
Orthorexia as an Eating Disorder Spectrum—A Review of the Literature


 , and
, and 
Abstract
1. Introduction
1.1. Introduction to Orthorexia Nervosa
1.2. Historical Context and Definition
1.3. Prevalence and Risk Factors
1.4. Challenges in Classification and Diagnosis
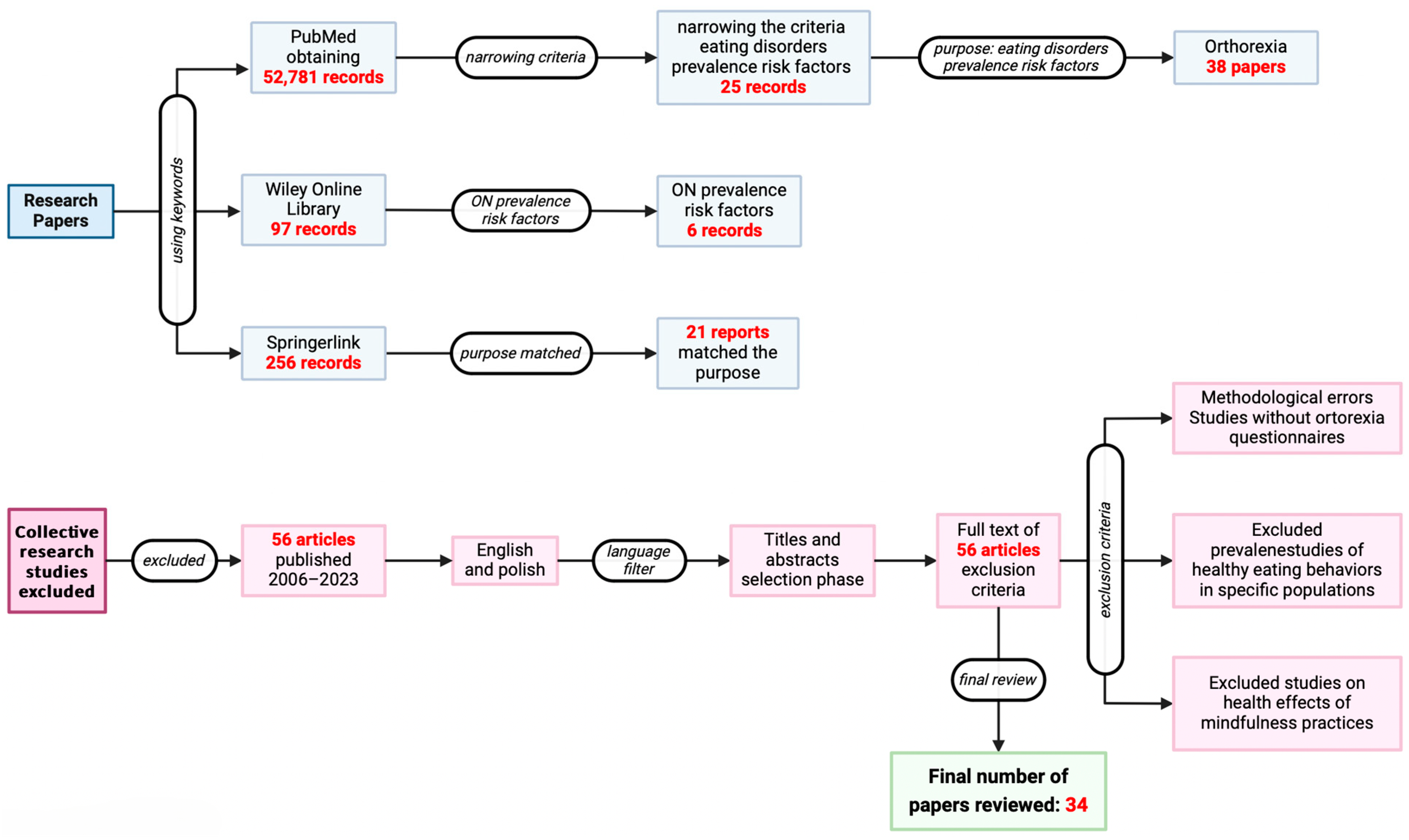
2. Methodology and Selection Criteria
3. Overview of the Research Review
3.1. Prevalence Studies
3.2. Personality Traits and Orthorexia
3.3. Orthorexia and Related Eating Disorders

{kind=link}
| No. | Researcher | Purpose of the Survey | Research Methods | Study Group | Frequency | Results and Comments | |
|---|---|---|---|---|---|---|---|
| Number of Participants | Group Characteristics | ||||||
| 1 | [26] | Assessing the prevalence of orthorexia nervosa and the different causes of orthorexia nervosa in Austrian female nutritionists. | FEV 1 assessment, BOT 2 evaluation | 283 | The group consisted of Austrian women aged 22–66 years who were dietitians | 12.8% of female participants showed symptoms of orthorexia nervosa | Stress, emotional crisis, and serious emotional and physical distress. These results suggest that orthorexia nervosa is a relatively common eating disorder among dieters. |
| 2 | [27] | The study shows the importance of understanding the effects of previous family experiences with ED 3 | Tugrul scale, EAT-26 4, Teruel Orthorexia Nervosa Scale (TOS) 5 | 225 | The study group consisted of adults aged 18–24 years old | “Healthy orthorexia nervosa” (HO) 6 and “diet-related disorders” (HEF) 7 had a significant impact on participants’ eating attitudes. The association between eating attitudes and HEF 7 was r = 0.57 | Orthorexia nervosa in healthy individuals may result from limited social activities and family problems. |
| 3 | [23] | Investigating whether mental anorexia correlates with ON 8 | ONI 9, BRIEF-A 10 | 405 | Among participants, 80% were female. Half Caucasian. Average age = 24 years, average BMI = 25 | The study found that orthorexia nervosa was weakly to moderately correlated with most BRIEF-A scales, with the most correlated with behavioral regulation, such as emotional control (r = 0.34) and inhibition (r = 0.30) | Anorexia and orthorexia nervosa have similar symptoms and share the same neuropsychological nature. |
| 4 | [25] | Investigate the associations between ON 8 and EDs 3, psychopathological symptoms, and defense mechanisms | ON (EHQ-21) 11, eating psychopathology (EDI-3) 12, psychopathological symptoms (BSI) 13, defense mechanisms (DSQ-40) 14 | 270 | Students from the University of Palermo in southern Italy and were assigned to three groups: 52 people with ON 8 symptoms, 157 people constituted a healthy eating control group, and 61 people following a normal diet | Not specified | ON 8 associated with more frequent psychopathological episodes and the use of various pathological defense strategies. |
| 5 | [28] | The aim was to find out examination of the risks of developing ON 8 with emphasis on individual factors | Answered self-administered questionnaires assessing ON 8 | 3235 | The study group consisted of 10.32% men and 89.67% women, with a mean age of 21.13 years. Participants self-completed questionnaires assessing orthorexia nervosa (ON) 8 and other | In a study conducted on the same random population, it was discovered that orthorexia nervosa (ON) 8 was exhibited by 3.28% of the participants. The mean F-DOS 15 scale score for the whole group was 19.2 (SD = 4.95), while in the orthorexic group the mean score was 32.62 (SD = 2.27) | ON 8 can collude with different character models, and some of them are characterized by a significant level of psychopathology. |
| 6 | [21] | The aim was to measure orthorexia using an assessment method | Temperament Character Inventory-56 (TCI-56) 16, Ortho-11-Hu 17 | 739 | Participants’ ages ranged from 18 to 72 years. The research group consisted of doctors, athletes, nutritionists, performance artists, and Ashtanga yoga practitioners | The mean ORTO-11-Hu 17 score was 22.71 (SD = 4.55). The high ON tendency group (score 14–29) comprised 234 subjects and the low ON 8 tendency group (score 35–43) comprised 245 subjects. Women were more likely than men to show high ON 8 tendencies | Psychological indicators of AN 18 and BN 19 indicate the following important parameters of orthorexia nervosa. |
| 7 | [20] | Investigate whether ON 8 correlates with anorexia and bulimia in relation to perfectionism, attitudes towards body image and attachment style | ORTO-15 20, MPS 21, MBSRQ-AS 22, RSQ 23, RSES 24 | 220 | The survey group was 46 men and 174 women; 180 of those were first- and second-year psychology students at James Cook University | The mean score for ORTO-15 (based on nine items) was 22.71 (SD = 4.55). There was no significant difference in ORTO-15 20 scores between men and women | Stronger orthorexic tendencies were significantly correlated with incidences of perfectionism. |
| 8 | [18] | Analysis of possible links the relationship of ON and psychological behaviors and functions that are widespread to EDs 3 | ORTO-11-ES 26, EDI-2 27 | 492 | The research group consisted of students from the University of Castilla-La Mancha in Spain (280 young women and 212 men) | Confirmatory factor analysis (CFA) 25 identified 11 items and 3 attributes as the superior matching model; CFI 28 = 0.94, TLI 29 = 0.91, RMSEA 30 = 0.058 | Many mental and organizational behavioral issues of the erectile impairment are shared by those at increased risk of ON 8. |
| 9 | [46] | The aim was to explore the relationship between inappropriate spatial pattern of social behavior and coping strategies | ON (ORTO-15 20—reduced to ORTO-7CS), EAT-26 4, alexithymia (TAS-20) 31, emotion dysregulation (DERS-16) 32 | 196 | The study involved167 women, 29 men. The age range was 18–66 years | Not specified | Problems with recognition and control of experienced emotions are associated with higher rates of ON 8. |
| 10 | [41] | Assessment of the occurrence of ON 8 in people with disordered eating behavior and body image in the study group | Eating Attitudes Test-26, the Body Shape Questionnaire-34, ORTO-15 20 | 92 | Participants are adult Australians recruited at the university | The prevalence rate of orthorexia nervosa was 21% using an ORTO-15 20 cut-off value of <35 | Significant risk factors for ON 8 include being overweight, being unhappy with body image, and challenges in terms of verbal skills. |
| 11 | [29] | Investigating the relationship between ORTO-15 20 score and test for obsessive–compulsive symptoms, eating disorders, and body-related discomfort. | ORTO-15 20 test, the Maudsley Obsessive–Compulsive Questionnaire, the Eating Attitudes Test-26, the Body Uneasiness Test | 120 | Students currently signed up for the first year of their medical studies and master’s degrees in literature and philosophy at the University of Pavia, of which there were 83 women and 37 men | In female students, a statistically relevant, though weak, correlation was observed between ORTO-15 20 and body image discomfort (r = 0.39) | Lower the ORTO-15 20 scores the less pathological body image discomfort and obsessive–compulsive symptoms. |
| 12 | [30] | Study aimed to identify the relationships between orthorexia nervosa and social appearance anxiety | Orthorexia Nervosa Scale | 430 | 215 nursing students and 215 physical education students | Among students in the Faculty of Sport Sciences (FSS), orthorexia nervosa was present in 28.8% of cases, while in the Faculty of Nursing (ND) it was 16.3% | There was a negative relationship between scale SAAS 33 and RSES 24, which are considered determinants of ON 8. |
| 13 | [31] | Study examined the prospective associations between five components bodily perceptions and manifestations of ON 8 in adult women in a social context | Other | 558 | Women from the worldwide population | Not specified | Negative body image might be implicated in the onset or maintenance of ON 8 symptoms. |
| 14 | [18] | The prevalence of ON 8 and to analyze potential links between ON 8 and psychological traits frequently observed in eating disorders (EDs) 3 | The ORTO-11-ES 26 questionnaire, the Eating Disorder Inventory (EDI-2) 27 | 454 | The research group consisted of students from the University of Castilla-La Mancha in Spain (280 young women and 212 men) | Confirmatory factor analysis (CFA) identified 11 items and 3 attributes as the superior matching model; CF 28 I = 0.94, TLI 29 = 0.91, RMSEA 30 = 0.058 | The results of the EDI-2 28 study in the ON 8 exposure group seemed to suggest that the specific characteristics of individuals were associated with a higher risk of ON 8. |
| 15 | [32] | Evaluation of the relationship between religiosity and orthorexia nervosa | Teruel Orthorexia Nervosa | 428 | Participants were individuals over the age of 18 with Lebanese citizenship | Not specified | The level of self-esteem was associated with low levels of mental orthorexia nervosa. Higher religiosity was shown to be associated with higher self-esteem. |
| 16 | [24] | This study examined how used test scores correlate with BOT 2 scores in relation to age, gender, and self-reported exercise duration. | Sociocultural Attitudes Towards Appearance Questionnaire (SATAQ) relate to Bratman’s orthorexia nervosa test (BOT) | 251 | The research group consists of people attending fitness classes in five fitness centers in a city in southwest Sweden | The prevalence of orthorexia nervosa (ON) 8 in the men’s and women’s study was determined by different analytical models | Women’s gym participants who exercised more frequently had high BOT scores. This validates the link between increased exercise and problematic weight management behaviors, as well as ED 3. |
| 17 | [33] | The goal was to scrutinize the connection between exercise addiction EA and ON 8 | Compulsive Exercise Disorder Inventory (EAI) 34, Düsseldorfer Orthorexie Skala (DOS) | 1008 | The group consisted of 559 male and 449 female active members of three fitness studios | In the study group, 10.2% have symptoms of anorexia and 3.4% suffer from orthorexia nervosa. In addition, 2.3% of participants struggle with both disorders simultaneously | Exercise addiction and excessive exercising connected with more pronounced ON 8. |
| 18 | [12] | The focus was on investigating the frequency of ON 8 in university students who take part in various competitions | ORTO-15 20 | 215 | The study group was aged between 20 and 22 from universities in North East England who had completed the ORTO-15 test (≤40) | ON 8 symptoms were high in all students (76%) | Students and especially those who take part in university competitions can get sick from ON 8. |
| 19 | [34] | Ashtanga yoga is a predisposition to ON 8 | ORTO-15 20 | 136 | The research thicket was the local Ashtanga yoga community | In a study of 136 people, the mean score on the ORTO-15 20 test was 35.27 ± 3.69. As many as 86% of participants scored below 40 | Ashtanga yoga predisposes ON 8. The results of the study suggest that an intense focus on a healthy diet, which is often promoted in the context of Ashtanga yoga practice, may lead to the development of orthorexia nervosa (ON) 8. |
| 20 | [35] | The aim of the study was to assess the prevalence and some psychological and other correlates of ON 8 tendencies among gym-goers | (Orto-11-Hu) 17 and independent variables (Eating Disorder Inventory, Maudsley Obsessional–Compulsive Inventory, health and exercise habits, and demographics) | 207 | The participants were gym-goers. The average age was about 32 years. Most were women from higher level of education | The mean score on the ORTO-11-Hu test was 27.7. The propensity to ON 8 was more prevalent in those who strived for an ideal body shape | Results suggest that ON 8 is associated with frequent exercise and younger age. |
| 21 | [36] | The aim was to study the relationship between vegetarianism and orthorexia nervosa (ON) 8 | General characteristics, anthropometric data, the Bratman Test for Orthorexia nervosa (BOT) 2, and questions assessing attitudes toward food and nutrition | 2611 | 1346 vegetarians and 1265 non-vegetarians | The incidence of mania for healthy food is more common among vegetarians than non-vegetarians | Intense attachment to healthy food is higher in vegetarians, especially lactovegetarians, and ON 8 prevalence decreases with age. |
| 22 | [37] | Analysis to determine if ON 8 risk factors are related to lifestyle | ORTO-15 20 | 671 | Participants in the study were students at the University of Pavia. Participants were 654% female, 46% male | The results of the ORTO-15 20 test showed that 31.2% of participants scored below 35, indicating a risk of orthorexia nervosa | Diet is a major determinant of ON 8. |
| 23 | [38] | The aim of the study was to assess the prevalence of ON 8 symptoms in organic shop customers and compare the results those of with patients without OSC 35 | ORTO-15 20 Eating Habits Questionnaire (EHQ) | 121 | The research group was customers of organic shops | Prevalence among OSC was 69.4% and 23.1% using ORTO-15 20 with 40 and 35 cut-off points | Organic store customers (OSCs) 35 may be a population at risk for ON 8. |
| 24 | [47] | The aim of the study was assessment of the frequency of ON 8 and association with the sex and dietary habits in relation to early adulthood | ORTO-15 20 | 2130 | Participants were University of Pisa students who anonymously completed the ORTO-15 20 questionnaire and a form on sociodemographic characteristics and eating habits. | The mean ORTO-15 20 score was 36.93 ± 4.22, with 34.9% of participants scoring below 35, indicating a risk of orthorexia nervosa | Higher ON 8 rates in women (37.8% vs. 30.7%), vegans/vegetarians (56.3% vs. 32.2%), and those with a low BMI (42.8% vs. 34.2%). |
| 25 | [48] | The aim was to explore problematic eating behaviors in a vegan population | Scales in Orthorexia nervosa, Self-Compassion, Mindful, Emotional, External, and Restraint Eating | 315 | The group consisted of 287 women and 28 men who followed a vegan diet and completed orthorexia nervosa tests | The prevalence of orthorexia nervosa in the study group was determined by correlation analysis | People with high levels of ON 8 show low levels of self-compassion and high levels of restrained eating. |
| 26 | [49] | The investigation focused on the relationship between ME and perfectionism in the etiology | Düsseldorf Orthorexia nervosa scale, the Mindful Eating Behavior scale, the Big-Three Perfectionism scale Short-form | 670 | The study group consisted of 588 women and 78 men (n = 670), and the age of the participants ranged from 18 to 74 years. | Not specified | A significant relationship was found between the “aware” aspect of ON 8. People suffering from perfectionism are in the ON risk group. |
| 27 | [14] | Prevalence and risk factors of ON | ORTO-15 20, EAT-26 4, MOCI 36, BDI-II 37, individual questionnaire | 864 | 599 women aged 17 to 23 and 265 men aged 15 to 21 | 27% | Overweight 13–16-year-olds are more likely to suffer from ON 8. |
| 28 | [39] | Test BOT 2 for ON 8 diagnosis, and its relationship to validated tools for assessing disordered eating | BOT 2, EAT-26 4, BDDQ 38, OCI-R 39 | 448 | The group was made up of college students with an average age of 22 years old | Significant positive correlations were observed between ON scores and total BOT scores (r = 0.47, p < 0.01), EAT-26 (r = 0.25, p < 0.01) and BDDQ (r = 0.19, p < 0.01) | Hispanic/Latino and overweight/obese as a predisposition for ON 8. |
| 29 | [47] | The “awareness” facet demonstrated a significant link with ON 8, and individuals with perfectionistic traits are more likely to be at risk for ON | ORTO-15 20 | 2130 | Participants were University of Pisa w students who anonymously completed the ORTO-15 20 questionnaire and a form on sociodemographic characteristics and eating habits. | 34.9% | ON rates were considerably higher among those with younger BMI values. |
| 30 | [41] | The aim is to estimate the prevalence of ON 8 and identify risk factors for orthorexia nervosa | Eating Attitudes Test-26, the Body Shape Questionnaire-34, ORTO-15 20 | 92 | Participants are adult Australians recruited at the university | The prevalence rate of orthorexia nervosa was 21% using an ORTO-15 20 cut-off value of < 35 | Key contributors to ON risk are being underweight, having issues with body appearance, and experiencing poor social functioning. |
| 31 | [40] | To investigate the frequency of ON in relation to dietary behavior and body satisfaction among college undergraduates. | ORTO-15, BPPPS 40, FFQ-6 41 | 1120 | Health and non-health students from seven universities in Poland | When the cut-off point was 40, a tendency towards orthorexia nervosa (ON) was shown by 75.0% of participants. When the cut-off point was 35, the prevalence of ON was equal to (28.3%) | Health students at increased exposure to high risk of ON 8. |
| 32 | [50] | Study to identify demographic factors and predictors of ON, including PrEP use, online portals, and Grindr ® | ORTO-15 20, EAT-26 4 | 394 | Participants were gay men aged 18 and over who identified themselves as male. There were 188 participants from Poland and 206 from Spain | Orthorexia nervosa was found in 40% of Polish participants, compared to 28% of Spanish participants | The most important predictors of mental anorexia in homosexual men are low BMI and use of Grindr. |
| 33 | [47] | The analysis was to demonstrate the frequency of ON and its relationship with gender and dietary style among participants | ORTO-15 20 | 2130 | Participants were University of Pisa w students who anonymously completed the ORTO-15 20 questionnaire and a form on sociodemographic characteristics and eating habits. | The mean ORTO-15 20 score was 36.93 ± 4.22, with 34.9% of participants scoring below 35, indicating a risk of orthorexia nervosa | Significantly higher rate of ON 8 in women than in men (37.8 vs. 30.7%). |
| 34 | [51] | The study aimed to establish the relationship between eating problems, mental anorexia, gender and BMI, and field of study among Turkish female students | EAT-40 42, ORTO-15 20 | 900 | The research group was students aged 17–23 | The proportion of orthorexia nervosa female subjects is higher than the number of males | Women are more likely to have ON 8. |
3.4. Risk Factors in Adolescents and Young Adults
3.5. Potential Treatments
4. Discussion
4.1. Comorbidities
4.2. Body Image and Eating Habits
4.3. The Influence of Social Media
4.4. Cultural Differences and Profession
4.5. Limitations
5. Conclusions
Funding
Conflicts of Interest
References
- Bogár, N.; Dukay-Szabó, S.; Simon, D.; Túry, F. Higher orthorexia tendency among female fashion models: An empirical international study. Eat. Weight. Disord. EWD 2024, 29, 44. [Google Scholar] [CrossRef] [PubMed]
- Donini, L.M.; Marsili, D.; Graziani, M.P.; Imbriale, M.; Cannella, C. Orthorexia nervosa: A preliminary study with proposal for diagnosis and attempt to measure the dimension of the phenomenon. Eat. Weight Disord. 2004, 9, 151–157. [Google Scholar] [CrossRef]
- Dunn, T.M.; Bratman, S. On orthorexia nervosa: A review of literature and proposed diagnostic criteria. Eat. Behav. 2016, 21, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Yılmaz, H.; Karakuş, G.; Tamam, L.; Demirkol, M.E.; Namlı, Z.; Yeşiloğlu, C. Association of Orthorexic Tendencies with Obsessive-Compulsive Symptoms, Eating Attitudes and Exercise. Neuropsychiatr. Dis. Treat. 2020, 16, 3035–3044. [Google Scholar] [CrossRef]
- López-Gil, J.F.; Tárraga-López, P.J.; Hershey, M.S.; López-Bueno, R.; Gutiérrez-Espinoza, H.; Soler-Marín, A.; Fernández-Montero, A.; Victoria-Montesinos, D. Overall Proportion of Orthorexia Nervosa Symptoms: A Systematic Review and Meta-Analysis Including 30,476 Individuals from 18 Countries. J. Glob. Health 2023, 13, 04087. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.G.; Lefevre, C.E. Instagram Use Is Linked to Increased Symptoms of Orthorexia Nervosa. Eat. Weight Disord. 2017, 22, 277–284. [Google Scholar] [CrossRef]
- Erol, Ö.; Özer, A. Determination of Orthorexia Nervosa Symptoms and Eating Attitudes in Medicine Students. Eur. J. Public Health 2019, 29 (Suppl. S4), ckz186.280. [Google Scholar] [CrossRef]
- Bo, S.; Zoccali, R.; Ponzo, V.; Soldati, L.; De Carli, L.; Benso, A.; Fea, E.; Rainoldi, A.; Durazzo, M.; Fassino, S.; et al. University Courses, Eating Problems and Muscle Dysmorphia: Are There Any Associations? J. Transl. Med. 2014, 12, 221. [Google Scholar] [CrossRef]
- Niedzielski, A.; Kaźmierczak-Wojtaś, N. Prevalence of Orthorexia Nervosa and Its Diagnostic Tools—A Literature Review. Int. J. Environ. Res. Public Health 2021, 18, 5488. [Google Scholar] [CrossRef]
- Donini, L.M.; Barrada, J.R.; Barthels, F.; Dunn, T.M.; Babeau, C.; Brytek-Matera, A.; Cena, H.; Cerolini, S.; Cho, H.H.; Coimbra, M.; et al. A consensus document on definition and diagnostic criteria for orthorexia nervosa. Eat. Weight. Disord. EWD 2022, 27, 3695–3711. [Google Scholar] [CrossRef]
- Stochel, M.; Janas-Kozik, M.; Zejda, J.E.; Hyrnik, J.; Jelonek, I.; Siwiec, A. Walidacja kwestionariusza ORTO-15 w grupie młodzieży miejskiej w wieku 15–21 lat. Psychiatr. Pol. 2015, 49, 119–134. [Google Scholar] [CrossRef]
- Clifford, T.; Blyth, C. A pilot study comparing the prevalence of orthorexia nervosa in regular students and those in University sports teams. Eat. Weight Disord. 2019, 24, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Łucka, I.; Janikowska-Hołoweńko, D.; Domarecki, P.; Plenikowska-Ślusarz, T.; Domarecka, M. Orthorexia nervosa—A separate clinical entity, a part of eating disorder spectrum or another manifestation of obsessive-compulsive disorder? Psychiatr. Pol. 2019, 53, 371–382. [Google Scholar] [CrossRef]
- Łucka, I.; Janikowska-Hołoweńko, D.; Domarecki, P.; Plenikowska-Ślusarz, T.; Domarecka, M. The prevalence and risk factors of orthorexia nervosa among school-age youth of Pomeranian and Warmian-Masurian voivodeships. Psychiatr. Pol. 2019, 53, 383–398. [Google Scholar] [CrossRef] [PubMed]
- Segura-Garcia, C.; Ramacciotti, C.; Rania, M.; Aloi, M.; Caroleo, M.; Bruni, A.; Gazzarrini, D.; Sinopoli, F.; De Fazio, P. The prevalence of orthorexia nervosa among eating disorder patients after treatment. Eat. Weight Disord. 2015, 20, 161–166. [Google Scholar] [CrossRef]
- Segura-García, C.; Papaianni, M.C.; Caglioti, F.; Procopio, L.; Nisticò, C.G.; Bombardiere, L.; Ammendolia, A.; Rizza, P.; De Fazio, P.; Capranica, L. Orthorexia nervosa: A frequent eating disordered behavior in athletes. Eat. Weight Disord. 2012, 17, e226–e233. [Google Scholar] [PubMed]
- Gramaglia, C.; Brytek-Matera, A.; Rogoza, R.; Zeppegno, P. Orthorexia and anorexia nervosa: Two distinct phenomena? A cross-cultural comparison of orthorexic behaviors in clinical and non-clinical samples. BMC Psychiatry 2017, 17, 75. [Google Scholar] [CrossRef]
- Parra-Fernandez, M.L.; Rodriguez-Cano, T.; Perez-Haro, M.J.; Onieva-Zafra, M.D.; Fernandez-Martinez, E.; Notario-Pacheco, B. Structural validation of ORTO-11-ES for diagnosis of orthorexia nervosa, Spanish version. Eat. Weight Disord. 2018, 23, 745–752. [Google Scholar] [CrossRef]
- Domingues, R.B.; Carmo, C. Orthorexia nervosa in yoga practitioners: Relationship with personality, attitudes about appearance, and yoga engagement. Eat. Weight Disord. 2021, 26, 789–795. [Google Scholar] [CrossRef]
- Barnes, M.A.; Caltabiano, M.L. The interrelationship between orthorexia nervosa, perfectionism, body image and attachment style. Eat. Weight Disord. 2017, 22, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Kiss-Leizer, M.; Rigó, A. People behind unhealthy obsession to healthy food: The personality profile of tendency to orthorexia nervosa. Eat. Weight Disord. 2019, 24, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Yung, J.J.; Tabri, N. The association of perfectionism, health-focused self-concept, and erroneous beliefs with orthorexia nervosa symptoms: A moderated mediation model. Int. J. Eat. Disord. 2022, 55, 892–901. [Google Scholar] [CrossRef]
- Noebel, N.A.; Oberle, C.D.; Marcell, H.S. Orthorexia nervosa and executive dysfunction: Symptomatology is related to difficulties with behavioural regulation. Eat. Weight Disord. 2022, 27, 2019–2026. [Google Scholar] [CrossRef]
- Eriksson, L.; Baigi, A.; Marklund, B.; Lindgren, E.C. Social physique anxiety and sociocultural attitudes toward appearance impact on orthorexia test in fitness participants. Scand. J. Med. Sci. Sports 2008, 18, 389–394. [Google Scholar] [CrossRef]
- Costanzo, G.; Marchetti, D.; Manna, G.; Verrocchio, M.C.; Falgares, G. The role of eating disorders features, psychopathology, and defence mechanisms in the comprehension of orthorexic tendencies. Eat. Weight Disord. 2022, 27, 2713–2724. [Google Scholar] [CrossRef]
- Kinzl, J.F.; Hauer, K.; Traweger, C.; Kiefer, I. Orthorexia nervosa in dieticians. Psychother. Psychosom. 2006, 75, 395–396. [Google Scholar] [CrossRef]
- Mutluer, G.; Yilmaz, D. Relationship between healthy eating fixation (Orthorexia) and past family life, and eating attitudes in young adults. Am. J. Health Educ. 2023, 54, 155–167. [Google Scholar] [CrossRef]
- Lasson, C.; Raynal, P. Personality profiles in young adults with orthorexic eating behaviours. Eat. Weight Disord. 2021, 26, 2727–2736. [Google Scholar] [CrossRef]
- Brytek-Matera, A.; Fonte, M.L.; Poggiogalle, E.; Donini, L.M.; Hellas, C. Orthorexia nervosa: Relationship with obsessive-compulsive symptoms, disordered eating patterns and body uneasiness among Italian university students. Eat. Weight Disord. 2017, 22, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Duran, S.; Çiçekoğlu, P. Relationship between orthorexia nervosa, muscle dysmorphic disorder (bigorexia), and self-confidence levels in male students. Perspect. Psychiatr. Care 2020, 56, 878. [Google Scholar] [CrossRef]
- Messer, M.; Liu, C.M.; McClure, Z.; Mode, J.; Tiffin, C.; Linardon, J. Negative body image components as risk factors for orthorexia nervosa: Prospective findings. Appetite 2022, 178, 106280. [Google Scholar] [CrossRef] [PubMed]
- Sfeir, M.; Malaeb, D.; Obeid, S.; Hallit, S. Association between religiosity and orthorexia nervosa with the mediating role of self-esteem among a sample of the Lebanese population–short communication. J. Eat. Disord. 2022, 10, 151. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, S. The connection between exercise addiction and orthorexia nervosa in German fitness sports. Eat. Weight Disord. 2018, 23, 581–586. [Google Scholar] [CrossRef]
- Valera, J.H.; Acuña Ruiz, P.; Romero Valdespino, B.; Visioli, F. Prevalence of orthorexia nervosa among ashtanga yoga practitioners: A pilot study. Eat. Weight Disord. 2014, 19, 469–472. [Google Scholar] [CrossRef]
- Bóna, E.; Szél, Z.; Kiss, D.; Gyarmathy, V.A. An unhealthy health behaviour: Analysis of orthorexic tendencies among Hungarian gym attendees. Eat. Weight Disord. 2019, 24, 13–20. [Google Scholar] [CrossRef]
- Dittfeld, A.; Gwizdek, K.; Jagielski, P.; Brzęk, A.; Ziora, K. Ocena związku pomiędzy ortoreksją a wegetarianizmem z użyciem BOT (Bratman Test for Orthorexia). Psychiatr. Pol. 2017, 51, 1133–1144. [Google Scholar] [CrossRef] [PubMed]
- Guglielmetti, M.; Ferraro, O.E.; Gorrasi, I.S.R.; Carraro, E.; Bo, S.; Abbate-Daga, G.; Tagliabue, A.; Ferraris, C. Lifestyle-Related Risk Factors of Orthorexia Can Differ among the Students of Distinct University Courses. Nutrients 2022, 14, 1111. [Google Scholar] [CrossRef] [PubMed]
- Voglino, G.; Bert, F.; Parente, B.; Lo Moro, G. Orthorexia Nervosa, a challenging evaluation: Analysis of a sample of customers from organic food stores. Psychol. Health Med. 2020, 26, 478–486. [Google Scholar] [CrossRef]
- Bundros, J.; Clifford, D.; Silliman, K.; Neyman Morris, M. Prevalence of Orthorexia nervosa among college students based on Bratman’s test and associated tendencies. Appetite 2016, 101, 86–94. [Google Scholar] [CrossRef]
- Plichta, M.; Jezewska-Zychowicz, M.; Gębski, J. Orthorexic tendency in Polish students: Exploring association with dietary patterns, body satisfaction and weight. Nutrients 2019, 11, 100. [Google Scholar] [CrossRef]
- Reynolds, R. Is the prevalence of orthorexia nervosa in an Australian university population 6.5%? Eat. Weight Disord. 2018, 23, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Dell’Osso, L.; Abelli, M.; Carpita, B.; Pini, S.; Castellini, G.; Carmassi, C.; Ricca, V. Historical evolution of the concept of anorexia nervosa and relationship with orthorexia nervosa, autism, and obsessive-compulsive spectrum. Neuropsychiatr. Dis. Treat. 2016, 12, 1651–1660. [Google Scholar] [PubMed]
- Dittfeld, A.; Gwizdek, K.; Koszowska, A.; Nowak, J.; Brończyk-Puzoń, A.; Jagielski, P.; Oświęcimska, J.; Ziora, K. Assessing the Risk of Orthorexia in Dietetic and Physiotherapy Students Using the BOT (Bratman Test for Orthorexia). Pediatr. Endocrinol. Diabetes Metab. 2016, 22, 6–14. [Google Scholar] [CrossRef]
- Bers, S.A.; Quinlan, D.M. Perceived-competence deficit in anorexia nervosa. J. Abnorm. Psychol. 1992, 101, 423–431. [Google Scholar] [CrossRef]
- Carter, J.C.; Kelly, A.C.; Norwood, S.J. Interpersonal problems in anorexia nervosa: Social inhibition as defining and detrimental. Personal. Individ. Differ. 2012, 53, 169–174. [Google Scholar] [CrossRef]
- Vuillier, L.; Robertson, S.; Greville-Harris, M. Orthorexic tendencies are linked with difficulties with emotion identification and regulation. J. Eat. Disord. 2020, 8, 15. [Google Scholar] [CrossRef] [PubMed]
- Dell’Osso, L.; Carpita, B.; Muti, D.; Cremone, I.M.; Massimetti, G.; Diadema, E.; Gesi, C.; Carmassi, C. Prevalence and characteristics of orthorexia nervosa in a sample of university students in Italy. Eat. Weight Disord. 2018, 23, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Kalika, E.; Egan, H.; Mantzios, M. Exploring the role of mindful eating and self-compassion on eating behaviours and orthorexia in people following a vegan diet. Eat. Weight Disord. 2022, 27, 2641–2651. [Google Scholar] [CrossRef] [PubMed]
- Miley, M.; Egan, H.; Wallis, D.; Mantzios, M. Orthorexia nervosa, mindful eating, and perfectionism: An exploratory investigation. Eat. Weight Disord. 2022, 27, 2869–2874. [Google Scholar] [CrossRef]
- Karniej, P.; Pérez, J.; Juárez-Vela, R.; Santolalla-Arnedo, I.; Gea-Caballero, V.; del Pozo-Herce, P.; Dissen, A.; Czapla, M. Orthorexia nervosa in gay men—The result of Spanish-Polish eating disorders study. BMC Public Health 2023, 23, 58. [Google Scholar] [CrossRef]
- Sanlier, N.; Yassibas, E.; Bilici, S.; Sahin, G.; Celik, B. Does the rise in eating disorders lead to increasing risk of orthorexia nervosa? Correlations with gender, education, and body mass index. Ecol. Food Nutr. 2016, 55, 266–278. [Google Scholar] [CrossRef] [PubMed]
- Gkiouleka, M.; Stavraki, C.; Sergentanis, T.N.; Vassilakou, T. Orthorexia Nervosa in Adolescents and Young Adults: A Literature Review. Children 2022, 9, 365. [Google Scholar] [CrossRef] [PubMed]
- White, M.; Berry, R.; Rodgers, R.F. Body Image and Body Change Behaviors Associated with Orthorexia Symptoms in Males. Body Image 2020, 34, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Agopyan, A.; Kenger, E.B.; Kermen, S.; Ulker, M.T.; Uzsoy, M.A.; Yetgin, M.K. The Relationship between Orthorexia Nervosa and Body Composition in Female Students of the Nutrition and Dietetics Department. Eat. Weight Disord. 2019, 24, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Arslantaş, H.; Adana, F.; Öğüt, S.; Ayakdaş, D.; Korkmaz, A. Relationship Between Eating Behaviors of Nursing Students and Orthorexia Nervosa (Obsession with Healthy Eating): A Cross-Sectional Study. J. Psychiatric Nurs. 2017, 8, 137–144. [Google Scholar] [CrossRef]
- Guerra, G.C.; Paone, A.; Lionetti, F.; Spinelli, M.; Fasolo, M.; D’Urso, G. The Role of Psychological Parental Control and Internalizing Problems in the Etiology of Vigorexia and Orthorexia in Adolescence. Children 2024, 11, 259. [Google Scholar] [CrossRef]
- Hyrnik, J.; Janas-Kozik, M.; Stochel, M.; Jelonek, I.; Siwiec, A.; Rybakowski, J.K. The Assessment of Orthorexia Nervosa Among 1899 Polish Adolescents Using the ORTO-15 Questionnaire. Int. J. Psychiatry Clin. Pract. 2016, 20, 199–203. [Google Scholar] [CrossRef]
- Pontillo, M.; Zanna, V.; Demaria, F.; Averna, R.; Di Vincenzo, C.; De Biase, M.; Di Luzio, M.; Foti, B.; Tata, M.C.; Vicari, S. Orthorexia Nervosa, Eating Disorders, and Obsessive-Compulsive Disorder: A Selective Review of the Last Seven Years. J. Clin. Med. 2022, 11, 6134. [Google Scholar] [CrossRef]
- Reynolds, R.; McMahon, S. Views of Health Professionals on the Clinical Recognition of Orthorexia Nervosa: A Pilot Study. Eat. Weight Disord. 2020, 25, 1117–1124. [Google Scholar] [CrossRef] [PubMed]
- Scheiber, R.; Diehl, S.; Karmasin, M. Socio-cultural power of social media on orthorexia nervosa: An empirical investigation on the mediating role of thin-ideal and muscular internalization, appearance comparison, and body dissatisfaction. Appetite 2023, 185, 106522. [Google Scholar] [CrossRef]
- López-Gil, J.F.; Chen, S.; Jiménez-López, E.; Abellán-Huerta, J.; Herrera-Gutiérrez, E.; Royo, J.M.P.; Mesas, A.E.; Tárraga-López, P.J. Are the Use and Addiction to Social Networks Associated with Disordered Eating Among Adolescents? Findings from the EHDLA Study. Int. J. Ment. Health Addict. 2023, 21, 1–15. [Google Scholar] [CrossRef]
- Yılmazel, G. Orthorexia Tendency and Social Media Addiction Among Candidate Doctors and Nurses. Perspect. Psychiatr. Care 2021, 57, 1846–1852. [Google Scholar] [CrossRef] [PubMed]
- Sanzari, C.M.; Hormes, J.M. U.S. Health Professionals’ Perspectives on Orthorexia Nervosa: Clinical Utility, Measurement and Diagnosis, and Perceived Influence of Sociocultural Factors. Eat. Weight Disord. 2023, 28, 31. [Google Scholar] [CrossRef]
- King, E.; Wengreen, H. Associations between level of interest in nutrition, knowledge of nutrition, and prevalence of orthorexia traits among undergraduate students. Nutr. Health 2023, 29, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Aktürk, U.; Gül, E.; Erci, B. The Effect of Orthorexia Nervosa Levels of Nursing Students and Diet Behaviors and Socio-Demographic Characteristics. Ecol. Food Nutr. 2019, 58, 397–409. [Google Scholar] [CrossRef] [PubMed]
- Erkin, Ö.; Kocaçal, E. Health perceptions and orthorexia nervosa tendencies among academics. Perspect. Psychiatr. Care 2022, 58, 2782–2790. [Google Scholar] [CrossRef] [PubMed]
- Aksoydan, E.; Camci, N. Prevalence of orthorexia nervosa among Turkish performance artists. Eat. Weight Disord. 2009, 14, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Villa, M.; Opawsky, N.; Manriquez, S.; Ananias, N.; Leonario-Rodriguez, M. Orthorexia nervosa risk and associated factors among Chilean nutrition students: A pilot study. J. Eat. Disord. 2022, 10, 6. [Google Scholar] [CrossRef] [PubMed]
- Valente, M.; Renckens, S.; Bunders-Aelen, J.; Syurina, E.V. The #orthorexia community on Instagram. Eat. Weight Disord. 2022, 27, 473–482. [Google Scholar]
| No. | Researcher | Purpose of the Survey | Research Methods | Study Group | Frequency | Results and Comments | |
|---|---|---|---|---|---|---|---|
| Number of Participants | Group Characteristics | ||||||
| 1 | [13] | How common ON 1 is and its interrelation with ED 2 and OCD 3 | ORTO-15 4, EAT-26 5, MOCI 6, individual questionnaire | 864 | 599 women aged 17 to 23 and 265 men aged 15 to 21 | 27%, a reading of 35 was regarded to be the cut-off point | ED 2 increases risk of ON 1; high BMI contributes to ON 1. The greatest danger was noted for those aged 13–16 and the smallest for those between 16–19 |
| 2 | [15] | Frequency of appearance ON 1 levels in women diagnosed with AN 7 and BN 8 | ORTO-15 4, YBC-EDS 9, Eat-26 5 | 32 | Females with a diagnosis of anorexia (AN 7) or bulimia (BN 8). | High prevalence of ON 1 among female patients with AN 7 and BN 8. The treatment was positive in the ORTO-15 4 test, which proved to be higher (28%) and (58%) than the control group, in which it was merely 6%. | AN 7 and BN 8 with a tendency towards ON 1 |
| 3 | [16] | Occurrence of similarities and dissimilarities between ON 1 and ED 2 in patients with AN 7 and BN 8 | ORTO-15 4, EAT-26 5, MDBSRQ 10 | 577 | Female ED 2 patients | Prevalence of ON 1 is notably high in women with AN 7 and BN 8. High performances on the ORTO-15 4 (28%) and EAT-26 5 (14%) were observed in athletes. | AN 7 and BN 8 increase the likelihood of ON 1 |
| 4 | [17] | Comparison of ON 1 and AN 7 between women with AN 7 and patients without diagnosed diseases | ORTO-15 4 | 136 | AN 7 patients from Italy and Poland | High prevalence of ON 1 among women with AN 7. In the Italian control group studied, 54% of participants scored 40 or more on the ORTO-15 4 test. 46% of this group may have orthorexic behavior | AN 7 predisposed to ON 1. Also, significant differences were detected between the Italian and Polish samples in the frequency of orthorexia nervosa and ORTO-15 4 scores, suggesting cultural differences requiring further investigation |
| 5 | [18] | Prevalence of ON 1 in students; a study of the relationship between ON 1 and psychological attitudes | ORTO-11-ES 11 Eating Disorder Inventory (EDI-2) 12 | 492 | The research group consisted of students from the University of Castilla-La Mancha in Spain (280 young women and 212 men) | The confirmatory factor analysis (CFA) identified 11 items and 3 attributes as the superior matching model; CFI 13 = 0.94, TLI 14 = 0.91, RMSEA 15 = 0.058 | Many behaviors resulting from ED 2 correlate with ON 1. ON 1 is more common in the female gender. |
| 6 | [19] | Observe the relationships between ON 1 and potential factors contributing to ON 1 in an international group of yoga practitioners | Teruel’s orthorexia nervosa scale, yoga immersion scale, passion scale, Frost’s perfectionism scale, NEO-PI-R self-discipline scale, EDI leanness scale, appearance beliefs scale | 469 | Yoga practitioners | Not determined | The pursuit of thinness was seen as a major risk factor for ON 1 |
| 7 | [20] | Examined whether perfectionism, figure disorders, relationships with the environment, and self-esteem bias contribute to the prognosis of ON 1 | OR ORTO-15 4, MPS, MBSRQ-AS, RSQ 16, RSES 17 | 220 | The survey group was 46 men and 174 women; 180 of those were first- and second-year psychology students at James Cook University | The mean score for ORTO-15 (based on nine items) was 22.71 (SD = 4.55). There was no significant difference in ORTO-15 4 scores between men and women | ON 1 correlates strongly with perfectionism, feelings of body satisfaction, and attachment style, especially in those with ED 2 present |
| 8 | [21] | The aim was to investigate the personality profile of people with a high orthorexic tendency | Temperament Character Inventory-56 (TCI-56), Ortho-11-Hu 18. | 739 | Participants’ ages ranged from 18 to 72 years. The research group consisted of doctors, athletes, nutritionists, performance artists, and Ashtanga yoga practitioners | The mean ORTO-11-Hu 18 score was 22.71 (SD = 4.55). The high ON 1 tendency group (score 14–29) comprised 234 subjects and the low ON 1 tendency group (score 35–43) comprised 245 subjects. Women were more likely than men to show high ON 1 tendencies | The psychological factors describe as one of the key symptoms of orthorexia nervosa may be its association with risk factors for AN 7 and BN 8 |
| 9 | [22] | To explore whether perfectionism and self-perception contribute to ON 1 symptoms in people with misconceptions about healthy eating | 12-item Clinical Perfectionism Questionnaire, 20-item Beliefs About Appearance Scale (BAAS), Orthorexia Nervosa Inventory (ONI) | 456 | The group consisted of 165 males and 287 females (4 reported gender as non-binary) ranging in age from 19 to 77 years old | In the table showing descriptive statistics and correlations, the frequency of orthorexia nervosa (ON 1) in the sample is 4.8% (n = 22) | Perfectionism is indirectly associated with ON 1 symptoms through health-focused self-awareness |
| 10 | [23] | The analyses examined whether the prevalence of orthorexia nervosa is associated with executive functioning disorders | Orthorexia Nervosa Inventory (ONI), BRIEF-A 19 | 405 | Among participants, 80% were female. Half Caucasian. Average age = 24 years; average BM 20 I = 25 | The prevalence of orthorexia nervosa (ON 1) symptoms was weakly to moderately correlated with all BRIEF-A 19 scales | In addition to their unique symptoms, orthorexia nervosa and anorexia may share similar neuropsychological characteristics |
| 11 | [24] | This study examined how scores on the SPAS 21 and the SATAQ 22 questionnaire relate to BOT 23 scores in relation to age, gender, and exercise durations | Sociocultural Attitudes Towards Appearance Questionnaire (SATAQ) 22 relate to Bratman’s orthorexia nervosa test (BOT) 23 | 251 | The group was made up of 85 men and 166 women. The age range was 17–62 years for men and 34 years for women. Most of the men (66%) and half of the women (50%) practiced between three to four times a week | Frequency of orthorexia nervosa (ON 1) was significantly correlated with internalization of the SATAQ subdomain in men (β = 0.14, p = 0.019). In women, the strongest factors were SPAS scores (β = 0.28, p < 0.0001) and frequency of exercise (β = 0.88, p < 0.0001) | Fitness center participants who exercised had high BOT 23 scores. Excessive exercise with pathological weight control woods the occurrence of pathological behavior and ED 2 |
| 12 | [25] | Investigate the associations between ON 1 and the core features of eating disorders (EDs), psychopathological symptoms, and defense mechanisms | ON 1 (EHQ-21) 24, eating psychopathology (EDI-3) 25, psychopathological symptoms (BSI) 26, and defense mechanisms (DSQ-40) 27 | 270 | Students from the University of Palermo in southern Italy and were assigned to three groups: 52 people with ON 1 symptoms, 157 people constituted a healthy eating control group and 61 people following a normal diet | Not specified | Group with ON 1 symptoms reported more ED 2 features, more psychopathological symptoms |
| No. | Researcher | Purpose of the Survey | Research Methods | Study Group | Frequency | Results and Comments | |
|---|---|---|---|---|---|---|---|
| Number of Participants | Group Characteristics | ||||||
| 1 | [6] | Impact of social media on ON 1 incidence in young adults | ORTO-15 2, web poll | 680 | The study group consisted of 23 men, 686 women, and 4 people identifying themselves as other | In the study group, mental orthorexia nervosa was present in 49% of the participants, a significantly higher rate compared to the general population, where it is less than 1%. | Risk of ON 1 increases with frequent use of Instagram |
| 2 | [53] | Correlation of orthorexia using SuperMimic software for healthy lifestyle and physical activity addiction | Internet survey Qualtrics 3, ORTO-7 4 | 113 | Undergraduate students aged 18–25 attending a large, private university in the northeastern United States | Relationship between ON 1 and ED 5 symptoms in most subjects | ON with high right-sidedness may occur in young men with ED |
| 3 | [55] | Determining the frequency of orthorexia nervosa in nursing students and the correlation between ED 5 and ON 1 | ORTO-11 6, EAT-40 7, | 181 | Nursing students | 45.3% | Nearly half of nursing students in residency suffering from ED 5 are at risk of having ON 1 |
| 4 | [56] | Impact of excessive parental control on the incidence of ON 1 in children during adolescence | ORTO-15 2 DAPCS 8 | 403 | The participants were Italian teenage athletes (231 boys and 172 girls) aged between 14 and 18 | Addiction-oriented control was linked to depression (b = 0.26; p < 0.001) and anxiety (b = 0.40; p < 0.001), while achievement-oriented control predicted depression (b = 0.28; p < 0.001) and anxiety (b = 0.32; p < 0.001) | Too much parental control can cause anxiety, leading to ON 1 incidences |
| 5 | [12] | Investigating the frequency of orthorexia nervosa in young athletes | ORTO-15 2 | 116 | The study group consisted of students with an average age of 21 ± 1 years and 99 non-athletes (21 ± 2) from universities in North East England who completed the ORTO-15 2 test, with a cut-off value of ≤40 | Symptoms of orthorexia nervosa were present in 76% of students. There was no significant difference in ORTO-15 2 scores between athletes (36.6 ± 3.9) and non-athletic students (37.2 ± 3.8; p = 0.279) | ON may occur in young students |
| 6 | [57] | Assessment of the prevalence of ON 1 in adolescents living in Poland | ORTO-15 2 | 1899 | The subjects were 992 girls and 907 boys aged 15 to 21 years old | The ORTO-15 2 value averaged 39.2 ± 3.6 points, with no gender difference | The incidence of ON 1 is similar to that estimated in adults |
| 7 | [7] | Analysis of the prevalence of orthorexia nervosa in medical students | ORTO-15 2, EAT-40 7 | 298 | Students of the Faculty of Medicine of the University of Inonu in 2017 | The prevalence of orthorexia nervosa among students was 76.2%, while 11.1% of students struggled with an eating disorder | The study postulates that health workers are more prone to orthorexia nervosa than other groups |
| 8 | [54] | The aim of this study is to investigate the correlation between ON and ED, body composition | EAT-40 7 ORTO-11 6 anthropometric measurements | 136 | Participants were female students who had scores on the Orthorexia nervosa Psychological Questionnaire (ORTO-11) 6 and the Eating Attitudes Test (EAT-40) 7 indicating the presence of orthorexia nervosa | The overwhelming proportion of participants (70.6%) obtained high scores on the ORTO-11 6 test | Female nutrition and dietetics students showed orthorexia nervosa tendencies |
| 9 | [8] | Investigating the association of ON 1 prevalence in dietetics students | ORTO-15 2 | 440 | The study group consisted of students from three different schools: 53 from the dietetic school, 200 from the exercise and sports science school, and 187 from the biology school | All schools showed a high prevalence of orthorexia nervosa traits: 35.9% in the dietetic school, 26.5% in the biology school, and 22.5% in the exercise and sports science school | There is a clear prevalence of orthorexia nervosa among dietetics students |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Łucka, I.; Mazur, A.; Łucka, A.; Sarzyńska, I.; Trojniak, J.; Kopańska, M. Orthorexia as an Eating Disorder Spectrum—A Review of the Literature. Nutrients 2024, 16, 3304. https://doi.org/10.3390/nu16193304
Łucka I, Mazur A, Łucka A, Sarzyńska I, Trojniak J, Kopańska M. Orthorexia as an Eating Disorder Spectrum—A Review of the Literature. Nutrients. 2024; 16(19):3304. https://doi.org/10.3390/nu16193304
Chicago/Turabian StyleŁucka, Izabela, Artur Mazur, Anna Łucka, Izabela Sarzyńska, Julia Trojniak, and Marta Kopańska. 2024. "Orthorexia as an Eating Disorder Spectrum—A Review of the Literature" Nutrients 16, no. 19: 3304. https://doi.org/10.3390/nu16193304
APA StyleŁucka, I., Mazur, A., Łucka, A., Sarzyńska, I., Trojniak, J., & Kopańska, M. (2024). Orthorexia as an Eating Disorder Spectrum—A Review of the Literature. Nutrients, 16(19), 3304. https://doi.org/10.3390/nu16193304