
An Assessment of Behavioral Risk Factors in Oncology Patients
 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
3.1. Socio-Demographic Characteristics and Lifestyle
3.2. Eating Habits and Lifestyle
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 20 May 2024).
- ReFaey, K.; Tripathi, S.; Grewal, S.S.; Bhargav, A.G.; Quinones, D.J.; Chaichana, K.L.; Antwi, S.O.; Cooper, L.T.; Meyer, F.B.; Dronca, R.S.; et al. Cancer Mortality Rates Increasing vs. Cardiovascular Disease Mortality Decreasing in the World: Future Implications. Mayo Clin. Proc. Innov. Qual. Outcomes 2021, 5, 645. [Google Scholar] [CrossRef]
- Cancer Today. Available online: https://gco.iarc.fr/today/online-analysis-table?v=2020&mode=cancer&mode_population=continents&population=900&populations=900&key=asr&sex=0&cancer=39&type=0&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=0&ages_group%5B%5D=17&group_cancer=1&include_nmsc=0&include_nmsc_other=1 (accessed on 20 May 2024).
- Anand, P.; Kunnumakara, A.B.; Sundaram, C.; Harikumar, K.B.; Tharakan, S.T.; Lai, O.S.; Sung, B.; Aggarwal, B.B. Cancer Is a Preventable Disease That Requires Major Lifestyle Changes. Pharm. Res. 2008, 25, 2097. [Google Scholar] [CrossRef]
- Berben, L.; Floris, G.; Wildiers, H.; Hatse, S. Cancer and Aging: Two Tightly Interconnected Biological Processes. Cancers 2021, 13, 1400. [Google Scholar] [CrossRef]
- Bagnardi, V.; Rota, M.; Botteri, E.; Tramacere, I.; Islami, F.; Fedirko, V.; Scotti, L.; Jenab, M.; Turati, F.; Pasquali, E.; et al. Alcohol Consumption and Site-Specific Cancer Risk: A Comprehensive Dose-Response Meta-Analysis. Br. J. Cancer 2015, 112, 580–593. [Google Scholar] [CrossRef]
- White, A.J.; DeRoo, L.A.; Weinberg, C.R.; Sandler, D.P. Lifetime Alcohol Intake, Binge Drinking Behaviors, and Breast Cancer Risk. Am. J. Epidemiol. 2017, 186, 541–549. [Google Scholar] [CrossRef]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans Personal Habits and Indoor Combustions. A Review of Human Carcinogens. In IARC Monographs on the Evaluation of Carcinogenic Risks in Humans; International Agency for Research on Cancer: Lyon, France, 2012; Volume 100 E, pp. 373–472. [Google Scholar]
- Cancer-Causing Substances in the Environment-NCI. Available online: https://www.cancer.gov/about-cancer/causes-prevention/risk/substances (accessed on 20 September 2023).
- Parsa, N. Environmental Factors Inducing Human Cancers. Iran. J. Public Health 2012, 41, 1. [Google Scholar]
- Turati, F.; Galeone, C.; Augustin, L.S.A.; La Vecchia, C. Glycemic Index, Glycemic Load and Cancer Risk: An Updated Meta-Analysis. Nutrients 2019, 11, 2342. [Google Scholar] [CrossRef]
- Theodoratou, E.; Timofeeva, M.; Li, X.; Meng, X.; Ioannidis, J.P.A. Nature, Nurture and Cancer Risks: Genetic and Nutritional Contributions to Cancer. Annu. Rev. Nutr. 2017, 37, 293. [Google Scholar] [CrossRef]
- Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; Abdulle, A.S.M.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar] [CrossRef] [PubMed]
- Caporaso, N.; Gu, F.; Chatterjee, N.; Sheng-Chih, J.; Yu, K.; Yeager, M.; Chen, C.; Jacobs, K.; Wheeler, W.; Landi, M.T.; et al. Genome-Wide and Candidate Gene Association Study of Cigarette Smoking Behaviors. PLoS ONE 2010, 4, e4653. [Google Scholar] [CrossRef]
- Smoking and Cancer|Overviews of Diseases/Conditions|Tips from Former Smokers|CDC. Available online: https://www.cdc.gov/tobacco/campaign/tips/diseases/cancer.html#five (accessed on 21 May 2024).
- Weng, M.W.; Lee, H.W.; Park, S.H.; Hu, Y.; Wang, H.T.; Chen, L.C.; Rom, W.N.; Huang, W.C.; Lepor, H.; Wu, X.R.; et al. Aldehydes Are the Predominant Forces Inducing DNA Damage and Inhibiting DNA Repair in Tobacco Smoke Carcinogenesis. Proc. Natl. Acad. Sci. USA 2018, 115, E6152–E6161. [Google Scholar] [CrossRef] [PubMed]
- Oral and Oropharyngeal Cancer: Risk Factors and Prevention|Cancer.Net. Available online: https://www.cancer.net/cancer-types/oral-and-oropharyngeal-cancer/risk-factors-and-prevention (accessed on 31 May 2024).
- Pati, S.; Irfan, W.; Jameel, A.; Ahmed, S.; Shahid, R.K. Obesity and Cancer: A Current Overview of Epidemiology, Pathogenesis, Outcomes, and Management. Cancers 2023, 15, 485. [Google Scholar] [CrossRef] [PubMed]
- Munsell, M.F.; Sprague, B.L.; Berry, D.A.; Chisholm, G.; Trentham-Dietz, A. Body Mass Index and Breast Cancer Risk According to Postmenopausal Estrogen-Progestin Use and Hormone Receptor Status. Epidemiol. Rev. 2014, 36, 114–136. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Greenwood, D.C.; Chan, D.S.M.; Vieira, R.; Vieira, A.R.; Navarro Rosenblatt, D.A.; Cade, J.E.; Burley, V.J.; Norat, T. Body Mass Index, Abdominal Fatness and Pancreatic Cancer Risk: A Systematic Review and Non-Linear Dose-Response Meta-Analysis of Prospective Studies. Ann. Oncol. 2012, 23, 843–852. [Google Scholar] [CrossRef] [PubMed]
- Schmid, D.; Ricci, C.; Behrens, G.; Leitzmann, M.F. Adiposity and Risk of Thyroid Cancer: A Systematic Review and Meta-Analysis. Obes. Rev. 2015, 16, 1042–1054. [Google Scholar] [CrossRef] [PubMed]
- Beral, V.; Hermon, C.; Peto, R.; Reeves, G.; Brinton, L.; Marchbanks, P.; Negri, E.; Ness, R.; Peeters, P.H.M.; Vessey, M.; et al. Ovarian Cancer and Body Size: Individual Participant Meta-Analysis Including 25,157 Women with Ovarian Cancer from 47 Epidemiological Studies. PLoS Med. 2012, 9, e1001200. [Google Scholar] [CrossRef]
- Barrington, W.E.; Schenk, J.M.; Etzioni, R.; Arnold, K.B.; Neuhouser, M.L.; Thompson, I.M.; Lucia, M.S.; Kristal, A.R. Difference in Association of Obesity With Prostate Cancer Risk Between US African American and Non-Hispanic White Men in the Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA Oncol. 2015, 1, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Coe, P.O.; O’Reilly, D.A.; Renehan, A.G. Excess Adiposity and Gastrointestinal Cancer. Br. J. Surg. 2014, 101, 1518–1531. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Gan, Y.; Li, W.; Wu, C.; Lu, Z. Overweight, Obesity and the Risk of Gallbladder and Extrahepatic Bile Duct Cancers: A Meta-Analysis of Observational Studies. Obesity 2016, 24, 1786–1802. [Google Scholar] [CrossRef]
- Ma, Y.; Yang, Y.; Wang, F.; Zhang, P.; Shi, C.; Zou, Y.; Qin, H. Obesity and Risk of Colorectal Cancer: A Systematic Review of Prospective Studies. PLoS ONE 2013, 8, e53916. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, X.; Wang, J.; Yan, Z.; Luo, J. Excess Body Weight and the Risk of Primary Liver Cancer: An Updated Meta-Analysis of Prospective Studies. Eur. J. Cancer 2012, 48, 2137–2145. [Google Scholar] [CrossRef]
- Niedermaier, T.; Behrens, G.; Schmid, D.; Schlecht, I.; Fischer, B.; Leitzmann, M.F. Body Mass Index, Physical Activity, and Risk of Adult Meningioma and Glioma. Neurology 2015, 85, 1342–1350. [Google Scholar] [CrossRef] [PubMed]
- Genkinger, J.M.; Spiegelman, D.; Anderson, K.E.; Bernstein, L.; Van Den Brandt, P.A.; Calle, E.E.; English, D.R.; Folsom, A.R.; Freudenheim, J.L.; Fuchs, C.S.; et al. A Pooled Analysis of 14 Cohort Studies of Anthropometric Factors and Pancreatic Cancer Risk. Int. J. Cancer 2011, 129, 1708–1717. [Google Scholar] [CrossRef] [PubMed]
- Jenabi, E.; Poorolajal, J. The Effect of Body Mass Index on Endometrial Cancer: A Meta-Analysis. Public Health 2015, 129, 872–880. [Google Scholar] [CrossRef] [PubMed]
- Hoyo, C.; Cook, M.B.; Kamangar, F.; Freedman, N.D.; Whiteman, D.C.; Bernstein, L.; Brown, L.M.; Risch, H.A.; Ye, W.; Sharp, L.; et al. Body Mass Index in Relation to Oesophageal and Oesophagogastric Junction Adenocarcinomas: A Pooled Analysis from the International BEACON Consortium. Int. J. Epidemiol. 2012, 41, 1706–1718. [Google Scholar] [CrossRef]
- Aune, D.; Sen, A.; Prasad, M.; Norat, T.; Janszky, I.; Tonstad, S.; Romundstad, P.; Vatten, L.J. BMI and All Cause Mortality: Systematic Review and Non-Linear Dose-Response Meta-Analysis of 230 Cohort Studies with 3.74 Million Deaths among 30.3 Million Participants. BMJ 2016, 353, i2156. [Google Scholar] [CrossRef]
- Petrelli, F.; Cortellini, A.; Indini, A.; Tomasello, G.; Ghidini, M.; Nigro, O.; Salati, M.; Dottorini, L.; Iaculli, A.; Varricchio, A.; et al. Association of Obesity With Survival Outcomes in Patients With Cancer: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2021, 4, e213520. [Google Scholar] [CrossRef]
- Moke, D.J.; Hamilton, A.S.; Chehab, L.; Deapen, D.; Freyer, D.R. Obesity and Risk for Second Malignant Neoplasms in Childhood Cancer Survivors: A Case-Control Study Utilizing the California Cancer Registry. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1612. [Google Scholar] [CrossRef]
- Taghizadeh, N.; Boezen, H.M.; Schouten, J.P.; Schröder, C.P.; De Vries, E.G.E.; Vonk, J.M. BMI and Lifetime Changes in BMI and Cancer Mortality Risk. PLoS ONE 2015, 10, e0125261. [Google Scholar] [CrossRef]
- Friedenreich, C.M.; Ryder-Burbidge, C.; McNeil, J. Physical Activity, Obesity and Sedentary Behavior in Cancer Etiology: Epidemiologic Evidence and Biologic Mechanisms. Mol. Oncol. 2021, 15, 790. [Google Scholar] [CrossRef]
- Moore, S.C.; Gierach, G.L.; Schatzkin, A.; Matthews, C.E. Physical Activity, Sedentary Behaviours, and the Prevention of Endometrial Cancer. Br. J. Cancer 2010, 103, 933. [Google Scholar] [CrossRef] [PubMed]
- Physical Activity. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 21 May 2024).
- Red Meat Genetic Signature for Colorectal Cancer-NCI. Available online: https://www.cancer.gov/news-events/cancer-currents-blog/2021/red-meat-colorectal-cancer-genetic-signature (accessed on 21 May 2024).
- Mititelu, M.; Ioniţă, A.C.; Moroşan, E. Research regarding integral processing of mussels from Black Sea. Farmacia 2014, 62, 625–632. [Google Scholar]
- Mititelu, M.; Neacsu, S.M.; Oprea, E.; Dumitrescu, D.-E.; Nedelescu, M.; Drăgănescu, D.; Nicolescu, T.O.; Rosca, A.C.; Ghica, M. Black Sea Mussels Qualitative and Quantitative Chemical Analysis: Nutritional Benefits and Possible Risks through Consumption. Nutrients 2022, 14, 964. [Google Scholar] [CrossRef] [PubMed]
- Ioniță-Mîndrican, C.-B.; Mititelu, M.; Musuc, A.M.; Oprea, E.; Ziani, K.; Neacșu, S.M.; Grigore, N.D.; Negrei, C.; Dumitrescu, D.-E.; Mireșan, H.; et al. Honey and Other Beekeeping Products Intake among the Romanian Population and Their Therapeutic Use. Appl. Sci. 2022, 12, 9649. [Google Scholar] [CrossRef]
- Mititelu, M.; Ghica, M.; Ionita, A.C.; Moroşan, E. The influence of heavy metals contamination in soil on the composition of some wild edible mushrooms. Farmacia 2019, 67, 398–404. [Google Scholar] [CrossRef]
- Pop, A.L.; Henteș, P.; Pali, M.-A.; Oșanu, L.; Ciobanu, A.; Nasui, B.A.; Mititelu, M.; Crișan, S.; Peneș, O.N. Study regarding a new extended-release calcium ascorbate and hesperidin solid oral formulation. Farmacia 2022, 70, 151–157. [Google Scholar] [CrossRef]
- Mititelu, M.; Hîncu, L.; Ozon, E.A.; Baconi, D.L.; Paunica, I.; Bălălău, O.D. Analysis of potentially toxic contaminants in milk powder. J. Mind Med. Sci. 2021, 8, 237–244. [Google Scholar] [CrossRef]
- Mititelu, M.; Oancea, C.-N.; Neacșu, S.M.; Olteanu, G.; Cîrțu, A.-T.; Hîncu, L.; Gheonea, T.C.; Stanciu, T.I.; Rogoveanu, I.; Hashemi, F.; et al. Evaluation of Non-Alcoholic Beverages and the Risk Related to Consumer Health among the Romanian Population. Nutrients 2023, 15, 3841. [Google Scholar] [CrossRef]
- Leahu, A.; Lupu, E.C. Statistical simulation and prediction in software reliability. Analele Univ. Ovidius Constanta Ser. Mat. 2008, 16, 81–90. [Google Scholar]
- Misiąg, W.; Piszczyk, A.; Szymańska-Chabowska, A.; Chabowski, M. Physical Activity and Cancer Care—A Review. Cancers 2022, 14, 4154. [Google Scholar] [CrossRef]
- Elad, B.; Habib, M.; Caspi, O. Cardio-Oncology Rehabilitation—Present and Future Perspectives. Life 2022, 12, 1006. [Google Scholar] [CrossRef]
- Gilchrist, S.C.; Barac, A.; Ades, P.A.; Alfano, C.M.; Franklin, B.A.; Jones, L.W.; La Gerche, A.; Ligibel, J.A.; Lopez, G.; Madan, K.; et al. Cardio-Oncology Rehabilitation to Manage Cardiovascular Outcomes in Cancer Patients and Survivors: A Scientific Statement From the American Heart Association. Circulation 2019, 139, E997–E1012. [Google Scholar] [CrossRef]
- Nonaka, M.; Hosoda, H.; Uezono, Y. Cancer Treatment-Related Cardiovascular Disease: Current Status and Future Research Priorities. Biochem. Pharmacol. 2021, 190, 114599. [Google Scholar] [CrossRef]
- OECD/European Observatory on Health Systems and Policies. România: Profilul de Țară Din 2023 în Ceea ce Privește Sănătatea, State of Health in the EU; OECD Publishing, Paris/European Observatory on Health Systems and Policies: Brussels, Belgium, 2023. [Google Scholar]
- Takahashi, S.; Matsumoto, K.; Ohba, K.; Nakano, Y.; Miyazawa, Y.; Kawaguchi, T. The Incidence and Management of Cancer-Related Anorexia During Treatment with Vascular Endothelial Growth Factor Receptor-Tyrosine Kinase Inhibitors. Cancer Manag. Res. 2023, 15, 1033. [Google Scholar] [CrossRef]
- Yeom, E.; Yu, K. Understanding the Molecular Basis of Anorexia and Tissue Wasting in Cancer Cachexia. Exp. Mol. Med. 2022, 54, 426–432. [Google Scholar] [CrossRef]
- Gallagher, E.J.; LeRoith, D. Obesity and cancer. Cancer Metastasis Rev. 2022, 41, 463–464. [Google Scholar] [CrossRef]
- Renehan, A.G.; Harvie, M.; Cutress, R.I.; Leitzmann, M.; Pischon, T.; Howell, S.; Howell, A. How to Manage the Obese Patient with Cancer. J. Clin. Oncol. 2016, 34, 4284–4294. [Google Scholar] [CrossRef]
- Silveira, E.A.; Kliemann, N.; Noll, M.; Sarrafzadegan, N.; de Oliveira, C. Visceral Obesity and Incident Cancer and Cardiovascular Disease: An Integrative Review of the Epidemiological Evidence. Obes. Rev. 2021, 22, e13088. [Google Scholar] [CrossRef]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Després, J.P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. Obesity and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation 2021, 143, E984–E1010. [Google Scholar] [CrossRef]
- Lyon, A.R.; López-Fernánde, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klei, J.; Boriani, G.; Cardinale, D.; Cordoba, R.; Cosyns, B.; et al. 2022 ESC Guidelines on Cardio-Oncology Developed in Collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur. Heart J. 2022, 43, 4229–4361. [Google Scholar] [CrossRef]
- Michos, E.D.; Marshall, C.H. Healthy Lifestyle Benefits Both Cancer and Cardiovascular Disease: More Bang for the Buck. Cardio Oncol. 2021, 3, 675–677. [Google Scholar] [CrossRef]
- Shi, M.; Luo, C.; Oduyale, O.K.; Zong, X.; Loconte, N.K.; Cao, Y. Alcohol Consumption Among Adults with a Cancer Diagnosis in the All of Us Research Program. JAMA Netw. Open 2023, 6, e2328328. [Google Scholar] [CrossRef]
- Mayne, S.T.; Cartmel, B.; Kirsh, V.; Goodwin, W.J. Alcohol and Tobacco Use Pre- and Post-Diagnosis and Survival in a Cohort of Patients with Early Stage Cancers of the Oral Cavity, Pharynx and Larynx. Cancer Epidemiol. Biomark. Prev. 2009, 18, 3368. [Google Scholar] [CrossRef]
- World Health Organization, International Agency of Research on Cancer. European Code Against Cancer. Available online: https://cancer-code-europe.iarc.fr/index.php/en/ (accessed on 25 May 2024).
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: A systematic review and meta-analysis of observational studies. Int. J. Cancer 2014, 135, 1884–1897. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Does a Mediterranean-type diet reduce cancer risk? Curr. Nutr. Rep. 2016, 5, 9–17. [Google Scholar] [CrossRef]
- How Nutrient Deficiency Causes Cancer-Dr. Zembroski. Available online: https://www.drzembroski.com/nutrient-deficiency-matches-radiation-cause-cancer/ (accessed on 31 May 2024).
- Ames, B.N. DNA Damage from Micronutrient Deficiencies Is Likely to Be a Major Cause of Cancer. Mutat. Res.-Fundam. Mol. Mech. Mutagen. 2001, 475, 7–20. [Google Scholar] [CrossRef]
- Haskins, C.P.; Champ, C.E.; Miller, R.; Vyfhuis, M.A.L. Nutrition in Cancer: Evidence and Equality. Adv. Radiat. Oncol. 2020, 5, 817–823. [Google Scholar] [CrossRef]
- Răşanu, T.; Mehedinţi-Hâncu, M.; Alexianu, M.; Mehedinţi, T.; Gheorghe, E.; Damian, I. Carnitine deficiency. Rom. J. Morphol. Embryol. 2012, 53, 203–206. [Google Scholar]
- Iliescu, D.M.; Micu, S.-I.; Ionescu, C.; Bulbuc, I.; Bordei, P.; Obadă, B.; Voinea, F.; Gheorghe, E.; Iliescu, M.G. Axial and para axial loading response evaluation on human cadaver harvested lumbar vertebral blocks: In vitro experiment with possible clinical implications for clinical practice. Exp. Ther. Med. 2021, 22, 1192. [Google Scholar] [CrossRef]
- Schloss, J.; Schloss, J. Cancer Treatment and Nutritional Deficiencies. In Nutritional Deficiency; IntechOpen: London, UK, 2016; Available online: https://www.intechopen.com/chapters/50604 (accessed on 25 May 2024). [CrossRef]
- Seidenberg, A.B.; Wiseman, K.P.; Klein, W.M.P. Do Beliefs about Alcohol and Cancer Risk Vary by Alcoholic Beverage Type and Heart Disease Risk Beliefs? Cancer Epidemiol. Biomark. Prev. 2023, 32, 46–53. [Google Scholar] [CrossRef]
- Bagnardi, V.; Blangiardo, M.; La Vecchia, C.; Corrao, G. Alcohol Consumption and the Risk of Cancer: A Meta-Analysis. Alcohol Res. Health 2001, 25, 263. [Google Scholar]
- Radon and Cancer-NCI. Available online: https://www.cancer.gov/about-cancer/causes-prevention/risk/substances/radon/radon-fact-sheet (accessed on 21 May 2024).
- Radon. Available online: https://www.who.int/news-room/fact-sheets/detail/radon-and-health (accessed on 21 May 2024).
- What Are the Risk Factors for Lung Cancer?|CDC. Available online: https://www.cdc.gov/cancer/lung/basic_info/risk_factors.htm (accessed on 21 May 2024).
- Taherdoost, H. Designing a Questionnaire for a Research Paper: A Comprehensive Guide to Design and Develop an Effective Questionnaire. Asian J. Manag. Sci. 2022, 11, 8–16. [Google Scholar] [CrossRef]
- James, B.L.; Loken, E.; Roe, L.S.; Myrissa, K.; Lawton, C.L.; Dye, L.; Rolls, B.J. Validation of the Diet Satisfaction Questionnaire: A new measure of satisfaction with diets for weight management. Obes. Sci. Pract. 2018, 4, 506–514. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dubasi, S.K.; Ranjan, P.; Arora, C.; Vikram, N.K.; Dwivedi, S.N.; Singh, N.; Kaloiya, G.S.; Shalimar. Questionnaire to assess adherence to diet and exercise advices for weight management in lifestyle-related diseases. J. Fam. Med. Prim. Care 2019, 8, 689–694. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total Population n (%) | Male n (%) | Female n (%) |
|---|---|---|---|
| 412 (100) | 202 (49.1) | 210 (50.9) | |
| Age (years) | p = 0.190 | ||
| 18–35 | 94 (22.8) | 48 (23.8) | 46 (21.9) |
| 36–53 | 140 (34.0) | 62 (30.7) | 78 (37.1) |
| 54–71 | 142 (34.5) | 66 (32.7) | 76 (36.2) |
| >71 | 36 (8.7) | 26 (12.9) | 10 (4.8) |
| Residence areas | p = 0.400 | ||
| Urban areas | 332 (80.6) | 158 (78.2) | 174 (82.9) |
| Rural areas | 80 (19.4) | 44 (21.8) | 36 (17.1) |
| Level of education | p = 0.604 | ||
| General/primary studies | 40 (9.7) | 22 (10.9) | 18 (8.6) |
| Secondary education (baccalaureate degree) | 90 (21.9) | 46 (22.8) | 44 (21.0) |
| Post-secondary studies | 52 (12.6) | 22 (10.9) | 30 (14.3) |
| Higher education (bachelor’s degree) | 146 (35.4) | 64 (31.7) | 82 (39.0) |
| Postgraduate studies (master’s degree, residency, doctorate, other specializations) | 84 (20.4) | 48 (23.7) | 36 (17.1) |
| Employment status | p = 0.604 | ||
| Medical leave | 46 (11.2) | 26 (12.9) | 20 (9.5) |
| Socially assisted | 6 (1.4) | 2 (1.0) | 4 (1.9) |
| Householder | 32 (7.8) | 10 (5.0) | 22 (10.5) |
| Retired | 138 (33.5) | 68 (33.6) | 70 (33.3) |
| Student/school student | 32 (7.8) | 20 (9.9) | 12 (5.7) |
| I go to work every day | 146 (35.4) | 70 (34.6) | 76 (36.2) |
| I work in a mixed regime (telework and commuting) | 12 (2.9) | 6 (3.0) | 6 (2.9) |
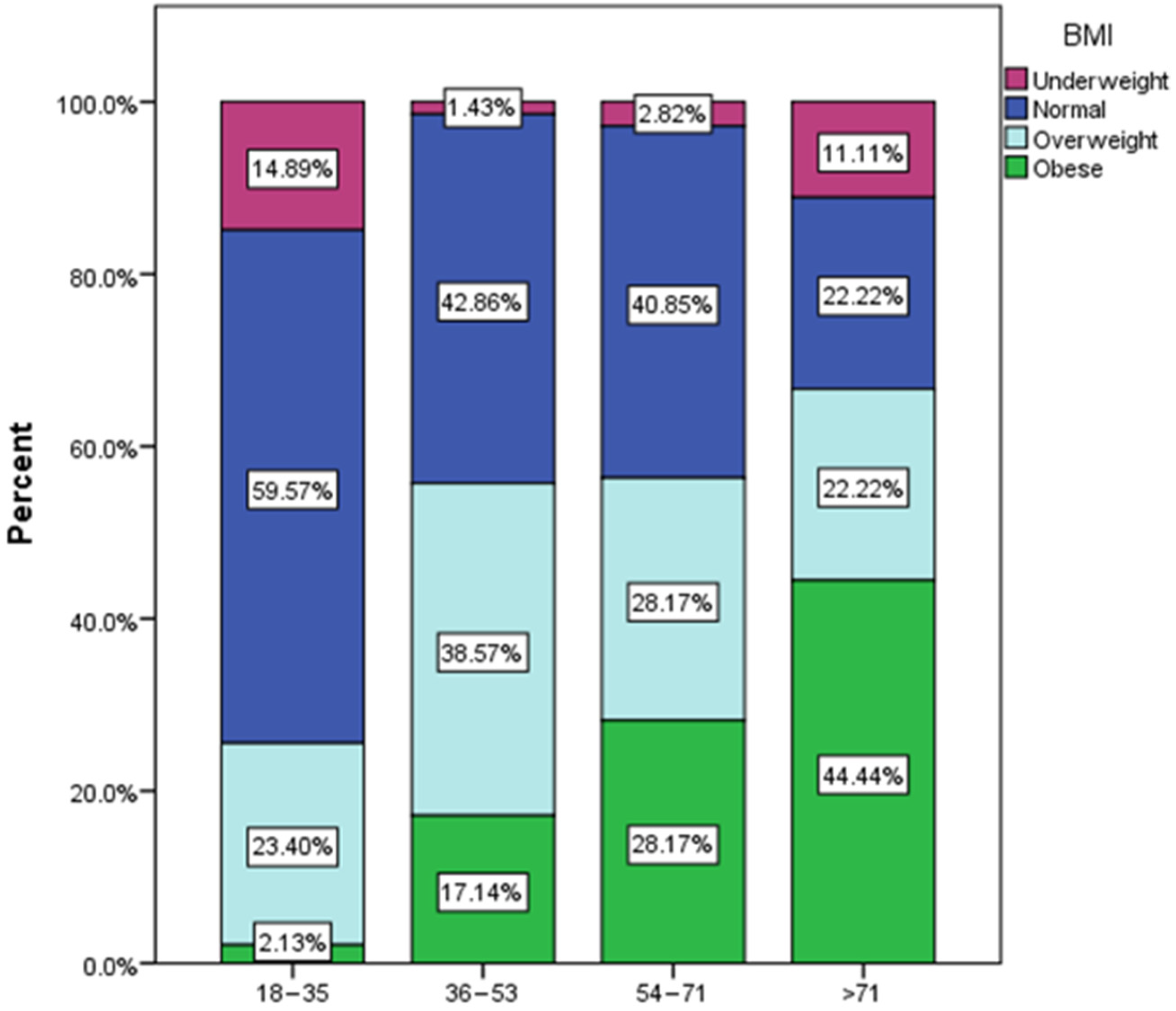
| Body mass index (BMI) | p = 0.799 | ||
| Normal weight (18.5–24.9) | 182 (44.2) | 96 (47.5) | 86 (41.0) |
| Overweight category (25–29.9) | 124 (30.1) | 58 (28.7) | 66 (31.4) |
| Underweight category (<18.5) | 24 (5.8) | 10 (5.0) | 14 (6.6) |
| Obese (≥30) | 82 (19.9) | 38 (18.8) | 44 (21.0) |
| Marital status | p = 0.026 | ||
| Single | 98 (23.8) | 64 (31.7) | 34 (16.2) |
| Divorced/separated | 56 (13.6) | 28 (13.9) | 28 (13.3) |
| Married | 258 (62.6) | 110 (54.4) | 148 (70.5) |
| Smoke habits | p = 0.438 | ||
| Yes, occasionally | 22 (5.4) | 16 (7.9) | 6 (2.9) |
| Yes, 1–2 cigarettes daily | 24 (5.8) | 12 (5.9) | 12 (5.7) |
| Yes, excessively daily | 52 (12.6) | 26 (12.9) | 26 (12.4) |
| No | 314 (76.2) | 148 (73.3) | 166 (79.0) |
| Alcohol consuming | p = 0.012 | ||
| Twice a week | 18 (4.3) | 10 (5.0) | 8 (3.8) |
| Very rarely or not at all | 320 (77.7) | 154 (76.2) | 166 (79.0) |
| More than two times a week | 14 (3.4) | 10 (5.0) | 4 (1.9) |
| Once a week | 40 (9.7) | 10 (5.0) | 30 (14.3) |
| One serving daily | 20 (4.9) | 18 (8.9) | 2 (1.0) |
| Sleep habits | p = 0.421 | ||
| I frequently have insomnia | 62 (15.1) | 24 (11.9) | 38 (18.1) |
| Less than 7 h per night | 146 (35.4) | 74 (36.6) | 72 (34.3) |
| More than 9 h per night | 14 (3.4) | 10 (5.0) | 4 (1.9) |
| 7–8 h per night | 190 (46.1) | 94 (46.5) | 96 (45.7) |
| Sports habits | p = 0.041 | ||
| Yes, 30 min daily | 48 (11.6) | 18 (8.9) | 30 (14.3) |
| Yes, at least one hour daily | 18 (4.4) | 10 (4.8) | 8 (3.8) |
| Yes, 2–3 times a week | 58 (14.1) | 30 (14.9) | 28 (13.3) |
| Yes, once a week | 8 (1.9) | 6 (3.0) | 2 (1.0) |
| Yes, very rarely | 80 (19.4) | 28 (13.9) | 52 (24.8) |
| No, due to health conditions | 54 (13.1) | 30 (14.9) | 24 (11.4) |
| No, because I am immobilized | 4 (1.0) | 2 (1.0) | 2 (1.0) |
| No, because I do not usually exercise | 142 (34.5) | 78 (38.6) | 64 (30.4) |
| Type of diet | p = 0.525 | ||
| Normal omnivorous diet | 320 (77.7) | 162 (80.2) | 158 (75.2) |
| Vegetarian diet/variations | 12 (2.9) | 6 (3.0) | 6 (2.9) |
| Vegan diet/variations | 4 (1.0) | 0 (0.0) | 4 (1.9) |
| Mediterranean diet | 34 (8.2) | 10 (8.9) | 16 (7.6) |
| Other | 42 (10.2) | 16 (7.9) | 26 (12.4) |
| Antecedents of oncological pathology in the family | p = 0.348 | ||
| Yes | 158 (38.4) | 68 (33.7) | 90 (42.9) |
| No | 172 (41.7) | 88 (43.5) | 84 (40.0) |
| I do not know | 82 (19.9) | 46 (22.8) | 36 (17.1) |
| Type of cancer | p < 0.0001 | ||
| Colon | 46 (11.2) | 24 (11.9) | 22 (10.5) |
| Gastric | 46 (11.2) | 24 (11.9) | 22 (10.5) |
| Liver | 28 (6.8) | 18 (8.9) | 10 (4.8) |
| Pancreatic | 40 (9.7) | 24 (11.9) | 16 (7.6) |
| Prostate | 36 (8.7) | 36 (17.8) | 0 (0.0) |
| Lung | 76 (18.4) | 40 (19.9) | 36 (17.1) |
| Kidney | 38 (9.2) | 16 (7.9) | 22 (10.5) |
| Breast | 54 (13.1) | 0 (0.0) | 54 (25.7) |
| Thyroid | 30 (7.3) | 10 (4.9) | 20 (9.5) |
| Other | 18 (4.4) | 10 (4.9) | 8 (3.8) |
| Variables | Nothing Changed n (%) | It Depreciated n (%) | It Improved n (%) |
|---|---|---|---|
| 180 (43.7) | 104 (25.2) | 128 (31.1) | |
| Category of food products | p = 0.0342 | ||
| Home-cooked meals | 156 (86.7) | 94 (90.4) | 120 (93.8) |
| Food cooked in restaurants | 16 (8.9) | 6 (5.8) | 4 (3.1) |
| Pizza, snacks, pastry, sweets | 2 (1.1) | 4 (3.8) | 2 (1.6) |
| Fast food products | 4 (2.2) | 0 (0.0) | 0 (0.0) |
| Products made from processed meats and canned goods | 2 (1.1) | 0 (0.0) | 2 (1.6) |
| Type of cooked foods | p = 0.0435 | ||
| Boiled or steamed foods | 66 (36.7) | 44 (42.3) | 46 (35.9) |
| Grilled foods | 12 (6.7) | 10 (9.6) | 4 (3.1) |
| Raw or minimally processed foods | 4 (2.2) | 0 (0.0) | 4 (3.1) |
| Fried foods | 40 (22.2) | 20 (19.2) | 20 (15.6) |
| Oven-baked foods | 56 (31.1) | 26 (25.0) | 50 (39.1) |
| Foods cooked over wood or charcoal | 2 (1.1) | 4 (3.8) | 4 (3.1) |
| Category of liquids | p = 0.0784 | ||
| Still water and natural juices | 108 (60.0) | 70 (67.3) | 80 (62.5) |
| Carbonated or sweetened non-alcoholic beverages | 26 (14.4) | 8 (7.7) | 8 (6.2) |
| Coffee | 20 (11.1) | 22 (21.2) | 28 (21.9) |
| Tea | 26 (14.4) | 4 (3.8) | 12 (9.4) |
| Meal distribution | p = 0.0876 | ||
| I consume 1–2 meals per day without a fixed schedule | 74 (41.1) | 26 (25.0) | 36 (28.1) |
| I consume 3 meals per day without a fixed schedule | 16 (8.9) | 4 (3.9) | 16 (12.5) |
| I consume 3 meals per day and 1–2 snacks without a fixed schedule | 70 (38.9) | 38 (36.5) | 40 (31.2) |
| I consume 3 meals per day on a fixed schedule | 6 (3.3) | 10 (9.6) | 24 (18.8) |
| I consume 3 meals per day and 1–2 snacks on a fixed schedule | 14 (7.8) | 26 (25.0) | 12 (9.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mititelu, M.; Licu, M.; Neacșu, S.M.; Călin, M.F.; Matei, S.R.; Scafa-Udriște, A.; Stanciu, T.I.; Busnatu, Ș.S.; Olteanu, G.; Măru, N.; et al. An Assessment of Behavioral Risk Factors in Oncology Patients. Nutrients 2024, 16, 2527. https://doi.org/10.3390/nu16152527
Mititelu M, Licu M, Neacșu SM, Călin MF, Matei SR, Scafa-Udriște A, Stanciu TI, Busnatu ȘS, Olteanu G, Măru N, et al. An Assessment of Behavioral Risk Factors in Oncology Patients. Nutrients. 2024; 16(15):2527. https://doi.org/10.3390/nu16152527
Chicago/Turabian StyleMititelu, Magdalena, Monica Licu, Sorinel Marius Neacșu, Mariana Floricica Călin, Silvia Raluca Matei, Alexandru Scafa-Udriște, Tiberius Iustinian Stanciu, Ștefan Sebastian Busnatu, Gabriel Olteanu, Nicoleta Măru, and et al. 2024. "An Assessment of Behavioral Risk Factors in Oncology Patients" Nutrients 16, no. 15: 2527. https://doi.org/10.3390/nu16152527