
Gluten-Free Diet Adherence Tools for Individuals with Celiac Disease: A Systematic Review and Meta-Analysis of Tools Compared to Laboratory Tests
 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Eligibility Criteria
2.3. Search and Data Extraction Strategy
2.4. Reference and Selection Manager
2.5. Data Collection and Risk of Bias Analysis
2.6. Statistical Analysis and Meta-Analysis
3. Results
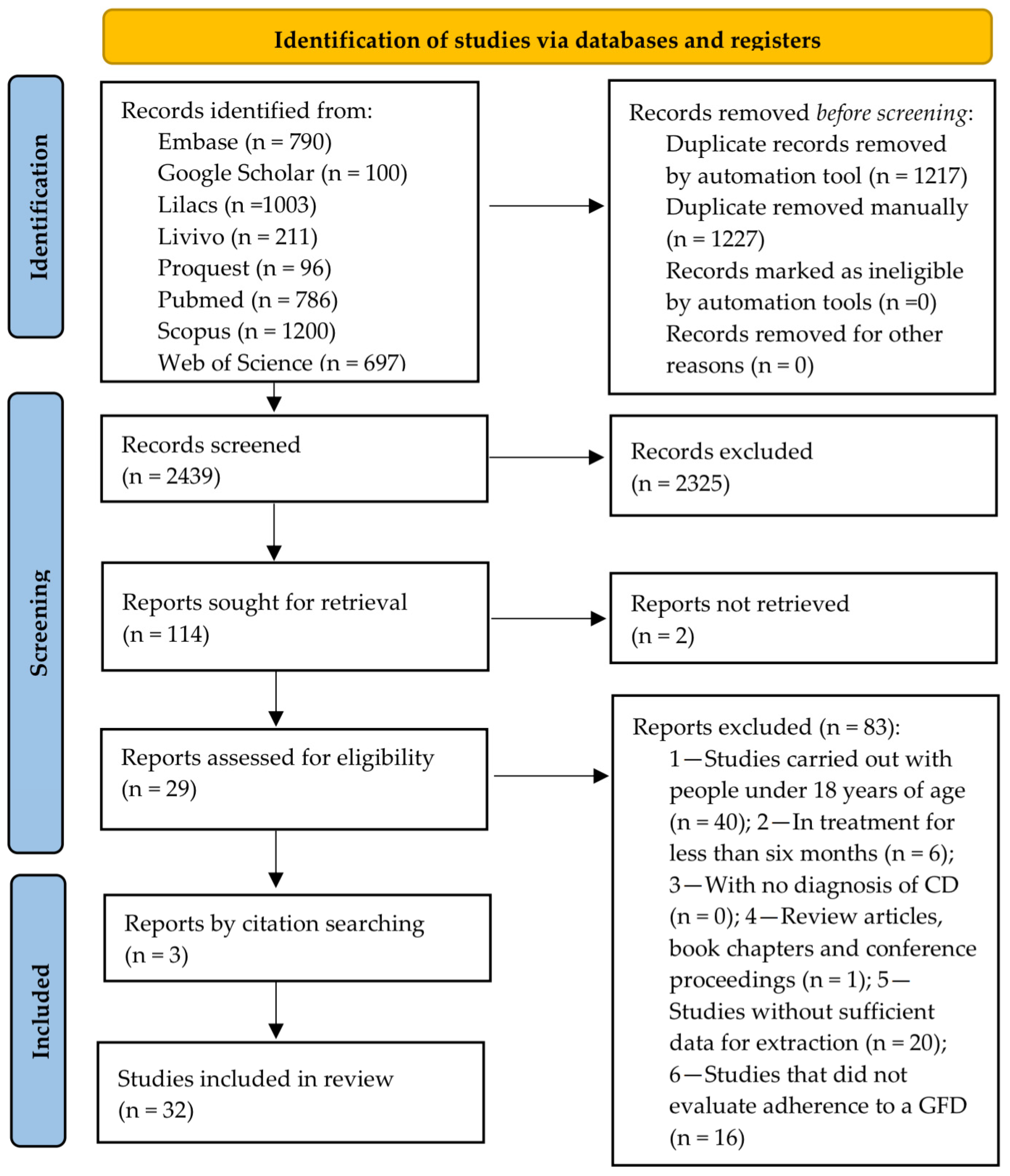
3.1. Study Selection
3.2. The Studies’ Characteristics
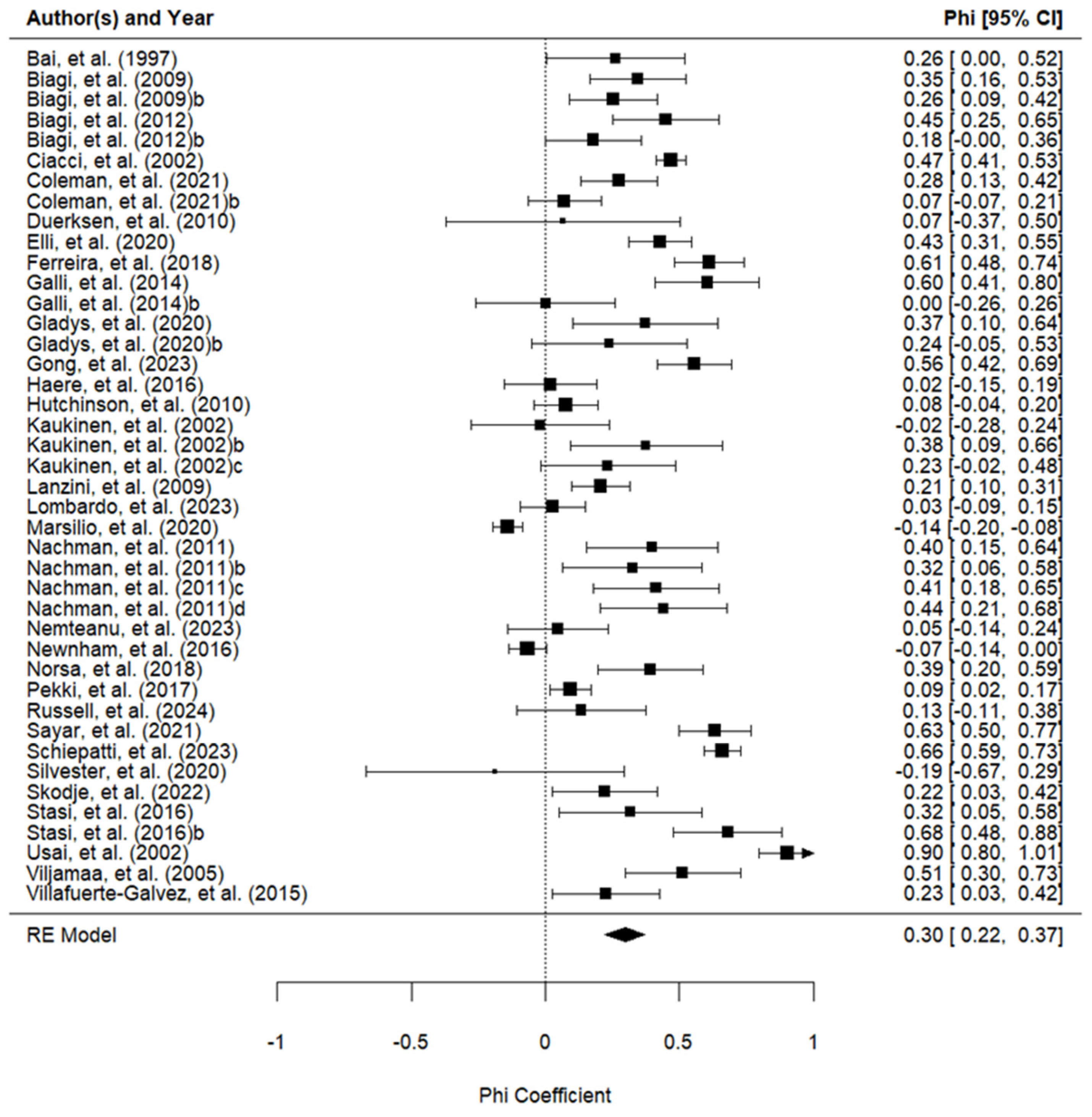
3.3. Meta-Analysis
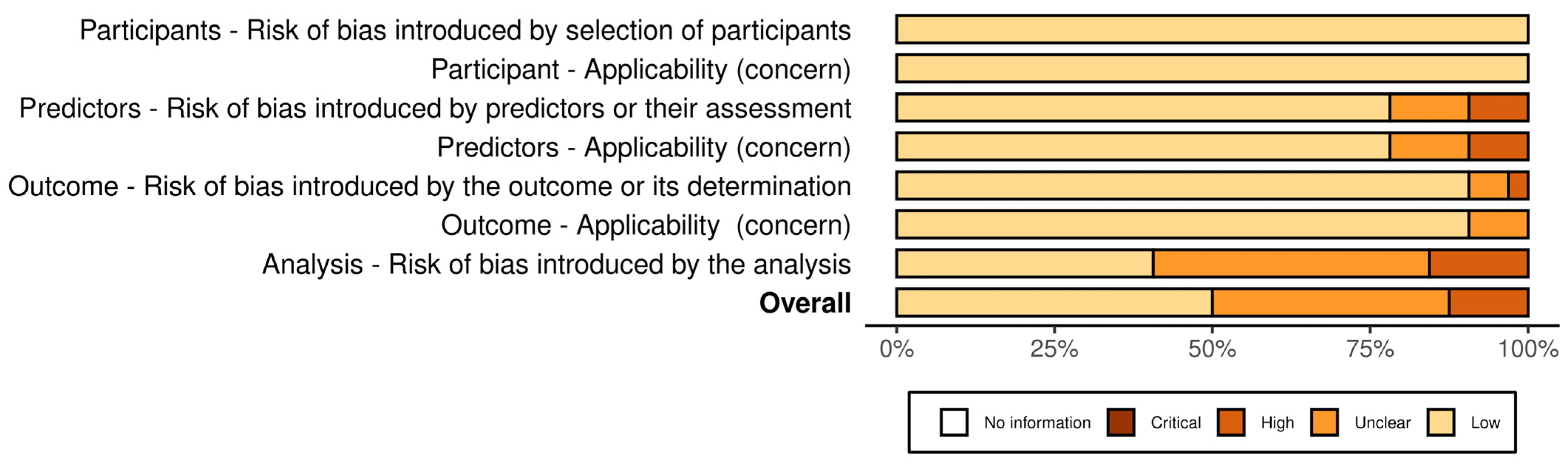
3.4. Risk of Bias and Concern
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Al-Toma, A.; Volta, U.; Auricchio, R.; Castillejo, G.; Sanders, D.S.; Cellier, C.; Mulder, C.J.; Lundin, K.E.A. European Society for the Study of Coeliac Disease (ESsCD) Guideline for Coeliac Disease and Other Gluten-Related Disorders. United Eur. Gastroenterol. J. 2019, 7, 583–613. [Google Scholar] [CrossRef] [PubMed]
- Fasano, A.; Catassi, C. Celiac Disease. N. Engl. J. Med. 2012, 367, 2419–2426. [Google Scholar] [CrossRef] [PubMed]
- Itzlinger, A.; Branchi, F.; Elli, L.; Schumann, M. Gluten-Free Diet in Celiac Disease—Forever and for All? Nutrients 2018, 10, 1796. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Leffler, D.A.; Bai, J.C.; Biagi, F.; Fasano, A.; Green, P.H.R.; Hadjivassiliou, M.; Kaukinen, K.; Kelly, C.P.; Leonard, J.N.; et al. The Oslo Definitions for Coeliac Disease and Related Terms. Gut 2013, 62, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Sahin, Y. Celiac Disease in Children: A Review of the Literature. World J. Clin. Pediatr. 2021, 10, 53–71. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Arora, A.; Strand, T.A.; Leffler, D.A.; Catassi, C.; Green, P.H.; Kelly, C.P.; Ahuja, V.; Makharia, G.K. Global Prevalence of Celiac Disease: Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2018, 16, 823–836. [Google Scholar] [CrossRef] [PubMed]
- Taraghikhah, N.; Ashtari, S.; Asri, N.; Shahbazkhani, B.; Al-Dulaimi, D.; Rostami-Nejad, M.; Rezaei-Tavirani, M.; Razzaghi, M.R.; Zali, M.R. An Updated Overview of Spectrum of Gluten-Related Disorders: Clinical and Diagnostic Aspects. BMC Gastroenterol. 2020, 20, 258. [Google Scholar] [CrossRef]
- Bernardo, D.; Peña, A.S. Developing Strategies to Improve the Quality of Life of Patients with Gluten Intolerance in Patients with and without Coeliac Disease. Eur. J. Intern. Med. 2012, 23, 6–8. [Google Scholar] [CrossRef] [PubMed]
- Galli, G.; Esposito, G.; Lahner, E.; Pilozzi, E.; Corleto, V.D.; Di Giulio, E.; Aloe Spiriti, M.A.; Annibale, B. Histological Recovery and Gluten-Free Diet Adherence: A Prospective 1-Year Follow-up Study of Adult Patients with Coeliac Disease. Aliment. Pharmacol. Ther. 2014, 40, 639–647. [Google Scholar] [CrossRef]
- Wieser, H.; Ruiz-Carnicer, Á.; Segura, V.; Comino, I.; Sousa, C. Challenges of Monitoring the Gluten-Free Diet Adherence in the Management and Follow-Up of Patients with Celiac Disease. Nutrients 2021, 13, 2274. [Google Scholar] [CrossRef]
- Elli, L.; Leffler, D.; Cellier, C.; Lebwohl, B.; Ciacci, C.; Schumann, M.; Lundin, K.E.A.; Chetcuti Zammit, S.; Sidhu, R.; Roncoroni, L.; et al. Guidelines for Best Practices in Monitoring Established Coeliac Disease in Adult Patients. Nat. Rev. Gastroenterol. Hepatol. 2024, 21, 198–215. [Google Scholar] [CrossRef] [PubMed]
- Villafuerte-Galvez, J.; Vanga, R.R.; Dennis, M.; Hansen, J.; Leffler, D.A.; Kelly, C.P.; Mukherjee, R. Factors Governing Long-Term Adherence to a Gluten-Free Diet in Adult Patients with Coeliac Disease. Aliment. Pharmacol. Ther. 2015, 42, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Fernández Miaja, M.; José, J.; Martín, D.; Treviño, S.J.; Suárez González, M.; Bousoño García, C. Study of Adherence to the Gluten-Free Diet in Coeliac Patients. An. Pediatría 2021, 94, 377–384. [Google Scholar] [CrossRef]
- Paganizza, S.; Zanotti, R.; D’Odorico, A.; Scapolo, P.; Canova, C. Is Adherence to a Gluten-Free Diet by Adult Patients with Celiac Disease Influenced by Their Knowledge of the Gluten Content of Foods? Gastroenterol. Nurs. 2019, 42, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, H.; Reeves, S.; Jeanes, Y.M. Identifying and Improving Adherence to the Gluten-Free Diet in People with Coeliac Disease. Proc. Nutr. Soc. 2019, 78, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Silvester, J.A.; Kurada, S.; Szwajcer, A.; Kelly, C.P.; Leffer, D.A.; Duerksen, D. Tests for Serum Transglutaminase and Endomysial Antibodies Do Not Detect Most Patients With Celiac Disease and Persistent Villous Atrophy on Gluten-Free Diets: A Meta-Analysis. Gastroenterology 2017, 153, 689–701. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, L.; Pérez-Martinez, I.; Lauret-Braña, E.; Suárez-González, A. Descriptive Study of the Diffe:.Rent Tools Used to Evaluate the Adherence to a Gluten-Free Diet in Celiac Disease Patients. Nutrients 2018, 10, 1777. [Google Scholar] [CrossRef] [PubMed]
- Biagi, F.; Bianchi, P.I.; Marchese, A.; Trotta, L.; Vattiato, C.; Balduzzi, D.; Brusco, G.; Andrealli, A.; Cisarò, F.; Astegiano, M.; et al. A Score That Verifies Adherence to a Gluten-Free Diet: A Cross-Sectional, Multicentre Validation in Real Clinical Life. Br. J. Nutr. 2012, 108, 1884–1888. [Google Scholar] [CrossRef] [PubMed]
- Leffler, D.A.; Dennis, M.; Edwards George, J.B.; Jamma, S.; Magge, S.; Cook, E.F.; Schuppan, D.; Kelly, C.P. A Simple Validated Gluten-Free Diet Adherence Survey for Adults With Celiac Disease. Clin. Gastroenterol. Hepatol. 2009, 7, 530–536. [Google Scholar] [CrossRef]
- Gładyś, K.; Dardzińska, J.; Guzek, M.; Adrych, K.; Małgorzewicz, S. Celiac Dietary Adherence Test and Standardized Dietician Evaluation in Assessment of Adherence to a Gluten-Free Diet in Patients with Celiac Disease. Nutrients 2020, 12, 2300. [Google Scholar] [CrossRef]
- Snell, K.I.E.; Levis, B.; Damen, J.A.A.; Dhiman, P.; Debray, T.P.A.; Hooft, L.; Reitsma, J.B.; Moons, K.G.M.; Collins, G.S.; Riley, R.D. Transparent Reporting of Multivariable Prediction Models for Individual Prognosis or Diagnosis: Checklist for Systematic Reviews and Meta-Analyses (TRIPOD-SRMA). BMJ 2023, 381, e073538. [Google Scholar] [CrossRef]
- Moons, K.G.M.; de Groot, J.A.H.; Bouwmeester, W.; Vergouwe, Y.; Mallett, S.; Altman, D.G.; Reitsma, J.B.; Collins, G.S. Critical Appraisal and Data Extraction for Systematic Reviews of Prediction Modelling Studies: The CHARMS Checklist. PLoS Med. 2014, 11, e1001744. [Google Scholar] [CrossRef]
- Wolff, R.F.; Moons, K.G.M.; Riley, R.D.; Whiting, P.F.; Westwood, M.; Collins, G.S.; Reitsma, J.B.; Kleijnen, J.; Mallett, S. PROBAST: A Tool to Assess the Risk of Bias and Applicability of Prediction Model Studies. Ann. Intern. Med. 2019, 170, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Felix, B.M.; López-Alcalde, J.; Roqué, M.; Muriel, A.; Zamora, J. CHARMS and PROBAST at Your Fingertips: A Template for Data Extraction and Risk of Bias Assessment in Systematic Reviews of Predictive Models. BMC Med. Res. Methodol. 2023, 23, 44. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018; Available online: https://www.R-project.org/ (accessed on 14 June 2024).
- Biagi, F.; Andrealli, A.; Bianchi, P.I.; Marchese, A.; Klersy, C.; Corazza, G.R. A Gluten-Free Diet Score to Evaluate Dietary Compliance in Patients with Coeliac Disease. Br. J. Nutr. 2009, 102, 882–887. [Google Scholar] [CrossRef]
- Norsa, L.; Branchi, F.; Bravo, M.; Ferretti, F.; Roncoroni, L.; Somalvico, F.; Conte, D.; Bardella, M.T.; Barigelletti, G.; Elli, L. Celiac Disease 30 Years after Diagnosis: Struggling with Gluten-Free Adherence or Gaining Gluten Tolerance? J. Pediatr. Gastroenterol. Nutr. 2018, 67, 361–366. [Google Scholar] [CrossRef]
- Schiepatti, A.; Maimaris, S.; Raju, S.A.; Green, O.L.; Linden, J.; Mantica, G.; Therrien, A.; Flores-, D.; Bañares, F.F.-; Esteve, M.; et al. Persistent Villous Atrophy Predicts Development of Complications and Mortality in Adult Patients with Coeliac Disease: A Multicentre Longitudinal Cohort Study and Development of a Score to Identify High-Risk Patients. Gut 2023, 72, 2095–2102. [Google Scholar] [CrossRef] [PubMed]
- Stasi, E.; Marafini, I.; Caruso, R.; Soderino, F.; Angelucci, E.; Del Vecchio Blanco, G.; Paoluzi, O.A.; Calabrese, E.; Sedda, S.; Zorzi, F.; et al. Frequency and Cause of Persistent Symptoms in Celiac Disease Patients on a Long-Term Gluten-Free Diet. J. Clin. Gastroenterol. 2016, 50, 239–243. [Google Scholar] [CrossRef]
- Usai, P.; Minerba, L.; Marini, B.; Cossu, R.; Spada, S.; Carpiniello, B.; Cuomo, R.; Boy, M.F. Case Control Study on Health-Related Quality of Life in Adult Coeliac Disease. Dig. Liver Dis. 2002, 34, 547–552. [Google Scholar] [CrossRef]
- Ciacci, C.; Cirillo, M.; Cavallaro, R.; Mazzacca, G. Long-Term Follow-up of Celiac Adults on Gluten-Free Diet: Prevalence and Correlates of Intestinal Damage. Digestion 2002, 66, 178–185. [Google Scholar] [CrossRef]
- Elli, L.; Bascuñán, K.; Di Lernia, L.; Bardella, M.T.; Doneda, L.; Soldati, L.; Orlando, S.; Ferretti, F.; Lombardo, V.; Barigelletti, G.; et al. Safety of Occasional Ingestion of Gluten in Patients with Celiac Disease: A Real-Life Study. BMC Med. 2020, 18, 42. [Google Scholar] [CrossRef] [PubMed]
- Lanzini, A.; Lanzarotto, F.; Villanacci, V.; Mora, A.; Bertolazzi, S.; Turini, D.; Carella, G.; Malagoli, A.; Ferrante, G.; Cesana, B.M.; et al. Complete Recovery of Intestinal Mucosa Occurs Very Rarely in Adult Coeliac Patients despite Adherence to Gluten-Free Diet. Aliment. Pharmacol. Ther. 2009, 29, 1299–1308. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, V.; Scricciolo, A.; Costantino, A.; Elli, L.; Legnani, G.; Cebolla, Á.; Doneda, L.; Mascaretti, F.; Vecchi, M.; Roncoroni, L. Evaluation of a Single Determination of Gluten Immunogenic Peptides in Urine from Unaware Celiac Patients to Monitor Gluten-Free Diet Adherence. Nutrients 2023, 15, 1259. [Google Scholar] [CrossRef] [PubMed]
- Marsilio, I.; Canova, C.; D’odorico, A.; Ghisa, M.; Zingone, L.; Lorenzon, G.; Savarino, E.V.; Zingone, F. Quality-of-Life Evaluation in Coeliac Patients on a Gluten-Free Diet. Nutrients 2020, 12, 2981. [Google Scholar] [CrossRef]
- Kaukinen, K.; Sulkanen, S.; Mäki, M.; Collin, P. IgA-Class Transglutaminase Antibodies in Evaluating the Efficacy of Gluten-Free Diet in Coeliac Disease. Eur. J. Gastroenterol. Hepatol. 2002, 14, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Metso, S.; Hyytiä-Ilmonen, H.; Kaukinen, K.; Huhtala, H.; Jaatinen, P.; Salmi, J.; Taurio, J.; Collin, P. Gluten-Free Diet and Autoimmune Thyroiditis in Patients with Celiac Disease. A Prospective Controlled Study. Scand. J. Gastroenterol. 2012, 47, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Pekki, H.; Kurppa, K.; Mäki, M.; Huhtala, H.; Laurila, K.; Ilus, T.; Kaukinen, K. Performing Routine Follow-up Biopsy 1 Year after Diagnosis Does Not Affect Long-Term Outcomes in Coeliac Disease. Aliment. Pharmacol. Ther. 2017, 45, 1459–1468. [Google Scholar] [CrossRef] [PubMed]
- Viljamaa, M.; Collin, P.; Huhtala, H.; Sievänen, H.; Mäki, M.; Kaukinen, K. Is Coeliac Disease Screening in Risk Groups Justified? A Fourteen-Year Follow-up with Special Focus on Compliance and Quality of Life. Aliment. Pharmacol. Ther. 2005, 22, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Coleman, S.H.; Rej, A.; Baggus, E.M.R.; Lau, M.S.; Marks, L.J.; Hadjivassiliou, M.; Cross, S.S.; Leffler, D.A.; Elli, L.; Sanders, D.S. What Is the Optimal Method Assessing for Persistent Villous Atrophy in Adult Coeliac Disease? J. Gastrointest. Liver Dis. 2021, 30, 205–212. [Google Scholar] [CrossRef]
- Hutchinson, J.M.; West, N.P.; Robins, G.G.; Howdle, P.D. Long-Term Histological Follow-up of People with Coeliac Disease in a UK Teaching Hospital. QJM Int. J. Med. 2010, 103, 511–517. [Google Scholar] [CrossRef]
- Gong, C.; Saborit, C.; Long, X.; Wang, A.; Zheng, B.; Chung, H.; Lewis, S.K.; Krishnareddy, S.; Bhagat, G.; Green, P.H.R.; et al. Serological Investigation of Persistent Villous Atrophy in Celiac Disease. Clin. Transl. Gastroenterol. 2023, 14, e00639. [Google Scholar] [CrossRef]
- Bai, J.C.; Gonzalez, D.; Mautalen, C.; Mazure, R.; Pedreira, S.; Vazquez, H.; Smecuol, E.; Siccardi, A.; Cataldi, M.; Niveloni, S.; et al. Long-Term Effect of Gluten Restriction on Bone Mineral Density of Patients with Coeliac Disease. Aliment. Pharmacol. Ther. 1997, 11, 157–164. [Google Scholar] [CrossRef]
- Nachman, F.; Sugai, E.; Vázquez, H.; González, A.; Andrenacci, P.; Niveloni, S.; Mazure, R.; Smecuol, E.; Moreno, M.L.; Hwang, H.J.; et al. Serological Tests for Celiac Disease as Indicators of Long-Term Compliance with the Gluten-Free Diet. Eur. J. Gastroenterol. Hepatol. 2011, 23, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Newnham, E.D.; Shepherd, S.J.; Strauss, B.J.; Hosking, P.; Gibson, P.R. Adherence to the Gluten-Free Diet Can Achieve the Therapeutic Goals in Almost All Patients with Coeliac Disease: A 5-Year Longitudinal Study from Diagnosis. J. Gastroenterol. Hepatol. 2016, 31, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Russell, A.K.; Lucas, E.C.; Henneken, L.M.; Pizzey, C.J.; Clarke, D.; Myleus, A.; Tye-Din, J.A. Stool Gluten Peptide Detection Is Superior to Urinary Analysis, Coeliac Serology, Dietary Adherence Scores and Symptoms in the Detection of Intermittent Gluten Exposure in Coeliac Disease: A Randomised, Placebo-Controlled, Low-Dose Gluten Challenge Study. Nutrients 2024, 16, 279. [Google Scholar] [CrossRef] [PubMed]
- Duerksen, D.R.; Wilhelm-Boyles, C.; Veitch, R.; Kryszak, D.; Parry, D.M. A Comparison of Antibody Testing, Permeability Testing, and Zonulin Levels with Small-Bowel Biopsy in Celiac Disease Patients on a Gluten-Free Diet. Dig. Dis. Sci. 2010, 55, 1026–1031. [Google Scholar] [CrossRef] [PubMed]
- Silvester, J.A.; Comino, I.; Kelly, C.P.; Sousa, C.; Duerksen, D.R. Most Patients With Celiac Disease on Gluten-Free Diets Consume Measurable Amounts of Gluten. Gastroenterology 2020, 158, 1497–1499. [Google Scholar] [CrossRef] [PubMed]
- Hære, P.; Høie, O.; Schulz, T.; Schönhardt, I.; Raki, M.; Lundin, K.E.A. Long-Term Mucosal Recovery and Healing in Celiac Disease Is the Rule—Not the Exception. Scand. J. Gastroenterol. 2016, 51, 1439–1446. [Google Scholar] [CrossRef]
- Skodje, G.I.; van Megen, F.; Stendahl, M.; Henriksen, C.; Lundin, K.E.A.; Veierød, M.B. Detection of Gluten Immunogenic Peptides and the Celiac Disease Adherence Test to Monitor Gluten-Free Diet: A Pilot Study. Eur. J. Clin. Nutr. 2022, 76, 902–903. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, S.; Chamorro, M.E.; Ortíz, J.; Carpinelli, M.M.; Giménez, V.; Langjahr, P. Anti-Transglutaminase Antibody in Adults with Celiac Disease and Their Relation to the Presence and Duration of Gluten-Free Diet. Rev. Gastroenterol. Peru 2018, 38, 228–233. [Google Scholar]
- Nemteanu, R.; Danciu, M.; Girleanu, I.; Ciortescu, I.; Gheorghe, L.; Trifan, A.; Plesa, A. Predictors of Slow Responsiveness and Partial Mucosal Recovery in Adult Patients with Celiac Disease. Gastroenterol. Hepatol. Bed Bench 2023, 16, 194–202. [Google Scholar] [PubMed]
- Sayar, S.; Aykut, H.; Kaya, Ö.; Kürbüz, K.; Ak, Ç.; Gökçen, P.; Bilgiç, N.M.; Adalı, G.; Kahraman, R.; Doganay, L.; et al. Bone Mineral Density Screening and the Frequency of Osteopenia/Osteoporosis in Turkish Adult Patients with Celiac Disease. Turk. J. Gastroenterol. 2021, 32, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Schiepatti, A.; Maimaris, S.; Lusetti, F.; Scalvini, D.; Minerba, P.; Cincotta, M.; Fazzino, E.; Biagi, F. High Prevalence of Functional Gastrointestinal Disorders in Celiac Patients with Persistent Symptoms on a Gluten-Free Diet: A 20-Year Follow-Up Study. Dig. Dis. Sci. 2023, 68, 3374–3382. [Google Scholar] [CrossRef] [PubMed]
- Lionetti, E.; Pjetraj, D.; Gatti, S.; Catassi, G.; Bellantoni, A.; Boffardi, M.; Cananzi, M.; Cinquetti, M.; Francavilla, R.; Malamisura, B.; et al. Prevalence and Detection Rate of Celiac Disease in Italy: Results of a SIGENP Multicenter Screening in School-Age Children. Dig. Liver Dis. 2023, 55, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Volta, U.; Bellentani, S.; Bianchi, F.B.; Brandi, G.; De Franceschi, L.; Miglioli, L.; Granito, A.; Balli, F.; Tiribelli, C. High Prevalence of Celiac Disease in Italian General Population. Dig. Dis. Sci. 2001, 46, 1500–1505. [Google Scholar] [CrossRef] [PubMed]
- Barone, M.; Della Valle, N.; Rosania, R.; Facciorusso, A.; Trotta, A.; Cantatore, F.P.; Falco, S.; Pignatiello, S.; Viggiani, M.T.; Amoruso, A.; et al. A Comparison of the Nutritional Status between Adult Celiac Patients on a Long-Term, Strictly Gluten-Free Diet and Healthy Subjects. Eur. J. Clin. Nutr. 2016, 70, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Atsawarungruangkit, A.; Silvester, J.A.; Weiten, D.; Green, K.L.; Wilkey, K.E.; Rigaux, L.N.; Bernstein, C.N.; Graff, L.A.; Walker, J.R.; Duerksen, D.R. Development of the Dietitian Integrated Evaluation Tool for Gluten-Free Diets (DIET-GFD). Nutrition 2020, 78, 110819. [Google Scholar] [CrossRef] [PubMed]
- Silvester, J.A.; Weiten, D.; Graff, L.A.; Walker, J.R.; Duerksen, D.R. Is It Gluten-Free? Relationship between Self-Reported Gluten-Free Diet Adherence and Knowledge of Gluten Content of Foods. Nutrition 2016, 32, 777–783. [Google Scholar] [CrossRef]
- Leffler, D.A.; George, J.B.E.; Dennis, M.; Cook, E.F.; Schuppan, D.; Kelly, C.P. A Prospective Comparative Study of Five Measures of Gluten-Free Diet Adherence in Adults with Coeliac Disease. Aliment. Pharmacol. Ther. 2007, 26, 1227–1235. [Google Scholar] [CrossRef]
- De Moreno, M.L.; Rodríguez-Herrera, A.; Sousa, C.; Comino, I. Biomarkers to Monitor Gluten-Free Diet Compliance in Celiac Patients. Nutrients 2017, 9, 46. [Google Scholar] [CrossRef]
- Sbravati, F.; Pagano, S.; Retetangos, C.; Spisni, E.; Bolasco, G.; Labriola, F.; Filardi, M.C.; Grondona, A.G.; Alvisi, P. Adherence to Gluten-Free Diet in a Celiac Pediatric Population Referred to the General Pediatrician After Remission. J. Pediatr. Gastroenterol. Nutr. 2020, 71, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Fueyo Díaz, R.; Santos, S.G.; Asensio Martínez, Á.; Antonia, M.; Calavera, S.; Magallón Botaya, R.; Díaz, F.; Santos, G.; Martínez, A.; Sánchez Cala-Vera, M.A.; et al. Adaptación Transcultural y Validación Del Celiac Dietary Adherence Test. Un Cuestionario Sencillo Para Determinar La Adherencia a La Dieta Sin Gluten. Rev. Esp. Enfermedades Dig. 2016, 108, 138–144. [Google Scholar]
- Johansson, K.; Norström, F.; Nordyke, K.; Myleus, A. Celiac Dietary Adherence Test Simplifies Determining Adherence to a Gluten-Free Diet in Swedish Adolescents. J. Pediatr. Gastroenterol. Nutr. 2019, 69, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Tapia, A.; Hill, I.D.; Semrad, C.; Ciar, C.; Kelly, C.P.; Lebwohl, B. American College of Gastroenterology Guidelines Update: Diagnosis and Management of Celiac Disease. Am. J. Gastroenterol. 2023, 118, 59–76. [Google Scholar] [CrossRef]
- Raiteri, A.; Granito, A.; Giamperoli, A.; Catenaro, T.; Negrini, G.; Tovoli, F. Current Guidelines for the Management of Celiac Disease: A Systematic Review with Comparative Analysis. World J. Gastroenterol. 2022, 28, 154–175. [Google Scholar] [CrossRef] [PubMed]
- Leffler, D.A.; Schuppan, D. Update on Serologic Testing in Celiac Disease. Am. J. Gastroenterol. 2010, 105, 2520–2524. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Bai, J.C.; Biagi, F.; Card, T.R.; Ciacci, C.; Ciclitira, P.J.; Green, P.H.R.; Hadjivassiliou, M.; Holdoway, A.; Van Heel, D.A.; et al. Diagnosis and Management of Adult Coeliac Disease: Guidelines from the British Society of Gastroenterology. Gut 2014, 63, 1210–1228. [Google Scholar] [CrossRef] [PubMed]
- Comino, I.; Fernández-Bañares, F.; Esteve, M.; Ortigosa, L.; Castillejo, G.; Fambuena, B.; Ribes-Koninckx, C.; Sierra, C.; Rodríguez-Herrera, A.; Salazar, J.C.; et al. Fecal Gluten Peptides Reveal Limitations of Serological Tests and Food Questionnaires for Monitoring Gluten-Free Diet in Celiac Disease Patients. Am. J. Gastroenterol. 2016, 111, 1456–1465. [Google Scholar] [CrossRef]
- Monachesi, C.; Verma, A.K.; Catassi, G.N.; Franceschini, E.; Gatti, S.; Gesuita, R.; Lionetti, E.; Catassi, C. Determination of Urinary Gluten Immunogenic Peptides to Assess Adherence to the Gluten-Free Diet: A Randomized, Double-Blind, Controlled Study. Clin. Transl. Gastroenterol. 2021, 12, E00411. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Study Design | Enrolment Period | Country | n | Females (n) | Age | GFD Period (Month) | GFD Adherence Tool | %Adherence Using the Tool | Laboratory Test | %Adherence Using the Laboratory Test |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Biagi et al., 2009 [26] | Cohort | NI | Italy | 168 | 126 | 42.4 ± 13.9 | 82 (15–389) | BIAGI | 79.7 | Biopsy | 91 |
| 162 | NI | EMA | 70.3 | ||||||||
| Biagi et al., 2012 [18] | Cohort | 2008–2011 | Italy | 141 | 108 | 34 ± 15 | 27 (6–298) | BIAGI | 82.2 | Biopsy | 85.8 |
| EMA | 73 | ||||||||||
| Galli et al., 2014 [31] | Cohort | 2009–2012 | Italy | 65 | 47 | 38 (18–70) | 12 | BIAGI | 81.5 | Biopsy | 67.6 |
| 57 | NI | EMA/tTG | 70 | ||||||||
| Marsilio et al., 2020 [33] | Cohort | 2020 | Italy | 100 | 86 | 39.73 ± 13.51 | 79.68 ± 76.68 | BIAGI | 90 | tTG | 85 |
| Coleman et al., 2021 [40] | Cohort | 2013–2019 | UK | 201 | 136 | 50.3 | >30 | BIAGI | 91 | Biopsy | 68.6 |
| Villafuerte-Galvez et al., 2015 [12] | Cohort | 2011–2012 | USA | 118 | NI | 53.6 ±1 15.4 | 118.8 ± 76.8 | CDAT | 73.7 | tTG | 82 |
| Haere et al., 2016 [49] | Cohort | NI | Norway | 127 | 79 | 55 ± 14 | 111.6 ± 60 | CDAT | 46.4 | Biopsy | 94.4 |
| Gladys et al., 2020 [20] | Cohort | 2015–2018 | Poland | 44 | 38 | 40.8 | 78 ± 86.4 | CDAT | 47.7 | Biopsy | 56.8 |
| Silvester et al., 2020 [48] | Cohort | NI | Canada | 18 | 12 | 41 (21–77) | 24 | CDAT | 77.7 | uGIPs fGIPs | 33.3 |
| Coleman et al., 2021 [40] | Cohort | 2013–2019 | England | 201 | 136 | 50.3 | >30 | CDAT | 49.7 | Biopsy | 68.6 |
| Skodje et al., 2022 [50] | Cohort | NI | Norway | 70 | 59 | 45 | 12 | CDAT | 53 | fGIPs | 91.4 |
| Lombardo et al., 2023 [9] | Cohort | 2019–2020 | Italy | 280 | 232 | 42.9 | 133.2 ± 122.4 | CDAT | 69.2 | uGIPs | 88.5 |
| Russell et al., 2024 [46] | RCT | 2020–2021 | Australia | 51 | 36 | 55 (44–62) | 120 (60–168) | CDAT | 72.5 | fGIPs | 23.5 |
| Schiepatti et al., 2023 [35] | Cohort | 2020–2022 | Italy, Spain, UK, USA | 694 | 491 | >18 | 32 (15–61) | CDAT/BIAGI | 83.5 | Biopsy | 77.3 |
| Ciacci et al., 2002 [29] | Cohort | 2002 | Italy | 390 | 299 | 27.9 ± 10.9 | 82.8 ± 90 | Interview | 42.5 | Biopsy | 76 |
| Usai et al., 2002 [28] | Cohort | 2002 | Italy | 66 | 66 | 46 (18–74) | >24 | Interview | 59 | EMA/AGA | 57.5 |
| Metso et al., 2012 [37] | Cohort | 2003–2006 | Finland | 26 | 22 | >45 | >12 meses | Interview | 92.3 | Biopsy | 100 |
| Gong et al., 2023 [42] | Cohort | 2008–2019 | USA | 106 | 66 | 43.9 | 84 | Interview | 74.5 | Biopsy | 54.7 |
| Gladys et al., 2020 [20] | Cohort | 2020 | Italy | 44 | 38 | 40.8 | 78 ± 86.4 | SDE | 75 | Biopsy | 56.8 |
| Bai et al., 1997 [43] | Cohort | 1997 | Argentina | 22 | NI | 44 (21–73) | 47 (23–75) | Self-reported | 59 | EMA/tTG | 95.4 |
| Kaukinen et al., 2002 [36] | Cohort | 2002 | Finland | 57 | NI | 49 (22–73) | 12 (12–216) | Self-reported | 80.7 | Biopsy | 52.6 |
| 87 | 63 | 87.3 | EMA | 87.3 | |||||||
| 87 | 63 | 87.3 | tTG | 73.3 | |||||||
| Viljamaa et al., 2005 [39] | Cohort | NI | Finland | 97 | 51 | 51 | 144 | Self-reported | 83 | tTG | 91.7 |
| Lanzini et al., 2009 [32] | Cohort | 2009 | Italy | 465 | 356 | 31 (18–81) | 16 (13–222) | Self-reported | 85.8 | Biopsy | 79.5 |
| Duerksen et al., 2010 [47] | Cohort | NI | Canada | 21 | 19 | 50.5 | 116.4 | Self-reported | 71.4 | Biopsy | 71.4 |
| Hutchinson et al., 2010 [41] | Cohort | 2009 | UK | 234 | 202 | >18 | 34.8 | Self-reported | 88 | Biopsy | 35 |
| Nachman et al., 2011 [44] | Cohort | 2004–2005 | Argentina | 53 | 48 | 18–66 | 12 | Self-reported | 60.3 | TTG | 62.2 |
| 48 | 52.8 | TTG | 49 | ||||||||
| 12 | 60.3 | tTG/DGP | 79.2 | ||||||||
| 48 | 52.8 | tTG/DGP | 71.7 | ||||||||
| Newnham et al., 2016 [45] | Cohort | NI | Australia | 44 | NI | 40 (18–71) | 60 | Self-reported | 97.7 | Biopsy | 16 |
| Stasi et al., 2016 [27] | Cohort | NI | Italy | 39 | NI | 40 | 66 (13–261) | Self-reported | 53.8 | Biopsy | 84.6 |
| 52 | 86.5 | EMA | 75 | ||||||||
| Pekki et al., 2017 [38] | Cohort | NI | Finland | 476 | NI | 55 | 96 | Self-reported | 98.7 | Biopsy | 58 |
| Ferreira et al., 2018 [51] | Cohort | 2015–2017 | Paraguay | 72 | 55 | 35.6 ± 12.4 | 294 | Self-reported | 68 | tTG | 44.4 |
| Norsa et al., 2018 [34] | Cohort | 2014–2015 | Italy | 63 | NI | 31.34 | 320 (1–432) | Self-reported | 46 | Biopsy | 74.6 |
| Elli et al., 2020 [30] | Cohort | 2017–2018 | Italy | 197 | 159 | 44.6 | 87 ± 74 | Self-reported | 75.6 | tTG | 94.4 |
| Sayar et al., 2021 [53] | Cohort | 2010 | Türkiye | 78 | 68 | 36.8 ± 7.7 | 31 | Self-reported | 78.2 | EMA/tTG | 59 |
| Nemteanu et al., 2023 [52] | Cohort | 2016–2021 | Romania | 102 | 79 | 39.54 ± 12.70 | 22.6 | Self-reported | 27.4 | tTG | 71.5 |
| Number of Studies | Grouped Estimation Phi (CI 95%) | |
|---|---|---|
| TOTAL | 42 | 0.297 (0.220; 0.372) |
| Tool used to evaluate GFD adherence * | ||
| CDAT | 8 | 0.112 (0.032; 0.192) A |
| SDE | 1 | 0.238 (−0.051; 0.528) AB |
| BIAGI | 8 | 0.242 (0.073; 0.410) AB |
| Self-report | 21 | 0.308 (0.209; 0.406) B |
| Interview | 3 | 0.641 (0.380; 0.903) B |
| Laboratory test used to evaluate GFD adherence | ||
| GIP | 4 | 0.088 (−0.031; 0.207) A |
| Biopsy | 20 | 0.264 (0.163; 0.365) AB |
| Serological (TTG, EMA, AGA) | 18 | 0.378 (0.256; 0.501) B |
| Tool X laboratory test * | ||
| BIAGI and Serological | 4 | 0.066 (−0.126; 0.258) A |
| CDAT and GIP | 4 | 0.088 (−0.031; 0.207) A |
| Self-report and Biopsy | 9 | 0.116 (0.016; 0.216) A |
| CDAT and Biopsy | 3 | 0.126 (−0.053; 0.304) AB |
| CDAT and Serological | 1 | 0.226 (0.027; 0.425) ABC |
| SDE and Biopsy | 1 | 0.238 (−0.051; 0.528) ABC |
| BIAGI and Biopsy | 4 | 0.410 (0.268; 0.551) BC |
| Self-report and Serological | 12 | 0.467 (0.384; 0.551) C |
| Interview and Biopsy | 2 | 0.489 (0.419; 0.559) C |
| Interview and Serological | 1 | 0.903 (0.796; 1.000) D |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ribeiro, C.d.S.; Uenishi, R.H.; Domingues, A.d.S.; Nakano, E.Y.; Botelho, R.B.A.; Raposo, A.; Zandonadi, R.P. Gluten-Free Diet Adherence Tools for Individuals with Celiac Disease: A Systematic Review and Meta-Analysis of Tools Compared to Laboratory Tests. Nutrients 2024, 16, 2428. https://doi.org/10.3390/nu16152428
Ribeiro CdS, Uenishi RH, Domingues AdS, Nakano EY, Botelho RBA, Raposo A, Zandonadi RP. Gluten-Free Diet Adherence Tools for Individuals with Celiac Disease: A Systematic Review and Meta-Analysis of Tools Compared to Laboratory Tests. Nutrients. 2024; 16(15):2428. https://doi.org/10.3390/nu16152428
Chicago/Turabian StyleRibeiro, Camila dos Santos, Rosa Harumi Uenishi, Alessandra dos Santos Domingues, Eduardo Yoshio Nakano, Raquel Braz Assunção Botelho, António Raposo, and Renata Puppin Zandonadi. 2024. "Gluten-Free Diet Adherence Tools for Individuals with Celiac Disease: A Systematic Review and Meta-Analysis of Tools Compared to Laboratory Tests" Nutrients 16, no. 15: 2428. https://doi.org/10.3390/nu16152428