Cholelithiasis, Gut Microbiota and Bile Acids after Bariatric Surgery—Can Cholelithiasis Be Prevented by Modulating the Microbiota? A Literature Review

 ,
,
Abstract
1. Introduction
2. Methods
3. Historical Overview of Bariatric Surgery
4. Etiopathogenesis of Cholelithiasis in General Population
5. Factors That Favor the Development of Cholelithiasis after Bariatric Surgery
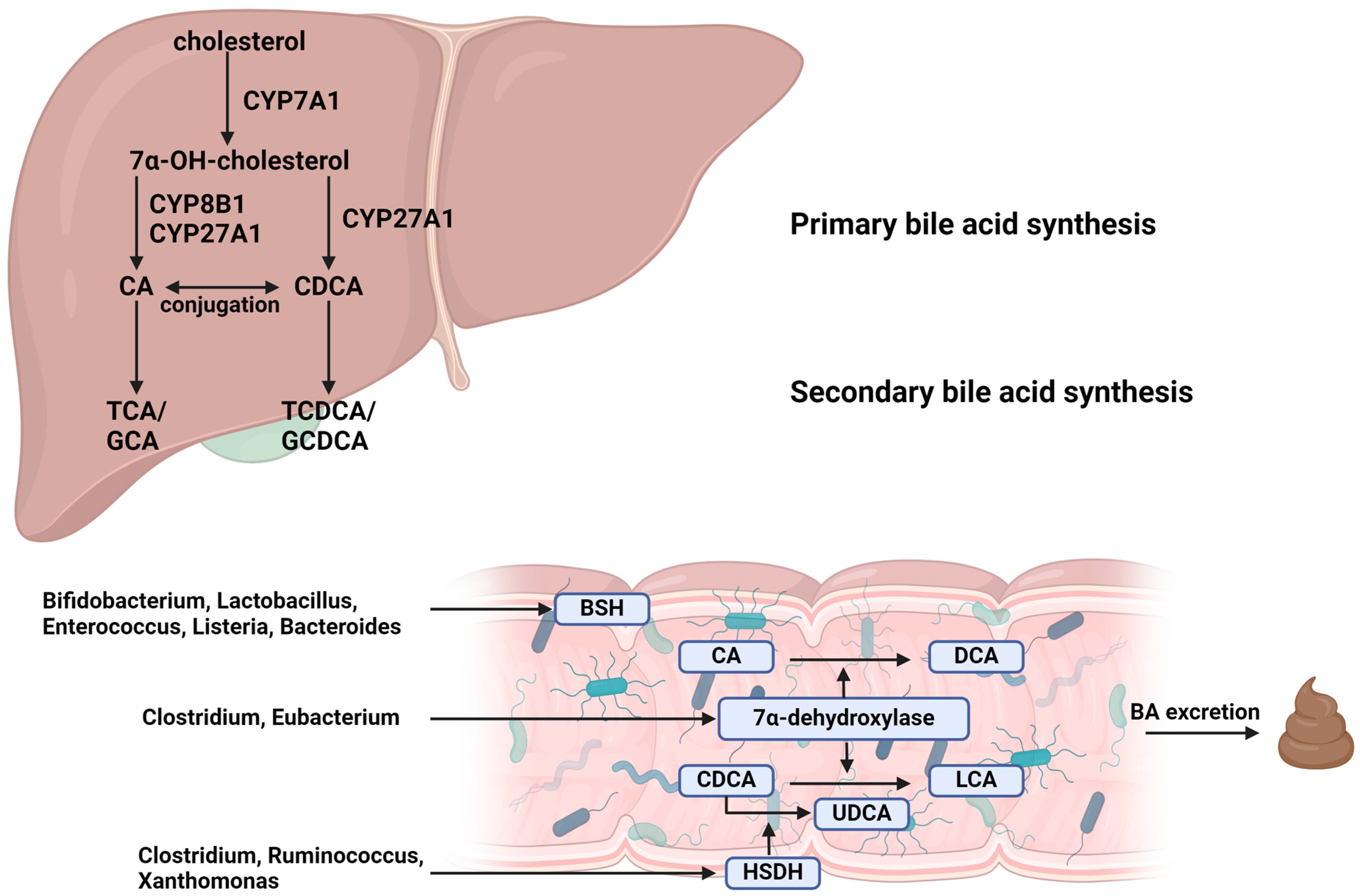
6. Microbial Modification of Bile Acids
- Farnesoid X receptor (FXR): activated by bile acids, FXR can regulate the expression of genes involved in bile acid synthesis, transport and excretion. It helps reduce BA synthesis in the liver and increases their excretion from the body.
- Takeda G protein-coupled Receptor 5 (TGR5): secondary bile acids, such as LCA and DCA, are potent activators of TGR5, which plays a role in energy metabolism and inflammatory reactions.
- Dysbiosis: imbalances in the gut microbiota can lead to an increase in harmful secondary bile acids, such as DCA and LCA, which have been linked to promoting liver inflammation, damage and carcinogenesis.
7. Microbiota, Bile Acids and Cholelithiasis
8. Microbiota and Bile Acid Changes after Bariatric Surgery
9. Microbiota Modulation and Fecal Microbiota Transplantation in the Context of Gut–Liver Axis
10. Conclusions
Funding
Conflicts of Interest
References
- Iglézias Brandão de Oliveira, C.; Adami Chaim, E.; da Silva, B.B. Impact of Rapid Weight Reduction on Risk of Cholelithiasis after Bariatric Surgery. Obes. Surg. 2003, 13, 625–628. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, E.A. Epidemiology of Gallbladder Stone Disease. Best Pract. Res. Clin. Gastroenterol. 2006, 20, 981–996. [Google Scholar] [CrossRef] [PubMed]
- Lazarchuk, I.; Barzak, B.; Wozniak, S.; Mielczarek, A.; Lazarchuk, V. Cholelithiasis—A Particular Threat to Women. A Review of Risk Factors. Med. J. Cell Biol. 2023, 11, 20–27. [Google Scholar] [CrossRef]
- Acalovschi, M. Cholesterol Gallstones: From Epidemiology to Prevention. Postgrad. Med. J. 2001, 77, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.; Corcelles, R.; Boules, M.; Jamal, M.H.; Schauer, P.R.; Kroh, M.D. Predictive Factors of Biliary Complications after Bariatric Surgery. Surg. Obes. Relat. Dis. 2016, 12, 1706–1710. [Google Scholar] [CrossRef] [PubMed]
- Guzmán, H.M.; Sepúlveda, M.; Rosso, N.; San Martin, A.; Guzmán, F.; Guzmán, H.C. Incidence and Risk Factors for Cholelithiasis After Bariatric Surgery. Obes. Surg. 2019, 29, 2110–2114. [Google Scholar] [CrossRef]
- Li, V.K.M.; Pulido, N.; Fajnwaks, P.; Szomstein, S.; Rosenthal, R.; Martinez-Duartez, P. Predictors of Gallstone Formation after Bariatric Surgery: A Multivariate Analysis of Risk Factors Comparing Gastric Bypass, Gastric Banding, and Sleeve Gastrectomy. Surg. Endosc. 2009, 23, 1640–1644. [Google Scholar] [CrossRef] [PubMed]
- Talha, A.; Abdelbaki, T.; Farouk, A.; Hasouna, E.; Azzam, E.; Shehata, G. Cholelithiasis after Bariatric Surgery, Incidence, and Prophylaxis: Randomized Controlled Trial. Surg. Endosc. 2020, 34, 5331–5337. [Google Scholar] [CrossRef]
- Wang, W.; Cheng, Z.; Wang, Y.; Dai, Y.; Zhang, X.; Hu, S. Role of Bile Acids in Bariatric Surgery. Front. Physiol. 2019, 10, 374. [Google Scholar] [CrossRef]
- Liu, B.-N.; Liu, X.-T.; Liang, Z.-H.; Wang, J.-H. Gut Microbiota in Obesity. World J. Gastroenterol. 2021, 27, 3837–3850. [Google Scholar] [CrossRef]
- Dan, W.-Y.; Yang, Y.-S.; Peng, L.-H.; Sun, G.; Wang, Z.-K. Gastrointestinal Microbiome and Cholelithiasis: Current Status and Perspectives. World J. Gastroenterol. 2023, 29, 1589–1601. [Google Scholar] [CrossRef] [PubMed]
- Haththotuwa, R.N.; Wijeyaratne, C.N.; Senarath, U. Chapter 1—Worldwide Epidemic of Obesity. In Obesity and Obstetrics, 2nd ed.; Mahmood, T.A., Arulkumaran, S., Chervenak, F.A., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 3–8. ISBN 978-0-12-817921-5. [Google Scholar]
- Ruban, A.; Stoenchev, K.; Ashrafian, H.; Teare, J. Current Treatments for Obesity. Clin. Med. 2019, 19, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, D.; Shikora, S.A.; Aarts, E.; Aminian, A.; Angrisani, L.; Cohen, R.V.; de Luca, M.; Faria, S.L.; Goodpaster, K.P.S.; Haddad, A.; et al. 2022 American Society of Metabolic and Bariatric Surgery (ASMBS) and International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO) Indications for Metabolic and Bariatric Surgery. Obes. Surg. 2023, 33, 3–14. [Google Scholar] [CrossRef]
- Wyleżoł, M.; Paśnik, K.; Dąbrowiecki, S.; Głuszek, S.; Michalik, M.; Strzelczyk, J.; Wierzbicki, Z.; Kwiatkowski, A.; Stanowski, E. Polish Recommendations for Bariatric Surgery. Videosurg. Miniinvasive 2009, 2009, 8. [Google Scholar]
- Gumbs, A.A.; Gagner, M.; Dakin, G.; Pomp, A. Sleeve Gastrectomy for Morbid Obesity. Obes. Surg. 2007, 17, 962–969. [Google Scholar] [CrossRef]
- Benaiges, D.; Más-Lorenzo, A.; Goday, A.; Ramon, J.M.; Chillarón, J.J.; Pedro-Botet, J.; Roux, J.A.F.-L. Laparoscopic Sleeve Gastrectomy: More than a Restrictive Bariatric Surgery Procedure? World J. Gastroenterol. 2015, 21, 11804–11814. [Google Scholar] [CrossRef]
- Langer, F.B.; Reza Hoda, M.A.; Bohdjalian, A.; Felberbauer, F.X.; Zacherl, J.; Wenzl, E.; Schindler, K.; Luger, A.; Ludvik, B.; Prager, G. Sleeve Gastrectomy and Gastric Banding: Effects on Plasma Ghrelin Levels. Obes. Surg. 2005, 15, 1024–1029. [Google Scholar] [CrossRef] [PubMed]
- Wiggins, T.; Majid, M.S.; Agrawal, S. From the Knife to the Endoscope-a History of Bariatric Surgery. Curr. Obes. Rep. 2020, 9, 315–325. [Google Scholar] [CrossRef]
- Zuegel, N.P.; Lang, R.A.; Hüttl, T.P.; Gleis, M.; Ketfi-Jungen, M.; Rasquin, I.; Kox, M. Complications and Outcome after Laparoscopic Bariatric Surgery: LAGB versus LRYGB. Langenbecks Arch. Surg. 2012, 397, 1235–1241. [Google Scholar] [CrossRef]
- Deitel, M. History of the MGB and OAGB Operations. Int. J. Surg. 2019, 66, 79–83. [Google Scholar] [CrossRef]
- Carbajo, M.; García-Caballero, M.; Toledano, M.; Osorio, D.; García-Lanza, C.; Carmona, J.A. One-Anastomosis Gastric Bypass by Laparoscopy: Results of the First 209 Patients. Obes. Surg. 2005, 15, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Alalwan, A.A.; Friedman, J.; Park, H.; Segal, R.; Brumback, B.A.; Hartzema, A.G. US National Trends in Bariatric Surgery: A Decade of Study. Surgery 2021, 170, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.W.; Weir, C.B.; Ghassemzadeh, S. Gallstones (Cholelithiasis). In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Chen, L.; Yang, H.; Li, H.; He, C.; Yang, L.; Lv, G. Insights into Modifiable Risk Factors of Cholelithiasis: A Mendelian Randomization Study. Hepatology 2022, 75, 785–796. [Google Scholar] [CrossRef] [PubMed]
- Lammert, F.; Gurusamy, K.; Ko, C.W.; Miquel, J.-F.; Méndez-Sánchez, N.; Portincasa, P.; van Erpecum, K.J.; van Laarhoven, C.J.; Wang, D.Q.-H. Gallstones. Nat. Rev. Dis. Primers 2016, 2, 16024. [Google Scholar] [CrossRef]
- Littlefield, A.; Lenahan, C. Cholelithiasis: Presentation and Management. J. Midwifery Womens Health 2019, 64, 289–297. [Google Scholar] [CrossRef]
- Sun, H.; Warren, J.; Yip, J.; Ji, Y.; Hao, S.; Han, W.; Ding, Y. Factors Influencing Gallstone Formation: A Review of the Literature. Biomolecules 2022, 12, 550. [Google Scholar] [CrossRef]
- Monkhouse, S.; Morgan, J.; Norton, S. Complications of Bariatric Surgery: Presentation and Emergency Management—A Review. Ann. R. Coll. Surg. Engl. 2009, 91, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Amorim-Cruz, F.; Santos-Sousa, H.; Ribeiro, M.; Nogueiro, J.; Pereira, A.; Resende, F.; Costa-Pinho, A.; Preto, J.; Lima-da-Costa, E.; Sousa-Pinto, B. Risk and Prophylactic Management of Gallstone Disease in Bariatric Surgery: A Systematic Review and A Bayesian Meta-Analysis. J. Gastrointest. Surg. 2023, 27, 433–448. [Google Scholar] [CrossRef]
- Manatsathit, W.; Leelasinjaroen, P.; Al-Hamid, H.; Szpunar, S.; Hawasli, A. The Incidence of Cholelithiasis after Sleeve Gastrectomy and Its Association with Weight Loss: A Two-Centre Retrospective Cohort Study. Int. J. Surg. 2016, 30, 13–18. [Google Scholar] [CrossRef]
- Andrés-Imaz, A.; Martí-Gelonch, L.; Eizaguirre-Letamendia, E.; Asensio-Gallego, J.I.; Enríquez-Navascués, J.M. Incidence and Risk Factors for de Novo Cholelithiasis after Bariatric Surgery. Cir. Esp. 2021, 99, 648–654. [Google Scholar] [CrossRef]
- Desbeaux, A.; Hec, F.; Andrieux, S.; Fayard, A.; Bresson, R.; Pruvot, M.-H.; Mulliez, E. Risk of Biliary Complications in Bariatric Surgery. J. Visc. Surg. 2010, 147, e217–e220. [Google Scholar] [CrossRef] [PubMed]
- Boerlage, T.C.C.; Haal, S.; Maurits de Brauw, L.; Acherman, Y.I.Z.; Bruin, S.; van de Laar, A.W.J.M.; Moes, D.E.; van Wagensveld, B.A.; de Vries, C.E.E.; van Veen, R.; et al. Ursodeoxycholic Acid for the Prevention of Symptomatic Gallstone Disease after Bariatric Surgery: Study Protocol for a Randomized Controlled Trial (UPGRADE Trial). BMC Gastroenterol. 2017, 17, 164. [Google Scholar] [CrossRef]
- Dai, Y.; Luo, B.; Li, W. Incidence and Risk Factors for Cholelithiasis after Bariatric Surgery: A Systematic Review and Meta-Analysis. Lipids Health Dis. 2023, 22, 5. [Google Scholar] [CrossRef]
- Wan, Q.; Zhao, R.; Chen, Y.; Wang, Y.; Wu, Y.; Wu, X. Comparison of the Incidence of Cholelithiasis after Sleeve Gastrectomy and Roux-En-Y Gastric Bypass: A Meta-Analysis. Surg. Obes. Relat. Dis. 2021, 17, 1198–1205. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Lau, H.C.; Zhang, X.; Yu, J. Bile Acids, Gut Microbiota, and Therapeutic Insights in Hepatocellular Carcinoma. Cancer Biol. Med. 2024, 21, 144–162. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Gu, Y.; Li, L.; Liu, T.; Song, X.; Sun, Y.; Cao, X.; Wang, B.; Jiang, K.; Cao, H. Bile Acid–Gut Microbiota Axis in Inflammatory Bowel Disease: From Bench to Bedside. Nutrients 2021, 13, 3143. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, L.; Sánchez, B.; Margolles, A. Determination of Bile Salt Hydrolase Activity in Bifidobacteria. Methods Mol. Biol. 2021, 2278, 149–155. [Google Scholar] [CrossRef]
- Chinda, D.; Takada, T.; Mikami, T.; Shimizu, K.; Oana, K.; Arai, T.; Akitaya, K.; Sakuraba, H.; Katto, M.; Nagara, Y.; et al. Spatial Distribution of Live Gut Microbiota and Bile Acid Metabolism in Various Parts of Human Large Intestine. Sci. Rep. 2022, 12, 3593. [Google Scholar] [CrossRef]
- Tonin, F.; Otten, L.G.; Arends, I.W.C.E. NAD+-Dependent Enzymatic Route for the Epimerization of Hydroxysteroids. ChemSusChem 2019, 12, 3192–3203. [Google Scholar] [CrossRef]
- Zhang, X.; Fan, D.; Hua, X.; Zhang, T. Large-Scale Production of Ursodeoxycholic Acid from Chenodeoxycholic Acid by Engineering 7α- and 7β-Hydroxysteroid Dehydrogenase. Bioprocess. Biosyst. Eng. 2019, 42, 1537–1545. [Google Scholar] [CrossRef]
- Tonin, F.; Arends, I.W.C.E. Latest Development in the Synthesis of Ursodeoxycholic Acid (UDCA): A Critical Review. Beilstein J. Org. Chem. 2018, 14, 470–483. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, M. Bile Acid Detergency: Permeability, Inflammation, and Effects of Sulfation. Am. J. Physiol. Gastrointest. Liver Physiol. 2022, 322, G480–G488. [Google Scholar] [CrossRef]
- Huang, S.; Pang, D.; Li, X.; You, L.; Zhao, Z.; Cheung, P.C.-K.; Zhang, M.; Liu, D. A Sulfated Polysaccharide from Gracilaria Lemaneiformis Regulates Cholesterol and Bile Acid Metabolism in High-Fat Diet Mice. Food Funct. 2019, 10, 3224–3236. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.D.; Chen, J.; Hoffmann, C.; Bittinger, K.; Chen, Y.-Y.; Keilbaugh, S.A.; Bewtra, M.; Knights, D.; Walters, W.A.; Knight, R.; et al. Linking Long-Term Dietary Patterns with Gut Microbial Enterotypes. Science 2011, 334, 105–108. [Google Scholar] [CrossRef]
- Filippis, F.D.; Pellegrini, N.; Vannini, L.; Jeffery, I.B.; Storia, A.L.; Laghi, L.; Serrazanetti, D.I.; Cagno, R.D.; Ferrocino, I.; Lazzi, C.; et al. High-Level Adherence to a Mediterranean Diet Beneficially Impacts the Gut Microbiota and Associated Metabolome. Gut 2016, 65, 1812–1821. [Google Scholar] [CrossRef]
- Gutiérrez-Díaz, I.; Fernández-Navarro, T.; Sánchez, B.; Margolles, A.; González, S. Mediterranean Diet and Faecal Microbiota: A Transversal Study. Food Funct. 2016, 7, 2347–2356. [Google Scholar] [CrossRef]
- Liu, J.; Yan, Q.; Luo, F.; Shang, D.; Wu, D.; Zhang, H.; Shang, X.; Kang, X.; Abdo, M.; Liu, B.; et al. Acute Cholecystitis Associated with Infection of Enterobacteriaceae from Gut Microbiota. Clin. Microbiol. Infect. 2015, 21, 851.e1–851.e9. [Google Scholar] [CrossRef]
- Ye, F.; Shen, H.; Li, Z.; Meng, F.; Li, L.; Yang, J.; Chen, Y.; Bo, X.; Zhang, X.; Ni, M. Influence of the Biliary System on Biliary Bacteria Revealed by Bacterial Communities of the Human Biliary and Upper Digestive Tracts. PLoS ONE 2016, 11, e0150519. [Google Scholar] [CrossRef]
- Wu, T.; Zhang, Z.; Liu, B.; Hou, D.; Liang, Y.; Zhang, J.; Shi, P. Gut Microbiota Dysbiosis and Bacterial Community Assembly Associated with Cholesterol Gallstones in Large-Scale Study. BMC Genom. 2013, 14, 669. [Google Scholar] [CrossRef]
- Joossens, M.; Huys, G.; Cnockaert, M.; De Preter, V.; Verbeke, K.; Rutgeerts, P.; Vandamme, P.; Vermeire, S. Dysbiosis of the Faecal Microbiota in Patients with Crohn’s Disease and Their Unaffected Relatives. Gut 2011, 60, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Saltykova, I.V.; Petrov, V.A.; Logacheva, M.D.; Ivanova, P.G.; Merzlikin, N.V.; Sazonov, A.E.; Ogorodova, L.M.; Brindley, P.J. Biliary Microbiota, Gallstone Disease and Infection with Opisthorchis Felineus. PLoS Negl. Trop. Dis. 2016, 10, e0004809. [Google Scholar] [CrossRef]
- Hardy, J.; Francis, K.P.; DeBoer, M.; Chu, P.; Gibbs, K.; Contag, C.H. Extracellular Replication of Listeria Monocytogenes in the Murine Gall Bladder. Science 2004, 303, 851–853. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Escobedo, G.; Marshall, J.M.; Gunn, J.S. Chronic and Acute Infection of the Gall Bladder by Salmonella Typhi: Understanding the Carrier State. Nat. Rev. Microbiol. 2011, 9, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Yakoob, J.; Khan, M.R.; Abbas, Z.; Jafri, W.; Azmi, R.; Ahmad, Z.; Naeem, S.; Lubbad, L. Helicobacter Pylori: Association with Gall Bladder Disorders in Pakistan. Br. J. Biomed. Sci. 2011, 68, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Bansal, V.K.; Misra, M.C.; Chaubal, G.; Datta Gupta, S.; Das, B.; Ahuja, V.; Sagar, S. Helicobacter Pylori in Gallbladder Mucosa in Patients with Gallbladder Disease. Indian J. Gastroenterol. 2012, 31, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Dar, M.Y.; Ali, S.; Raina, A.H.; Raina, M.A.; Shah, O.J.; Shah, M.A.; Mudassar, S. Association of Helicobacter Pylori with Hepatobiliary Stone Disease, a Prospective Case Control Study. Indian J. Gastroenterol. 2016, 35, 343–346. [Google Scholar] [CrossRef]
- Fatemi, S.M.; Doosti, A.; Shokri, D.; Ghorbani-Danili, S.; Molazadeh, M.; Tavakoli, H.; Minakari, M.; Tavakkoli, H. Is There Correlation BetweenHelicobacter Pyloriand EnterohepaticHelicobacterSpecies With Gallstone Cholecystitis?: 61. Off. J. Am. Coll. Gastroenterol.|ACG 2017, 112, S28. [Google Scholar] [CrossRef]
- Molinero, N.; Ruiz, L.; Milani, C.; Gutiérrez-Díaz, I.; Sánchez, B.; Mangifesta, M.; Segura, J.; Cambero, I.; Campelo, A.B.; García-Bernardo, C.M.; et al. The Human Gallbladder Microbiome Is Related to the Physiological State and the Biliary Metabolic Profile. Microbiome 2019, 7, 100. [Google Scholar] [CrossRef]
- Oh, J.K.; Kim, Y.R.; Lee, B.; Choi, Y.M.; Kim, S.H. Prevention of Cholesterol Gallstone Formation by Lactobacillus Acidophilus ATCC 43121 and Lactobacillus Fermentum MF27 in Lithogenic Diet-Induced Mice. Food Sci. Anim. Resour. 2021, 41, 343–352. [Google Scholar] [CrossRef]
- Chuang, S.-C.; Hsi, E.; Lee, K.-T. Mucin Genes in Gallstone Disease. Clin. Chim. Acta 2012, 413, 1466–1471. [Google Scholar] [CrossRef]
- Castro-Torres, I.G.; de Jesús Cárdenas-Vázquez, R.; Velázquez-González, C.; Ventura-Martínez, R.; De la O-Arciniega, M.; Naranjo-Rodríguez, E.B.; Martínez-Vázquez, M. Future Therapeutic Targets for the Treatment and Prevention of Cholesterol Gallstones. Eur. J. Pharmacol. 2015, 765, 366–374. [Google Scholar] [CrossRef] [PubMed]
- Guarino, M.P.L.; Cocca, S.; Altomare, A.; Emerenziani, S.; Cicala, M. Ursodeoxycholic Acid Therapy in Gallbladder Disease, a Story Not yet Completed. World J. Gastroenterol. 2013, 19, 5029–5034. [Google Scholar] [CrossRef] [PubMed]
- Sanders, D.J.; Bomman, S.; Krishnamoorthi, R.; Kozarek, R.A. Endoscopic Retrograde Cholangiopancreatography: Current Practice and Future Research. World J. Gastrointest. Endosc. 2021, 13, 260–274. [Google Scholar] [CrossRef] [PubMed]
- Boicean, A.; Birlutiu, V.; Ichim, C.; Todor, S.B.; Hasegan, A.; Bacila, C.; Solomon, A.; Cristian, A.; Dura, H. Predictors of Post-ERCP Pancreatitis (P.E.P.) in Choledochal Lithiasis Extraction. J. Pers. Med. 2023, 13, 1356. [Google Scholar] [CrossRef] [PubMed]
- Elmunzer, B.J.; Foster, L.D.; Serrano, J.; Coté, G.A.; Edmundowicz, S.A.; Wani, S.; Shah, R.; Bang, J.Y.; Varadarajulu, S.; Singh, V.K.; et al. Indomethacin with or without Prophylactic Pancreatic Stent Placement to Prevent Pancreatitis after ERCP: A Randomised Non-Inferiority Trial. Lancet 2024, 403, 450–458. [Google Scholar] [CrossRef] [PubMed]
- Attili, A.F.; Scafato, E.; Marchioli, R.; Marfisi, R.M.; Festi, D. Diet and Gallstones in Italy: The Cross-Sectional MICOL Results. Hepatology 1998, 27, 1492–1498. [Google Scholar] [CrossRef] [PubMed]
- Attili, A.F.; Carulli, N.; Roda, E.; Barbara, B.; Capocaccia, L.; Menotti, A.; Okoliksanyi, L.; Ricci, G.; Capocaccia, R.; Festi, D. Epidemiology of Gallstone Disease in Italy: Prevalence Data of the Multicenter Italian Study on Cholelithiasis (M.I.COL.). Am. J. Epidemiol. 1995, 141, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Stinton, L.M.; Myers, R.P.; Shaffer, E.A. Epidemiology of Gallstones. Gastroenterol. Clin. N. Am. 2010, 39, 157–169. [Google Scholar] [CrossRef] [PubMed]
- Portincasa, P.; Moschetta, A.; Palasciano, G. Cholesterol Gallstone Disease. Lancet 2006, 368, 230–239. [Google Scholar] [CrossRef]
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Final Report. Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- Tsai, C.-J.; Leitzmann, M.F.; Willett, W.C.; Giovannucci, E.L. Prospective Study of Abdominal Adiposity and Gallstone Disease in US Men. Am. J. Clin. Nutr. 2004, 80, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.M.M.; Zimmet, P.; Shaw, J. Metabolic Syndrome--a New World-Wide Definition. A Consensus Statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Pak, M.; Lindseth, G. Risk Factors for Cholelithiasis. Gastroenterol. Nurs. 2016, 39, 297–309. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.; Xing, Y.; Fu, Y.; Chen, X.; Guan, L.; Liao, F.; Zhou, X. Causal Association between Metabolic Syndrome and Cholelithiasis: A Mendelian Randomization Study. Front. Endocrinol. 2023, 14, 1180903. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Díaz, I.; Molinero, N.; Cabrera, A.; Rodríguez, J.I.; Margolles, A.; Delgado, S.; González, S. Diet: Cause or Consequence of the Microbial Profile of Cholelithiasis Disease? Nutrients 2018, 10, 1307. [Google Scholar] [CrossRef] [PubMed]
- Steenackers, N.; Vanuytsel, T.; Augustijns, P.; Tack, J.; Mertens, A.; Lannoo, M.; Van der Schueren, B.; Matthys, C. Adaptations in Gastrointestinal Physiology after Sleeve Gastrectomy and Roux-En-Y Gastric Bypass. Lancet Gastroenterol. Hepatol. 2021, 6, 225–237. [Google Scholar] [CrossRef] [PubMed]
- Komorniak, N.; Martynova-Van Kley, A.; Nalian, A.; Wroński, M.; Kaseja, K.; Kowalewski, B.; Kaźmierczak-Siedlecka, K.; Łoniewski, I.; Kaczmarczyk, M.; Podsiadło, K.; et al. Association between Fecal Microbiota, SCFA, Gut Integrity Markers and Depressive Symptoms in Patients Treated in the Past with Bariatric Surgery-The Cross-Sectional Study. Nutrients 2022, 14, 5372. [Google Scholar] [CrossRef] [PubMed]
- Davies, N.K.; O’Sullivan, J.M.; Plank, L.D.; Murphy, R. Altered Gut Microbiome after Bariatric Surgery and Its Association with Metabolic Benefits: A Systematic Review. Surg. Obes. Relat. Dis. 2019, 15, 656–665. [Google Scholar] [CrossRef]
- Anhê, F.F.; Varin, T.V.; Schertzer, J.D.; Marette, A. The Gut Microbiota as a Mediator of Metabolic Benefits after Bariatric Surgery. Can. J. Diabetes 2017, 41, 439–447. [Google Scholar] [CrossRef]
- Ciobârcă, D.; Cătoi, A.F.; Copăescu, C.; Miere, D.; Crișan, G. Bariatric Surgery in Obesity: Effects on Gut Microbiota and Micronutrient Status. Nutrients 2020, 12, 235. [Google Scholar] [CrossRef]
- Guman, M.S.S.; Hoozemans, J.B.; Haal, S.; de Jonge, P.A.; Aydin, Ö.; Lappa, D.; Meijnikman, A.S.; Westerink, F.; Acherman, Y.; Bäckhed, F.; et al. Adipose Tissue, Bile Acids, and Gut Microbiome Species Associated With Gallstones After Bariatric Surgery. J. Lipid Res. 2022, 63, 100280. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Hao, C.; Yao, W.; Zhu, D.; Lu, H.; Li, L.; Ma, B.; Sun, B.; Xue, D.; Zhang, W. Intestinal Flora Imbalance Affects Bile Acid Metabolism and Is Associated with Gallstone Formation. BMC Gastroenterol. 2020, 20, 59. [Google Scholar] [CrossRef] [PubMed]
- Alnouti, Y. Bile Acid Sulfation: A Pathway of Bile Acid Elimination and Detoxification. Toxicol. Sci. 2009, 108, 225–246. [Google Scholar] [CrossRef] [PubMed]
- Liang, L.; Yi, Y.; Lv, Y.; Qian, J.; Lei, X.; Zhang, G. A Comprehensive Genome Survey Provides Novel Insights into Bile Salt Hydrolase (BSH) in Lactobacillaceae. Molecules 2018, 23, 1157. [Google Scholar] [CrossRef] [PubMed]
- Jia, B.; Park, D.; Hahn, Y.; Jeon, C.O. Metagenomic Analysis of the Human Microbiome Reveals the Association between the Abundance of Gut Bile Salt Hydrolases and Host Health. Gut Microbes 2020, 11, 1300–1313. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Hu, C.; Zhang, X.; Jia, W. Role of Gut Microbiota, Bile Acids and Their Cross-talk in the Effects of Bariatric Surgery on Obesity and Type 2 Diabetes. J. Diabetes Investig. 2018, 9, 13–20. [Google Scholar] [CrossRef]
- Patti, M.-E.; Houten, S.M.; Bianco, A.C.; Bernier, R.; Larsen, P.R.; Holst, J.J.; Badman, M.K.; Maratos-Flier, E.; Mun, E.C.; Pihlajamaki, J.; et al. Serum Bile Acids Are Higher in Humans With Prior Gastric Bypass: Potential Contribution to Improved Glucose and Lipid Metabolism. Obesity 2009, 17, 1671–1677. [Google Scholar] [CrossRef]
- De Vuono, S.; Ricci, M.A.; Nulli Migliola, E.; Monti, M.C.; Morretta, E.; Boni, M.; Ministrini, S.; Carino, A.; Fiorucci, S.; Distrutti, E.; et al. Serum Bile Acid Levels Before and After Sleeve Gastrectomy and Their Correlation with Obesity-Related Comorbidities. Obes. Surg. 2019, 29, 2517–2526. [Google Scholar] [CrossRef]
- Nemati, R.; Lu, J.; Dokpuang, D.; Booth, M.; Plank, L.D.; Murphy, R. Increased Bile Acids and FGF19 After Sleeve Gastrectomy and Roux-En-Y Gastric Bypass Correlate with Improvement in Type 2 Diabetes in a Randomized Trial. Obes. Surg. 2018, 28, 2672–2686. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Hylemon, P.B.; Ridlon, J.M.; Heuman, D.M.; Daita, K.; White, M.B.; Monteith, P.; Noble, N.A.; Sikaroodi, M.; Gillevet, P.M. Colonic Mucosal Microbiome Differs from Stool Microbiome in Cirrhosis and Hepatic Encephalopathy and Is Linked to Cognition and Inflammation. Am. J. Physiol. Gastrointest. Liver Physiol. 2012, 303, G675–G685. [Google Scholar] [CrossRef]
- Ocaña-Wilhelmi, L.; Martín-Núñez, G.M.; Ruiz-Limón, P.; Alcaide, J.; García-Fuentes, E.; Gutiérrez-Repiso, C.; Tinahones, F.J.; Moreno-Indias, I. Gut Microbiota Metabolism of Bile Acids Could Contribute to the Bariatric Surgery Improvements in Extreme Obesity. Metabolites 2021, 11, 733. [Google Scholar] [CrossRef] [PubMed]
- Ridlon, J.M.; Kang, D.-J.; Hylemon, P.B. Bile Salt Biotransformations by Human Intestinal Bacteria. J. Lipid Res. 2006, 47, 241–259. [Google Scholar] [CrossRef] [PubMed]
- Fearon, N.M.; Kearns, E.C.; Kennedy, C.A.; Conneely, J.B.; Heneghan, H.M. The Impact of Ursodeoxycholic Acid on Gallstone Disease after Bariatric Surgery: A Meta-Analysis of Randomized Control Trials. Surg. Obes. Relat. Dis. 2022, 18, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Van den Bossche, L.; Hindryckx, P.; Devisscher, L.; Devriese, S.; Van Welden, S.; Holvoet, T.; Vilchez-Vargas, R.; Vital, M.; Pieper, D.H.; Vanden Bussche, J.; et al. Ursodeoxycholic Acid and Its Taurine- or Glycine-Conjugated Species Reduce Colitogenic Dysbiosis and Equally Suppress Experimental Colitis in Mice. Appl. Environ. Microbiol. 2017, 83, e02766-16. [Google Scholar] [CrossRef] [PubMed]
- Medina, D.A.; Pedreros, J.P.; Turiel, D.; Quezada, N.; Pimentel, F.; Escalona, A.; Garrido, D. Distinct Patterns in the Gut Microbiota after Surgical or Medical Therapy in Obese Patients. PeerJ 2017, 5, e3443. [Google Scholar] [CrossRef] [PubMed]
- Murphy, R.; Tsai, P.; Jüllig, M.; Liu, A.; Plank, L.; Booth, M. Differential Changes in Gut Microbiota After Gastric Bypass and Sleeve Gastrectomy Bariatric Surgery Vary According to Diabetes Remission. Obes. Surg. 2017, 27, 917–925. [Google Scholar] [CrossRef] [PubMed]
- Federico, A.; Dallio, M.; Tolone, S.; Gravina, A.G.; Patrone, V.; Romano, M.; Tuccillo, C.; Mozzillo, A.L.; Amoroso, V.; Misso, G.; et al. Gastrointestinal Hormones, Intestinal Microbiota and Metabolic Homeostasis in Obese Patients: Effect of Bariatric Surgery. In Vivo 2016, 30, 321–330. [Google Scholar] [PubMed]
- Wang, B.; Yao, M.; Lv, L.; Ling, Z.; Li, L. The Human Microbiota in Health and Disease. Engineering 2017, 3, 71–82. [Google Scholar] [CrossRef]
- Davis, C.D. The Gut Microbiome and Its Role in Obesity. Nutr. Today 2016, 51, 167–174. [Google Scholar] [CrossRef]
- Al-Assal, K.; Martinez, A.C.; Torrinhas, R.S.; Cardinelli, C.; Waitzberg, D. Gut Microbiota and Obesity. Clin. Nutr. Exp. 2018, 20, 60–64. [Google Scholar] [CrossRef]
- Chambers, E.S.; Preston, T.; Frost, G.; Morrison, D.J. Role of Gut Microbiota-Generated Short-Chain Fatty Acids in Metabolic and Cardiovascular Health. Curr. Nutr. Rep. 2018, 7, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Pilmis, B.; Le Monnier, A.; Zahar, J.-R. Gut Microbiota, Antibiotic Therapy and Antimicrobial Resistance: A Narrative Review. Microorganisms 2020, 8, 269. [Google Scholar] [CrossRef] [PubMed]
- Rinninella, E.; Raoul, P.; Cintoni, M.; Franceschi, F.; Miggiano, G.A.D.; Gasbarrini, A.; Mele, M.C. What Is the Healthy Gut Microbiota Composition? A Changing Ecosystem across Age, Environment, Diet, and Diseases. Microorganisms 2019, 7, 14. [Google Scholar] [CrossRef] [PubMed]
- Redondo-Useros, N.; Nova, E.; González-Zancada, N.; Díaz, L.E.; Gómez-Martínez, S.; Marcos, A. Microbiota and Lifestyle: A Special Focus on Diet. Nutrients 2020, 12, 1776. [Google Scholar] [CrossRef] [PubMed]
- Afzaal, M.; Saeed, F.; Shah, Y.A.; Hussain, M.; Rabail, R.; Socol, C.T.; Hassoun, A.; Pateiro, M.; Lorenzo, J.M.; Rusu, A.V.; et al. Human Gut Microbiota in Health and Disease: Unveiling the Relationship. Front. Microbiol. 2022, 13, 999001. [Google Scholar] [CrossRef] [PubMed]
- Albillos, A.; de Gottardi, A.; Rescigno, M. The Gut-Liver Axis in Liver Disease: Pathophysiological Basis for Therapy. J. Hepatol. 2020, 72, 558–577. [Google Scholar] [CrossRef] [PubMed]
- Tilg, H.; Adolph, T.E.; Trauner, M. Gut-Liver Axis: Pathophysiological Concepts and Clinical Implications. Cell Metab. 2022, 34, 1700–1718. [Google Scholar] [CrossRef] [PubMed]
- Afecto, E.; Ponte, A.; Fernandes, S.; Silva, J.; Gomes, C.; Correia, J.; Carvalho, J. Fecal Microbiota Transplantation in Hepatic Encephalopathy: A Review of the Current Evidence and Future Perspectives. AGEB 2021, 84, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Trebicka, J.; Macnaughtan, J.; Schnabl, B.; Shawcross, D.L.; Bajaj, J.S. The Microbiota in Cirrhosis and Its Role in Hepatic Decompensation. J. Hepatol. 2021, 75, S67–S81. [Google Scholar] [CrossRef]
- Boicean, A.; Birlutiu, V.; Ichim, C.; Brusnic, O.; Onișor, D.M. Fecal Microbiota Transplantation in Liver Cirrhosis. Biomedicines 2023, 11, 2930. [Google Scholar] [CrossRef]
- Xue, L.; Deng, Z.; Luo, W.; He, X.; Chen, Y. Effect of Fecal Microbiota Transplantation on Non-Alcoholic Fatty Liver Disease: A Randomized Clinical Trial. Front. Cell Infect. Microbiol. 2022, 12, 759306. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Shao, W.; Liu, Q.; Liu, N.; Wang, Q.; Xu, J.; Zhang, X.; Weng, Z.; Lu, Q.; Jiao, L.; et al. Gut Microbiota Promotes Cholesterol Gallstone Formation by Modulating Bile Acid Composition and Biliary Cholesterol Secretion. Nat. Commun. 2022, 13, 252. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Author | Number of Examined Patients | Type of Surgery (n Patients) | Post-Surgical Evaluation | Microbiota Changes after Surgery | Bile Acids Changes after Surgery | Additional Information |
|---|---|---|---|---|---|---|
| [93] | 16 | RYGB SG | no data | Increased Enterobacteriaceae and decreased Clostridiales and Bifidobacteriaceae after RYGB | There was a reduction in most of the primary bile acids with RYGB. In SG, the primary bile acids seemed to be increased. The secondary bile acids were reduced in RYGB and increased in SG | After RYGB, an increase in Proteobacteria and Veillonella was observed, the genus Blautia from Clostridiales decreased in the same way as the family Bifidobacteriaceae and its genus Bifidobacterium. No significant changes were observed after SG. |
| [83] | 88 | RYGB (82) OLGB (6) | 2 years | Increased Bacteroidetes, Firmicutes | Higher concentrations of secondary bile acids were detected in patients with gallstones. In patients without gallstones, the bile acids glycochenodeoxycholate 3-sulfate, glycochenodeoxycholate glucuronide, glycocholate, glycodeoxycholate 3-sulfate, glycohyocholate, glycolithocholate sulfate, taurochenodeoxycholic acid 3-sulfate and taurolithocholate 3-sulfate were increased | Patients who developed gallstones after surgery had a higher abundance of Bacteroides intestinalis, Finegoldia magna, Ruminococcus gnavus and Prevotella buccalis and those who did not had a higher abundance of Lactobacillaceae and Enterobacteriaceae. |
| [88] | no data | RYGB SG | no data | Increased Proteobacteria and Bacteroidetes, and decreased Firmicutes | Serum bile acid levels are significantly increased 2–4 years after RYGB and both RYGB and SG can result in increased circulating levels of BA | Patients who developed gallstones after RYGB had a higher abundance of Escherichia coli, Klebsiella pneumoniae, Veillonella dispar and Veillonella parvula and those who underwent SG had a lower abundance of Eubacterium rectale, Bacteroides vulgatus, Bacteroides sp.3_1_40A, Coprococcus comes, Ruminococcus obeum, Dorea longicatena, Lachnospiraceae bact.5_1_63FAA and Clostridium sp. L2_50. |
| [97] | 19 | RYGB SG MT | 1 year | Increased Proteobacteria and Bacteroidetes after RYGB, increased Proteobacteria and decreased Bacteroidetes in SG | no data | The abundance of Firmicutes was mostly unaffected after both RYGB and SG. The microbiota changes also caused an increase in the Bacteroides/Firmicutes ratio in SG patients, and conversely a strong decrease in the RYGB group. |
| [98] | 14 | RYGB SG | 1 year | Increased Firmicutes, Actinobacteria and decreased Bacteroidetes after RYGB; increased Bacteroidetes after SG | no data | In patients with diabetes persisting 1 year after RYGB or SG, there were no phyla level changes. In patients who achieved diabetes remission after RYGB, there were an increase in Firmicutes, Actinobacietra and Bacteroidetes, and in those who achieved diabetes remission after SG, there wero no phyla level changes. |
| [99] | 47 | BIB | 1 year | Increased Lactobacillus and Megasphaera and decreased Roseburia | no data | The two major types of bacteria after surgery were Lactobacillus crispatus and Streptococcus spp. The next major bacterial population found in obese people after surgery is related to Megasphaera elsdenii, which is considered the most important rumen lactate-utilizing bacterium. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Komorniak, N.; Pawlus, J.; Gaweł, K.; Hawryłkowicz, V.; Stachowska, E. Cholelithiasis, Gut Microbiota and Bile Acids after Bariatric Surgery—Can Cholelithiasis Be Prevented by Modulating the Microbiota? A Literature Review. Nutrients 2024, 16, 2551. https://doi.org/10.3390/nu16152551
Komorniak N, Pawlus J, Gaweł K, Hawryłkowicz V, Stachowska E. Cholelithiasis, Gut Microbiota and Bile Acids after Bariatric Surgery—Can Cholelithiasis Be Prevented by Modulating the Microbiota? A Literature Review. Nutrients. 2024; 16(15):2551. https://doi.org/10.3390/nu16152551
Chicago/Turabian StyleKomorniak, Natalia, Jan Pawlus, Katarzyna Gaweł, Viktoria Hawryłkowicz, and Ewa Stachowska. 2024. "Cholelithiasis, Gut Microbiota and Bile Acids after Bariatric Surgery—Can Cholelithiasis Be Prevented by Modulating the Microbiota? A Literature Review" Nutrients 16, no. 15: 2551. https://doi.org/10.3390/nu16152551
APA StyleKomorniak, N., Pawlus, J., Gaweł, K., Hawryłkowicz, V., & Stachowska, E. (2024). Cholelithiasis, Gut Microbiota and Bile Acids after Bariatric Surgery—Can Cholelithiasis Be Prevented by Modulating the Microbiota? A Literature Review. Nutrients, 16(15), 2551. https://doi.org/10.3390/nu16152551