

The Long-Term Effect of Kidney Transplantation on the Serum Fatty Acid Profile



Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Fatty Acid Analysis
2.3. Statistical Analysis
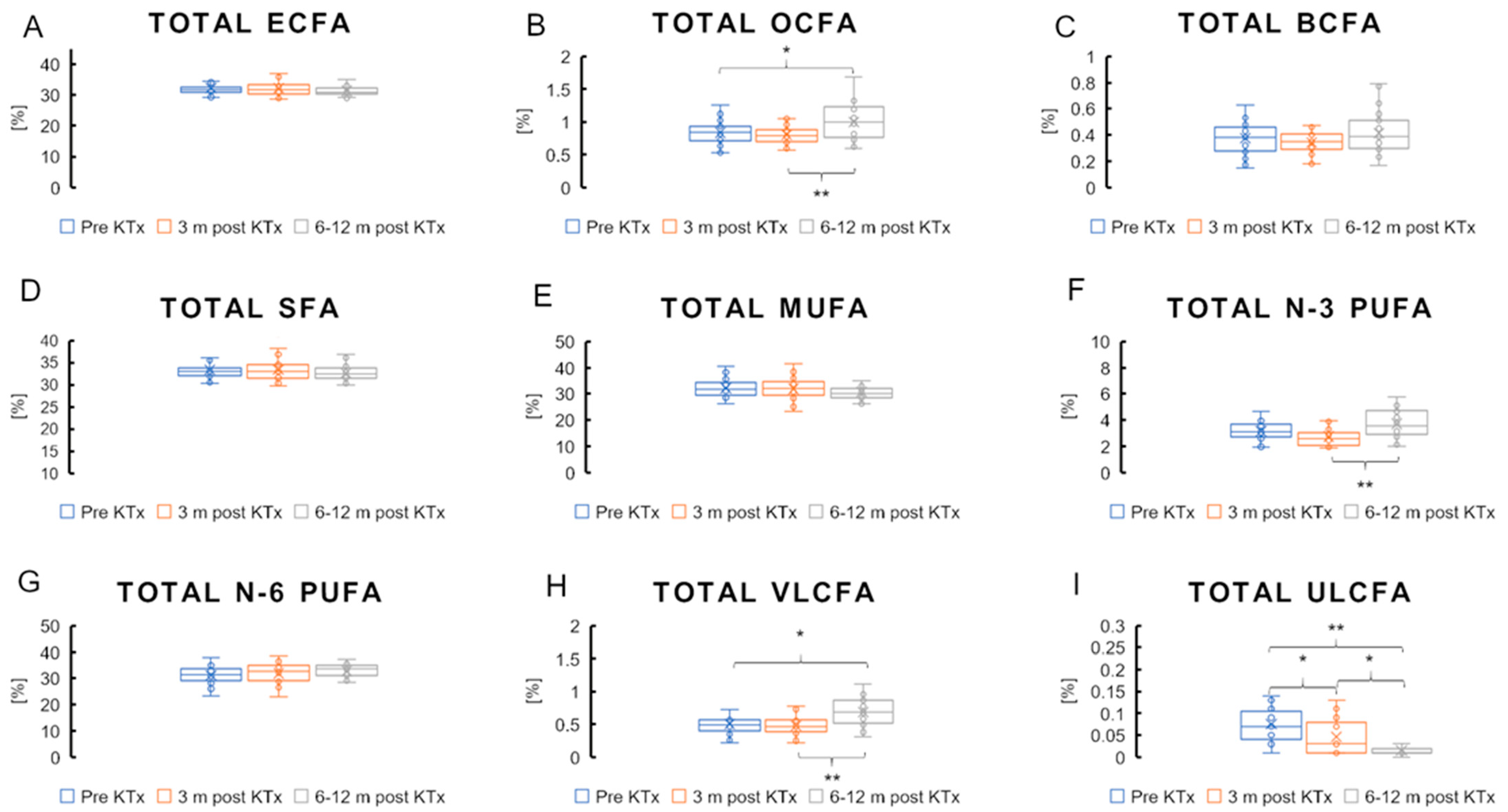
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hager, M.R.; Narla, A.D.; Tannock, L.R. Dyslipidemia in patients with chronic kidney disease. Rev. Endocr. Metab. Disord. 2017, 18, 29–40. [Google Scholar] [CrossRef]
- Pontremoli, R.; Bellizzi, V.; Bianchi, S.; Bigazzi, R.; Cernaro, V.; Del Vecchio, L.; De Nicola, L.; Leoncini, G.; Mallamaci, F.; Zoccali, C.; et al. Management of dyslipidaemia in patients with chronic kidney disease: A position paper endorsed by the Italian Society of Nephrology. J. Nephrol. 2020, 33, 417–430. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. Omega-3 fatty acids and inflammatory processes: From molecules to man. Biochem. Soc. Trans. 2017, 45, 1105–1115. [Google Scholar] [CrossRef]
- Calder, P.C. n−3 Polyunsaturated fatty acids, inflammation, and inflammatory diseases 2. Am. J. Clin. Nutr. 2006, 83, 1505S–1519S. [Google Scholar] [CrossRef] [PubMed]
- Mika, A.; Sikorska-Wiśniewska, M.; Małgorzewicz, S.; Stepnowski, P.; Dębska-Ślizień, A.; Śledziński, T.; Chmielewski, M. Potential contribution of monounsaturated fatty acids to cardiovascular risk in chronic kidney disease. Pol. Arch. Intern. Med. 2018, 128, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.-X.; Yu, J.-H.; Sun, J.-H.; Ma, W.-Q.; Wang, J.-J.; Sun, G.-J. Effects of Omega-3 Fatty Acids Supplementation on Serum Lipid Profile and Blood Pressure in Patients with Metabolic Syndrome: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Foods 2023, 12, 725. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.R., III; Juraschek, S.P.; Anderson, C.A.; Guallar, E.; Henoch-Ryugo, K.; Charleston, J.; Turban, S.; Bennett, M.R.; Appel, L.J. The Effects of n-3 Long-Chain Polyunsaturated Fatty Acid Supplementation on Biomarkers of Kidney Injury in Adults With Diabetes: Results of the GO-FISH trial. Diabetes Care 2013, 36, 1462–1469. [Google Scholar] [CrossRef] [PubMed]
- Sikorska-Wisniewska, M.; Mika, A.; Sledzinski, T.; Czaplinska, M.; Malgorzewicz, S.; Debska-Slizien, A.; Chmielewski, M. Disorders of Serum Polyunsaturated Fatty Acids in Renal Transplant Patients. Transplant. Proc. 2020, 52, 2324–2330. [Google Scholar] [CrossRef]
- Gammelmark, A.; Nielsen, M.S.; Bork, C.S.; Lundbye-Christensen, S.; Tjønneland, A.; Overvad, K.; Schmidt, E. Association of fish consumption and dietary intake of marine n-3 PUFA with myocardial infarction in a prospective Danish cohort study. Br. J. Nutr. 2016, 116, 167–177. [Google Scholar] [CrossRef]
- Zhong, N.; Han, P.; Wang, Y.; Zheng, C. Associations of polyunsaturated fatty acids with cardiovascular disease and mortality: A study of NHANES database in 2003–2018. BMC Endocr. Disord. 2023, 23, 185. [Google Scholar] [CrossRef]
- Śledziński, M.; Hliwa, A.; Gołębiewska, J.; Mika, A. The Impact of Kidney Transplantation on the Serum Fatty Acid Profile in Patients with End-Stage Kidney Disease. Nutrients 2022, 14, 772. [Google Scholar] [CrossRef] [PubMed]
- Jalalzadeh, M.; Mousavinasab, N.; Peyrovi, S.; Ghadiani, M.H. The impact of acute rejection in kidney transplantation on long-term allograft and patient outcome. Nephro-Urol. Mon. 2015, 7, e24439. [Google Scholar] [CrossRef]
- Małgorzewicz, S.; Ciechanowski, K.; Kozłowska, L.; Krzanowska, K.; Krzanowski, M.; Kaczkan, M.; Borek, P.; Jankowska, M.; Rutkowski, B.; Dębska-Ślizień, A. Nutrition recommendations in chronic kidney disease—The position of the working group of the Polish Nephrological Society. Ren. Dis. Transplant. Forum 2019, 12, 240–278. [Google Scholar]
- Tiwari, P.; Singh, N.; Sharma, B. Long Term Treatment of Corticostreroids May Cause Hepatotoxicity and Oxidative Damage: A Case Controlled Study. Indian J. Clin. Biochem. 2024, 39, 179–187. [Google Scholar] [CrossRef]
- Ko, M.S.; Choi, Y.H.; Jung, S.H.; Lee, J.S.; Kim, H.S.; Lee, C.H.; Kim, S.G. Tacrolimus therapy causes hepatotoxicity in patients with a history of liver disease. Int. J. Clin. Pharmacol. Ther. 2015, 53, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Chadban, S.J.; Barraclough, K.A.; Campbell, S.B.; Clark, C.J.; Coates, P.T.; Cohney, S.J.; Cross, N.B.; Eris, J.M.; Henderson, L.; Howell, M.R.; et al. KHA-CARI guideline: KHA-CARI adaptation of the KDIGO Clinical Practice Guideline for the Care of Kidney Transplant Recipients. Nephrology 2012, 17, 204–214. [Google Scholar] [CrossRef] [PubMed]
- Chan, M.; Patwardhan, A.; Ryan, C.; Trevillian, P.; Chadban, S.; Westgarth, F.; Fry, K. Evidence-based guidelines for the nutritional management of adult kidney transplant recipients. J. Ren. Nutr. 2011, 21, 47–51. [Google Scholar] [CrossRef]
- Lin, L.; Allemekinders, H.; Dansby, A.; Campbell, L.; Durance-Tod, S.; Berger, A.; Jones, P.J.H. Evidence of health benefits of canola oil. Nutr. Rev. 2013, 71, 370–385. [Google Scholar] [CrossRef]
- Mika, A.; Sledzinski, T. Alterations of specific lipid groups in serum of obese humans: A review. Obes. Rev. 2017, 18, 247–272. [Google Scholar] [CrossRef]
- Ma, B.; Gavzy, S.J.; France, M.; Song, Y.; Lwin, H.W.; Kensiski, A.; Saxena, V.; Piao, W.; Lakhan, R.; Iyyathurai, J.; et al. Rapid intestinal and systemic metabolic reprogramming in an immunosuppressed environment. BMC Microbiol. 2023, 23, 394. [Google Scholar] [CrossRef] [PubMed]
- Tory, R. The Study of the Effect of Immunosuppressive Drugs on Lipid Metabolism. Master’s Thesis, University of British Columbia, Vancouver, BC, Canada, 2008. [Google Scholar] [CrossRef]
- Massy, Z.A. Can we minimize long-term side effects of immunosuppressive drugs on lipid metabolism? In Immunosuppression under Trial: Proceedings of the 31st Conference on Transplantation and Clinical Immunology; Cochat, P., Traeger, J., Merieux, C., Derchavane, M., Eds.; Springer: Dordrecht, The Netherlands, 1999; pp. 105–109. [Google Scholar] [CrossRef]
- Mika, A.; Stepnowski, P.; Kaska, L.; Proczko, M.; Wisniewski, P.; Sledzinski, M.; Sledzinski, T. A comprehensive study of serum odd- and branched-chain fatty acids in patients with excess weight. Obesity 2016, 24, 1669–1676. [Google Scholar] [CrossRef]
- Abdoul-Aziz, S.K.A.; Zhang, Y.; Wang, J. Milk Odd and Branched Chain Fatty Acids in Dairy Cows: A Review on Dietary Factors and Its Consequences on Human Health. Animals 2021, 11, 3210. [Google Scholar] [CrossRef]
- Moyses-Neto, M.; Garcia, T.M.P.; Nardin, M.E.P.; Muglia, V.A.; Molina, C.A.F.; Romao, E.A. Causes of hypercalcemia in renal transplant recipients: Persistent hyperparathyroidism and others. Braz. J. Med. Biol. Res. 2021, 54, e10558. [Google Scholar] [CrossRef] [PubMed]
- To, N.B.; Nguyen, Y.T.-K.; Moon, J.Y.; Ediriweera, M.K.; Cho, S.K. Pentadecanoic Acid, an Odd-Chain Fatty Acid, Suppresses the Stemness of MCF-7/SC Human Breast Cancer Stem-Like Cells through JAK2/STAT3 Signaling. Nutrients 2020, 12, 1663. [Google Scholar] [CrossRef] [PubMed]
- Ediriweera, M.K.; To, N.B.; Lim, Y.; Cho, S.K. Odd-chain fatty acids as novel histone deacetylase 6 (HDAC6) inhibitors. Biochimie 2021, 186, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Venn-Watson, S.; Lumpkin, R.; Dennis, E.A. Efficacy of dietary odd-chain saturated fatty acid pentadecanoic acid parallels broad associated health benefits in humans: Could it be essential? Sci. Rep. 2020, 10, 8161. [Google Scholar] [CrossRef]
- Weitkunat, K.; Schumann, S.; Nickel, D.; Hornemann, S.; Petzke, K.J.; Schulze, M.B.; Pfeiffer, A.F.H.; Klaus, S. Odd-chain fatty acids as a biomarker for dietary fiber intake: A novel pathway for endogenous production from propionate. Am. J. Clin. Nutr. 2017, 105, 1544–1551. [Google Scholar] [CrossRef]
- Weitkunat, K.; Stuhlmann, C.; Postel, A.; Rumberger, S.; Fankhänel, M.; Woting, A.; Petzke, K.J.; Gohlke, S.; Schulz, T.J.; Blaut, M.; et al. Short-chain fatty acids and inulin, but not guar gum, prevent diet-induced obesity and insulin resistance through differential mechanisms in mice. Sci. Rep. 2017, 7, 6109. [Google Scholar] [CrossRef] [PubMed]
- Imamura, F.; Fretts, A.; Marklund, M.; Ardisson Korat, A.V.; Yang, W.-S.; Lankinen, M.; Qureshi, W.; Helmer, C.; Chen, T.-A.; Wong, K.; et al. Fatty acid biomarkers of dairy fat consumption and incidence of type 2 diabetes: A pooled analysis of prospective cohort studies. PLoS Med. 2018, 15, e1002670. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, T.; Shimada, K.; Hiki, M.; Kume, A.; Kitamura, Y.; Oshida, K.; Yanagisawa, N.; Kiyanagi, T.; Matsumori, R.; Daida, H. High hexacosanoic acid levels are associated with coronary artery disease. Atherosclerosis 2014, 233, 429–433. [Google Scholar] [CrossRef]
- Liu, M.; Zuo, L.-S.-Y.; Sun, T.-Y.; Wu, Y.-Y.; Liu, Y.-P.; Zeng, F.-F.; Chen, Y.-M. Circulating Very-Long-Chain Saturated Fatty Acids Were Inversely Associated with Cardiovascular Health: A Prospective Cohort Study and Meta-Analysis. Nutrients 2020, 12, 2709. [Google Scholar] [CrossRef]
- Okahashi, A.; Okada, T.; Saito, E.; Miyashita, M.; Kuromori, Y.; Iwata, F.; Hara, M.; Mugishima, H.; Kitamura, Y.; Shimizu, T. Concentrations of very long-chain fatty acid in whole blood are associated with cardiovascular risk factors in children. Clin. Chim. Acta 2009, 401, 141–143. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Parameters | Pre KTx | 3 m Post KTx | 6–12 m Post KTx | p | |||
|---|---|---|---|---|---|---|---|
| Pre vs. 3 m | Pre vs. 6–12 m | 3 m vs. 6–12 m | Reference Value | ||||
| n = 25 | |||||||
| Age | 50.3 ± 14.0 | ||||||
| Sex | M:13 F:12 | ||||||
| BMI (kg/m2) | 25.7 ± 3.29 | 25.8 ± 3.23 | 26.2 ± 3.36 | NS | NS | NS | 18.5–24.9 |
| Hemoglobin (g/dL) | 11.2 ± 1.43 | 12.6 ± 2.26 | 13.4 ± 1.91 | <0.05 | <0.001 | NS | 13.0–17.0 |
| eGFR-CKD (mL/min/1.73 m2) | 7.5 ± 3.35 | 49.8 ± 15.1 | 58.5 ± 15.6 | <0.001 | <0.001 | <0.05 | >60 |
| CRP (mg/L) | 7.9 ± 9.1 | 2.9 ± 6.6 | 2.7 ± 3.1 | <0.05 | 0.057 | NS | 0.0–5.0 |
| Creatinine (mg/dL) | 8.0 ± 2.8 | 1.5 ± 0.4 | 1.3 ± 0.3 | <0.001 | <0.001 | NS | 0.7–1.3 |
| Sodium (mmol/L) | 139 ± 2.24 | 141 ± 2.52 | 141 ± 2.70 | NS | NS | NS | 136–145 |
| Potassium (mmol/L) | 4.7 ± 0.1 | 4.4 ± 0.5 | 4.3 ± 0.5 | <0.05 | <0.05 | NS | 3.5–5.1 |
| ALT (U/L) | 20.5 ± 12.0 | 28.6 ± 18.5 | 51.8 ± 49.79 | NS | <0.05 | NS | <55 |
| AST (U/L) | 21.2 ± 13.4 | 22.8 ± 15.8 | 41.6 ± 38.32 | NS | NS | NS | 5–34 |
| TG (mg/dL) | 212 ± 151 | 196 ± 92 | 160 ± 130 | NS | NS | NS | <150 |
| CHOL (mg/dL) | 194 ± 52 | 232 ± 39 | 176 ± 28 | NS | NS | NS | 115–190 |
| Immunosuppressive drugs | |||||||
| MP + Tc + MM | n = 21 | ||||||
| MP + Cc + MM | n = 3 | ||||||
| MP + Tc | n = 1 | ||||||
| renal replacement therapy before KTx | |||||||
| Peritoneal Dialysis n = 6 Hemodialysis n = 17 | |||||||
| FA (%) | Pre KTx | 3 m Post KTx | 6–12 m Post KTx | p | ||
|---|---|---|---|---|---|---|
| Pre vs. 3 m | Pre vs. 6–12 m | 3 m vs. 6–12 m | ||||
| C14:0 | 1.20 ± 0.34 | 1.46 ± 0.60 | 1.51 ± 0.41 | NS | 0.031 | NS |
| C16:0 | 22.7 ± 1.49 | 23.2 ± 2.11 | 20.8 ± 2.01 | NS | <0.001 | <0.001 |
| C17:0 | 0.31 ± 0.053 | 0.30 ± 0.050 | 0.37 ± 0.093 | NS | NS | 0.008 |
| C19:0 | 0.020 ± 0.009 | 0.020 ± 0.007 | 0.033 ± 0.010 | NS | <0.001 | <0.001 |
| C20:0 | 0.12 ± 0.042 | 0.13 ± 0.038 | 0.20 ± 0.086 | NS | <0.001 | <0.001 |
| C21:0 | 0.020 ± 0.014 | 0.019 ± 0.008 | 0.032 ± 0.016 | NS | 0.024 | 0.010 |
| C22:0 | 0.21 ± 0.085 | 0.21 ± 0.068 | 0.32 ± 0.095 | NS | 0.024 | 0.010 |
| C23:0 | 0.066 ± 0.028 | 0.077 ± 0.030 | 0.122 ± 0.049 | NS | <0.001 | <0.001 |
| C24:0 | 0.22 ± 0.08 | 0.23 ± 0.08 | 0.33 ± 0.09 | NS | <0.001 | <0.001 |
| C25:0 | 0.052 ± 0.031 | 0.028 ± 0.020 | 0.016 ± 0.011 | <0.001 | <0.001 | 0.074 |
| C26:0 | 0.031 ± 0.021 | 0.020 ± 0.010 | 0.014 ± 0.008 | 0.021 | <0.001 | NS |
| C30:0 | 0.022 ± 0.010 | 0.009 ± 0.007 | traces | NS | <0.001 | <0.001 |
| C32:0 | 0.013 ± 0.005 | 0.004 ± 0.004 | traces | NS | <0.001 | <0.001 |
| iso C16:0 | 0.049 ± 0.017 | 0.054 ± 0.021 | 0.077 ± 0.033 | NS | <0.001 | 0.002 |
| iso C17:0 | 0.11 ± 0.030 | 0.10 ± 0.026 | 0.11 ± 0.050 | NS | NS | 0.051 |
| C14:1 | 0.05 ± 0.03 | 0.08 ± 0.05 | 0.08 ± 0.06 | NS | 0.060 | NS |
| C18:1 | 28.5 ± 2.73 | 28.0 ± 3.62 | 26.6 ± 3.55 | NS | 0.052 | NS |
| C20:1 | 0.14 ± 0.052 | 0.17 ± 0.078 | 0.25 ± 0.104 | NS | <0.001 | 0.004 |
| C22:1 | 0.022 ± 0.013 | 0.022 ± 0.010 | 0.030 ±0.016 | NS | 0.049 | 0.065 |
| C24:1 | 0.29 ± 0.11 | 0.32 ± 0.15 | 0.46 ± 0.19 | NS | <0.001 | <0.001 |
| ETA (20:4 n-3) | 0.076 ± 0.024 | 0.065 ± 0.034 | 0.107 ± 0.042 | NS | 0.020 | <0.001 |
| EPA (20:5 n-3) | 0.82 ± 0.22 | 0.79 ± 0.42 | 1.05 ± 0.38 | NS | 0.052 | 0.022 |
| DPAn3 (22:5 n-3) | 0.45 ± 0.094 | 0.39 ± 0.084 | 0.48 ± 0.11 | 0.057 | NS | 0.005 |
| DHA (22:6 n-3) | 1.55 ± 0.44 | 1.21 ± 0.43 | 1.65 ± 0.63 | 0.010 | NS | <0.001 |
| LA (18:2 n-6) | 23.0 ± 3.21 | 25.3 ± 3.96 | 24.5 ± 2.75 | 0.003 | 0.054 | NS |
| EDA (20:2 n-6) | 0.12 ± 0.040 | 0.13 ± 0.032 | 0.20 ± 0.056 | <0.001 | <0.001 | NS |
| DGLA (20:3 n-6) | 1.20 ± 0.39 | 0.95 ± 0.36 | 1.32 ± 0.34 | 0.009 | NS | <0.001 |
| ARA (20:4 n-6) | 6.45 ± 1.03 | 5.06 ± 0.90 | 6.25 ± 1.29 | <0.001 | NS | <0.001 |
| AdA (22:4 n-6) | 0.16 ± 0.039 | 0.13 ± 0.045 | 0.18 ± 0.061 | NS | NS | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Śledziński, M.; Gołębiewska, J.; Mika, A. The Long-Term Effect of Kidney Transplantation on the Serum Fatty Acid Profile. Nutrients 2024, 16, 3319. https://doi.org/10.3390/nu16193319
Śledziński M, Gołębiewska J, Mika A. The Long-Term Effect of Kidney Transplantation on the Serum Fatty Acid Profile. Nutrients. 2024; 16(19):3319. https://doi.org/10.3390/nu16193319
Chicago/Turabian StyleŚledziński, Maciej, Justyna Gołębiewska, and Adriana Mika. 2024. "The Long-Term Effect of Kidney Transplantation on the Serum Fatty Acid Profile" Nutrients 16, no. 19: 3319. https://doi.org/10.3390/nu16193319