Efficacy of Food Industry By-Product β-Glucan/Chitin–Chitosan on Lipid Profile of Overweight and Obese Individuals: Sustainability and Nutraceuticals

 , ,
, ,  and
and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Subjects
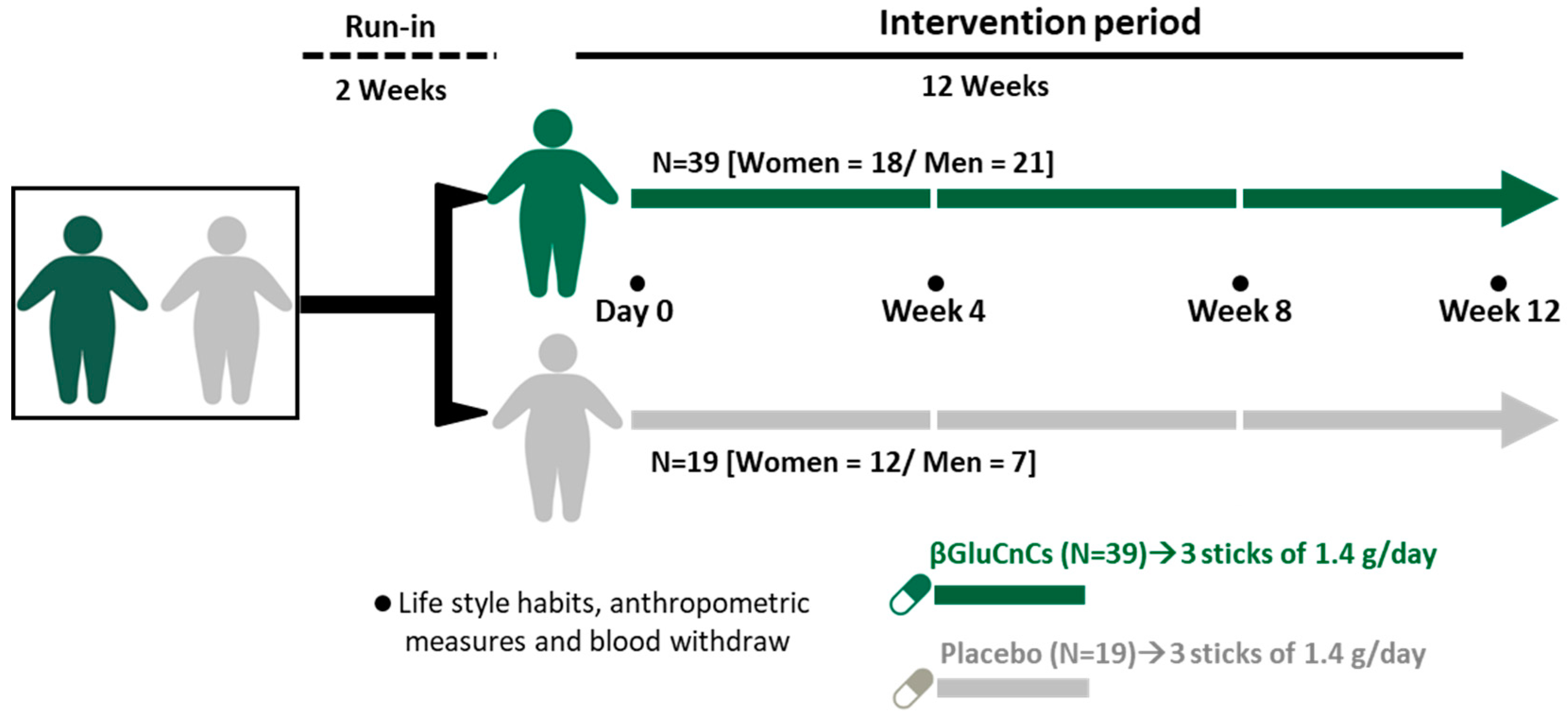
2.2. Study Design and Dietary Monitoring
2.3. Biological Samples
2.4. Anthropometric Data, Blood Pressure, Biochemical Measurements and Serum Lipid Profile
2.5. HDL Particles (Number and Size) Analysis by 1H-NMR
2.6. Apolipoprotein (Apo) A1 and Apolipoprotein B Levels
2.7. In Vitro Assessment of LDL Susceptibility to Oxidation and HDL-Antioxidant Capacity
2.7.1. Lipoprotein Preparation
2.7.2. Conjugated Dienes
2.7.3. Antioxidant Capacity of HDL
2.8. Insulin and Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) Index
2.9. Statistical Analysis
3. Results
3.1. Clinical and Biochemical Characteristics at Baseline
3.2. Effect of Nutraceutical Intervention on on Anthropometric, Hemodynamic and Biochemical Characteristics
3.3. Effects of the 12-Week Intervention on Serum Lipid Profile
3.4. Changes in Concentration and Diameter of Circulating HDL Particles in the βGluCnCs and Placebo Groups at Baseline and during the Intervention Period
3.5. Effect of the 12-Week Intervention on ApoA1 and ApoB Levels
3.6. Effect of the 12-Week Intervention on Lipoprotein Functionality
3.6.1. LDL Susceptibility to Oxidation
3.6.2. HDL Antioxidant Capacity
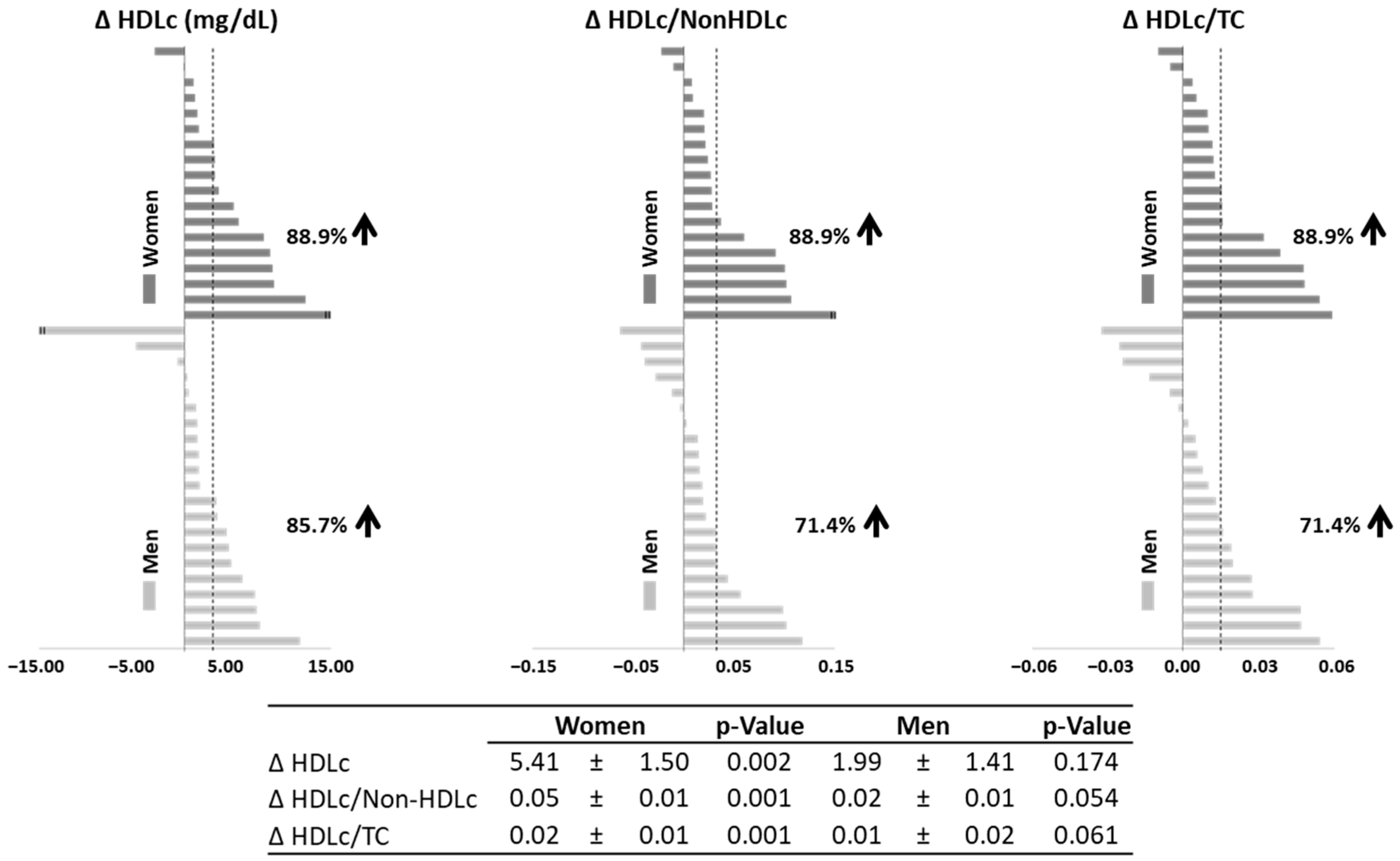
3.7. Response of Lipid Profile by Sex to 12-Week Intervention with βGluCnCs
3.8. Response to the 12-Week βGluCnCs Intervention in Relation to the BMI and LDLc Levels at Baseline
3.9. Effects of the 12-Week Intervention in Insulin Levels and HOMA-IR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 20 August 2024).
- Shabana; Shahid, S.U.; Sarwar, S. The Abnormal Lipid Profile in Obesity and Coronary Heart Disease (CHD) in Pakistani Subjects. Lipids Health Dis. 2020, 19, 73. [Google Scholar] [CrossRef]
- Stadler, J.T.; Lackner, S.; Mörkl, S.; Trakaki, A.; Scharnagl, H.; Borenich, A.; Wonisch, W.; Mangge, H.; Zelzer, S.; Meier-Allard, N.; et al. Obesity Affects HDL Metabolism, Composition and Subclass Distribution. Biomedicines 2021, 9, 242. [Google Scholar] [CrossRef]
- Bora, K.; Pathak, M.S.; Borah, P.; Das, D. Association of Decreased High-Density Lipoprotein Cholesterol (HDL-C) with Obesity and Risk Estimates for Decreased HDL-C Attributable to Obesity: Preliminary Findings from a Hospital-Based Study in a City from Northeast India. J. Prim. Care Community Health 2017, 8, 26. [Google Scholar] [CrossRef] [PubMed]
- Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Final Report. Circulation 2002, 106, 3143–3421. [CrossRef]
- Khera, A.V.; Plutzky, J. Management of Low Levels of High-Density Lipoprotein-Cholesterol. Circulation 2013, 128, 72–78. [Google Scholar] [CrossRef]
- Stadler, J.T.; Marsche, G. Obesity-Related Changes in High-Density Lipoprotein Metabolism and Function. Int. J. Mol. Sci. 2020, 21, 8985. [Google Scholar] [CrossRef]
- Park, K.H.; Yadav, D.; Kim, S.J.; Kim, J.R.; Cho, K.H. Slim Body Weight Is Highly Associated with Enhanced Lipoprotein Functionality, Higher HDL-C, and Large HDL Particle Size in Young Women. Front. Endocrinol. 2018, 9, 406. [Google Scholar] [CrossRef]
- Genua, I.; Puig, N.; Miñambres, I.; Benítez, S.; Gil, P.; Grau-Agramunt, M.; Rivas-Urbina, A.; Balagué, C.; Fernández-Alanin, S.; García-Osuna, Á.; et al. Clinical Medicine Changes in the Composition and Function of Lipoproteins after Bariatric Surgery in Patients with Severe Obesity. J. Clin. Med. 2021, 10, 1716. [Google Scholar] [CrossRef]
- Benito-Vicente, A.; Uribe, K.B.; Jebari, S.; Galicia-Garcia, U.; Ostolaza, H.; Martin, C. Familial Hypercholesterolemia: The Most Frequent Cholesterol Metabolism Disorder Caused Disease. Int. J. Mol. Sci. 2018, 19, 3426. [Google Scholar] [CrossRef]
- Wang, H.H.; Garruti, G.; Liu, M.; Portincasa, P.; Wang, D.Q.H. Cholesterol and Lipoprotein Metabolism and Atherosclerosis: Recent Advances in Reverse Cholesterol Transport. Ann. Hepatol. 2017, 16, s27–s42. [Google Scholar] [CrossRef]
- Thompson, S.V.; Hannon, B.A.; An, R.; Holscher, H.D. Effects of Isolated Soluble Fiber Supplementation on Body Weight, Glycemia, and Insulinemia in Adults with Overweight and Obesity: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Am. J. Clin. Nutr. 2017, 106, 1514–1528. [Google Scholar] [CrossRef] [PubMed]
- Iversen, K.N.; Carlsson, F.; Andersson, A.; Michaëlsson, K.; Langton, M.; Risérus, U.; Hellström, P.M.; Landberg, R. A Hypocaloric Diet Rich in High Fiber Rye Foods Causes Greater Reduction in Body Weight and Body Fat than a Diet Rich in Refined Wheat: A Parallel Randomized Controlled Trial in Adults with Overweight and Obesity (the RyeWeight Study). Clin. Nutr. ESPEN 2021, 45, 155–169. [Google Scholar] [CrossRef]
- Maki, K.C.; Beiseigel, J.M.; Jonnalagadda, S.S.; Gugger, C.K.; Reeves, M.S.; Farmer, M.V.; Kaden, V.N.; Rains, T.M. Whole-Grain Ready-to-Eat Oat Cereal, as Part of a Dietary Program for Weight Loss, Reduces Low-Density Lipoprotein Cholesterol in Adults with Overweight and Obesity More than a Dietary Program Including Low-Fiber Control Foods. J. Am. Diet. Assoc. 2010, 110, 205–214. [Google Scholar] [CrossRef]
- Bakr, A.F.; Farag, M.A. Soluble Dietary Fibers as Antihyperlipidemic Agents: A Comprehensive Review to Maximize Their Health Benefits. ACS Omega 2023, 8, 24680. [Google Scholar] [CrossRef]
- van Bennekum, A.M.; Nguyen, D.V.; Schulthess, G.; Hauser, H.; Phillips, M.C. Mechanisms of Cholesterol-Lowering Effects of Dietary Insoluble Fibres: Relationships with Intestinal and Hepatic Cholesterol Parameters. Br. J. Nutr. 2005, 94, 331–337. [Google Scholar] [CrossRef]
- Joyce, S.A.; Kamil, A.; Fleige, L.; Gahan, C.G.M. The Cholesterol-Lowering Effect of Oats and Oat Beta Glucan: Modes of Action and Potential Role of Bile Acids and the Microbiome. Front. Nutr. 2019, 6, 171. [Google Scholar] [CrossRef]
- Kaur, R.; Sharma, M.; Ji, D.; Xu, M.; Agyei, D. Structural Features, Modification, and Functionalities of Beta-Glucan. Fibers 2019, 8, 1. [Google Scholar] [CrossRef]
- Ylitalo, R.; Lehtinen, S.; Wuolijoki, E.; Ylitalo, P.; Lehtimäki, T. Cholesterol-Lowering Properties and Safety of Chitosan. Arzneimittelforschung 2002, 52, 1–7. [Google Scholar] [CrossRef]
- Tosh, S.M. Review of Human Studies Investigating the Post-Prandial Blood-Glucose Lowering Ability of Oat and Barley Food Products. Eur. J. Clin. Nutr. 2013, 67, 310–317. [Google Scholar] [CrossRef]
- Bashir, K.M.I.; Choi, J.S. Clinical and Physiological Perspectives of β-Glucans: The Past, Present, and Future. Int. J. Mol. Sci. 2017, 18, 1906. [Google Scholar] [CrossRef]
- Jenkins, D.J.A.; Kendall, C.W.C.; Vuksan, V.; Vidgen, E.; Parker, T.; Faulkner, D.; Mehling, C.C.; Garsetti, M.; Testolin, G.; Cunnane, S.C.; et al. Soluble Fiber Intake at a Dose Approved by the US Food and Drug Administration for a Claim of Health Benefits: Serum Lipid Risk Factors for Cardiovascular Disease Assessed in a Randomized Controlled Crossover Trial. Am. J. Clin. Nutr. 2002, 75, 834–839. [Google Scholar] [CrossRef] [PubMed]
- Behall, K.M.; Scholfield, D.J.; Hallfrisch, J. Lipids Significantly Reduced by Diets Containing Barley in Moderately Hypercholesterolemic Men. J. Am. Coll. Nutr. 2004, 23, 55–62. [Google Scholar] [CrossRef]
- Desai, N.; Rana, D.; Salave, S.; Gupta, R.; Patel, P.; Karunakaran, B.; Sharma, A.; Giri, J.; Benival, D.; Kommineni, N. Chitosan: A Potential Biopolymer in Drug Delivery and Biomedical Applications. Pharmaceutics 2023, 15, 1313. [Google Scholar] [CrossRef] [PubMed]
- Aranaz, I.; Alcántara, A.R.; Civera, M.C.; Arias, C.; Elorza, B.; Caballero, A.H.; Acosta, N. Chitosan: An Overview of Its Properties and Applications. Polymers 2021, 13, 3256. [Google Scholar] [CrossRef] [PubMed]
- Jin, Q.; Yu, H.; Wang, X.; Li, K.; Li, P. Effect of the Molecular Weight of Water-Soluble Chitosan on Its Fat-/Cholesterol-Binding Capacities and Inhibitory Activities to Pancreatic Lipase. PeerJ 2017, 5, e3279. [Google Scholar] [CrossRef]
- Bokura, H.; Kobayashi, S. Chitosan Decreases Total Cholesterol in Women: A Randomized, Double-Blind, Placebo-Controlled Trial. Eur. J. Clin. Nutr. 2003, 57, 721–725. [Google Scholar] [CrossRef]
- Fatahi, S.; Sayyari, A.A.; Salehi, M.; Safa, M.; Sohouli, M.; Shidfar, F.; Santos, H.O. The Effects of Chitosan Supplementation on Anthropometric Indicators of Obesity, Lipid and Glycemic Profiles, and Appetite-Regulated Hormones in Adolescents with Overweight or Obesity: A Randomized, Double-Blind Clinical Trial. BMC Pediatr. 2021, 22, 527. [Google Scholar] [CrossRef]
- Baker, W.L.; Tercius, A.; Anglade, M.; White, C.M.; Coleman, C.I. A Meta-Analysis Evaluating the Impact of Chitosan on Serum Lipids in Hypercholesterolemic Patients. Ann. Nutr. Metab. 2009, 55, 368–374. [Google Scholar] [CrossRef]
- Jung, E.Y.; Cho, M.K.; Hong, Y.H.; Kim, J.H.; Park, Y.; Chang, U.J.; Suh, H.J. Yeast Hydrolysate Can Reduce Body Weight and Abdominal Fat Accumulation in Obese Adults. Nutrition 2014, 30, 25–32. [Google Scholar] [CrossRef]
- Jung, E.Y.; Kim, S.Y.; Bae, S.H.; Chang, U.J.; Choi, J.W.; Suh, H.J. Weight Reduction Effects of Yeast Hydrolysate below 10 KDa on Obese Ypung Women. J. Food Biochem. 2011, 35, 337–350. [Google Scholar] [CrossRef]
- Molina, R.M.; Sitjas, F.X.C.; Castellana, J.C.; Gutiérrez, J.S.; Martínez, M.R.; Buraglia, M.Á.B.M.; Cediel, I.M.-A.; Caballero, Á.M.H. Fat Binder Obtained from Biomass Resulting from Beer Production. WO2014001589A1, 3 January 2014. [Google Scholar]
- Santas, J.; Lázaro, E.; Cuñé, J. Effect of a Polysaccharide-Rich Hydrolysate from Saccharomyces Cerevisiae (LipiGo®) in Body Weight Loss: Randomised, Double-Blind, Placebo-Controlled Clinical Trial in Overweight and Obese Adults. J. Sci. Food Agric. 2017, 97, 4250–4257. [Google Scholar] [CrossRef] [PubMed]
- Valero-Pérez, M.; Bermejo, L.M.; López-Plaza, B.; García, M.A.; Palma-Milla, S.; Gómez-Candela, C. Regular Consumption of Lipigo® Promotes the Reduction of Body Weight and Improves the Rebound Effect of Obese People Undergo a Comprehensive Weight Loss Program. Nutrients 2020, 12, 1960. [Google Scholar] [CrossRef]
- Tremblay, A.J.; Morrissette, H.; Gagné, J.M.; Bergeron, J.; Gagné, C.; Couture, P. Validation of the Friedewald Formula for the Determination of Low-Density Lipoprotein Cholesterol Compared with β-Quantification in a Large Population. Clin. Biochem. 2004, 37, 785–790. [Google Scholar] [CrossRef] [PubMed]
- Mallol, R.; Amigó, N.; Rodríguez, M.A.; Heras, M.; Vinaixa, M.; Plana, N.; Rock, E.; Ribalta, J.; Yanes, O.; Masana, L.; et al. Liposcale: A Novel Advanced Lipoprotein Test Based on 2D Diffusion-Ordered 1H NMR Spectroscopy. J. Lipid Res. 2015, 56, 737–746. [Google Scholar] [CrossRef]
- Mallol, R.; Rodríguez, M.A.; Heras, M.; Vinaixa, M.; Cañellas, N.; Brezmes, J.; Plana, N.; Masana, L.; Correig, X. Surface Fitting of 2D Diffusion-Edited 1H NMR Spectroscopy Data for the Characterisation of Human Plasma Lipoproteins. Metabolomics 2011, 7, 572–582. [Google Scholar] [CrossRef]
- Johnson, C.S. Diffusion Ordered Nuclear Magnetic Resonance Spectroscopy: Principles and Applications. Prog. Nucl. Magn. Reson. Spectrosc. 1999, 34, 203–256. [Google Scholar] [CrossRef]
- Pintó, X.; Masana, L.; Civeira, F.; Real, J.; Ibarretxe, D.; Candas, B.; Puzo, J.; Díaz, J.L.; Amigó, N.; Esteban, M.; et al. Consensus Document of an Expert Group from the Spanish Society of Arteriosclerosis (SEA) on the Clinical Use of Nuclear Magnetic Resonance to Assess Lipoprotein Metabolism (Liposcale®). Clin. Investig. Arterioscler. 2020, 32, 219–229. [Google Scholar] [CrossRef]
- Havel, R.J.; Eder, H.A.; Bragdon, J.H. The Distribution and Chemical Composition of Ultracentrifugally Separated Lipoproteins in Human Serum. J. Clin. Investig. 1955, 34, 1345–1353. [Google Scholar] [CrossRef]
- De Juan-Franco, E.; Pérez, A.; Ribas, V.; Antonio Sánchez-Hernández, J.; Blanco-Vaca, F.; Ordóñez-Llanos, J.; Luis Sánchez-Quesada, J. Standardization of a Method to Evaluate the Antioxidant Capacity of High-Density Lipoproteins. Int. J. Biomed. Sci. Int. J. Biomed. Sci. 2009, 5, 402–410. [Google Scholar]
- Esterbauer, H.; Striegl, G.; Puhl, H.; Rotheneder, M. Continuous Monitoring of In Vitro Oxidation of Human Low Density Lipoprotein. Free Radic. Res. Commun. 1989, 6, 67–75. [Google Scholar] [CrossRef]
- Aldini, G.; Yeum, K.J.; Russell, R.M.; Krinsky, N.I. A Method to Measure the Oxidizability of Both the Aqueous and Lipid Compartments of Plasma. Free Radic. Biol. Med. 2001, 31, 1043–1050. [Google Scholar] [CrossRef]
- Padro, T.; Santisteban, V.; Huedo, P.; Puntes, M.; Aguiló, M.; Espadaler-Mazo, J.; Badimon, L. Lactiplantibacillus Plantarum Strains KABP011, KABP012, and KABP013 Modulate Bile Acids and Cholesterol Metabolism in Humans. Cardiovasc. Res. 2024, 120, 708–722. [Google Scholar] [CrossRef]
- Padro, T.; Muñoz-García, N.; Vilahur, G.; Chagas, P.; Deyà, A.; Antonijoan, R.M.; Badimon, L. Moderate Beer Intake and Cardiovascular Health in Overweight Individuals. Nutrients 2018, 10, 1237. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and Beta-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Bonizzi, A.; Piuri, G.; Corsi, F.; Cazzola, R.; Mazzucchelli, S. HDL Dysfunctionality: Clinical Relevance of Quality Rather than Quantity. Biomedicines 2021, 9, 729. [Google Scholar] [CrossRef]
- THE 17 GOALS|Sustainable Development. Available online: https://sdgs.un.org/goals (accessed on 5 September 2024).
- Lee, S.; Kim, Y.; Han, M. Influence of Waist Circumference Measurement Site on Visceral Fat and Metabolic Risk in Youth. J. Obes. Metab. Syndr. 2022, 31, 296–302. [Google Scholar] [CrossRef]
- Yu, J.; Xia, J.; Yang, C.; Pan, D.; Xu, D.; Sun, G.; Xia, H. Effects of Oat Beta-Glucan Intake on Lipid Profiles in Hypercholesterolemic Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Nutrients 2022, 14, 2043. [Google Scholar] [CrossRef]
- Ho, H.V.T.; Sievenpiper, J.L.; Zurbau, A.; Blanco Mejia, S.; Jovanovski, E.; Au-Yeung, F.; Jenkins, A.L.; Vuksan, V. The Effect of Oat β-Glucan on LDL-Cholesterol, Non-HDL-Cholesterol and ApoB for CVD Risk Reduction: A Systematic Review and Meta-Analysis of Randomised-Controlled Trials. Br. J. Nutr. 2016, 116, 1369–1382. [Google Scholar] [CrossRef]
- Nwachukwu, I.D.; Devassy, J.G.; Aluko, R.E.; Jones, P.J.H. Cholesterol-Lowering Properties of Oat β-Glucan and the Promotion of Cardiovascular Health: Did Health Canada Make the Right Call? Appl. Physiol. Nutr. Metab. 2015, 40, 535–542. [Google Scholar] [CrossRef]
- Kanauchi, O.; Deuchi, K.; Imasato, Y.; Shizukuishi, M.; Kobayashi, E. Mechanism for the Inhibition of Fat Digestion by Chitosan and for the Synergistic Effect of Ascorbate. Biosci. Biotechnol. Biochem. 1995, 59, 786–790. [Google Scholar] [CrossRef]
- Othman, R.A.; Moghadasian, M.H.; Jones, P.J.H. Cholesterol-Lowering Effects of Oat β-Glucan. Nutr. Rev. 2011, 69, 299–309. [Google Scholar] [CrossRef]
- Ausar, S.F.; Morcillo, M.; León, A.E.; Ribotta, P.D.; Masih, R.; Vilaro Mainero, M.; Amigone, J.L.; Rubin, G.; Lescano, C.; Castagna, L.F.; et al. Improvement of HDL- and LDL-Cholesterol Levels in Diabetic Subjects by Feeding Bread Containing Chitosan. J. Med. Food 2003, 6, 397–399. [Google Scholar] [CrossRef] [PubMed]
- Maezaki, Y.; Tsuji, K.; Nakagawa, Y.; Kawai, Y.; Akimoto, M.; Tsugita, T.; Takekawa, W.; Terada, A.; Hara, H.; Mitsuoka, T. Hypocholesterolemic Effect of Chitosan in Adult Males. Biosci. Biotechnol. Biochem. 1993, 57, 1439–1444. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Fogacci, F.; Veronesi, M.; Strocchi, E.; Grandi, E.; Rizzoli, E.; Poli, A.; Marangoni, F.; Borghi, C. A Randomized Placebo-Controlled Clinical Trial to Evaluate the Medium-Term Effects of Oat Fibers on Human Health: The Beta-Glucan Effects on Lipid Profile, Glycemia and InTestinal Health (BELT) Study. Nutrients 2020, 12, 686. [Google Scholar] [CrossRef] [PubMed]
- Anraku, M.; Fujii, T.; Furutani, N.; Kadowaki, D.; Maruyama, T.; Otagiri, M.; Gebicki, J.M.; Tomida, H. Antioxidant Effects of a Dietary Supplement: Reduction of Indices of Oxidative Stress in Normal Subjects by Water-Soluble Chitosan. Food Chem. Toxicol. 2009, 47, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Berecochea-Lopez, A.; Decordé, K.; Ventura, E.; Godard, M.; Bornet, A.; Teissèdre, P.L.; Cristol, J.P.; Rouanet, J.M. Fungal Chitin−Glucan from Aspergillus Niger Efficiently Reduces Aortic Fatty Streak Accumulation in the High-Fat Fed Hamster, an Animal Model of Nutritionally Induced Atherosclerosis. J. Agric. Food Chem. 2009, 57, 1093–1098. [Google Scholar] [CrossRef] [PubMed]
- Bays, H.E.; Evans, J.L.; Maki, K.C.; Evans, M.; Maquet, V.; Cooper, R.; Anderson, J.W. Chitin-Glucan Fiber Effects on Oxidized Low-Density Lipoprotein: A Randomized Controlled Trial. Eur. J. Clin. Nutr. 2013, 67, 2. [Google Scholar] [CrossRef]
- Kounatidis, D.; Vallianou, N.G.; Poulaki, A.; Evangelopoulos, A.; Panagopoulos, F.; Stratigou, T.; Geladari, E.; Karampela, I.; Dalamaga, M. ApoB100 and Atherosclerosis: What’s New in the 21st Century? Metabolites 2024, 14, 123. [Google Scholar] [CrossRef]
- Carr, S.S.; Hooper, A.J.; Sullivan, D.R.; Burnett, J.R. Non-HDL-Cholesterol and Apolipoprotein B Compared with LDL-Cholesterol in Atherosclerotic Cardiovascular Disease Risk Assessment. Pathology 2019, 51, 148–154. [Google Scholar] [CrossRef]
- Cugnet-Anceau, C.; Nazare, J.A.; Biorklund, M.; Le Coquil, E.; Sassolas, A.; Sothier, M.; Holm, J.; Landin-Olsson, M.; Önning, G.; Laville, M.; et al. A Controlled Study of Consumption of Beta-Glucan-Enriched Soups for 2 Months by Type 2 Diabetic Free-Living Subjects. Br. J. Nutr. 2010, 103, 422–428. [Google Scholar] [CrossRef]
- Rondanelli, M.; Opizzi, A.; Monteferrario, F.; Klersy, C.; Cazzola, R.; Cestaro, B. Beta-Glucan- or Rice Bran-Enriched Foods: A Comparative Crossover Clinical Trial on Lipidic Pattern in Mildly Hypercholesterolemic Men. Eur. J. Clin. Nutr. 2011, 65, 864–871. [Google Scholar] [CrossRef] [PubMed]
- Spigoni, V.; Aldigeri, R.; Antonini, M.; Micheli, M.M.; Fantuzzi, F.; Fratter, A.; Pellizzato, M.; Derlindati, E.; Zavaroni, I.; Bonadonna, R.C.; et al. Effects of a New Nutraceutical Formulation (Berberine, Red Yeast Rice and Chitosan) on Non-HDL Cholesterol Levels in Individuals with Dyslipidemia: Results from a Randomized, Double Blind, Placebo-Controlled Study. Int. J. Mol. Sci. 2017, 18, 1498. [Google Scholar] [CrossRef] [PubMed]
- Siebel, A.L.; Heywood, S.E.; Kingwell, B.A. HDL and Glucose Metabolism: Current Evidence and Therapeutic Potential. Front. Pharmacol. 2015, 6, 258. [Google Scholar] [CrossRef] [PubMed]
- Andrade, E.F.; Lobato, R.V.; De Araújo, T.V.; Zangerônimo, M.G.; De Sousa, R.V.; Pereira, L.J. Effect of Beta-Glucans in the Control of Blood Glucose Levels of Diabetic Patients: A Systematic Review. Nutr. Hosp. 2014, 31, 170–177. [Google Scholar] [CrossRef]
- Guo, W.; Yi, L.; Zhou, B.; Li, M. Chitosan Modifies Glycemic Levels in People with Metabolic Syndrome and Related Disorders: Meta-Analysis with Trial Sequential Analysis. Nutr. J. 2020, 19, 130. [Google Scholar] [CrossRef]
- Behall, K.M.; Scholfield, D.J.; Hallfrisch, J. Diets Containing Barley Significantly Reduce Lipids in Mildly Hypercholesterolemic Men and Women. Am. J. Clin. Nutr. 2004, 80, 1185–1193. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ingredients (mg in Each Stick) | ||
|---|---|---|
| βGluCnCs | Placebo | |
| β-glucan | 909 | 0 |
| Chitin–chitosan | 91 | 0 |
| Microcrystalline cellulose | 0 | 1000 |
| Xylitol | 23 | 23 |
| Isomaltitol | 129.5 | 129.5 |
| Gum Arabic | 32.2 | 32.2 |
| Citric acid | 2 | 2 |
| Orange flavor | 200 | 200 |
| Sucralose | 0.4 | 0.4 |
| Stevia | 0.4 | 0.4 |
| Silicon dioxide | 12.5 | 12.5 |
| Baseline | Week 4 | Week 8 | Week 12 | p-Value | |
|---|---|---|---|---|---|
| βGluCnCs | |||||
| TC (mg/dL) | 193.2 ± 4.86 | 193.2 ± 5.2 | 194.0 ± 5.0 | 200.2 ± 5.6 | 0.059 |
| HDLc (mg/dL) | 51.8 ± 1.68 | 54.3 ± 1.9 | 55.6 ± 1.9 | 56.2 ± 2.1 | 0.001 |
| Non-HDLc (mg/dL) | 141.4 ± 4.9 | 138.8 ± 5.1 | 138.4 ± 4.8 | 144.0 ± 5.3 | 0.108 |
| HDLc/non-HDLc | 0.39 ± 0.02 | 0.42 ± 0.02 | 0.42 ± 0.02 | 0.42 ± 0.02 | 0.002 |
| HDLc/TC | 0.27 ± 0.01 | 0.29 ± 0.01 | 0.29 ± 0.01 | 0.29 ± 0.01 | 0.002 |
| LDLc (mg/dL) | 122.6 ± 4.3 | 117.3 ± 4.3 | 118.4 ± 4.4 | 124.1 ± 4.4 | 0.032 |
| VLDLc (mg/dL) | 18.8 ± 1.4 | 21.5 ± 2.4 | 20.0 ± 1.47 | 19.9 ± 2.0 | 0.349 |
| TG (mg/dL) | 95.2 ± 7.1 | 109.0 ± 12.0 | 101.0 ± 7.4 | 100.3 ± 10.2 | 0.343 |
| Placebo | |||||
| TC (mg/dL) | 187.0 ± 8.1 | 185.5 ± 8.0 | 187.5 ± 9.0 | 188.6 ± 9.7 | 0.868 |
| HDLc (mg/dL) | 48.3 ± 2.7 | 49.9 ± 2.8 | 51.1 ± 3.3 | 51.2 ± 3.5 | 0.066 |
| Non-HDLc (mg/dL) | 138.7 ± 8.1 | 135.7 ± 7.7 | 136.4 ± 8.4 | 137.4 ± 9.0 | 0.799 |
| HDLc/non-HDLc | 0.37 ± 0.03 | 0.38 ± 0.03 | 0.40 ± 0.03 | 0.39 ± 0.03 | 0.169 |
| HDLc/TC | 0.26 ± 0.02 | 0.27 ± 0.01 | 0.28 ± 0.02 | 0.28 ± 0.02 | 0.147 |
| LDLc (mg/dL) | 117.8 ± 7.7 | 112.5 ± 8.5 | 115.3 ± 9.0 | 116.3 ± 9.5 | 0.499 |
| VLDLc (mg/dL) | 20.9 ± 1.9 | 23.2 ± 3.7 | 21.2 ± 2.013 | 21.1 ± 1.7 | 0.657 |
| TG (mg/dL) | 105.6 ± 9.6 | 117.2 ± 18.7 | 107.1 ± 10.3 | 106.6 ± 8.5 | 0.653 |
| Baseline | Week 12 | p-Value | |
|---|---|---|---|
| βGluQnQs | |||
| ApoA1 (mg/mL) | 1.16 ± 0.03 | 1.09 ± 0.04 | 0.295 |
| ApoB (mg/mL) | 0.43 ± 0.03 | 0.32 ± 0.02 | 0.001 |
| ApoA1/ApoB | 2.72 ± 0.20 | 3.75 ± 0.30 | 0.002 |
| Placebo | |||
| ApoA1 (mg/mL) | 1.02 ± 0.05 | 0.93 ± 0.04 | 0.066 |
| ApoB (mg/mL) | 0.49 ± 0.04 | 0.38 ± 0.05 | 0.062 |
| ApoA1/ApoB | 2.37 ± 0.31 | 2.79 ± 0.27 | 0.217 |
| Baseline | Week 12 | p-Value | ||
|---|---|---|---|---|
| ApoA1 (mg/mL) | Women | 1.07 ± 0.04 | 1.11 ± 0.05 | 0.272 |
| Men | 1.04 ± 0.05 | 1.05 ± 0.05 | 0.815 | |
| ApoB (mg/mL) | Women | 0.40 ± 0.03 | 0.30 ± 0.03 | 0.059 |
| Men | 0.48 ± 0.04 | 0.35 ± 0.04 | 0.005 | |
| ApoA1/ApoB | Women | 2.94 ± 0.26 | 4.01 ± 0.38 | 0.024 |
| Men | 2.40 ± 0.30 | 3.38 ± 0.49 | 0.049 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santisteban, V.; Muñoz-Garcia, N.; López-Yerena, A.; Puntes, M.; Badimon, L.; Padro, T. Efficacy of Food Industry By-Product β-Glucan/Chitin–Chitosan on Lipid Profile of Overweight and Obese Individuals: Sustainability and Nutraceuticals. Nutrients 2024, 16, 3420. https://doi.org/10.3390/nu16193420
Santisteban V, Muñoz-Garcia N, López-Yerena A, Puntes M, Badimon L, Padro T. Efficacy of Food Industry By-Product β-Glucan/Chitin–Chitosan on Lipid Profile of Overweight and Obese Individuals: Sustainability and Nutraceuticals. Nutrients. 2024; 16(19):3420. https://doi.org/10.3390/nu16193420
Chicago/Turabian StyleSantisteban, Victoria, Natàlia Muñoz-Garcia, Anallely López-Yerena, Montserrat Puntes, Lina Badimon, and Teresa Padro. 2024. "Efficacy of Food Industry By-Product β-Glucan/Chitin–Chitosan on Lipid Profile of Overweight and Obese Individuals: Sustainability and Nutraceuticals" Nutrients 16, no. 19: 3420. https://doi.org/10.3390/nu16193420