Composition and Antioxidant Status of Human Milk of Women Living in Bydgoszcz (Poland)

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
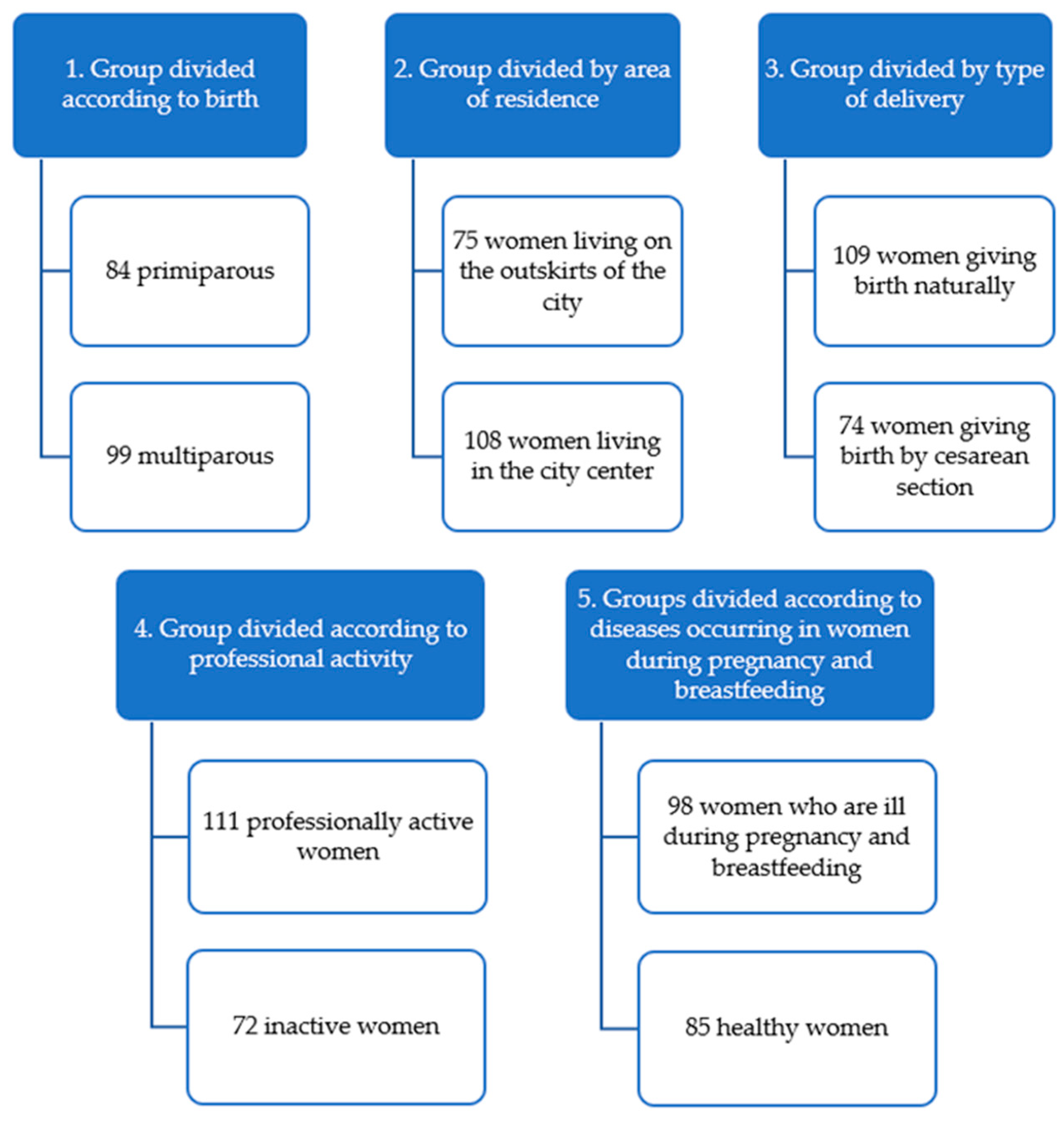
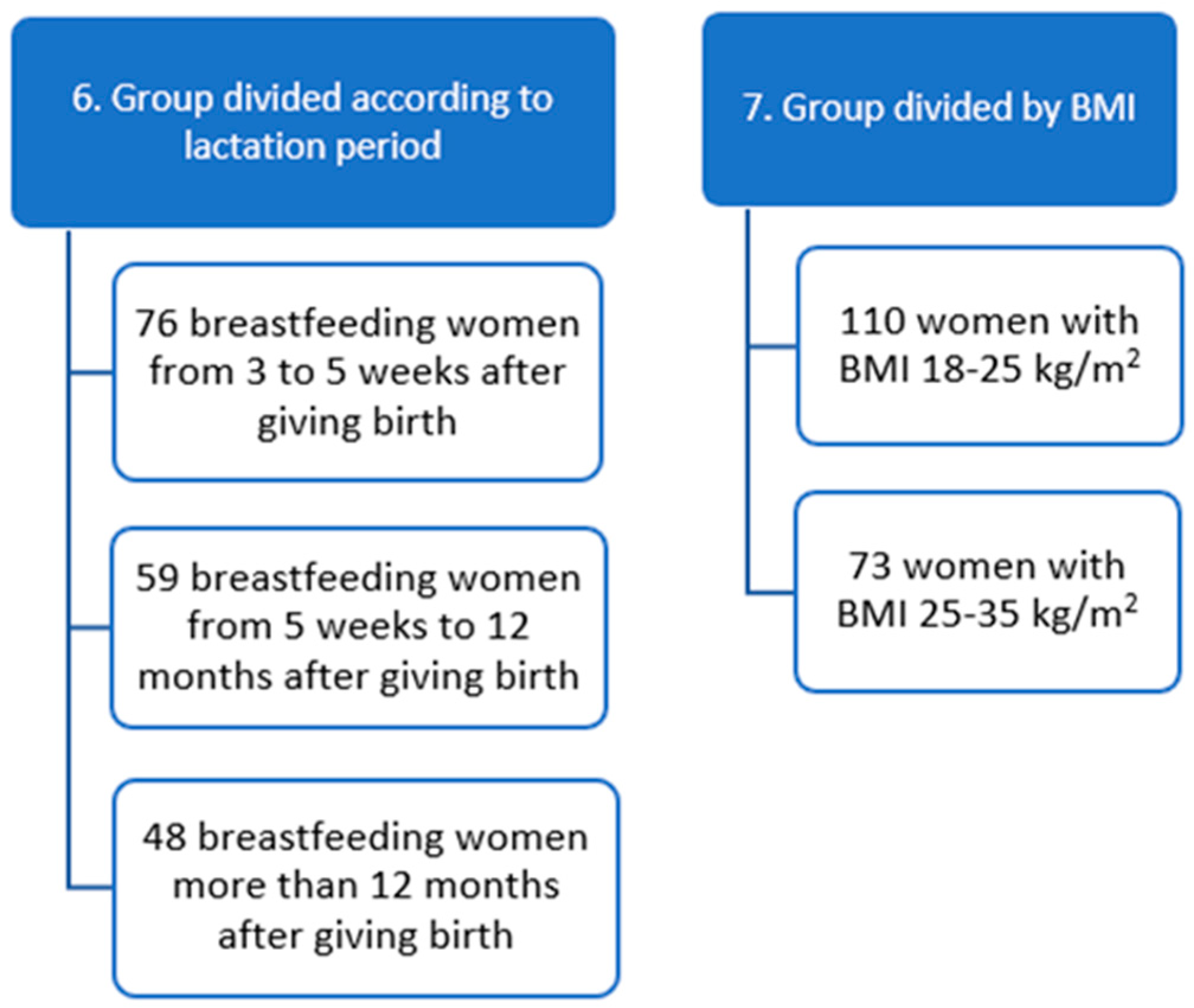
2.1. Study Group
2.2. Materials
2.2.1. Determination of the Basic Composition of Human Milk
2.2.2. Determination of Cortisol Concentration in Human Milk
2.2.3. Analysis of the Antioxidant Status of Human Milk
Determination in Human Milk Samples
Determination of the Ability of Human Milk to Reduce Fe (III) Ions
2.3. Statistical Analysis
- |rs| < 0.2—no linear relationship.
- 0.2 ≤ |rs| < 0.4—weak dependency.
- 0.4 ≤ |rs| < 0.7—moderate dependence.
- 0.7 ≤ |rs| < 0.9—strong dependency.
- |rs| ≥ 0.9—a very strong dependency.
3. Results
3.1. Characteristics of Study Groups
3.2. Analysis of Cortisol Concentration, Basic Composition, and Antioxidant Status of Human Milk
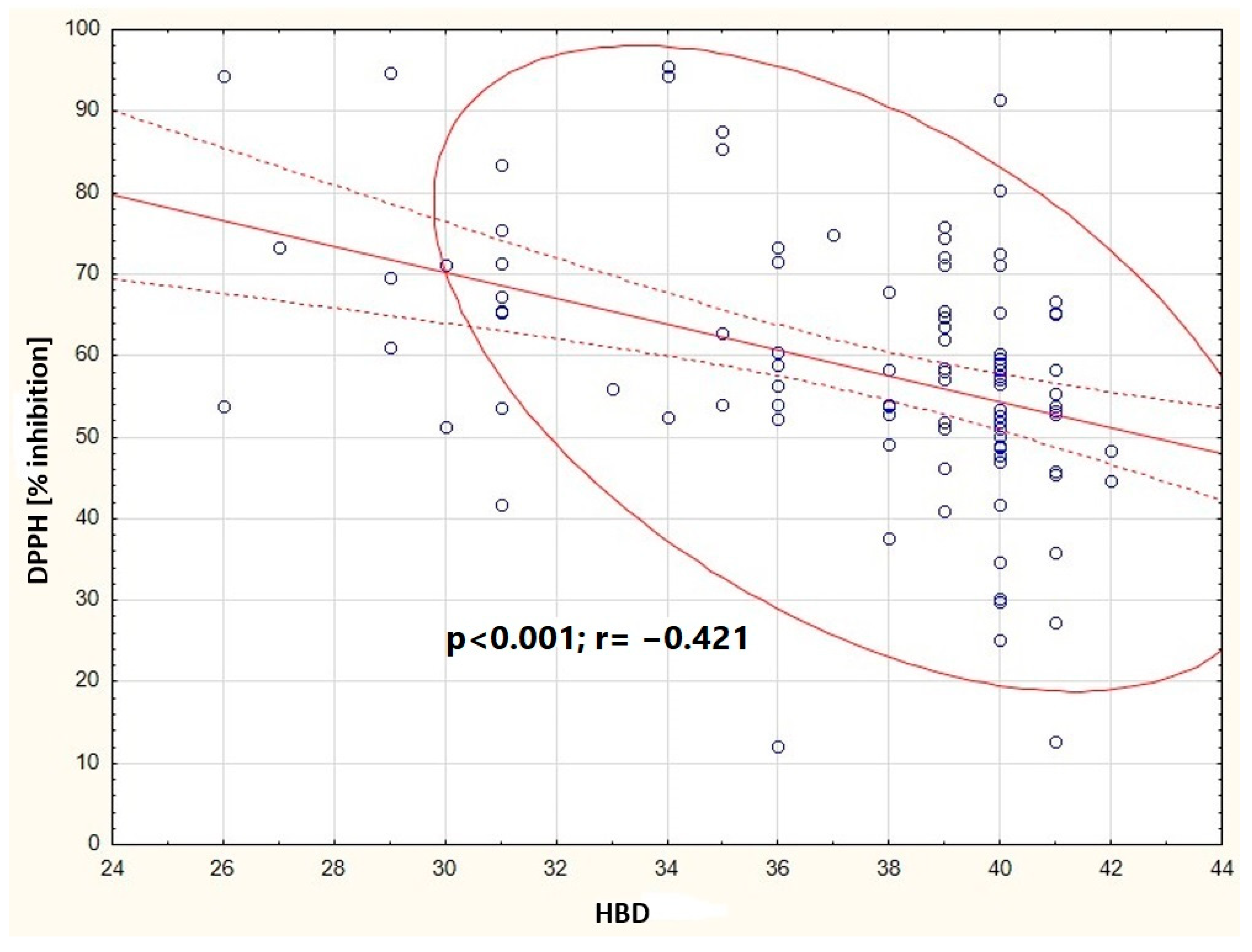
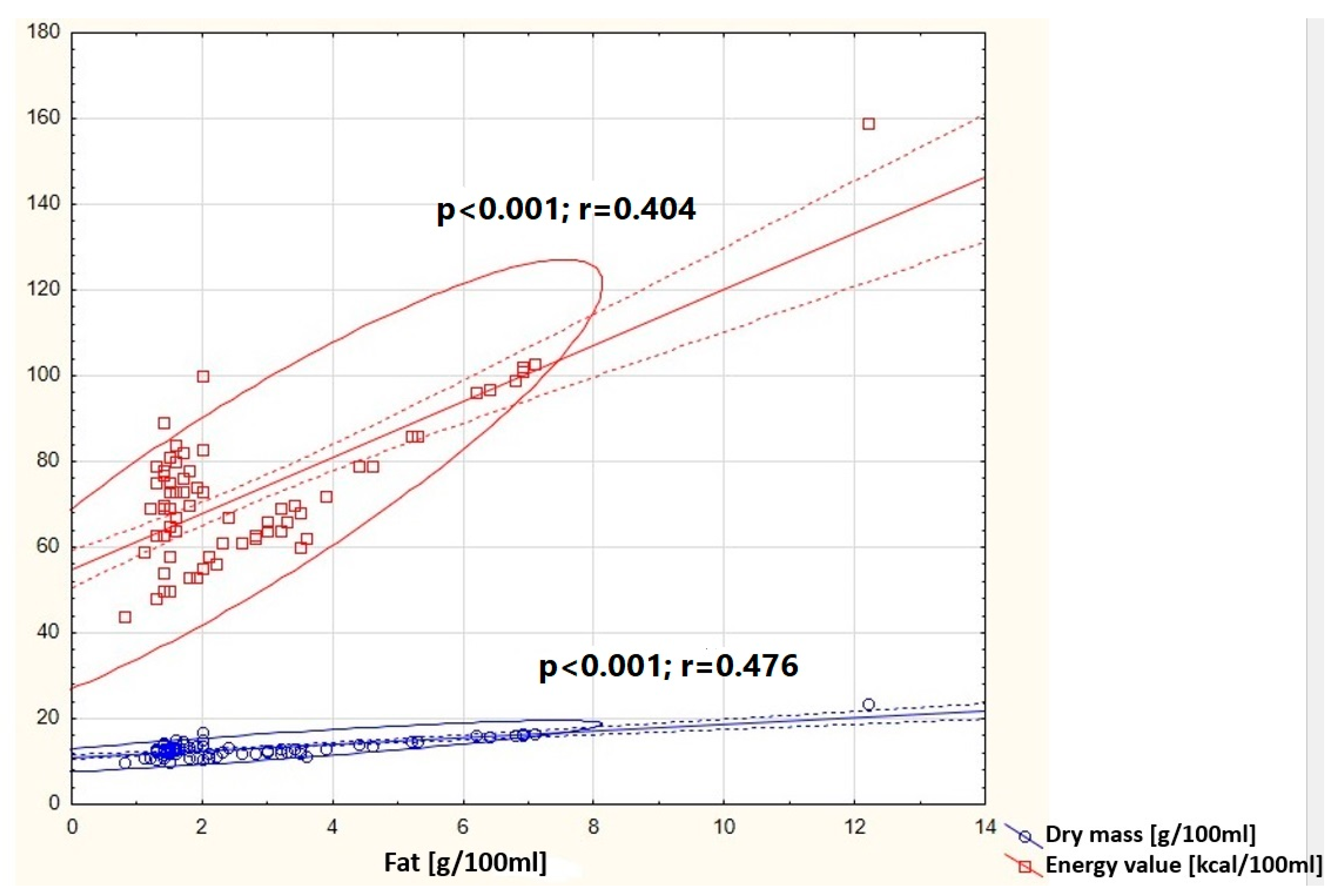
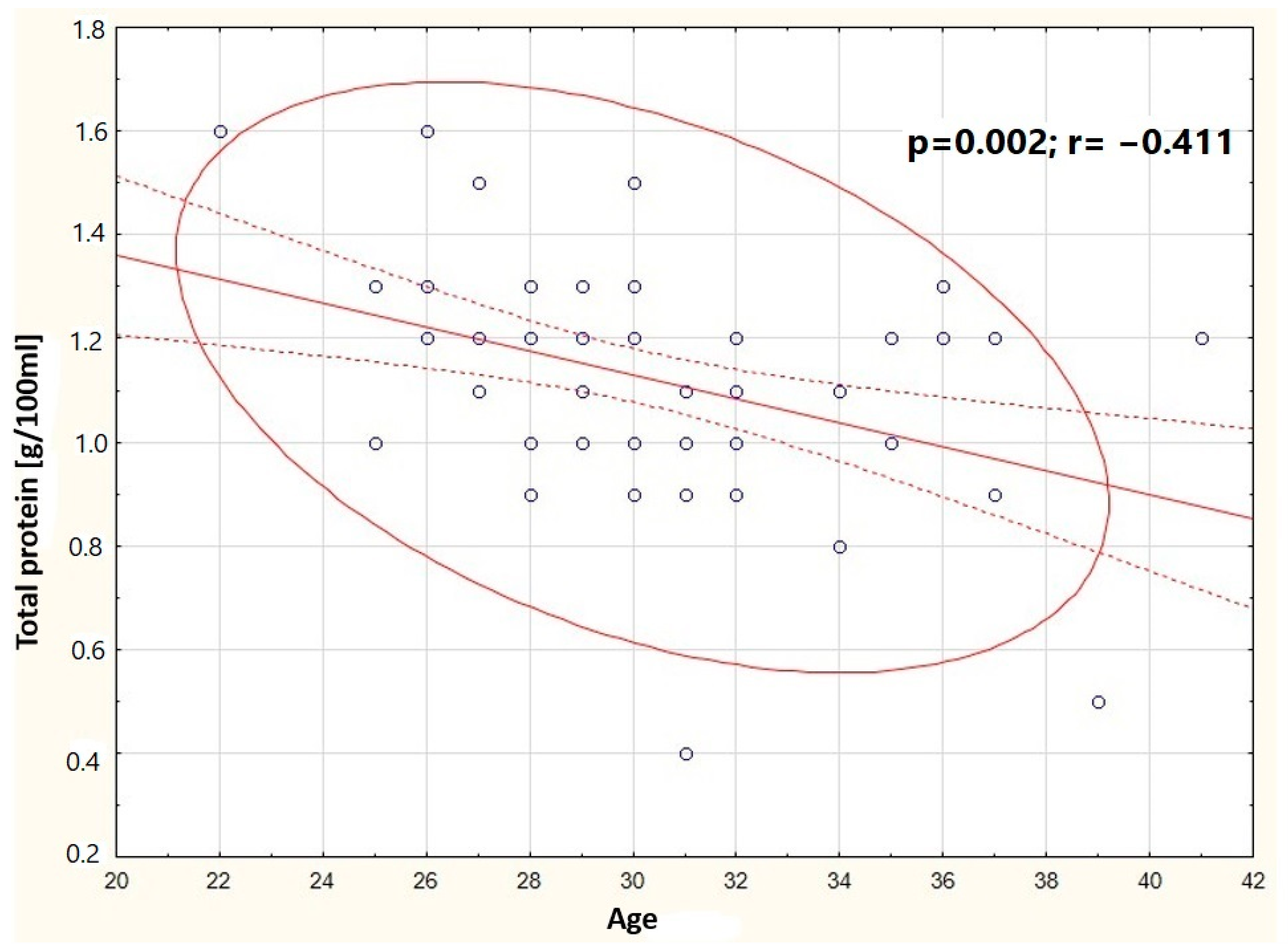
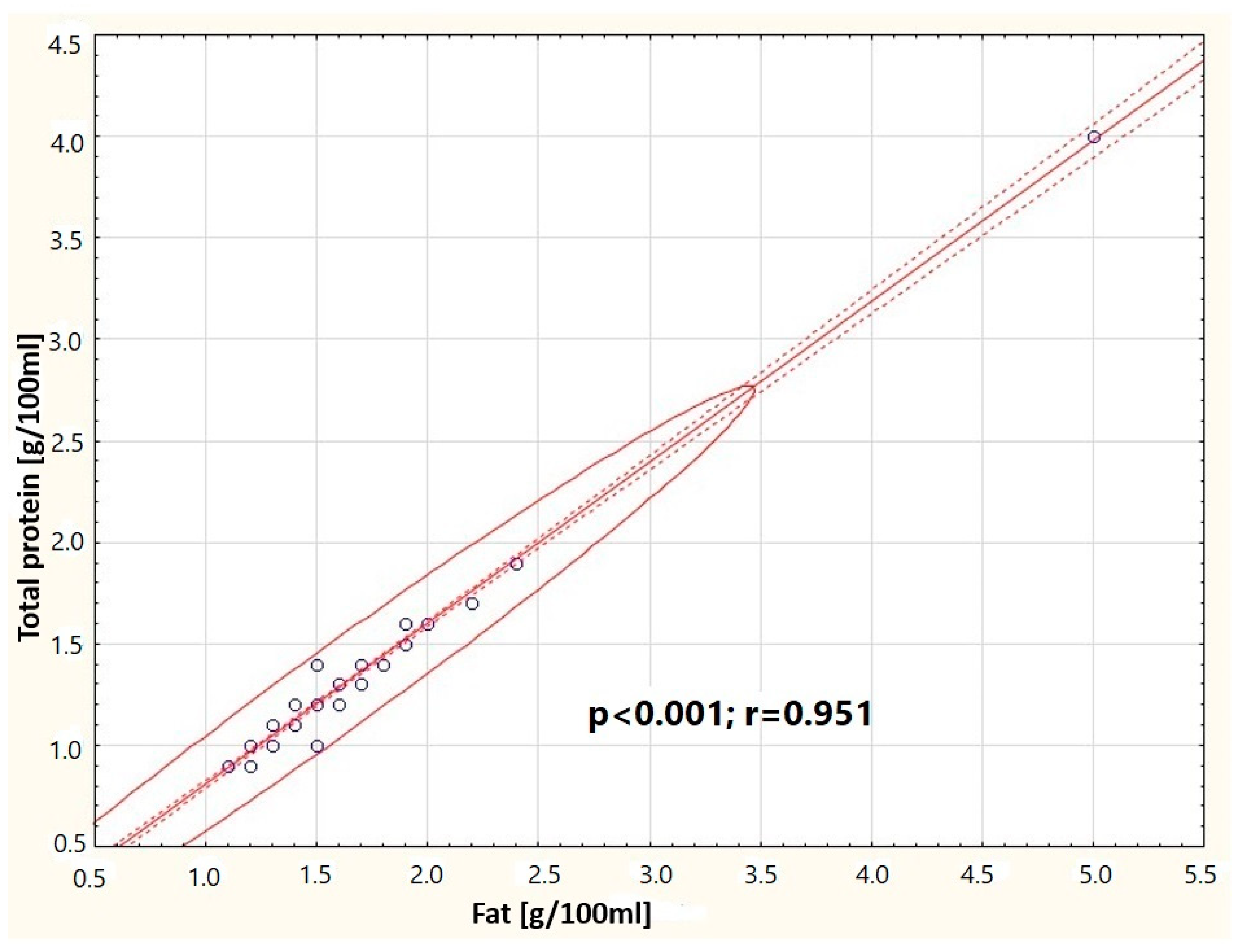
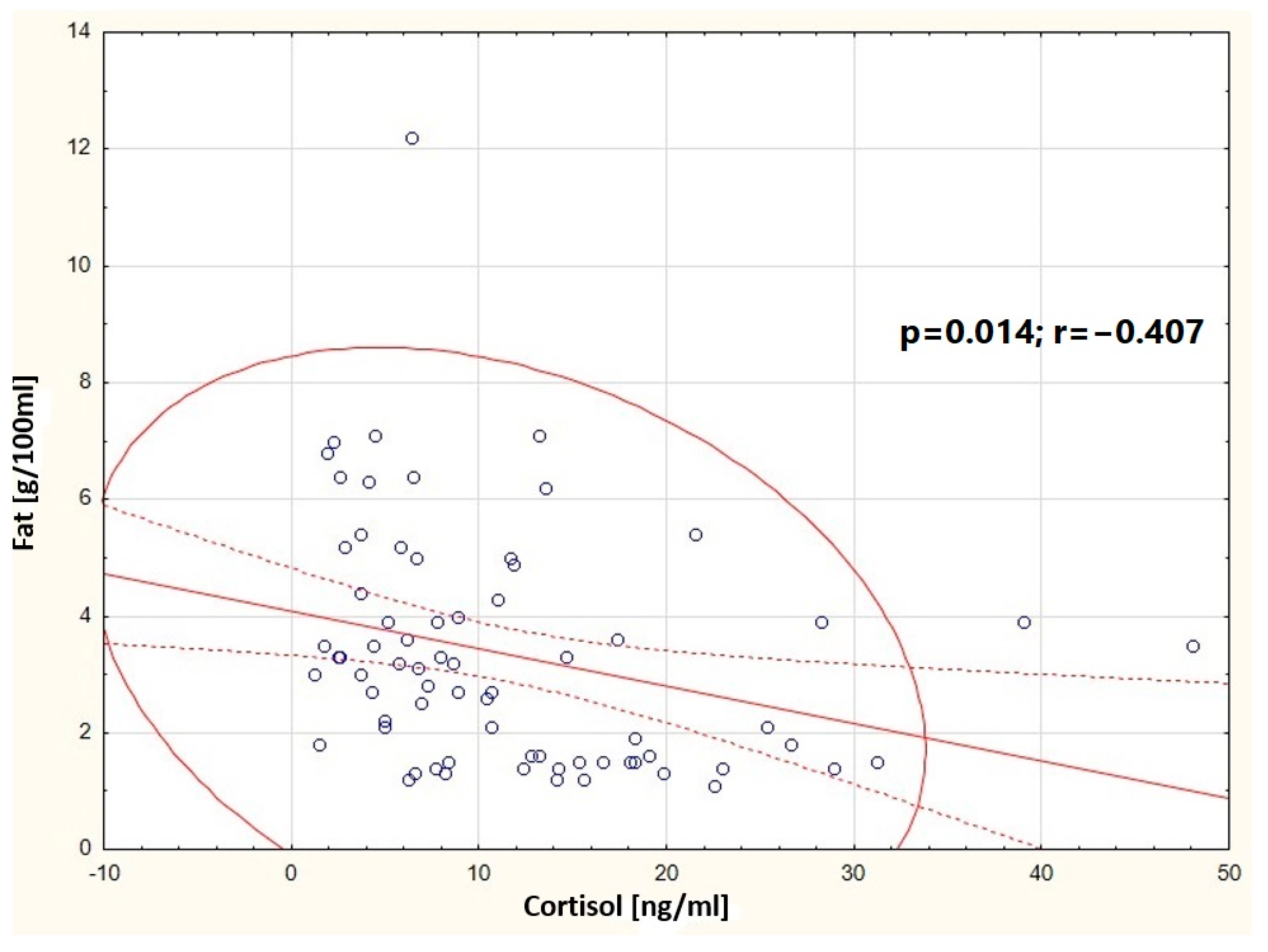
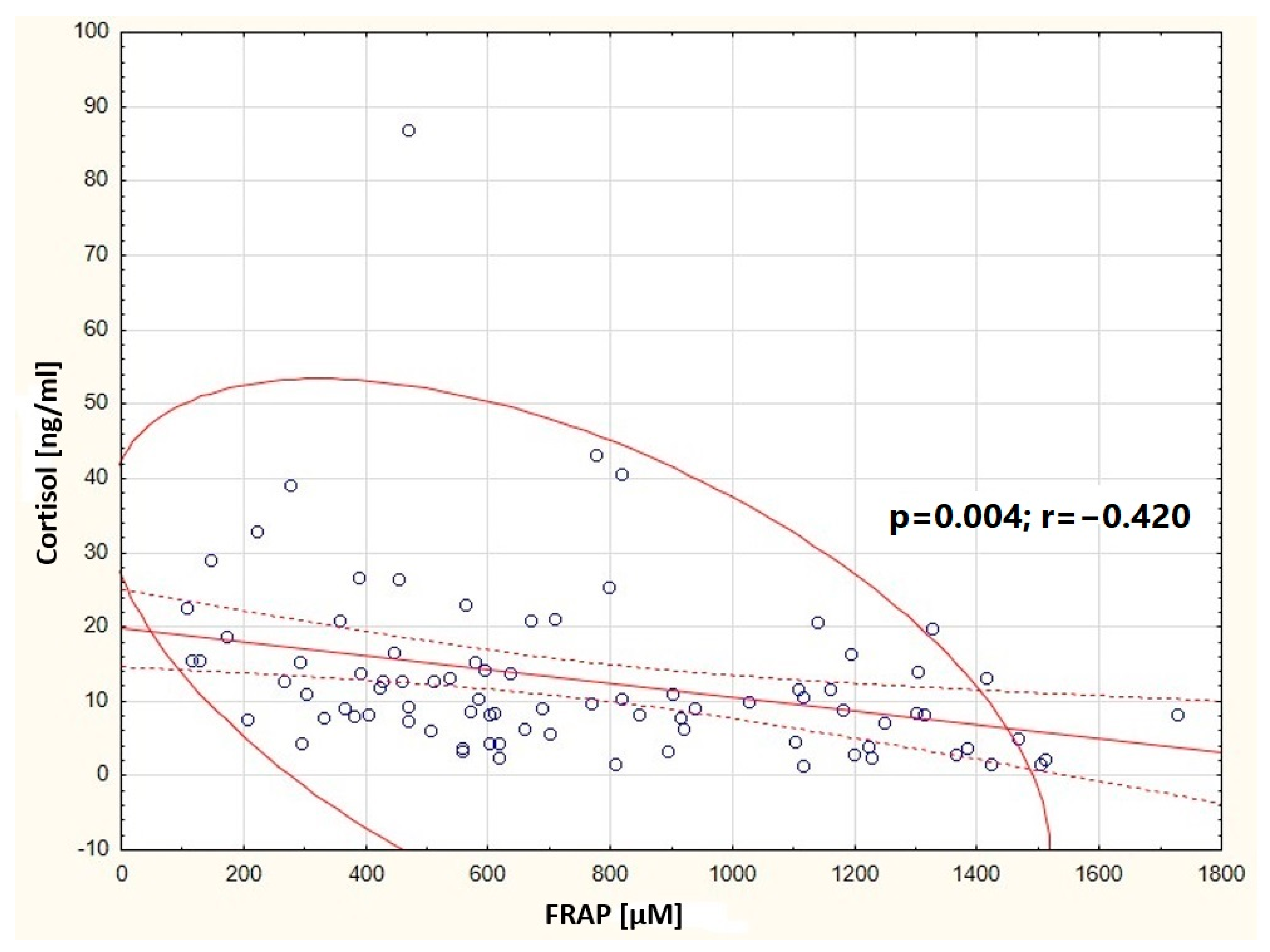
3.3. Correlations
4. Discussion
4.1. Changes in the Basic Composition of Human Milk in the Context of Many Factors
Antioxidant Status of Human Milk in the Context of the Analyzed Factors
4.2. Cortisol Concentration in Human Milk in the Context of the Analyzed Factors
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO/UNICEF. Global Nutrition Targets 2025: Breastfeeding Policy Brief (WHO/NMH/NHD/14.7); World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Kleinman, R.E.; Greer, F.R. (Eds.) Pediatric Nutrition, 8th ed.; American Academy of Pediatrics: Itasca, IL, USA, 2019. [Google Scholar]
- Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Mis, N.F.; Hojsak, I.; Hulst, J.M.; Indrio, F.; Lapillonne, A.; et al. Complementary Feeding: A Position Paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Rozensztrauch, A.; Klaniewska, M.; Berghausen-Mazur, M. Factors affecting the mother’s choice of infant feeding method in Poland: A cross-sectional preliminary study in Poland. Ir. J. Med. Sci. 2022, 191, 1735–1743. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ballard, O.; Morrow, A.L. Human milk composition: Nutrients and bioactive factors. Pediatr. Clin. N. Am. 2013, 60, 49–74. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, K.; Jiang, J.; Xiao, H.; Wu, K.; Qi, C.; Sun, J.; Li, D. Changes in the metabolite profile of breast milk over lactation stages and their relationship with dietary intake in Chinese women: HPLC-QTOFMS based metabolomic analysis. Food Funct. 2018, 9, 5189–5197. [Google Scholar] [CrossRef] [PubMed]
- Munblit, D.; Treneva, M.; Peroni, D.G.; Colicino, S.; Chow, L.Y.; Dissanayeke, S.; Pampura, A.; Boner, A.L.; Geddes, D.T.; Boyle, R.J.; et al. Immune Components in Human Milk Are Associated with Early Infant Immunological Health Outcomes: A Prospective Three-Country Analysis. Nutrients 2017, 9, 532. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kunz, C.; Niesen, M.; von Lilienfeld-Toal, H.; Burmeister, W. Vitamin D, 25-hydroxy-vitamin D and 1,25-dihydroxy-vitamin D in cow’s milk, infant formulas and breast milk during different stages of lactation. Int. J. Vitam. Nutr. Res. 1984, 54, 141–148. [Google Scholar] [PubMed]
- Katzer, D.; Pauli, L.; Mueller, A.; Reutter, H.; Reinsberg, J.; Fimmers, R.; Bartmann, P.; Bagci, S. Melatonin Concentrations and Antioxidative Capacity of Human Breast Milk According to Gestational Age and the Time of Day. J. Hum. Lact. 2016, 32, NP105–NP110. [Google Scholar] [CrossRef] [PubMed]
- Tie, W.J.; Gardner, H.; Lai, C.T.; Hepworth, A.R.; Al-Tamimi, Y.; Paech, M.J.; Hartmann, P.E.; Geddes, D.T. Changes in milk composition associated with pethidine-PCEA usage after Caesarean section. Matern. Child Nutr. 2017, 13, 12275. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fidler, N.; Sauerwald, T.; Pohl, A.; Demmelmair, H.; Koletzko, B. Docosahexaenoic acid transfer into human milk after dietary supplementation: A randomized clinical trial. J. Lipid Res. 2000, 41, 1376–1383. [Google Scholar] [CrossRef] [PubMed]
- Nommsen, L.A.; Lovelady, C.A.; Heinig, M.J.; Lönnerdal, B.; Dewey, K.G. Determinants of energy, protein, lipid, and lactose concentrations in human milk during the first 12 mo of lactation: The DARLING Study. Am. J. Clin. Nutr. 1991, 53, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Zielinska, M.A.; Hamulka, J.; Wesolowska, A. Carotenoid Content in Breastmilk in the 3rd and 6th Month of Lactation and Its Associations with Maternal Dietary Intake and Anthropometric Characteristics. Nutrients 2019, 11, 193. [Google Scholar] [CrossRef] [PubMed]
- Atanassova, M.; Georgieva, S.; Ivancheva, K. Total phenolic and total flavonoid contents, antioxidant capacity and biological contaminants in medicinal herbs. J. Univ. Chem. Technol. Metall. 2011, 46, 81–88. [Google Scholar]
- Benzie, F.F.; Strain, J.J. Ferric reducing/antioxidant power assay: Direct measure of total antioxidant activity of biological fluids and modified version for simultaneous measurement of total antioxidant power and ascorbic acid concentration. Methods Enzymol. 1999, 299, 15–23. [Google Scholar] [PubMed]
- Ongprasert, K.; Ruangsuriya, J.; Malasao, R.; Sapbamrer, R.; Suppansan, P.; Ayood, P.; Kittisakmontri, K.; Siviroj, P. Macronutrient, immunoglobulin a and total antioxidant capacity profiles of human milk from 1 to 24 months: A cross-sectional study in Thailand. Int. Breastfeed. J. 2020, 15, 90. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Czosnykowska-Łukacka, M.; Lis-Kuberka, J.; Królak-Olejnik, B.; Orczyk-Pawiłowicz, M. Changes in Human Milk Immunoglobulin Profile During Prolonged Lactation. Front. Pediatr. 2020, 8, 428. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mandel, D.; Lubetzky, R.; Dollberg, S.; Barak, S.; Mimouni, F.B. Fat and energy contents of expressed human breast milk in prolonged lactation. Pediatrics 2005, 116, e432–e435. [Google Scholar] [CrossRef] [PubMed]
- Schmeits, B.L.; Cook, J.A.; Vander Jagt, D.J.; Magnussen, M.A.; Bhatt, S.K.; Bobik, E.G.; Huang, Y.S. Fatty acid composition of the milk lipids of women in Nepal. Nutr. Res. 1999, 19, 1339–1348. [Google Scholar] [CrossRef]
- Quinn, E.A.; Diki Bista, K.; Childs, G. Milk at altitude: Human milk macronutrient composition in a high-altitude adapted population of Tibetans. Am. J. Phys. Anthropol. 2016, 159, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Qian, J.; Chen, T.; Lu, W.; Wu, S.; Zhu, J. Breast milk macro- and micronutrient composition in lactating mothers from suburban and urban Shanghai. J. Paediatr. Child Health 2010, 46, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Soliman, M.; Osman, F.; Ashoub, A.; Hussein, L. Fatty acid patterns of breast milk of Egyptian mothers from the city and the village. Int. J. Vitam. Nutr. Res. 1983, 53, 438–443. [Google Scholar] [PubMed]
- Gao, C.; Liu, G.; Whitfield, K.C.; Kroeun, H.; Green, T.; Gibson, R.; Makrides, M.; Zhou, S.J. Comparison of Human Milk Fatty Acid Composition of Women from Cambodia and Australia. J. Hum. Lact. 2018, 34, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Smit, E.N.; Martini, I.A.; Mulder, H.; Boersma, E.R.; Muskiet, F.A. Estimated biological variation of the mature human milk fatty acid composition. Prostaglandins Leukot. Essent. Fat. Acids 2002, 66, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Auestad, N.; Halter, R.; Hall, R.T.; Blatter, M.; Bogle, M.L.; Burks, W.; Erickson, J.R.; Fitzgerald, K.M.; Dobson, V.; Innis, S.M.; et al. Growth and development in term infants fed long-chain polyunsaturated fatty acids: A double-masked, randomized, parallel, prospective, multivariate study. Pediatrics 2001, 108, 372–381. [Google Scholar] [CrossRef] [PubMed]
- Birch, E.E.; Hoffman, D.R.; Castañeda, Y.S.; Fawcett, S.L.; Birch, D.G.; Uauy, R.D. A randomized controlled trial of long-chain polyunsaturated fatty acid supplementation of formula in term infants after weaning at 6 wk of age. Am. J. Clin. Nutr. 2002, 75, 570–580. [Google Scholar] [CrossRef] [PubMed]
- Francois, C.A.; Connor, S.L.; Wander, R.C.; Connor, W.E. Acute effects of dietary fatty acids on the fatty acids of human milk. Am. J. Clin. Nutr. 1998, 67, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Stoney, R.M.; Woods, R.K.; Hosking, C.S.; Hill, D.J.; Abramson, M.J.; Thien, F.C. Maternal breast milk long-chain n-3 fatty acids are associated with increased risk of atopy in breastfed infants. Clin. Exp. Allergy 2004, 34, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Dodge, M.L.; Wander, R.C.; Xia, Y.; Butler, J.A.; Whanger, P.D. Glutathione peroxidase activity modulates fatty acid profiles of plasma and breast milk in Chinese women. J. Trace Elem. Med. Biol. 1999, 12, 221–320. [Google Scholar] [CrossRef]
- Marangoni, F.; Agostoni, C.; Lammardo, A.M.; Bonvissuto, M.; Giovannini, M.; Galli, C.; Riva, E. Polyunsaturated fatty acids in maternal plasma and in breast milk. Prostaglandins Leukot. Essent. Fat. Acids 2002, 66, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, R.Y.; Castro, G.S.; Jordão, A.A., Jr.; Sartorelli, D.S. Breast milk fatty acid composition of women living far from the coastal area in Brazil. J. Pediatr. 2013, 89, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Mosley, E.E.; Wright, A.L.; McGuire, M.K.; McGuire, M.A. Trans Fatty acids in milk produced by women in the United States. Am. J. Clin. Nutr. 2005, 82, 1292–1297. [Google Scholar] [CrossRef] [PubMed]
- Precht, D.; Molkentin, J. C18:1, C18:2 and C18:3 trans and cis fatty acid isomers including conjugated cis delta 9, trans delta 11 linoleic acid (CLA) as well as total fat composition of German human milk lipids. Food/Nahrung 1999, 43, 233–244. [Google Scholar] [CrossRef] [PubMed]
- Burianova, I.; Bronsky, J.; Pavlikova, M.; Janota, J.; Maly, J. Maternal body mass index, parity and smoking are associated with human milk macronutrient content after preterm delivery. Early Hum. Dev. 2019, 137, 104832. [Google Scholar] [CrossRef] [PubMed]
- Mangel, L.; Mimouni, F.B.; Feinstein-Goren, N.; Lubetzky, R.; Mandel, D.; Marom, R. The effect of maternal habitus on macronutrient content of human milk colostrum. J. Perinatol. 2017, 37, 818–821. [Google Scholar] [CrossRef] [PubMed]
- Boutsikou, T.; Malamitsi-Puchner, A. Caesarean section: Impact on mother and child. Acta Paediatr. 2011, 100, 1518–1522. [Google Scholar] [CrossRef] [PubMed]
- Signore, C.; Spong, C.Y. Vaginal birth after cesarean: New insights manuscripts from an NIH Consensus Development Conference, March 8-10, 2010. Semin. Perinatol. 2010, 34, 309–310. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Macias, C.; Schweigert, F.J. Changes in the concentration of carotenoids, vitamin A, alpha-tocopherol and total lipids in human milk throughout early lactation. Ann. Nutr. Metab. 2001, 45, 82–85. [Google Scholar] [CrossRef] [PubMed]
- Xavier, A.A.O.; Díaz-Salido, E.; Arenilla-Vélez, I.; Aguayo-Maldonado, J.; Garrido-Fernández, J.; Fontecha, J.; Sánchez-García, A.; Pérez-Gálvez, A. Carotenoid Content in Human Colostrum is Associated to Preterm/Full-Term Birth Condition. Nutrirnts 2018, 10, 1654. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zarban, A.; Taheri, F.; Chahkandi, T.; Sharifzadeh, G.; Khorashadizadeh, M. Antioxidant and radical scavenging activity of human colostrum, transitional and mature milk. J. Clin. Biochem. Nutr. 2009, 45, 150–154. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- van der Voorn, B.; de Waard, M.; van Goudoever, J.B.; Rotteveel, J.; Heijboer, A.C.; Finken, M.J. Breast-Milk Cortisol and Cortisone Concentrations Follow the Diurnal Rhythm of Maternal Hypothalamus-Pituitary-Adrenal Axis Activity. J. Nutr. 2016, 146, 2174–2179. [Google Scholar] [CrossRef] [PubMed]
- Hinde, K.; Skibiel, A.L.; Foster, A.B.; Del Rosso, L.; Mendoza, S.P.; Capitanio, J.P. Cortisol in mother’s milk across lactation reflects maternal life history and predicts infant temperament. Behav. Ecol. 2015, 26, 269–281. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Grey, K.R.; Davis, E.P.; Sandman, C.A.; Glynn, L.M. Human milk cortisol is associated with infant temperament. Psychoneuroendocrinology 2013, 38, 1178–1185. [Google Scholar] [CrossRef]
- Hart, S.; Boylan, L.M.; Border, B.; Carroll, S.R.; Mcgunegle, D.; Lampe, R.M. Breast milk levels of cortisol and secretory Immunoglobulin A (SIgA) differ with maternal mood and infant neuro-behavioral functioning. Infant Behav. Dev. 2004, 27, 101–106. [Google Scholar] [CrossRef]
- Kulski, J.K.; Hartmann, P.E. Changes in the concentration of cortisol in milk during different stages of human lactation. Aust. J. Exp. Biol. Med. Sci. 1981, 59, 769–778. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, M.; Nolvi, S.; Härkönen, J.; Aatsinki, A.K.; Karlsson, L.; Karlsson, H.; Uusitupa, H.M. Associations between maternal socioeconomic, psychosocial and seasonal factors, infant characteristics and human milk cortisol concentrations. Am. J. Hum. Biol. 2021, 33, e23561. [Google Scholar] [CrossRef] [PubMed]
- Linderborg, K.M.; Kortesniemi, M.; Aatsinki, A.K.; Karlsson, L.; Karlsson, H.; Yang, B.; Uusitupa, H.M. Interactions between cortisol and lipids in human milk. Int. Breastfeed. J. 2020, 15, 66. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yang, T.; Zhang, Y.; Ning, Y.; You, L.; Ma, D.; Zheng, Y.; Yang, X.; Li, W.; Wang, J.; Wang, P. Breast milk macronutrient composition and the associated factors in urban Chinese mothers. Chin. Med. J. 2014, 127, 1721–1725. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Median (Q1–Q3) |
|---|---|
| Age (years) | 30 (28–33) |
| HBD (week) | 39 (36–40) |
| BMI (kg/m2) | 23.14 (20.98–26.13) |
| Fat in milk (g/dL) | 2.2 (1.5–4.0) |
| Total protein in milk (g/dL) | 1.2 (1.1–1.3) |
| Carbohydrates in milk (g/dL) | 7.9 (7.6–8.2) |
| Dry Matter (g/dL) | 13.1 (12.2–14.2) |
| Calorie content (kcal/dL) | 72 (63–80) |
| Cortisol (ng/mL) | 9.2 (6.03–14.61) |
| Delivery type | n (%) |
| Vaginal delivery | 109 (59%) |
| Cesarean section | 74 (41%) |
| Place of residence | n (%) |
| City center | 108 (60%) |
| The outskirts of the city | 75 (40%) |
| Maternal parity | n (%) |
| Primiparous | 84 (46%) |
| Multiparous | 99 (54%) |
| Stimulants | n (%) |
| Yes | 36 (20%) |
| No | 147 (80%) |
| Supplementation | n (%) |
| Yes | 144 (79%) |
| No | 39 (21%) |
| Diseases during pregnancy and breastfeeding | n (%) |
| Yes | n = 98 (54%) |
| No | n = 85 (46%) |
| Labor force participation | n (%) |
| Yes | n = 109 (60%) |
| No | n = 74 (40%) |
| Miscarriage | n (%) |
| Yes | 33 (18%) including: 1 miscarriage 23 (70%) 2–3 miscarriages 10 (30%) |
| No | 150 (82%) |
| (a) | ||||||||||
| Group I | Group II | Group III | ||||||||
| Multiparous | Primiparous | p | Women Living on the Outskirts of the City | Women Living in the City Center | p | Women Giving Birth Naturally | Women Giving Birth by Cesarean Section | p | ||
| n = 99 | n = 84 | n = 75 | n = 108 | n = 109 | n = 74 | |||||
| Age (years) | 32 29–34 | 29 27–32 | <0.001 | 30 28–32 | 31 28–34 | 0.101 | 30 28–33 | 30.5 29–34 | 0.489 | |
| BMI (kg/m2) (Me; Q25–Q75) | 23.6 21.25–26.34 | 22.55 20.84–25.43 | 0.150 | 23.52 20.94–26.13 | 23.04 20.99–26.13 | 0.647 | 22.8 21.2–25.7 | 23.61 20.96–26.77 | 0.443 | |
| HBD (tyg.) (Me; Q25–Q75) | 39 36–40 | 39 36–40 | 0.664 | 39 36–40 | 39 36–40 | 0.136 | 39 38–40 | 38 32–40 | 0.004 | |
| (b) | ||||||||||
| Group IV | Group V | Group VI | ||||||||
| Professionally Active Women | Professionally Inactive Women | p | Women who Fell Ill During Pregnancy and Breastfeeding | Healthy Women | p | Breast-feeding from 3 to 5 Weeks | Breast-feeding from 5 Weeks up to 12 Months of Lactation | Breast-feeding from 12 to 24 Months | pa/b pa/c pb/c | |
| n = 111 | n = 72 | n = 98 | n = 85 | n = 76 | n = 59 | n = 48 | ||||
| Age (years) | 31 29–33 | 29.5 27–32 | 0.066 | 30 26–34 | 30 26–32 | 0.474 | 31 28–34 | 30 28–32 | 31 29–33 | 0.612 > 0.999 0.212 |
| BMI (kg/m2) (Me; Q25–Q75) | 23.53 20.91–26.34 | 23.04 21.24–25.00 | 0.634 | 22.86 20.94–25.82 | 23.24 21.45–26.35 | 0.823 | 24.35 22.18–27.49 | 22.57 20.89–24.80 | 21.6 19.61–24.50 | 0.009 < 0.001 0.853 |
| HBD (tyg.) (Me; Q25–Q75) | 39 35–40 | 39 36–40 | 0.689 | 39 36–40 | 39 35–40 | 0.863 | 35 31–39 | 40 39–41 | 40 39–40 | <0.001 < 0.001 > 0.999 |
| (a) | ||||||||||
| Group I | Group II | |||||||||
| Multiparous | Primiparous | p | Women Living on the Outskirts of the City | Women Living in the City Center | p | |||||
| n = 99 | n = 84 | n = 75 | n = 108 | |||||||
| Fats (Me; Q25–Q75) | 1.9 1.5–3.9 | 2.65 1.6–4.55 | 0.040 | 3.2 1.6–4.2 | 1.9 1.5–3.95 | 0.031 | ||||
| Total protein (Me; Q25–Q75) | 1.2 1.1–1.3 | 1.2 1.1–1.4 | 0.262 | 1.2 1–1.3 | 1.2 1.1–1.3 | 0.450 | ||||
| Carbohydrates (Me; Q25–Q75) | 8 7.7–8.2 | 7.8 7.5–8.1 | 0.179 | 7.9 7.5–8.2 | 7.9 7.6–8.1 | 0.851 | ||||
| Dry matter (Me; Q25–Q75) | 13.2 12.2–14.1 | 13 12.25–14.3 | 0.958 | 13.1 12.4–14.1 | 13 12.05–14.25 | 0.688 | ||||
| Caloric value (Me; Q25–Q75) | 72 64–80 | 71.5 63–80.5 | 0.998 | 72 65–82 | 73 62.5–80 | 0.585 | ||||
| Cortisol [ng/mL] (Me; Q25–Q75) | 8.57 5.7–14.35 | 10.24 6.22–15.41 | 0.641 | 8.13 6.84–12.74 | 10.67 6.87–16.27 | 0.007 | ||||
| FRAP (Me; Q25–Q75) | 758.52 454.2–1108 | 764.75 461–978.54 | 0.779 | 729.75 449.65–1053.75 | 776.68 461.76–1026.5 | 0.570 | ||||
| DPPH (Me; Q25–Q75) | 57.64 50.99–67.23 | 56.5 47.26–72.17 | 0.731 | 56.53 50.54–68.5 | 57.37 48.38–71.53 | 0.910 | ||||
| Group III | Group IV | |||||||||
| Women Giving Birth Naturally | Women Giving Birth by Cesarean Section | p | Professionally Active Women | Professionally Inactive Women | p | |||||
| n = 109 | n = 74 | n = 111 | n = 72 | |||||||
| Fats (Me; Q25–Q75) | 3.2 1.6–4.4 | 1.85 1.5–3.2 | 0.009 | 2 1.5–3.9 | 3.05 1.55–4.15 | 0.176 | ||||
| Total protein (Me; Q25–Q75) | 1.2 1.1–1.3 | 1.2 1.1–1.4 | 0.491 | 1.2 1.1–1.4 | 1.1 1–1.3 | 0.002 | ||||
| Carbohydrates (Me; Q25–Q75) | 8 7.6–8.2 | 7.9 7.5–8.1 | 0.366 | 7.9 7.6–8.2 | 7.9 7.5–8.1 | 0.196 | ||||
| Dry matter (Me; Q25–Q75) | 13.4 12.4–14.3 | 12.8 12–13.4 | 0.041 | 13.5 12.4–14.5 | 12.8 11.95–13.95 | 0.046 | ||||
| Caloric value (Me; Q25–Q75) | 73 62–79 | 69.5 62–79 | 0.127 | 74 65–82 | 69 61–78 | 0.087 | ||||
| Cortisol [ng/mL] (Me; Q25–Q75) | 8.83 6.02–18.29 | 11 6.25–18.29 | 0.177 | 9.55 6.25–13.79 | 8.7 5.06–15.45 | 0.586 | ||||
| FRAP (Me; Q25–Q75) | 758.52 461.77–1058.09 | 767.65 454.2–984.8 | 0.944 | 708.55 445.12–908.40 | 806.21 522.18–1120.36 | 0.146 | ||||
| DPPH (Me; Q25–Q75) | 56.4 47.83–67.87 | 58.46 52.26–69.55 | 0.259 | 53.01 42.61–66.10 | 58.42 53.27–71.32 | 0.002 | ||||
| (b) | ||||||||||
| Group V | Group VI | Group VII | ||||||||
| Women Who Fell Ill During Pregnancy and Breastfeeding | Healthy Women | p | Breastfeeding from 3 to 5 Weeks | Breastfeeding from 5 Weeks up to 12 Months of Lactation | Breastfeeding from 12 to 24 Months | pa/b pa/c pb/c | Women with a BMI of 18–25 kg/m2 | Women with a BMI of 25–35 kg/m2 | p | |
| n = 98 | n = 85 | n = 76 | n = 59 | n = 48 | n = 110 | n = 73 | ||||
| Fats (Me; Q25–Q75) | 3.05 1.6–4.4 | 1.8 1.5–3.4 | 0.005 | 1.5 1.4–1.7 | 3.4 2.6–4.4 | 4.4 3.2–6.1 | <0.001 < 0.001 0.103 | 2.8 1.6–4.3 | 1.85 1.5–3.3 | 0.034 |
| Total protein (Me; Q25–Q75) | 1.2 1.1–1.3 | 1.2 1.1–1.3 | 0.395 | 1.2 1.1–1.4 | 1.1 1.0–1.2 | 1.2 1.1–1.5 | 0.003 > 0.999 0.087 | 1.2 1.1–1.3 | 1.2 1.1–1.3 | 0.465 |
| Carbohydrates (Me; Q25–Q75) | 7.9 7.6–8.1 | 7.9 7.6–8.2 | 0.964 | 7.9 7.5–8.3 | 8 7.8–8.1 | 7.9 7.4–8.1 | >0.999 0.107 0.127 | 7.9 7.6–8.1 | 7.9 7.6–8.2 | 0.237 |
| Dry matter (Me; Q25–Q75) | 13.05 12.2–14.5 | 13.1 12.2–14.1 | 0.461 | 13.1 12.5–14 | 12.5 11.7–13.9 | 13.45 12.1–15.2 | 0.158 > 0.999 0.042 | 13 12.1–13.9 | 13.3 12.4–14.8 | 0.245 |
| Caloric value (Me; Q25–Q75) | 71 63–86 | 73 64–80 | 0.564 | 74 98–79.5 | 67 60–77 | 77 64–90 | 0.016 > 0.999 0.004 | 72 63–78 | 73.5 64–86 | 0.223 |
| Cortisol [ng/mL] (Me; Q25–Q75) | 8.86 5.81–13.58 | 9.65 6.26–15.31 | 0.434 | 13.21 9.18–19.47 | 6.1 3.9–10.9 | 8.48 4.9–11 | <0.001 < 0.001 0.956 | 9.08 5.69–14.61 | 9.43 6.36–13.32 | 0.671 |
| FRAP (Me; Q25–Q75) | 702.74 472.36–984.10 | 635.88 445.11–1114.39 | 0.433 | 887.7 608.6–115.82 | 582.37 374.5–935.4 | 775.25 461.97–947.67 | 0.001 0.489 0.267 | 699.47 454.2–984.1 | 778.95 461.17–1058 | 0.535 |
| DPPH (Me; Q25–Q75) | 58.09 48.99–72.05 | 56.47 49.11–67.32 | 0.404 | 62.67 55.21–74.01 | 50.25 43.20–60.00 | 54.40 47.32–66.00 | <0.001 0.002 0.877 | 58.42 53.27–71.32 | 55.99 47.23–68.05 | 0.041 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dombrowska-Pali, A.; Chrustek, A.; Olszewska-Słonina, D.; Socha, M.W. Composition and Antioxidant Status of Human Milk of Women Living in Bydgoszcz (Poland). Nutrients 2024, 16, 3396. https://doi.org/10.3390/nu16193396
Dombrowska-Pali A, Chrustek A, Olszewska-Słonina D, Socha MW. Composition and Antioxidant Status of Human Milk of Women Living in Bydgoszcz (Poland). Nutrients. 2024; 16(19):3396. https://doi.org/10.3390/nu16193396
Chicago/Turabian StyleDombrowska-Pali, Agnieszka, Agnieszka Chrustek, Dorota Olszewska-Słonina, and Maciej W. Socha. 2024. "Composition and Antioxidant Status of Human Milk of Women Living in Bydgoszcz (Poland)" Nutrients 16, no. 19: 3396. https://doi.org/10.3390/nu16193396