
A Novel Machine-Learning Algorithm to Predict the Early Termination of Nutrition Support Team Follow-Up in Hospitalized Adults: A Retrospective Cohort Study
 , , ,
, , ,  , , ,
, , ,
Abstract
1. Introduction
2. Methods
2.1. Study Design and Population
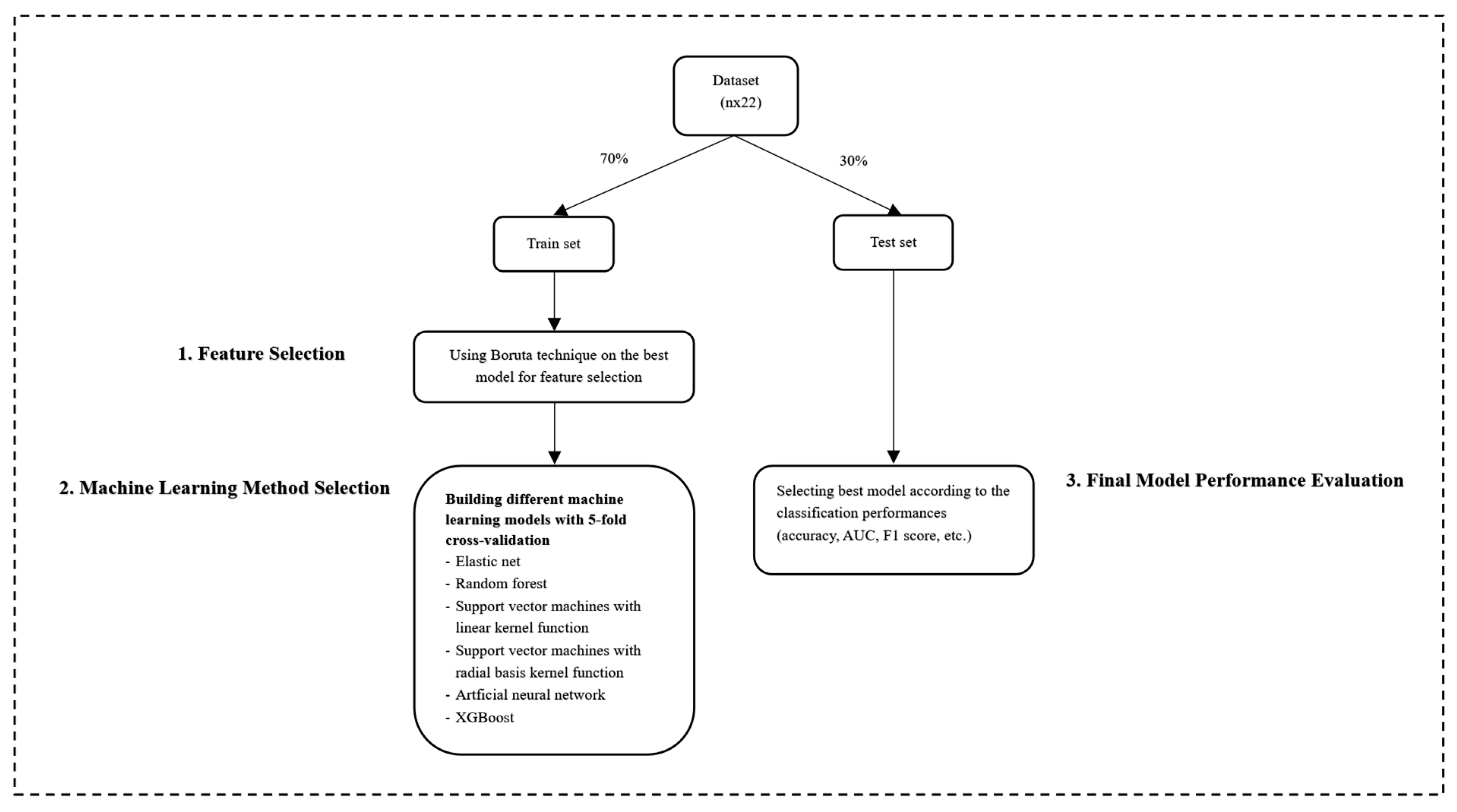
2.2. Statistical Analysis
2.3. Ethics Approval
3. Results
3.1. Baseline Characteristics
3.2. Feature Selection
3.3. Comparison of Model Performance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lochs, H.; Allison, S.P.; Meier, R.; Pirlich, M.; Kondrup, J.; Schneider, S.; van den Berghe, G.; Pichard, C. Introductory to the ESPEN Guidelines on Enteral Nutrition: Terminology, definitions and general topics. Clin. Nutr. 2006, 25, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Naylor, C.J.; Griffiths, R.D.; Fernandez, R.S. Does a multidisciplinary total parenteral nutrition team improve patient outcomes? A systematic review. JPEN J. Parenter. Enter. Nutr. 2004, 28, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, J.F.; Nightingale, J.M. Cost savings of an adult hospital nutrition support team. Nutrition 2005, 21, 1127–1133. [Google Scholar] [CrossRef] [PubMed]
- Braun, K.; Utech, A.; Velez, M.E.; Walker, R. Parenteral Nutrition Electrolyte Abnormalities and Associated Factors Before and After Nutrition Support Team Initiation. JPEN J. Parenter. Enter. Nutr. 2018, 42, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Piquet, M.A.; Bertrand, P.C.; Roulet, M. Role of a nutrition support team in reducing the inappropriate use of parenteral nutrition. Clin. Nutr. 2004, 23, 437. [Google Scholar] [CrossRef] [PubMed]
- Martinez, M.J.; Martinez, M.A.; Montero, M.; Campelo, E.; Castro, I.; Inaraja, M.T. Hypophosphatemia in postoperative patients with total parenteral nutrition: Influence of nutritional support teams. Nutr. Hosp. 2006, 21, 657–660. [Google Scholar] [PubMed]
- Katagiri, S.; Shiba, T.; Tohara, H.; Yamaguchi, K.; Hara, K.; Nakagawa, K.; Komatsu, K.; Watanabe, K.; Ohsugi, Y.; Maekawa, S.; et al. Re-initiation of Oral Food Intake Following Enteral Nutrition Alters Oral and Gut Microbiota Communities. Front. Cell Infect. Microbiol. 2019, 9, 434. [Google Scholar] [CrossRef] [PubMed]
- Thibault, R.; Abbasoglu, O.; Ioannou, E.; Meija, L.; Ottens-Oussoren, K.; Pichard, C.; Rothenberg, E.; Rubin, D.; Siljamaki-Ojansuu, U.; Vaillant, M.F.; et al. ESPEN guideline on hospital nutrition. Clin. Nutr. 2021, 40, 5684–5709. [Google Scholar] [CrossRef]
- Senkal, M.; Dormann, A.; Stehle, P.; Shang, E.; Suchner, U. Survey on structure and performance of nutrition-support teams in Germany. Clin. Nutr. 2002, 21, 329–335. [Google Scholar] [CrossRef]
- Ravasco, P.; Martins, P.; Ruivo, A.; Camilo, M.E. Survey on the current practice of nutritional therapy in Portugal. Clin. Nutr. 2004, 23, 113–119. [Google Scholar] [CrossRef]
- Hearnshaw, S.A.; Thompson, N.P.; Northern Nutrition Network. Use of parenteral nutrition in hospitals in the North of England. J. Hum. Nutr. Diet. 2007, 20, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Hvas, C.L.; Farrer, K.; Donaldson, E.; Blackett, B.; Lloyd, H.; Forde, C.; Garside, G.; Paine, P.; Lal, S. Quality and safety impact on the provision of parenteral nutrition through introduction of a nutrition support team. Eur. J. Clin. Nutr. 2014, 68, 1294–1299. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.; Park, Y.S.; Park, D.J.; Kim, S.; Lee, H.; Kim, M.; Lee, E.; Lee, H.Y.; Lee, E. Bridging Policy and Service Performance of Hospital-Based Nutrition Support by Healthcare Information Technology. Nutrients 2021, 13, 595. [Google Scholar] [CrossRef] [PubMed]
- Kirk, D.; Kok, E.; Tufano, M.; Tekinerdogan, B.; Feskens, E.J.M.; Camps, G. Machine Learning in Nutrition Research. Adv. Nutr. 2022, 13, 2573–2589. [Google Scholar] [CrossRef] [PubMed]
- Wunderle, C.; Gomes, F.; Schuetz, P.; Stumpf, F.; Austin, P.; Ballesteros-Pomar, M.D.; Cederholm, T.; Fletcher, J.; Laviano, A.; Norman, K.; et al. ESPEN guideline on nutritional support for polymorbid medical inpatients. Clin. Nutr. 2023, 42, 1545–1568. [Google Scholar] [CrossRef] [PubMed]
- Amano, K.; Maeda, I.; Ishiki, H.; Miura, T.; Hatano, Y.; Tsukuura, H.; Taniyama, T.; Matsumoto, Y.; Matsuda, Y.; Kohara, H.; et al. Effects of enteral nutrition and parenteral nutrition on survival in patients with advanced cancer cachexia: Analysis of a multicenter prospective cohort study. Clin. Nutr. 2021, 40, 1168–1175. [Google Scholar] [CrossRef] [PubMed]
- Halil, M.G.; Demirkan, K.; Doganay, M.; Cengiz, C.; Gunduz, M.; Abbasoglu, O. Accreditation of nutrition support teams: A new initiative by the Turkish Society of Clinical Enteral & Parenteral Nutrition. Nutrition 2023, 114, 112112. [Google Scholar] [CrossRef] [PubMed]
- Kursa, M.B.; Rudnicki, W.R. Feature selection with the Boruta package. J. Stat. Softw. 2010, 36, 1–13. [Google Scholar] [CrossRef]
- Mindiyarti, N.; Sartono, B.; Indahwati, I.; Hadi, A.F.; Ramadhani, E. A study in determining indicators of food-insecure households using SHAP and Boruta SHAP. AIP Conf. Proc. 2023, 2720, 020011. [Google Scholar]
- Ouyang, B.; Song, Y.; Li, Y.; Wu, F.; Yu, H.; Wang, Y.; Yin, Z.; Luo, X.; Sant, G.; Bauchy, M. Using machine learning to predict concrete’s strength: Learning from small datasets. Eng. Res. Express 2021, 3, 015022. [Google Scholar] [CrossRef]
- Kuhn, M. R Package, Version 6.0-91; Package “caret”: Classification and Regression Training. 2022. Available online: https://cran.r-project.org/web/packages/caret/caret.pdf (accessed on 5 July 2024).
- DAĞ, O.; Karabulut, E.; Alpar, R. Gmdh2: Binary classification via gmdh-type neural network algorithms-R package and web-based tool. Int. J. Comput. Intell. Syst. 2019, 12, 649–660. [Google Scholar] [CrossRef]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Muller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, M.; Atal, I.; Li, J.; Smith, P.; Ravaud, P.; Fergie, M.; Callaghan, M.; Selfe, J. Reporting quality of studies using machine learning models for medical diagnosis: A systematic review. BMJ Open 2020, 10, 034568. [Google Scholar] [CrossRef] [PubMed]
- Guenter, P.; Blackmer, A.; Malone, A.; Mirtallo, J.M.; Phillips, W.; Tyler, R.; Barrocas, A.; Resnick, H.E.; Anthony, P.; Abdelhadi, R. Update on use of enteral and parenteral nutrition in hospitalized patients with a diagnosis of malnutrition in the United States. Nutr. Clin. Pract. 2022, 37, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Salinari, A.; Machi, M.; Armas Diaz, Y.; Cianciosi, D.; Qi, Z.; Yang, B.; Ferreiro Cotorruelo, M.S.; Villar, S.G.; Dzul Lopez, L.A.; Battino, M.; et al. The Application of Digital Technologies and Artificial Intelligence in Healthcare: An Overview on Nutrition Assessment. Diseases 2023, 11, 97. [Google Scholar] [CrossRef] [PubMed]
- Knights, V.; Kolak, M.; Markovikj, G.; Gajdoš Kljusurić, J. Modeling and Optimization with Artificial Intelligence in Nutrition. Appl. Sci. 2023, 13, 7835. [Google Scholar] [CrossRef]
- Patel, C.; Omer, E.; Diamond, S.J.; McClave, S.A. Can Nutritional Assessment Tools Predict Response to Nutritional Therapy? Curr. Gastroenterol. Rep. 2016, 18, 15. [Google Scholar] [CrossRef] [PubMed]
- Yin, L.; Song, C.; Cui, J.; Lin, X.; Li, N.; Fan, Y.; Zhang, L.; Liu, J.; Chong, F.; Wang, C.; et al. A fusion decision system to identify and grade malnutrition in cancer patients: Machine learning reveals feasible workflow from representative real-world data. Clin. Nutr. 2021, 40, 4958–4970. [Google Scholar] [CrossRef]
- Raphaeli, O.; Singer, P. Towards personalized nutritional treatment for malnutrition using machine learning-based screening tools. Clin. Nutr. 2021, 40, 5249–5251. [Google Scholar] [CrossRef]
- Parsons, E.L.; Baldwin, C.; Fitzpatrick, J.; Knight, A.; Manthorpe, J.; Thomas, J.E.; Weekes, E.; Whelan, K.; Wilson, R.; Murrells, T.; et al. Designing a national clinical audit of nutritional care in health and social care settings: Consideration and future directions. Proc. Nutr. Soc. 2013, 72, 251–260. [Google Scholar] [CrossRef]
- Ukleja, A.; Gilbert, K.; Mogensen, K.M.; Walker, R.; Ward, C.T.; Ybarra, J.; Holcombe, B.; Task Force on Standards for Nutrition Support: Adult Hospitalized Patients, the American Society for Parenteral and Enteral Nutrition. Standards for Nutrition Support: Adult Hospitalized Patients. Nutr. Clin. Pract. 2018, 33, 906–920. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.M.; Wang, M.; Sun, N.X.; Liu, Y.Y.; Yin, T.F.; Chen, C. Screening and application of nutritional support in elderly hospitalized patients of a tertiary care hospital in China. PLoS ONE 2019, 14, 0213076. [Google Scholar] [CrossRef] [PubMed]
- Poisson, P.; Laffond, T.; Campos, S.; Dupuis, V.; Bourdel-Marchasson, I. Relationships between oral health, dysphagia and undernutrition in hospitalised elderly patients. Gerodontology 2016, 33, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Ikezawa, K.; Hirose, M.; Maruyama, T.; Yuji, K.; Yabe, Y.; Kanamori, T.; Kaide, N.; Tsuchiya, Y.; Hara, S.; Suzuki, H. Effect of early nutritional initiation on post-cerebral infarction discharge destination: A propensity-matched analysis using machine learning. Nutr. Diet. 2022, 79, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hubner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.G.; et al. ESPEN practical guideline: Clinical nutrition in surgery. Clin. Nutr. 2021, 40, 4745–4761. [Google Scholar] [CrossRef]
- Lobo, D.N.; Gianotti, L.; Adiamah, A.; Barazzoni, R.; Deutz, N.E.P.; Dhatariya, K.; Greenhaff, P.L.; Hiesmayr, M.; Hjort Jakobsen, D.; Klek, S.; et al. Perioperative nutrition: Recommendations from the ESPEN expert group. Clin. Nutr. 2020, 39, 3211–3227. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Measure | Formula | Definition |
|---|---|---|
| Accuracy | Ratio of correctly classified samples to the total number of samples. | |
| Sensitivity (Recall) | Ability of a model to correctly identify positive samples | |
| Specificity | Ability of a model to correctly identify negative samples | |
| Positive Predictive Value (Precision—PPV) | Indication of how many of the samples classified as positive by the model are actually positive | |
| Negative Predictive Value (NPV) | Indication of how many of the samples classified as negative by the model are actually negative | |
| Balanced Accuracy | Arithmetic means of sensitivity and specificity | |
| F1 Score | Harmonic mean of precision and recall | |
| Area Under ROC Curve (AUC) | Indication of how well the classes is separated from each other according to the model obtained |
| Reason for Follow-Up | |||
|---|---|---|---|
| Total (n = 2298) | Oral (n = 990) | Others (n = 1308) | |
| Age, mean (SD) | 61.52 (17.20) | 57.91 (15.97) | 64.26 (17.59) |
| BMI, mean (SD) | 23.70 (5.35) | 24.39 (5.39) | 23.17 (5.27) |
| NRS-2002, median (IQR) | 5 (1) | 4 (1) | 5 (1) |
| Gender, n (%) | |||
| Male | 1285 (55.92%) | 562 (43.74%) | 723 (56.26%) |
| Female | 1013 (44.08%) | 428 (42.25%) | 585 (57.75%) |
| Wards, n (%) | |||
| Internal medicine wards | 923 (40.17%) | 328 (35.54%) | 595 (64.46%) |
| Surgical wards | 720 (31.33%) | 483 (67.08%) | 237 (32.92%) |
| ICUs | 655 (28.5%) | 179 (27.33%) | 476 (72.67%) |
| Diagnosis, n (%) | |||
| Cancer | 1484 (64.58%) | 741 (49.93%) | 743 (50.07%) |
| Diseases of digestive system | 228 (9.92%) | 145 (63.6%) | 83 (36.4%) |
| Other | 586 (25.5%) | 104 (17.75%) | 482 (82.25%) |
| Type of MNT, n (%) | |||
| PN | 1471 (64.01%) | 880 (59.82%) | 591 (40.18%) |
| EN | 717 (31.2%) | 89 (12.41%) | 628 (87.59%) |
| Supplemental PN | 110 (4.79%) | 21 (19.09%) | 89 (80.91%) |
| Indication for MNT, n (%) | |||
| Inability to use GIS | 1578 (69.06%) | 610 (38.66%) | 968 (61.34%) |
| Surgical outcomes | 342 (14.97%) | 259 (75.73%) | 83 (24.27%) |
| Impaired consciousness | 154 (6.74) | 16 (10.39%) | 138 (89.61%) |
| Other | 211 (9.23) | 101 (47.87%) | 110 (52.13%) |
| Comorbidities, n (%) | |||
| DM | 468 (20.37%) | 172 (36.75%) | 296 (63.25%) |
| CAD | 296 (12.88%) | 101 (34.12%) | 195 (65.88%) |
| COPD | 149 (6.48%) | 53 (35.57%) | 96 (64.43%) |
| CKD | 127 (5.50%) | 36 (28.35%) | 91 (71.65%) |
| CHF | 117 (5.09%) | 26 (22.22%) | 91 (77.78%) |
| ANN | EN | RF | XGBoost | SVM-Radial | SVM-Linear | |
|---|---|---|---|---|---|---|
| Accuracy | 0.770 | 0.770 | 0.754 | 0.745 | 0.762 | 0.722 |
| Sensitivity | 0.772 | 0.768 | 0.738 | 0.742 | 0.742 | 0.721 |
| Specificity | 0.768 | 0.771 | 0.765 | 0.747 | 0.778 | 0.722 |
| PPV | 0.719 | 0.720 | 0.707 | 0.693 | 0.720 | 0.666 |
| NPV | 0.814 | 0.813 | 0.792 | 0.790 | 0.797 | 0.771 |
| Baccuracy | 0.770 | 0.770 | 0.752 | 0.745 | 0.760 | 0.722 |
| F1 Score | 0.744 | 0.744 | 0.722 | 0.716 | 0.731 | 0.692 |
| AUC (95% C.I.) | 0.770 (0.738–0.802) | 0.770 (0.738–0.801) | 0.752 (0.719–0.785) | 0.745 (0.712–0.778) | 0.760 (0.728–0.792) | 0.722 (0.688–0.755) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yalçın, N.; Kaşıkcı, M.; Kelleci-Çakır, B.; Allegaert, K.; Güner-Oytun, M.; Ceylan, S.; Balcı, C.; Demirkan, K.; Halil, M.; Abbasoğlu, O. A Novel Machine-Learning Algorithm to Predict the Early Termination of Nutrition Support Team Follow-Up in Hospitalized Adults: A Retrospective Cohort Study. Nutrients 2024, 16, 2492. https://doi.org/10.3390/nu16152492
Yalçın N, Kaşıkcı M, Kelleci-Çakır B, Allegaert K, Güner-Oytun M, Ceylan S, Balcı C, Demirkan K, Halil M, Abbasoğlu O. A Novel Machine-Learning Algorithm to Predict the Early Termination of Nutrition Support Team Follow-Up in Hospitalized Adults: A Retrospective Cohort Study. Nutrients. 2024; 16(15):2492. https://doi.org/10.3390/nu16152492
Chicago/Turabian StyleYalçın, Nadir, Merve Kaşıkcı, Burcu Kelleci-Çakır, Karel Allegaert, Merve Güner-Oytun, Serdar Ceylan, Cafer Balcı, Kutay Demirkan, Meltem Halil, and Osman Abbasoğlu. 2024. "A Novel Machine-Learning Algorithm to Predict the Early Termination of Nutrition Support Team Follow-Up in Hospitalized Adults: A Retrospective Cohort Study" Nutrients 16, no. 15: 2492. https://doi.org/10.3390/nu16152492
APA StyleYalçın, N., Kaşıkcı, M., Kelleci-Çakır, B., Allegaert, K., Güner-Oytun, M., Ceylan, S., Balcı, C., Demirkan, K., Halil, M., & Abbasoğlu, O. (2024). A Novel Machine-Learning Algorithm to Predict the Early Termination of Nutrition Support Team Follow-Up in Hospitalized Adults: A Retrospective Cohort Study. Nutrients, 16(15), 2492. https://doi.org/10.3390/nu16152492