
The Risk of Malnutrition and Sarcopenia in Elderly People Living with HIV during the COVID-19 Pandemic

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Assessments
2.2.1. Nutritional Status
2.2.2. Body Composition
2.2.3. Physical Performance
2.2.4. Sociodemographic Characteristics and HIV-Related Characteristics
2.3. Statistical Analysis
3. Results
3.1. Nutritional Status
3.2. Body Composition
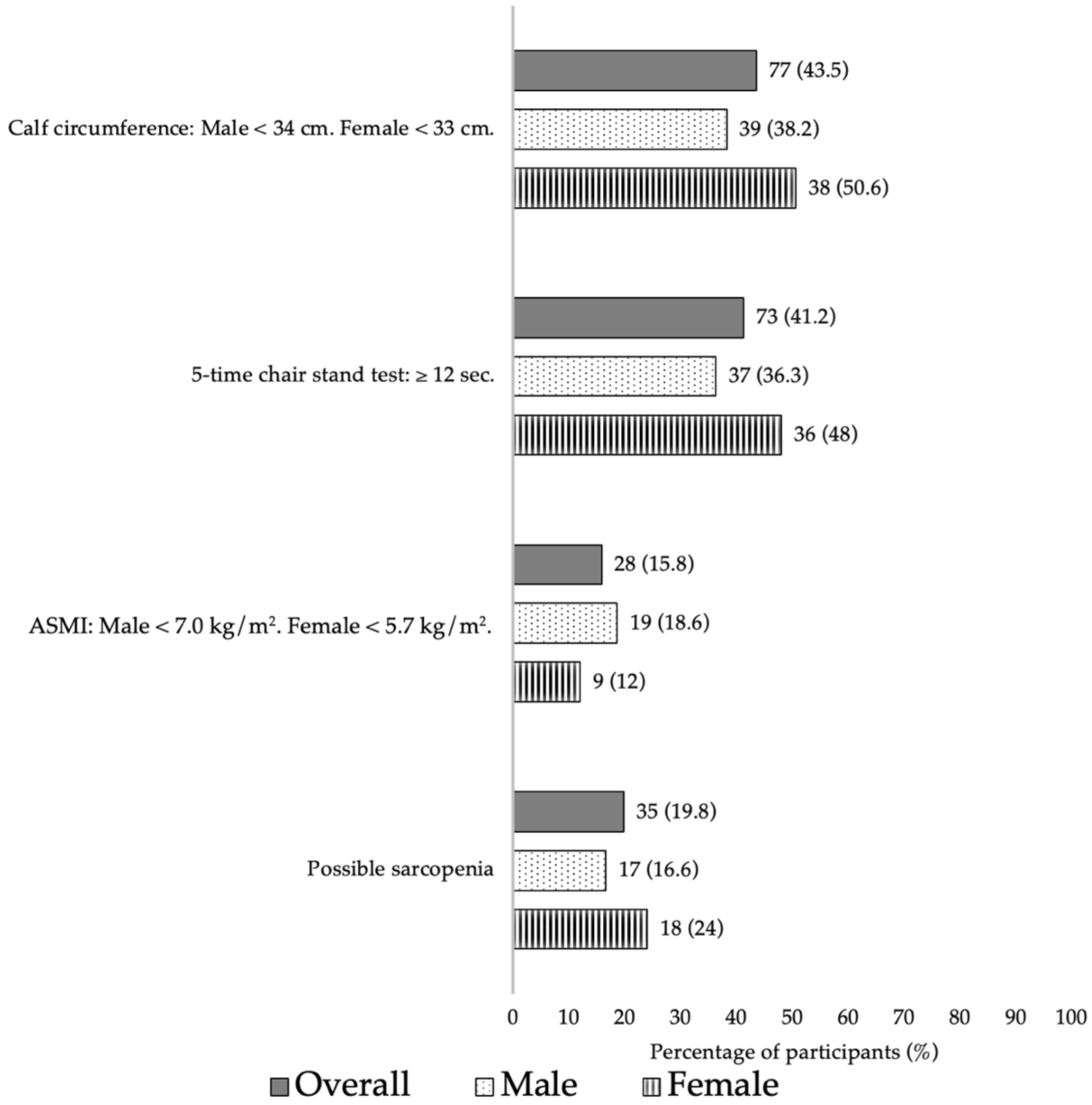
3.3. Physical Performance
3.4. Correlation and Association of Total Muscle Mass with Nutritional Status and Physical Performance
3.5. Prevalence of “At-Risk” Sarcopenia
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ssentongo, P.; Heilbrunn, E.S.; Ssentongo, A.E.; Advani, S.; Chinchilli, V.M.; Nunez, J.J.; Du, P. Epidemiology and outcomes of COVID-19 in HIV-infected individuals: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 6283. [Google Scholar] [CrossRef]
- Antwi, J.; Appiah, B.; Oluwakuse, B.; Abu, B.A.Z. The nutrition-COVID-19 interplay: A review. Curr. Nutr. Rep. 2021, 10, 364–374. [Google Scholar] [CrossRef]
- Hawkins, K.L.; Brown, T.T.; Margolick, J.B.; Erlandson, K.M. Geriatric syndromes: New frontiers in HIV and sarcopenia. AIDS 2017, 31 (Suppl. S2), S137–S146. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Camprubi-Robles, M.; Bear, D.E.; Cederholm, T.; Malafarina, V.; Welch, A.A.; Cruz-Jentoft, A.J. Muscle loss: The new malnutrition challenge in clinical practice. Clin. Nutr. 2019, 38, 2113–2120. [Google Scholar] [CrossRef]
- Russell, M.L.; Justice, A. Human Immunodeficiency Virus in Older Adults. Clin. Geriatr. Med. 2024, 40, 285–298. [Google Scholar] [CrossRef]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Demling, R.H. Nutrition, anabolism, and the wound healing process: An overview. Eplasty 2009, 9, e9. [Google Scholar]
- Tsai, A.C.; Ho, C.S.; Chang, M.C. Assessing the prevalence of malnutrition with the Mini Nutritional Assessment (MNA) in a nationally representative sample of elderly Taiwanese. J. Nutr. Health Aging 2008, 12, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Thet, D.; Siritientong, T.; Sangarlangkarn, A.; Lwin, H.M.S.; Phonphithak, S.; Apornpong, T.; Avihingsanon, A. Deterioration of nutritional status and its negative association with depression among older HIV-infected Asian population: A four-year longitudinal study. AIDS Res. Hum. Retroviruses 2022, 38, 592–600. [Google Scholar] [CrossRef]
- Li, X.; Wang, R.; Hou, Z.; Sun, Q. Urban-rural differences in the prevalence and associated factors of sarcopenia: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2024, 122, 105390. [Google Scholar] [CrossRef]
- Limpawattana, P.; Kotruchin, P.; Pongchaiyakul, C. Sarcopenia in Asia. Osteoporos. Sarcopenia 2015, 1, 92–97. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef] [PubMed]
- Vanitcharoenkul, E.; Unnanuntana, A.; Chotiyarnwong, P.; Laohaprasitiporn, P.; Adulkasem, N.; Asavamongkolkul, A.; Chandhanayingyong, C. Sarcopenia in Thai community-dwelling older adults: A national, cross-sectional, epidemiological study of prevalence and risk factors. BMC Public Health 2024, 24, 311. [Google Scholar] [CrossRef] [PubMed]
- Luk, F.W.L.; Li, T.; Ho, H.Y.; Chan, Y.Y.; Cheung, S.K.; Wong, V.; Kwok, T.C.Y.; Lui, G. Sarcopenia in people living with HIV in Hong Kong: Which definition correlates with health outcomes? J. Int. AIDS Soc. 2022, 25 (Suppl. S4), e25988. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.H.; Chen, K.T.; Hou, M.T.; Chang, Y.F.; Chang, C.S.; Liu, P.Y.; Wu, S.J.; Chiu, C.J.; Jou, I.M.; Chen, C.Y. Prevalence and associated factors of sarcopenia and severe sarcopenia in older Taiwanese living in rural community: The Tianliao Old People study 04. Geriatr. Gerontol. Int. 2014, 14 (Suppl. S1), 69–75. [Google Scholar] [CrossRef]
- Oliveira, V.H.F.; Webel, A.R.; Borsari, A.L.; Cárdenas, J.D.G.; Deminice, R. Health and sociodemographic factors associated with low muscle strength, muscle mass, and physical performance among people living with HIV. AIDS Care 2023, 35, 1863–1873. [Google Scholar] [CrossRef] [PubMed]
- Yuenyongchaiwat, K.; Chamnansingh, C.; Akekawatchai, C. Investigating the contributing risk factors toward sarcopenia prevalence and its development in human immunodeficiency virus (HIV) patients. Open Public Health J. 2024, 17, e18749445288299. [Google Scholar] [CrossRef]
- Nishimura, T.; Arima, K.; Okabe, T.; Mizukami, S.; Tomita, Y.; Kanagae, M.; Goto, H.; Horiguchi, I.; Abe, Y.; Aoyagi, K. Usefulness of chair stand time as a surrogate of gait speed in diagnosing sarcopenia. Geriatr. Gerontol. Int. 2017, 17, 659–661. [Google Scholar] [CrossRef] [PubMed]
- Zong, M.; Zhao, A.; Han, W.; Chen, Y.; Weng, T.; Li, S.; Tang, L.; Wu, J. Sarcopenia, sarcopenic obesity and the clinical outcome of the older inpatients with COVID-19 infection: A prospective observational study. BMC Geriatr. 2024, 24, 578. [Google Scholar] [CrossRef]
- Vasconcelos, L.G.L.; Me Mpomo, J.S.V.d.M.; Macena, M.d.L.; De Souza, T.O.M.; Dias, C.d.A.; Vasconcelos, S.M.L.; Ribeiro-Andrade, M.; Barros-Neto, J.A. Sarcopenia and risk of malnutrition as risk factors for complications from COVID-19. Medicina 2023, 56, e-206364. [Google Scholar] [CrossRef]
- Bahat, G.; Saka, B.; Tufan, F.; Akin, S.; Sivrikaya, S.; Yucel, N.; Erten, N.; Karan, M.A. Prevalence of sarcopenia and its association with functional and nutritional status among male residents in a nursing home in Turkey. Aging Male 2010, 13, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Tramontano, A.; Veronese, N.; Giantin, V.; Manzato, E.; Rodriguez-Hurtado, D.; Trevisan, C.; De Zaiacomo, F.; Sergi, G. Nutritional status, physical performance and disability in the elderly of the Peruvian Andes. Aging Clin. Exp. Res. 2016, 28, 1195–1201. [Google Scholar] [CrossRef] [PubMed]
- Neves, T.; Fett, C.A.; Ferriolli, E.; Crespilho Souza, M.G.; Dos Reis Filho, A.D.; Martin Lopes, M.B.; Carraro Martins, N.M.; Rezende Fett, W.C. Correlation between muscle mass, nutritional status and physical performance of elderly people. Osteoporos. Sarcopenia 2018, 4, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Heymsfield, S.B.; Wang, Z.M.; Ross, R. Skeletal muscle mass and distribution in 468 men and women aged 18–88 yr. J. Appl. Physiol. 2000, 89, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Yarasheski, K.E.; Scherzer, R.; Kotler, D.P.; Dobs, A.S.; Tien, P.C.; Lewis, C.E.; Kronmal, R.A.; Heymsfield, S.B.; Bacchetti, P.; Grunfeld, C. Age-related skeletal muscle decline is similar in HIV-infected and uninfected individuals. J. Gerontol. A Biol. Sci. Med. Sci. 2011, 66, 332–340. [Google Scholar] [CrossRef]
- Wasserman, P.; Segal-Maurer, S.; Rubin, D.S. High prevalence of low skeletal muscle mass associated with male gender in midlife and older HIV-infected persons despite CD4 cell reconstitution and viral suppression. J. Int. Assoc. Provid. AIDS Care 2014, 13, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.; Li, F.; Chen, X. Factors affecting mortality in elderly hypertensive hospitalized patients with COVID-19: A retrospective study. Clin. Interv. Aging 2023, 18, 1905–1921. [Google Scholar] [CrossRef]
- World Health Organization; Regional Office for the Western Pacific. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia: Sydney, Australia, 2000. [Google Scholar]
- Iannuzzi-Sucich, M.; Prestwood, K.M.; Kenny, A.M. Prevalence of sarcopenia and predictors of skeletal muscle mass in healthy, older men and women. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, M772–M777. [Google Scholar] [CrossRef]
- Yalcin, A.; Aras, S.; Atmis, V.; Cengiz, O.K.; Varli, M.; Cinar, E.; Atli, T. Sarcopenia prevalence and factors associated with sarcopenia in older people living in a nursing home in Ankara Turkey. Geriatr. Gerontol. Int. 2016, 16, 903–910. [Google Scholar] [CrossRef]
- Landi, F.; Liperoti, R.; Fusco, D.; Mastropaolo, S.; Quattrociocchi, D.; Proia, A.; Russo, A.; Bernabei, R.; Onder, G. Prevalence and risk factors of sarcopenia among nursing home older residents. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 48–55. [Google Scholar] [CrossRef]
- Du, Y.; Wang, X.; Xie, H.; Zheng, S.; Wu, X.; Zhu, X.; Zhang, X.; Xue, S.; Li, H.; Hong, W.; et al. Sex differences in the prevalence and adverse outcomes of sarcopenia and sarcopenic obesity in community dwelling elderly in East China using the AWGS criteria. BMC Endocr. Disord. 2019, 19, 109. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | Male (n = 102) | Female (n = 75) | p-Value * |
|---|---|---|---|---|
| Age (years), median (IQR) | 58.00 (55.00–62.00) | 58.00 (55.00–61.25) | 58.00 (56.00–62.00) | 0.301 |
| Marital status, n (%) | <0.001 | |||
| Single | 42 (23.7) | 36 (35.3) | 6 (8) | |
| Married | 53 (29.9) | 36 (35.3) | 17 (22.7) | |
| Other | 82 (46.4) | 30 (29.4) | 52 (69.3) | |
| Occupation, n (%) | 0.046 | |||
| Employed | 140 (79.1) | 86 (84.3) | 54 (72) | |
| Unemployed | 37 (20.9) | 16 (15.7) | 21 (28) | |
| Drinking, n (%) | 0.001 | |||
| Yes | 36 (20.3) | 29 (28.4) | 7 (9.3) | |
| No | 141 (79.7) | 73 (71.6) | 68 (90.7) | |
| Smoking, n (%) | 0.001 | |||
| Yes | 18 (10.2) | 17 (16.7) | 1 (1.3) | |
| No | 159 (89.8) | 85 (83.3) | 74 (98.7) | |
| Exercise, n (%) | 0.641 | |||
| Yes | 98 (55.4) | 58 (56.9) | 40 (53.3) | |
| No | 79 (44.6) | 44 (43.1) | 35 (46.7) | |
| Anthropometric data, median (IQR) | ||||
| Height (cm) | 163.00 (155.50–170.00) | 168.00 (165.00–171.25) | 155.00 (150.00–159.00) | <0.001 |
| Body weight (kg) | 60.40 (53.80–68.35) | 65.05 (57.97–73.20) | 56.80 (50.10–60.40) | <0.001 |
| Mid-arm circumference (cm) | 27.00 (25.00–28.00) | 27.00 (25.00–28.00) | 26.50 (25.00–28.50) | 0.733 |
| Calf circumference (cm) | 33.50 (31.00–36.00) | 34.50 (32.95–36.62) | 32.00 (30.00–35.00) | <0.001 |
| Waist circumference (cm) | 86.00 (80.00–92.00) | 88.00 (81.00–93.25) | 84.00 (78.00–90.00) | 0.039 |
| Hip circumference (cm) | 94.00 (89.00–98.00) | 94.00 (89.00–98.00) | 95.00 (89.00–99.00) | 0.479 |
| Waist/hip ratio | 0.92 (0.86–0.96) | 0.94 (0.88–0.97) | 0.88 (0.84–0.94) | <0.001 |
| Muscle mass (kg) | 45.10 (38.30–53.05) | 51.25 (47.17–56.92) | 37.70 (35.20–40.60) | <0.001 |
| Fat mass (kg) | 15.20 (11.30–19.55) | 12.95 (9.90–18.02) | 17.80 (14.70–21.30) | <0.001 |
| Fat (%) | 25.10 (19.25–31.80) | 19.90 (16.75–25.10) | 32.10 (27.50–35.20) | <0.001 |
| Visceral fat rating | 9.00 (6.50–11.00) | 10.00 (8.00–12.00) | 7.00 (6.00–8.00) | <0.001 |
| Total body water (kg) | 33.00 (28.05–38.85) | 37.55 (34.57–41.65) | 27.60 (25.80–29.70) | <0.001 |
| Body mass index (kg/m2) | 23.30 (20.80–25.65) | 23.25 (20.80–25.52) | 22.00 (18.00–26.00) | 0.778 |
| Duration of HIV infection (years), median (IQR) | 23.00 (19.00–25.00) | 23.00 (19.00–25.00) | 22.00 (18.00–26.00) | 0.878 |
| Duration of ART (years), median (IQR) | 20.00 (16.00–23.00) | 20.00 (15.75–23.00) | 20.00 (16.00–23.00) | 0.927 |
| ART regimens, n (%) | 0.100 | |||
| NNRTI-based regimen | 109 (61.6) | 59 (57.8) | 50 (66.7) | |
| INSTI-based regimen | 33 (18.6) | 17 (16.7) | 16 (21.3) | |
| PI-based regimen | 31 (17.5) | 22 (21.6) | 9 (12) | |
| Other | 4 (2.3) | 4 (3.9) | 0 (0) | |
| Number of comorbidities, median (IQR) | 4.00 (2.00–5.00) | 4.00 (2.00–5.00) | 4.00 (3.00–5.00) | 0.453 |
| Types of comorbidities | ||||
| Hypertension | 72 (40.7) | 48 (47.1) | 24 (32) | 0.044 |
| Diabetes | 31 (17.5) | 25 (24.5) | 6 (8) | 0.005 |
| Lipodystrophy | 79 (44.6) | 45 (44.1) | 34 (45.3) | 0.872 |
| Osteoporosis | 6 (3.4) | 1 (1) | 5 (6.7) | 0.084 |
| Laboratory data, median (IQR) | ||||
| CD4 (cells/mm3) | 633.00 (474.50–777.50) | 574.50 (420.75–741.25) | 685.00 (540.00–840.00) | <0.001 |
| Albumin (g/dL) | 4.40 (4.08–4.60) | 4.40 (4.10–4.70) | 4.30 (4.00–4.50) | 0.059 |
| Hemoglobin (g/dL) | 14.10 (13.00–15.00) | 14.70 (13.87–15.80) | 13.30 (12.60–14.10) | <0.001 |
| Creatinine (mg/dL) | 0.93 (0.78–1.08) | 1.01 (0.93–1.15) | 0.78 (0.70–0.87) | <0.001 |
| AST (U/L) | 26.00 (21.00–30.50) | 27.00 (21.00–31.00) | 24.00 (20.00–30.00) | 0.083 |
| ALT (U/L) | 27.00 (20.50–38.00) | 28.50 (22.00–42.00) | 26.00 (18.00–34.00) | 0.059 |
| hs-CRP (mg/L) | 0.10 (0.05–0.25) | 0.09 (0.05–0.24) | 0.11 (0.05–0.25) | 0.608 |
| Insulin (μU/mL) | 6.90 (4.65–10.40) | 6.70 (4.47–10.00) | 7.20 (5.00–11.70) | 0.289 |
| Glucose (mg/dL) | 96.00 (87.00–106.00) | 98.50 (91.00–112.25) | 92.00 (85.00–101.00) | <0.001 |
| Triglycerides (mg/dL) | 120.00 (84.00–176.50) | 129.00 (84.00–193.50) | 111.00 (80.00–149.00) | 0.014 |
| LDL (mg/dL) | 126.50 (100.75–127.00) | 122.50 (95.87–143.15) | 134.35 (108.45–154.25) | 0.091 |
| HDL (mg/dL) | 49.00 (40.00–58.00) | 44.00 (38.00–55.00) | 54.00 (45.00–63.00) | <0.001 |
| Duration of CST (second), median (IQR) | 11.00 (9.00–13.00) | 10.00 (8.00–13.00) | 11.00 (9.00–14.00) | 0.027 |
| MNA scores, median (IQR) | 25.50 (23.50–27.00) | 26.00 (24.00–27.50) | 24.50 (23.50–27.00) | 0.024 |
| Nutritional status, n (%) | ||||
| Normal nutritional status | 127 (71.8) | 79 (77.4) | 48 (64) | 0.143 |
| At risk of malnutrition | 46 (26) | 21 (20.6) | 25 (33.3) | |
| Malnourished | 4 (2.2) | 2 (2) | 2 (2.7) |
| Nutritional Scores | Muscle Mass | Duration of 5-Time CST | |
|---|---|---|---|
| Age (years) | −0.155 a | −0.241 b | 0.102 |
| BMI (kg/m2) | 0.491 c | 0.438 c | 0.056 |
| Duration of HIV (years) | −0.135 | 0.019 | −0.202 b |
| Duration of ART (years) | −0.139 | −0.051 | −0.146 |
| Number of comorbidities | −0.207 b | −0.084 | −0.003 |
| CD4 (cells/mm3) | 0.070 | −0.187 a | 0.086 |
| Nutritional scores | - | 0.355 c | −0.061 |
| Muscle mass (kg) | 0.355 c | - | −0.173 a |
| Duration of 5-time CST (second) | −0.061 | −0.173 a | - |
| Bivariable Analysis | Multivariable Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| Coefficient | 95% Confidence Interval | p-Value | Coefficient | 95% Confidence Interval | p-Value | |||
| Age (years) | −0.45 | −0.71 | −0.18 | 0.001 | −0.17 | −0.28 | −0.07 | 0.002 |
| Sex (female vs. male) | −14.41 | −16.32 | −12.50 | <0.001 | −11.16 | −12.62 | −9.70 | <0.001 |
| Calf circumference (cm) | 2.19 | 1.88 | 2.51 | <0.001 | 1.1 | 0.81 | 1.38 | <0.001 |
| Mid-arm circumference (cm) | 1.46 | 1.05 | 1.87 | <0.001 | 0.73 | 0.43 | 1.02 | <0.001 |
| Duration of 5-time CST (sec) | −0.49 | −0.91 | −0.08 | 0.021 | −0.18 | −0.34 | −0.03 | 0.015 |
| CD4 by 100 (cells/mm3) | −0.76 | −1.35 | −0.16 | 0.013 | −0.01 | −0.22 | 0.20 | 0.921 |
| Glucose (mg/dL) | 0.07 | 0.03 | 0.12 | 0.002 | 0.01 | −0.02 | 0.03 | 0.600 |
| HDL (mg/dL) | −0.24 | −0.34 | −0.14 | <0.001 | −0.02 | −0.07 | 0.03 | 0.417 |
| Hemoglobin (g/dL) | 2.14 | 1.28 | 3.01 | <0.001 | 0.05 | −0.46 | 0.57 | 0.841 |
| Nutritional scores | 1.13 | 0.68 | 1.57 | <0.001 | −0.14 | −0.37 | 0.10 | 0.248 |
| Characteristics | Sarcopenic (n = 35) | Non-Sarcopenic (n = 142) | p-Value |
|---|---|---|---|
| Sex, n (%) | 0.255 | ||
| Male | 17 (48.6) | 85 (59.9) | |
| Female | 18 (51.4) | 57 (40.1) | |
| Age (years), median (IQR) | 59 (57.00–63.00) | 57 (55.00–62.00) | 0.033 |
| BMI (kg/m2), median (IQR) | 20.80 (19.40–23.30) | 23.70 (21.50–25.80) | <0.001 |
| Exercise, n (%) | 0.448 | ||
| Yes | 17 (48.6) | 81 (57) | |
| No | 18 (51.4) | 61 (43) | |
| Diabetes, n (%) | 7 (20) | 24 (16.9) | 0.628 |
| Hypertension, n (%) | 13 (37.1) | 59 (41.5) | 0.703 |
| Lipodystrophy, n (%) | 17 (48.6) | 62 (43.7) | 0.705 |
| Duration of HIV infection (years), median (IQR) | 22 (18–25) | 23 (19–25) | 0.664 |
| Duration of ART (years), median (IQR) | 20 (17.00–23.00) | 20 (15.75–23.00) | 0.718 |
| CD4 (cells/mm3), median (IQR) | 675 (484.00–851.00) | 623 (470.50–776.75) | 0.668 |
| Nutritional scores, median (IQR) | 25.00 (22.50–27.00) | 25.50 (23.50–27.50) | 0.050 |
| Nutritional status, n (%) | 0.096 | ||
| Normal nutritional status | 21 (60) | 106 (74.6) | |
| Abnormal nutritional status | 14 (40) | 36 (25.4) | |
| Body weight (kg) | 54.70 (49.20–60.40) | 62.55 (56.52–70.52) | <0.001 |
| Waist circumference (cm) | 84.00 (75.00–87.00) | 87.50 (81.00–94.00) | 0.005 |
| Hip circumference (cm) | 89.00 (88.00–95.00) | 95.00 (90.00–99.00) | <0.001 |
| Mid-arm circumference (cm) | 25.00 (23.00–27.00) | 27.00 (25.00–29.00) | <0.001 |
| Calf circumference (cm) | 31.00 (30.00–32.50) | 34.25 (32.50–36.00) | <0.001 |
| Fat % | 23.70 (19.30–32.10) | 25.60 (19.12–31.80) | 0.879 |
| Fat mass (kg) | 13.00 (10.10–17.00) | 16.30 (11.80–19.85) | 0.048 |
| Muscle mass (kg) | 37.70 (35.20–47.10) | 46.75 (39.77–54.52) | <0.001 |
| Total body water (kg) | 27.60 (25.80–34.50) | 34.20 (29.10–39.92) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thet, D.; Lappichetpaiboon, S.; Trakultritrung, C.; Sotangkur, N.; Phonphithak, S.; Lwin, H.M.S.; Apornpong, T.; Han, W.M.; Avihingsanon, A.; Siritientong, T. The Risk of Malnutrition and Sarcopenia in Elderly People Living with HIV during the COVID-19 Pandemic. Nutrients 2024, 16, 2540. https://doi.org/10.3390/nu16152540
Thet D, Lappichetpaiboon S, Trakultritrung C, Sotangkur N, Phonphithak S, Lwin HMS, Apornpong T, Han WM, Avihingsanon A, Siritientong T. The Risk of Malnutrition and Sarcopenia in Elderly People Living with HIV during the COVID-19 Pandemic. Nutrients. 2024; 16(15):2540. https://doi.org/10.3390/nu16152540
Chicago/Turabian StyleThet, Daylia, Sawitee Lappichetpaiboon, Chidchanok Trakultritrung, Nongnapas Sotangkur, Supalak Phonphithak, Hay Mar Su Lwin, Tanakorn Apornpong, Win Min Han, Anchalee Avihingsanon, and Tippawan Siritientong. 2024. "The Risk of Malnutrition and Sarcopenia in Elderly People Living with HIV during the COVID-19 Pandemic" Nutrients 16, no. 15: 2540. https://doi.org/10.3390/nu16152540