
Vitamin D Deficiency as a Contributing Factor to Chronic Rhinitis in Middle-Aged and Older Adults: An Epidemiological Study


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Assessment of Chronic Rhinitis
2.3. Measurement of Serum 25-Hydroxy Vitamin D Level
2.4. Statistical Analysis
3. Results
3.1. Baseline Demographic and Lifestyle Factors According to Chronic Rhinitis
3.2. Demographic and Lifestyle Factors on Vitamin D Status and Its Association with Chronic Rhinitis
3.3. Multiple Logistic Regression Analyses of Vitamin D Status Deficiency and Chronic Rhinitis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dykewicz, M.S.; Wallace, D.V.; Amrol, D.J.; Baroody, F.M.; Bernstein, J.A.; Craig, T.J.; Dinakar, C.; Ellis, A.K.; Finegold, I.; Golden, D.B.K.; et al. Rhinitis 2020: A practice parameter update. J. Allergy Clin. Immunol. 2020, 146, 721–767. [Google Scholar] [CrossRef] [PubMed]
- Avdeeva, K.S.; Fokkens, W.J.; Segboer, C.L.; Reitsma, S. The prevalence of non-allergic rhinitis phenotypes in the general population: A cross-sectional study. Allergy 2022, 77, 2163–2174. [Google Scholar] [CrossRef]
- Baptist, A.P.; Nyenhuis, S. Rhinitis in the Elderly. Immunol. Allergy Clin. N. Am. 2016, 36, 343–357. [Google Scholar] [CrossRef]
- Hellings, P.W.; Klimek, L.; Cingi, C.; Agache, I.; Akdis, C.; Bachert, C.; Bousquet, J.; Demoly, P.; Gevaert, P.; Hox, V.; et al. Non-allergic rhinitis: Position paper of the European Academy of Allergy and Clinical Immunology. Allergy 2017, 72, 1657–1665. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Barragan, M.; Good, M.; Kolls, J.K. Regulation of Dendritic Cell Function by Vitamin D. Nutrients 2015, 7, 8127–8151. [Google Scholar] [CrossRef]
- Anderson, J.; Do, L.A.H.; Toh, Z.Q.; Hoe, E.; Reitsma, A.; Mulholland, K.; Licciardi, P.V. Vitamin D Induces Differential Effects on Inflammatory Responses During Bacterial and/or Viral Stimulation of Human Peripheral Blood Mononuclear Cells. Front. Immunol. 2020, 11, 602. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, B.; El Abd, A.; Ducharme, F.M. Effects of Vitamin D Supplementation on COVID-19 Related Outcomes: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 2134. [Google Scholar] [CrossRef]
- Feng, Q.; Bønnelykke, K.; Ek, W.E.; Chawes, B.L.; Yuan, S.; Cheung, C.L.; Li, G.H.; Leung, R.Y.; Cheung, B.M. Null association between serum 25-hydroxyvitamin D levels with allergic rhinitis, allergic sensitization and non-allergic rhinitis: A Mendelian randomization study. Clin. Exp. Allergy 2021, 51, 78–86. [Google Scholar] [CrossRef]
- Bakhshaee, M.; Sharifian, M.; Esmatinia, F.; Rasoulian, B.; Mohebbi, M. Therapeutic effect of vitamin D supplementation on allergic rhinitis. Eur. Arch. Otorhinolaryngol. 2019, 276, 2797–2801. [Google Scholar] [CrossRef]
- Yepes-Nuñez, J.J.; Brożek, J.L.; Fiocchi, A.; Pawankar, R.; Cuello-García, C.; Zhang, Y.; Morgano, G.P.; Agarwal, A.; Gandhi, S.; Terracciano, L.; et al. Vitamin D supplementation in primary allergy prevention: Systematic review of randomized and non-randomized studies. Allergy 2018, 73, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Kim, K.W.; Kim, M.J.; Sol, I.S.; Yoon, S.H.; Ahn, H.S.; Kim, H.J.; Sohn, M.H.; Kim, K.E. Vitamin D levels in allergic rhinitis: A systematic review and meta-analysis. Pediatr. Allergy Immunol. 2016, 27, 580–590. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.W.; Kim, J.Y.; Cho, S.H.; Choi, B.W.; Min, K.U.; Kang, H.R. Allergic rhinitis and serum 25-hydroxyvitamin D level in Korean adults. Ann. Allergy Asthma Immunol. 2013, 111, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Frieri, M.; Valluri, A. Vitamin D deficiency as a risk factor for allergic disorders and immune mechanisms. Allergy Asthma Proc. 2011, 32, 438–444. [Google Scholar] [CrossRef]
- Tian, H.Q.; Cheng, L. The role of vitamin D in allergic rhinitis. Asia Pac. Allergy 2017, 7, 65–73. [Google Scholar] [CrossRef]
- Changhai, L.; Zaichun, W.; Bo, Y.; Dan, L.; Shaohua, W. Micronutrients and Allergic Diseases: A Mendelian Randomization Study. Int. Arch. Allergy Immunol. 2024, 6, 1–11. [Google Scholar] [CrossRef]
- Pinto, J.M.; Jeswani, S. Rhinitis in the geriatric population. Allergy Asthma Clin. Immunol. 2010, 6, 10. [Google Scholar] [CrossRef]
- Mousavi, S.E.; Amini, H.; Heydarpour, P.; Amini Chermahini, F.; Godderis, L. Air pollution, environmental chemicals, and smoking may trigger vitamin D deficiency: Evidence and potential mechanisms. Environ. Int. 2019, 122, 67–90. [Google Scholar] [CrossRef]
- Lee, K. Sex-specific relationships between alcohol consumption and vitamin D levels: The Korea National Health and Nutrition Examination Survey 2009. Nutr. Res. Pract. 2012, 6, 86–90. [Google Scholar] [CrossRef]
- Looker, A.C. Do body fat and exercise modulate vitamin D status? Nutr. Rev. 2007, 65, S124–S126. [Google Scholar] [CrossRef]
- Choi, J.H.; Lee, B.; Lee, J.Y.; Kim, C.H.; Park, B.; Kim, D.Y.; Kim, H.J.; Park, D.Y. Relationship between Sleep Duration, Sun Exposure, and Serum 25-Hydroxyvitamin D Status: A Cross-sectional Study. Sci. Rep. 2020, 10, 4168. [Google Scholar] [CrossRef] [PubMed]
- Fiamenghi, V.I.; Mello, E.D. Vitamin D deficiency in children and adolescents with obesity: A meta-analysis. J. Pediatr (Rio J). 2021, 97, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Forman, J.P.; Giovannucci, E.; Holmes, M.D.; Bischoff-Ferrari, H.A.; Tworoger, S.S.; Willett, W.C.; Curhan, G.C. Plasma 25-hydroxyvitamin D levels and risk of incident hypertension. Hypertension 2007, 49, 1063–1069. [Google Scholar] [CrossRef]
- Mitri, J.; Muraru, M.D.; Pittas, A.G. Vitamin D and type 2 diabetes: A systematic review. Eur. J. Clin. Nutr. 2011, 65, 1005–1015. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Peng, M.; Chen, S.; Wu, S.; Zhang, W. Vitamin D deficiency is associated with dyslipidemia: A cross-sectional study in 3788 subjects. Curr. Med. Res. Opin. 2019, 35, 1059–1063. [Google Scholar] [CrossRef]
- Carlberg, C.; Velleuer, E. Vitamin D and Aging: Central Role of Immunocompetence. Nutrients 2024, 16, 398. [Google Scholar] [CrossRef]
- Ruggiero, C.; Tafaro, L.; Cianferotti, L.; Tramontana, F.; Macchione, I.G.; Caffarelli, C.; Virdis, A.; Ferracci, M.; Rinonapoli, G.; Mecocci, P.; et al. Targeting the Hallmarks of Aging with Vitamin D: Starting to Decode the Myth. Nutrients 2024, 16, 906. [Google Scholar] [CrossRef]
- Ferri, E.; Casati, M.; Cesari, M.; Vitale, G.; Arosio, B. Vitamin D in physiological and pathological aging: Lesson from centenarians. Rev. Endocr. Metab. Disord. 2019, 20, 273–282. [Google Scholar] [CrossRef]
- Sempos, C.T.; Vesper, H.W.; Phinney, K.W.; Thienpont, L.M.; Coates, P.M. Vitamin D status as an international issue: National surveys and the problem of standardization. Scand. J. Clin. Lab. Investig. Suppl. 2012, 243, 32–40. [Google Scholar] [CrossRef]
- Rosen, C.J. Clinical practice. Vitamin D insufficiency. N. Engl. J. Med. 2011, 364, 248–254. [Google Scholar] [CrossRef]
- Holick, M.F.; Chen, T.C. Vitamin D deficiency: A worldwide problem with health consequences. Am. J. Clin. Nutr. 2008, 87, 1080s–1086s. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: What clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Pantazidou, G.; Papaioannou, I.; Skoulakis, C.; Petinaki, E.; Hajiioannou, J. Vitamin D Levels in Chronic Rhinosinusitis in Patients With or Without Nasal Polyposis: A Systematic Review. Cureus 2023, 15, e46275. [Google Scholar] [CrossRef] [PubMed]
- Gaudet, M.; Plesa, M.; Mogas, A.; Jalaleddine, N.; Hamid, Q.; Al Heialy, S. Recent advances in vitamin D implications in chronic respiratory diseases. Respir. Res. 2022, 23, 252. [Google Scholar] [CrossRef]
- Zheng, S.; Yang, J.; Hu, X.; Li, M.; Wang, Q.; Dancer, R.C.A.; Parekh, D.; Gao-Smith, F.; Thickett, D.R.; Jin, S. Vitamin D attenuates lung injury via stimulating epithelial repair, reducing epithelial cell apoptosis and inhibits TGF-β induced epithelial to mesenchymal transition. Biochem. Pharmacol. 2020, 177, 113955. [Google Scholar] [CrossRef]
- Canpolat, U.; Özcan, F.; Özeke, Ö.; Turak, O.; Yayla, Ç.; Açıkgöz, S.K.; Çay, S.; Topaloğlu, S.; Aras, D.; Aydoğdu, S. Impaired cardiac autonomic functions in apparently healthy subjects with vitamin D deficiency. Ann. Noninvasive Electrocardiol. 2015, 20, 378–385. [Google Scholar] [CrossRef]
- Dimova, R.; Tankova, T.; Chakarova, N. Vitamin D in the Spectrum of Prediabetes and Cardiovascular Autonomic Dysfunction. J. Nutr. 2017, 147, 1607–1615. [Google Scholar] [CrossRef]
- Mulligan, J.K.; Bleier, B.S.; O’Connell, B.; Mulligan, R.M.; Wagner, C.; Schlosser, R.J. Vitamin D3 correlates inversely with systemic dendritic cell numbers and bone erosion in chronic rhinosinusitis with nasal polyps and allergic fungal rhinosinusitis. Clin. Exp. Immunol. 2011, 164, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Stokes, P.J.; Rimmer, J. The relationship between serum vitamin D and chronic rhinosinusitis: A systematic review. Am. J. Rhinol. Allergy 2016, 30, 23–28. [Google Scholar] [CrossRef]
- Song, H.R.; Kweon, S.S.; Choi, J.S.; Rhee, J.A.; Lee, Y.H.; Nam, H.S.; Jeong, S.K.; Park, K.S.; Ryu, S.Y.; Choi, S.W.; et al. High prevalence of vitamin D deficiency in adults aged 50 years and older in Gwangju, Korea: The Dong-gu Study. J. Korean Med. Sci. 2014, 29, 149–152. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | Chronic Rhinitis | |||
|---|---|---|---|---|
| Yes n (%) | No n (%) | p-Value | ||
| N | 2668 (21.1%) | 9986 (78.9%) | ||
| Age (year) | 40–49 | 788 (29.5%) | 2386 (23.9%) | <0.001 |
| 50–59 | 767 (28.7%) | 2660 (26.6%) | ||
| 60–69 | 583 (21.9%) | 2502 (25.1%) | ||
| 70–79 | 445 (16.7%) | 1975 (19.8%) | ||
| 80–89 | 80 (3.0%) | 454 (4.5%) | ||
| ≥90 | 5 (0.2%) | 9 (0.1%) | ||
| Sex | Male | 1187(44.5%) | 4263 (42.7%) | 0.095 |
| Female in menopause | 1481 (55.5%) | 5723 (57.3%) | ||
| Obesity | Underweight | 76 (2.9%) | 294 (2.9%) | 0.011 |
| Normal | 1734 (65.1%) | 6176 (62.0%) | ||
| Overweight | 853 (32.0%) | 3497 (35.1%) | ||
| Hypertension | No | 1860 (69.7%) | 6665 (66.7%) | 0.003 |
| Yes | 808 (30.3%) | 3321 (33.2%) | ||
| Diabetes | No | 2383 (89.3%) | 8794 (88.1%) | 0.073 |
| Yes | 285 (10.7%) | 1192 (11.9%) | ||
| Hyperlipidemia | No | 2281 (85.5%) | 8622 (86.4%) | 0.269 |
| Yes | 386 (14.5%) | 1362 (13.6%) | ||
| Hypercholesterolemia | No | 1982 (81.9%) | 7222 (80.8%) | 0.206 |
| Yes | 438 (18.1%) | 1720 (19.2%) | ||
| Hypertriglyceridemia | No | 1767 (83.7%) | 6495 (83.0%) | 0.457 |
| Yes | 345 (16.3%) | 1332 (17.0%) | ||
| Smoking status | No | 2124 (82.0%) | 7967 (82.5%) | 0.606 |
| Yes | 465 (18.0%) | 1693 (17.5%) | ||
| Alcohol drinking | No | 1333 (51.6%) | 5137 (53.4%) | 0.121 |
| Yes | 1248 (48.4%) | 4490 (46.6%) | ||
| Regular exercise (hard) | No | 2252 (87.0%) | 8426 (87.4%) | 0.649 |
| Yes | 336 (13.0%) | 859 (12.6%) | ||
| Regular exercise (moderate) | No | 2372 (91.8%) | 8790 (91.1%) | 0.264 |
| Yes | 212 (8.2%) | 1220 (8.9%) | ||
| Sleep duration (hour) | <6 | 508 (20.2%) | 1823 (19.4%) | 0.252 |
| 6 to 9 | 1914 (75.9%) | 7126 (75.9%) | ||
| ≥10 | 99 (3.9%) | 435 (4.6%) | ||
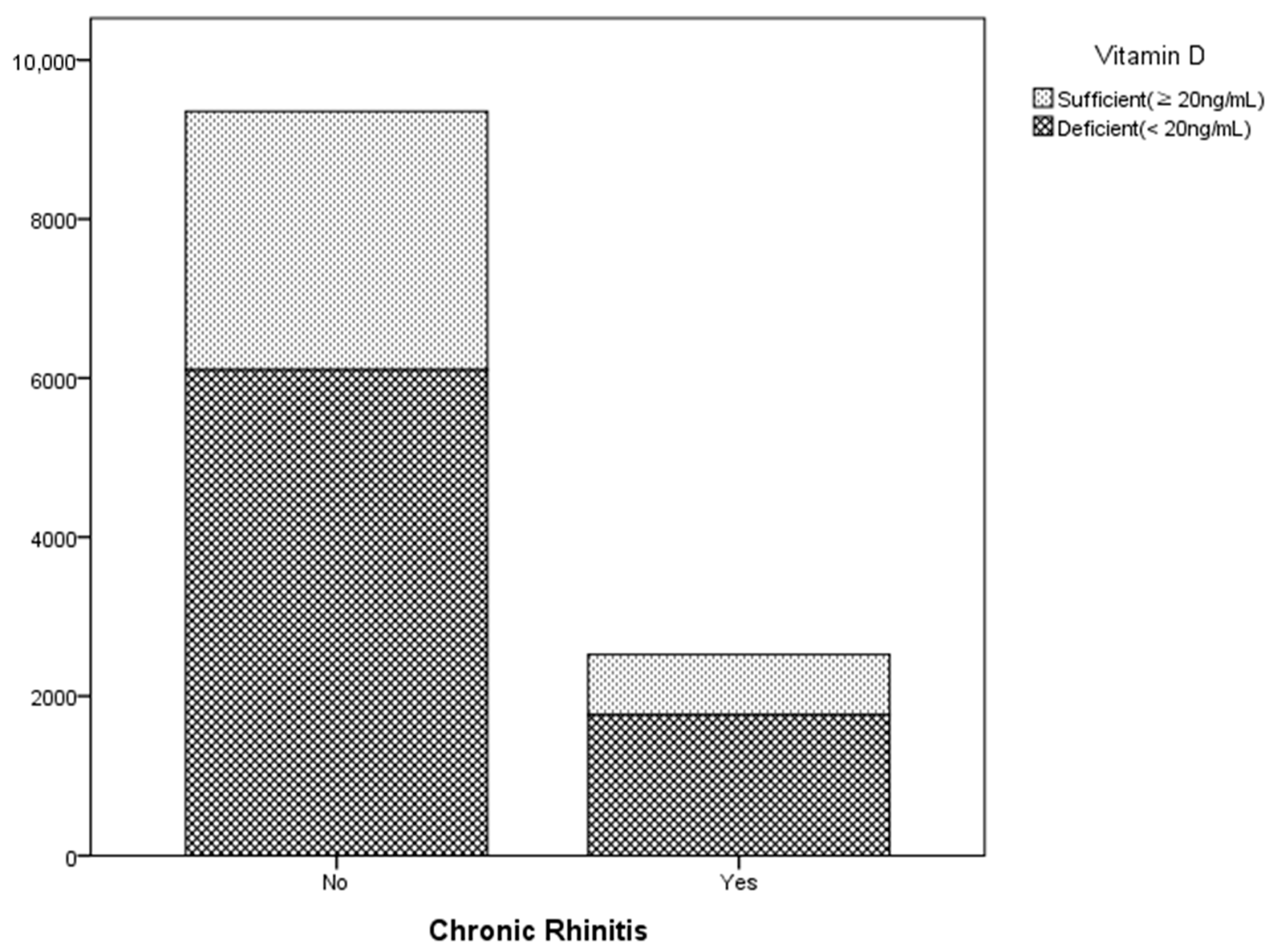
| Vitamin D level (ng/mL) | <20 | 1764 (69.9%) | 6103 (65.2%) | <0.001 |
| ≥20 | 758 (30.1%) | 3252 (34.8%) | ||
| Variable | Vit. D (ng/mL) | Vit. D (ng/mL) <20 ng/mL | Vit. D (ng/mL) >20 ng/mL | p-Value | |
|---|---|---|---|---|---|
| Geometric Mean | % | % | |||
| Age (year) | 40–49 | 16.75 | 29.9 | 18.7 | <0.001 |
| 50–59 | 18.25 | 28.3 | 27.5 | ||
| 60–69 | 19.03 | 22.3 | 29.0 | ||
| 70–79 | 18.91 | 16.6 | 21.2 | ||
| 80–89 | 18.99 | 2.8 | 3.5 | ||
| ≥90 | 17.35 | 0.1 | 0.1 | ||
| Sex | Male | 19.36 | 38.8 | 53.6 | <0.001 |
| Female | 17.28 | 61.2 | 46.4 | ||
| Obesity | Underweight | 18.32 | 2.5 | 2.9 | 0.037 |
| Normal | 18.26 | 62.1 | 63.9 | ||
| Overweight | 18.07 | 35.3 | 33.1 | ||
| Hypertension | No | 18.08 | 69.2 | 66.7 | 0.005 |
| Yes | 18.43 | 30.8 | 33.3 | ||
| Diabetes | No | 18.17 | 89.0 | 88.3 | 0.246 |
| Yes | 18.33 | 11.0 | 11.7 | ||
| Hyperlipidemia | No | 18.15 | 86.7 | 85.7 | 0.161 |
| Yes | 18.44 | 13.3 | 14.3 | ||
| Hypercholesterolemia | No | 18.25 | 81.0 | 81.2 | 0.773 |
| Yes | 18.13 | 19.0 | 18.8 | ||
| Hypertriglyceridemia | No | 18.31 | 82.3 | 84.7 | 0.002 |
| Yes | 17.68 | 17.7 | 15.3 | ||
| Smoking status | Non-smoker | 18.11 | 82.8 | 80.4 | 0.002 |
| Smoker | 18.71 | 17.2 | 19.6 | ||
| Alcohol drinking | No | 17.76 | 53.6 | 48.5 | <0.001 |
| Yes | 18.71 | 46.4 | 51.5 | ||
| Regular exercise (hard) | No | 18.11 | 87.6 | 85.4 | 0.001 |
| Yes | 18.87 | 12.4 | 14.6 | ||
| Regular exercise (moderate) | No | 18.11 | 91.7 | 89.9 | 0.001 |
| Yes | 19.27 | 8.3 | 10.1 | ||
| Sleep duration (hour) | <6 | 18.02 | 19.5 | 18.5 | 0.13 |
| 6 to 9 | 18.20 | 76.5 | 76.9 | ||
| ≥10 | 18.71 | 4.0 | 4.7 | ||
| Chronic rhinitis | No | 18.19 | 77.6 | 81.1 | <0.001 |
| Yes | 17.73 | 22.4 | 18.9 | ||
| Parameter | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | ||
| Chronic rhinitis | Yes | 1.24 | 1.127–1.364 | <0.001 | 1.22 | 1.105–1.342 | <0.001 | 1.25 | 1.132–1.379 | <0.001 | 1.24 | 1.115–1.377 | <0.001 | 1.21 | 1.082–1.348 | 0.001 |
| No | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | 1 (Ref) | |||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.C.; Park, D.-Y. Vitamin D Deficiency as a Contributing Factor to Chronic Rhinitis in Middle-Aged and Older Adults: An Epidemiological Study. Nutrients 2024, 16, 3385. https://doi.org/10.3390/nu16193385
Park SC, Park D-Y. Vitamin D Deficiency as a Contributing Factor to Chronic Rhinitis in Middle-Aged and Older Adults: An Epidemiological Study. Nutrients. 2024; 16(19):3385. https://doi.org/10.3390/nu16193385
Chicago/Turabian StylePark, Sang Chul, and Do-Yang Park. 2024. "Vitamin D Deficiency as a Contributing Factor to Chronic Rhinitis in Middle-Aged and Older Adults: An Epidemiological Study" Nutrients 16, no. 19: 3385. https://doi.org/10.3390/nu16193385