; Reverete de Araujo, R.; Bechara, M.D.; Sloan, K.P.; Sloan, L.A. Metabolic Syndrome and Cardiovascular Diseases: Going beyond Traditional Risk Factors. Diabetes Metab. Res. Rev. 2022, 38, e3502. [Google Scholar] [CrossRef]
- Pagliai, G.; Venturi, M.; Dinu, M.; Galli, V.; Colombini, B.; Giangrandi, I.; Maggini, N.; Sofi, F.; Granchi, L. Effect of Consumption of Ancient Grain Bread Leavened with Sourdough or with Baker’s Yeast on Cardio-Metabolic Risk Parameters: A Dietary Intervention Trial. Int. J. Food Sci. Nutr. 2021, 72, 367–374. [Google Scholar] [CrossRef]
- Singh, V.; Kaur, R.; Kumari, P.; Pasricha, C.; Singh, R. ICAM-1 and VCAM-1: Gatekeepers in Various Inflammatory and Cardiovascular Disorders. Clinica Chimica Acta 2023, 548, 117487. [Google Scholar] [CrossRef] [PubMed]
- Seidel, C.; Boehm, V.; Vogelsang, H.; Wagner, A.; Persin, C.; Glei, M.; Pool-Zobel, B.L.; Jahreis, G. Influence of Prebiotics and Antioxidants in Bread on the Immune System, Antioxidative Status and Antioxidative Capacity in Male Smokers and Non-Smokers. Br. J. Nutr. 2007, 97, 349–356. [Google Scholar] [CrossRef]
- Chen, C.C.; Chow, M.P.; Huang, W.C.; Lin, Y.C.; Chang, Y.J. Flavonoids Inhibit Tumor Necrosis Factor-α-Induced up-Regulation of Intercellular Adhesion Molecule-1 (ICAM-1) in Respiratory Epithelial Cells through Activator Protein-1 and Nuclear Factor-ΚB: Structure-Activity Relationships. Mol. Pharmacol. 2004, 66, 683–693. [Google Scholar]
- Jahreis, G.; Vogelsang, H.; Kiessling, G.; Schubert, R.; Bunte, C.; Hammes, W.P. Influence of Probiotic Sausage (Lactobacillus paracasei) on Blood Lipids and Immunological Parameters of Healthy Volunteers. Food Res. Int. 2002, 35, 133–138. [Google Scholar] [CrossRef]
- Tjärnlund-Wolf, A.; Brogren, H.; Lo, E.H.; Wang, X. Plasminogen Activator Inhibitor-1 and Thrombotic Cerebrovascular Diseases. Stroke 2012, 43, 2833–2839. [Google Scholar] [CrossRef]
- MacKay, K.A.; Tucker, A.J.; Duncan, A.M.; Graham, T.E.; Robinson, L.E. Whole Grain Wheat Sourdough Bread Does Not Affect Plasminogen Activator Inhibitor-1 in Adults with Normal or Impaired Carbohydrate Metabolism. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Tucker, A.J.; MacKay, K.A.; Robinson, L.E.; Graham, T.E.; Bakovic, M.; Duncan, A.M. The Effect of Whole Grain Wheat Sourdough Bread Consumption on Serum Lipids in Healthy Normoglycemic/Normoinsulinemic and Hyperglycemic/Hyperinsulinemic Adults Depends on Presence of the APOE E3/E3 Genotype: A Randomized Controlled Trial. Nutr. Metab. 2010, 7, 37. [Google Scholar] [CrossRef] [PubMed]
- Gabriele, M.; Arouna, N.; Árvay, J.; Longo, V.; Pucci, L. Sourdough Fermentation Improves the Antioxidant, Antihypertensive, and Anti-Inflammatory Properties of Triticum Dicoccum. Int. J. Mol. Sci. 2023, 24, 6283. [Google Scholar] [CrossRef]
- Ayyash, M.; Johnson, S.K.; Liu, S.Q.; Mesmari, N.; Dahmani, S.; Al Dhaheri, A.S.; Kizhakkayil, J. In Vitro Investigation of Bioactivities of Solid-State Fermented Lupin, Quinoa and Wheat Using Lactobacillus spp. Food Chem. 2019, 275, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Rolim, M.E.; Fortes, M.I.; Von Frankenberg, A.; Duarte, C.K. Consumption of Sourdough Bread and Changes in the Glycemic Control and Satiety: A Systematic Review. Crit. Rev. Food Sci. Nutr. 2022, 64, 801–816. [Google Scholar] [CrossRef] [PubMed]
- Iversen, K.N.; Johansson, D.; Brunius, C.; Andlid, T.; Andersson, R.; Langton, M.; Landberg, R. Appetite and Subsequent Food Intake Were Unaffected by the Amount of Sourdough and Rye in Soft Bread—A Randomized Cross-over Breakfast Study. Nutrients 2018, 10, 1594. [Google Scholar] [CrossRef] [PubMed]
- Darzi, J.; Frost, G.S.; Robertson, M.D. Effects of a Novel Propionate-Rich Sourdough Bread on Appetite and Food Intake. Eur. J. Clin. Nutr. 2012, 66, 789–794. [Google Scholar] [CrossRef]
- Zamaratskaia, G.; Johansson, D.P.; Junqueira, M.A.; Deissler, L.; Langton, M.; Hellström, P.M.; Landberg, R. Impact of Sourdough Fermentation on Appetite and Postprandial Metabolic Responses-A Randomised Cross-over Trial with Whole Grain Rye Crispbread. Br. J. Nutr. 2017, 118, 686–697. [Google Scholar] [CrossRef]
- Najjar, A.M.; Parsons, P.M.; Duncan, A.M.; Robinson, L.E.; Yada, R.Y.; Graham, T.E. The Acute Impact of Ingestion of Breads of Varying Composition on Blood Glucose, Insulin and Incretins Following First and Second Meals. Br. J. Nutr. 2009, 101, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Bo, S.; Seletto, M.; Choc, A.; Ponzo, V.; Lezo, A.; Demagistris, A.; Evangelista, A.; Ciccone, G.; Bertolino, M.; Cassader, M.; et al. The Acute Impact of the Intake of Four Types of Bread on Satiety and Blood Concentrations of Glucose, Insulin, Free Fatty Acids, Triglyceride and Acylated Ghrelin. A Randomized Controlled Cross-over Trial. Food Res. Int. 2017, 92, 40–47. [Google Scholar] [CrossRef]
- Lluansí, A.; Llirós, M.; Carreras-Torres, R.; Bahí, A.; Capdevila, M.; Feliu, A.; Vilà-Quintana, L.; Elias-Masiques, N.; Cueva, E.; Peries, L.; et al. Impact of Bread Diet on Intestinal Dysbiosis and Irritable Bowel Syndrome Symptoms in Quiescent Ulcerative Colitis: A Pilot Study. PLoS ONE 2024, 19, e0297836. [Google Scholar] [CrossRef] [PubMed]
- Korem, T.; Zeevi, D.; Zmora, N.; Weissbrod, O.; Bar, N.; Lotan-Pompan, M.; Avnit-Sagi, T.; Kosower, N.; Malka, G.; Rein, M.; et al. Bread Affects Clinical Parameters and Induces Gut Microbiome-Associated Personal Glycemic Responses. Cell Metab. 2017, 25, 1243–1253. [Google Scholar] [CrossRef]
- Marchandin, H.; Damay, A.; Roudière, L.; Teyssier, C.; Zorgniotti, I.; Dechaud, H.; Jean-Pierre, H.; Jumas-Bilak, E. Phylogeny, Diversity and Host Specialization in the Phylum Synergistetes with Emphasis on Strains and Clones of Human Origin. Res. Microbiol. 2010, 161, 91–100. [Google Scholar] [CrossRef]
- Zeng, M.Y.; Inohara, N.; Nuñez, G. Mechanisms of Inflammation-Driven Bacterial Dysbiosis in the Gut. Mucosal Immunol. 2017, 10, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Konikoff, T.; Gophna, U. Oscillospira: A Central, Enigmatic Component of the Human Gut Microbiota. Trends Microbiol. 2016, 24, 523–524. [Google Scholar] [CrossRef] [PubMed]
- Duan, M.; Wang, Y.; Zhang, Q.; Zou, R.; Guo, M.; Zheng, H. Characteristics of Gut Microbiota in People with Obesity. PLoS ONE 2021, 16, e0255446. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| All | EBLong | EBShort | p Value | |
|---|---|---|---|---|
| n | 31 | 18 | 13 | |
| Age, mean (SD) | 66.7 (5.94) | 66.6 (7.04) | 66.8 (4.36) | 0.954 |
| Sex, Female, n (%) | 16 (51.6%) | 8 (44.4%) | 8 (61.5%) | 0.565 |
| Diabetes, n (%) | 26 (83.9%) | 17 (94.4%) | 9 (69.2%) | 0.134 |
| Hypertension, n (%) | 30 (96.8%) | 18 (100%) | 12 (92.3%) | 0.419 |
| Triglycerides, mg/dL, median [1st–3rd quartile] | 142 [90.5; 174] | 146 [90.0; 168] | 139 [92.0; 175] | 0.889 |
| HDLc, mg/dL, mean (SD) | 49.0 (11.7) | 50.3 (11.8) | 47.2 (11.7) | 0.475 |
| BMI, kg/m2, mean (SD) | 32.8 (3.26) | 34.1 (2.84) | 31.2 (3.13) | 0.015 |
| Scholarity | 0.895 | |||
| Elementary School | 13 (43.3%) | 7 (38.9%) | 6 (50.0%) | |
| Middle school | 9 (30.0%) | 6 (33.3%) | 3 (25.0%) | |
| Higher education | 8 (26.7%) | 5 (27.8%) | 3 (25.0%) | |
| Smoking habit | 0.634 | |||
| Non-smoker | 13 (41.9%) | 9 (50.0%) | 4 (30.8%) | |
| Smoker | 5 (16.1%) | 2 (11.1%) | 3 (23.1%) | |
| Former smoker | 13 (41.9%) | 7 (38.9%) | 6 (46.2%) | |
| Adherence to MedDiet (14 pt), points, mean (SD) | 9.71 (2.18) | 9.83 (2.07) | 9.54 (2.40) | 0.724 |
| Basal intake, kcal, mean (SD) | 1558 (345) | 1552 (387) | 1567 (291) | 0.900 |
| Physical activity, Mets/day, mean (SD) | 2502 (1885) | 2320 (1632) | 2753 (2234) | 0.560 |
| EBLong | EBShort | All | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up | p Value | Baseline | Follow-Up | p Value | Baseline | Follow-Up | p Value | |
| Clinical parameters | |||||||||
| Weight, kg | 92.9 (14.7) | 93.4 (14.3) | 0.710 | 84 (10.2) | 83.5 (9.5) | 0.415 | 89.1 (13.5) | 89.1 (13.2) | 0.462 |
| Waist, cm | 119 (17.3) | 114 (12.5) | 0.237 | 111 (10.3) | 110 (9.18) | 0.796 | 115 (15.1) | 112 (11.2) | 0.223 |
| Systolic pressure, mmHg | 136 (11.3) | 132 (14.5) | 0.470 | 134 (10.1) | 135 (9.91) | 0.395 | 135 (10.7) | 134 (12.6) | 0.830 |
| Diastolic pressure, mmHg | 80.2 (12.2) | 72.5 (10.2) | 0.020 | 77.6 (12.7) | 72.7 (11.3) | 0.208 | 79.1 (12.2) | 72.6 (10.5) | 0.008 |
| Glucose, mg/dL | 125 (30.7) | 128 (33.2) | 0.162 | 117 (23.8) | 117 (21.9) | 0.967 | 122 (27.8) | 124 (29.2) | 0.318 |
| Homa Index | 18.2 (7.97) | 17.3 (7.43) | 0.286 | 21.2 (15.6) | 21 (13.8) | 0.890 | 19.5 (11.7) | 18.8 (10.5) | 0.431 |
| Triglycerides, mg/dL | 146 [90; 168] | 130 [91; 158] | 0.862 | 139 [92; 175] | 124 [84; 179] | 0.839 | 139 [92; 175] | 124 [84; 179] | 0.814 |
| Total cholesterol, mg/dL | 199 (39.5) | 202 (38.6) | 0.378 | 189 (38.9) | 192 (56.3) | 0.707 | 195 (39) | 198 (46.3) | 0.444 |
| HDLc, mg/dL | 50.3 (11.8) | 50.6 (11.7) | 0.736 | 47.2 (11.7) | 48.7 (15.4) | 0.263 | 49 (11.7) | 49.8 (13.1) | 0.282 |
| LDLc, mg/dL | 120 (28.6) | 125 (35.1) | 0.123 | 115 (33.1) | 115 (44.2) | 0.918 | 118 (30.2) | 121 (38.8) | 0.314 |
| Inflammatory biomarkers | |||||||||
| IL6, pg/mL | 2.4 (1.73) | 3.06 (1.93) | 0.106 | 2.5 (1.5) | 2.14 (1.08) | 0.350 | 2.44 (1.62) | 2.67 (1.67) | 0.426 |
| IL8, pg/mL | 4.49 (2.21) | 3.86 (2.02) | 0.116 | 4.63 (2.78) | 4.4 (2.04) | 0.563 | 4.55 (2.42) | 4.09 (2.02) | 0.099 |
| TNF-α, pg/mL | 29.6 (9.59) | 29.9 (11.8) | 0.898 | 40.7 (15.4) | 35.5 (12.4) | 0.032 | 34.2 (13.3) | 32.2 (12.2) | 0.246 |
| PAI-1, pg/mL | 2740 (1070) | 2840 (999) | 0.466 | 2750 (529) | 2330 (773) | 0.018 | 2740 (872) | 2630 (933) | 0.318 |
| sICAM, pg/mL | 179,000 (67,500) | 170,000 (41,800) | 0.325 | 192,000 (59,300) | 160,000 (39,200) | 0.013 | 184,000 (63,500) | 166,000 (40,300) | 0.014 |
| LBP, ng/mL | 15,100 (2630) | 16,500 (4370) | 0.095 | 14,200 (3820) | 13,900 (3690) | 0.761 | 14,700 (3160) | 15,400 (4230) | 0.259 |
| Satiety-related hormones | |||||||||
| Insulin, pg/mL | 423 (201) | 388 (168) | 0.067 | 484 (282) | 490 (287) | 0.797 | 449 (236) | 431 (227) | 0.241 |
| Glucagon, pg/mL | 520 (188) | 493 (177) | 0.143 | 541 (117) | 539 (180) | 0.949 | 529 (160) | 512 (177) | 0.376 |
| GLP-1, pg/mL | 164 (97.8) | 165 (111) | 0.960 | 187 (125) | 223 (122) | 0.191 | 174 (109) | 189 (118) | 0.304 |
| Visfatin, pg/mL | 1910 (1310) | 1730 (1380) | 0.133 | 2030 (1440) | 1990 (1400) | 0.887 | 1960 (1340) | 1840 (1370) | 0.364 |
| Resistin, pg/mL | 4320 (1720) | 4360 (1310) | 0.883 | 6260 (3020) | 5630 (2240) | 0.339 | 5130 (2510) | 4890 (1840) | 0.445 |
| C-peptide, pg/mL | 1100 (423) | 1050 (358) | 0.389 | 1190 (511) | 1190 (613) | 0.940 | 1140 (457) | 1110 (481) | 0.618 |
| Ghrelin, pg/mL | 902 (297) | 904 (274) | 0.952 | 1180 (777) | 1130 (622) | 0.444 | 1020 (558) | 998 (458) | 0.531 |
| Leptin, pg/mL | 8920 (5110) | 8540 (5430) | 0.434 | 9170 (4680) | 9120 (4910) | 0.897 | 9020 (4850) | 8780 (5140) | 0.451 |
| EBLong vs. EBShort | ||||
|---|---|---|---|---|
| Non-Adjusted (Diff. [95% CI]) | p Value | Adjusted (Diff. [95% CI]) | p Value | |
| Clinical parameters | ||||
| Weight, kg | 9.82 [0.47; 19.2] | 0.050 | −0.2 [−2.03; 1.62] | 0.829 |
| Waist, cm | 4.49 [−3.89; 12.9] | 0.303 | −4.46 [−9.22; 0.3] | 0.082 |
| Systolic pressure, mmHg | −3.16 [−12.7; 6.38] | 0.522 | −11.6 [−21.1; −2.12] | 0.026 |
| Diastolic pressure, mmHg | −0.18 [−8.17; 7.81] | 0.966 | −6.43 [−14.6; 1.76] | 0.140 |
| Glucose, mg/dL | 11.3 [−9.48; 32] | 0.296 | 5.71 [−4.76; 16.2] | 0.296 |
| Homa Index | −3.64 [−11.2; 3.9] | 0.352 | 0.31 [−3.05; 3.67] | 0.858 |
| Triglycerides, mg/dL | −9.53 [−53.2; 34.1] | 0.672 | −33.3 [−66.6; −0.086] | 0.062 |
| Total cholesterol, mg/dL | 10.2 [−23.2; 43.5] | 0.554 | −4.44 [−25.3; 16.4] | 0.681 |
| HDLc, mg/dL | 1.87 [−7.65; 11.4] | 0.703 | −1.49 [−4.9; 1.91] | 0.399 |
| LDL cholesterol, mg/dL | 10.2 [−17.7; 38.1] | 0.479 | 2.03 [−16.1; 20.2] | 0.829 |
| Inflammatory biomarkers | ||||
| IL6, pg/mL | 0.92 [−0.25; 2.08] | 0.134 | 1 [−0.17; 2.16] | 0.107 |
| IL8, pg/mL | −0.55 [−1.99; 0.9] | 0.466 | −0.62 [−1.57; 0.34] | 0.219 |
| TNF-α, pg/mL | −5.59 [−14.2; 3] | 0.212 | 3.81 [−3.15; 10.8] | 0.295 |
| PAI-1, pg/mL | 516 [−135; 1170] | 0.131 | 744 [282; 1210] | 0.004 |
| sICAM, pg/mL | 9530 [−19,500; 38,600] | 0.525 | 22,100 [2250; 42,000] | 0.040 |
| LBP, ng/mL | 2520 [−411; 5450] | 0.103 | 1710 [−1210; 4630] | 0.263 |
| Satiety-related hormones | ||||
| Insulin, pg/mL | −102 [−262; 58.8] | 0.224 | −22 [−91.9; 47.9] | 0.543 |
| Glucagon, pg/mL | −46.3 [−173; 80.7] | 0.480 | −2.05 [−96.7; 92.6] | 0.966 |
| GLP-1, pg/mL | −58.6 [−141; 24] | 0.175 | −16.9 [−88.1; 54.2] | 0.646 |
| Visfatin, pg/mL | −258 [−1250; 731] | 0.613 | 19.9 [−626; 665] | 0.952 |
| Resistin, pg/mL | −1270 [−2530; −22.4] | 0.056 | −5.84 [−1190; 1180] | 0.992 |
| C-peptide, pg/mL | −149 [−498; 200] | 0.411 | 50.4 [−205; 306] | 0.703 |
| Ghrelin, pg/mL | −225 [−548; 97.1] | 0.181 | −45.4 [−163; 72.1] | 0.457 |
| Leptin, pg/mL | −584 [−4310; 3140] | 0.761 | −276 [−1920; 1370] | 0.745 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Vega, K.A.; Sanllorente, A.; Zomeño, M.-D.; Quindós, A.; Muñoz-Martínez, J.; Malcampo, M.; Aldea-Perona, A.; Hernáez, Á.; Lluansí, A.; Llirós, M.; et al. Sourdough Bread with Different Fermentation Times: A Randomized Clinical Trial in Subjects with Metabolic Syndrome. Nutrients 2024, 16, 2380. https://doi.org/10.3390/nu16152380
Pérez-Vega KA, Sanllorente A, Zomeño M-D, Quindós A, Muñoz-Martínez J, Malcampo M, Aldea-Perona A, Hernáez Á, Lluansí A, Llirós M, et al. Sourdough Bread with Different Fermentation Times: A Randomized Clinical Trial in Subjects with Metabolic Syndrome. Nutrients. 2024; 16(15):2380. https://doi.org/10.3390/nu16152380
Chicago/Turabian StylePérez-Vega, Karla Alejandra, Albert Sanllorente, María-Dolores Zomeño, Ana Quindós, Júlia Muñoz-Martínez, Mireia Malcampo, Ana Aldea-Perona, Álvaro Hernáez, Aleix Lluansí, Marc Llirós, and et al. 2024. "Sourdough Bread with Different Fermentation Times: A Randomized Clinical Trial in Subjects with Metabolic Syndrome" Nutrients 16, no. 15: 2380. https://doi.org/10.3390/nu16152380
APA StylePérez-Vega, K. A., Sanllorente, A., Zomeño, M.-D., Quindós, A., Muñoz-Martínez, J., Malcampo, M., Aldea-Perona, A., Hernáez, Á., Lluansí, A., Llirós, M., Elias, I., Elias-Masiques, N., Aldeguer, X., Muñoz, D., Gaixas, S., Blanchart, G., Schröder, H., Hernando-Redondo, J., Carrón, N., ... Castañer, O. (2024). Sourdough Bread with Different Fermentation Times: A Randomized Clinical Trial in Subjects with Metabolic Syndrome. Nutrients, 16(15), 2380. https://doi.org/10.3390/nu16152380