
Macronutrient Intake during Complementary Feeding in Very Low Birth Weight Infants Comparing Early and Late Introduction of Solid Foods: A Secondary Outcome Analysis
 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Group Stratification
2.2. Study Visits, Data Collection and Evaluation
2.3. Outcome Data
2.4. Statistical Analysis
3. Results
3.1. Study Participants, Baseline Characteristics and Dietary Records
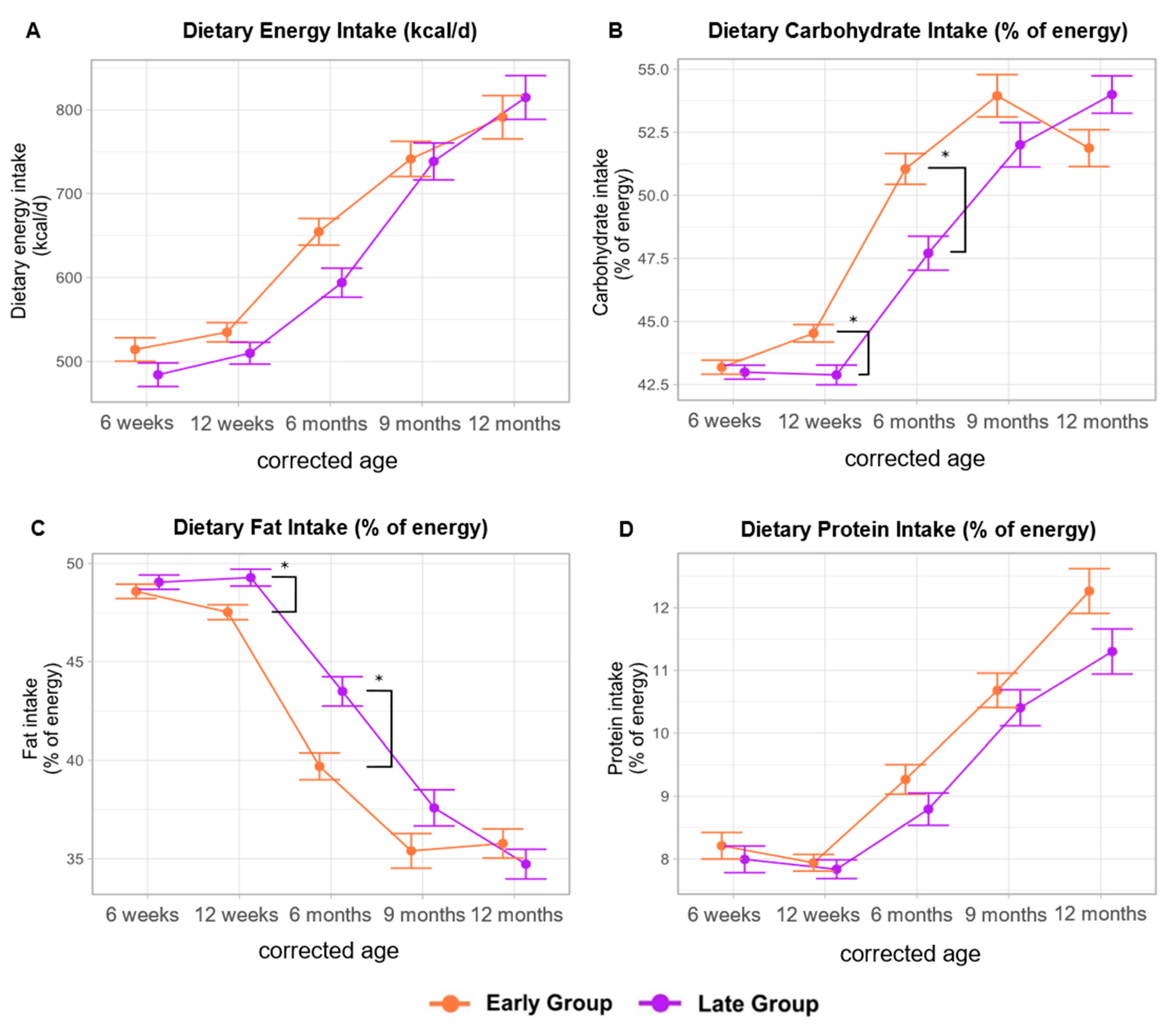
3.2. Macronutrient Intake Comparing Early Versus Late Introduction of Solid Foods
3.2.1. Dietary Protein Intake
3.2.2. Dietary Energy Intake and Macronutrient Distribution
3.2.3. Polyunsaturated Fatty Acid Profile
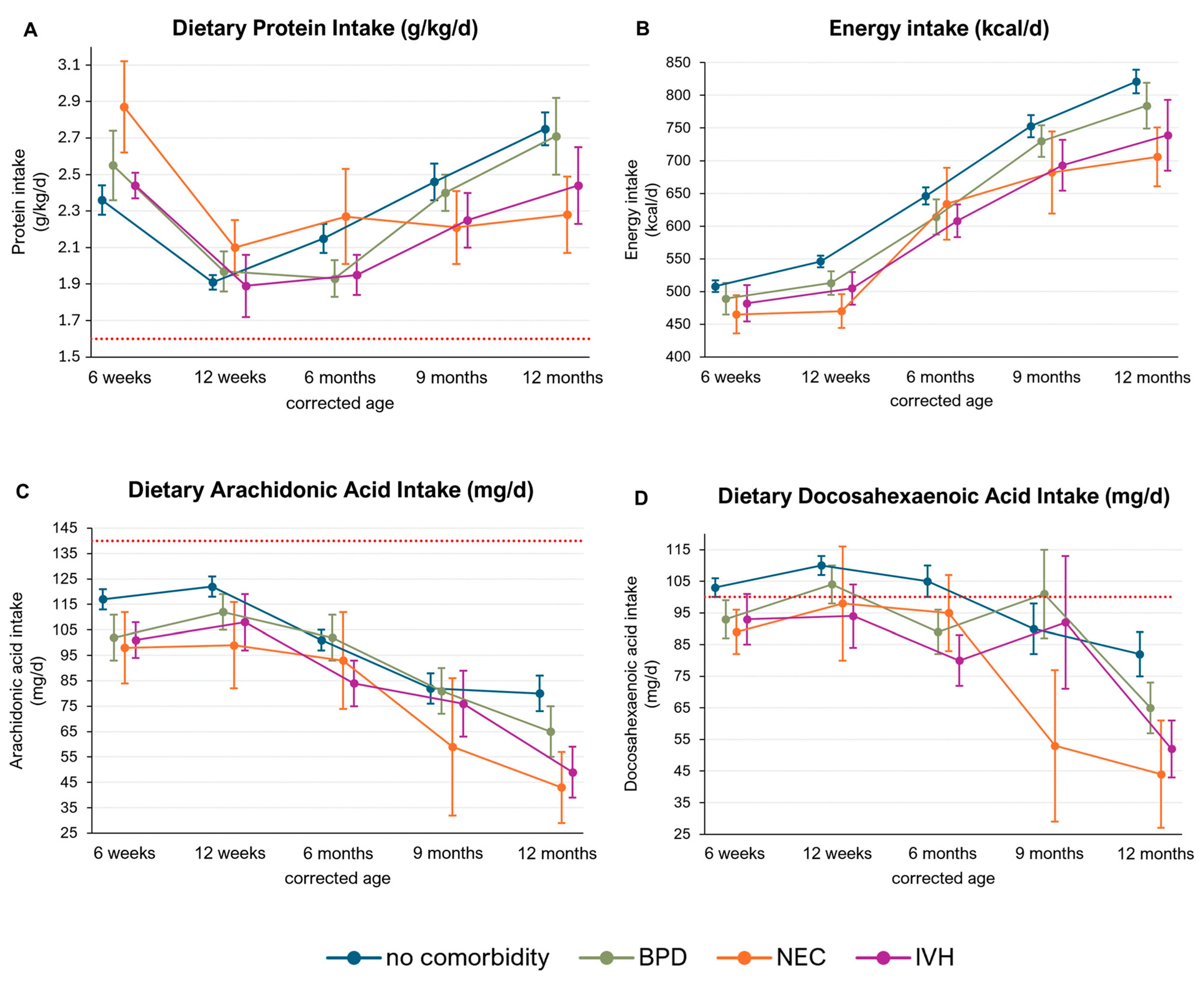
3.3. Macronutrient Intake in Infants with Preterm Birth-Related Comorbidities
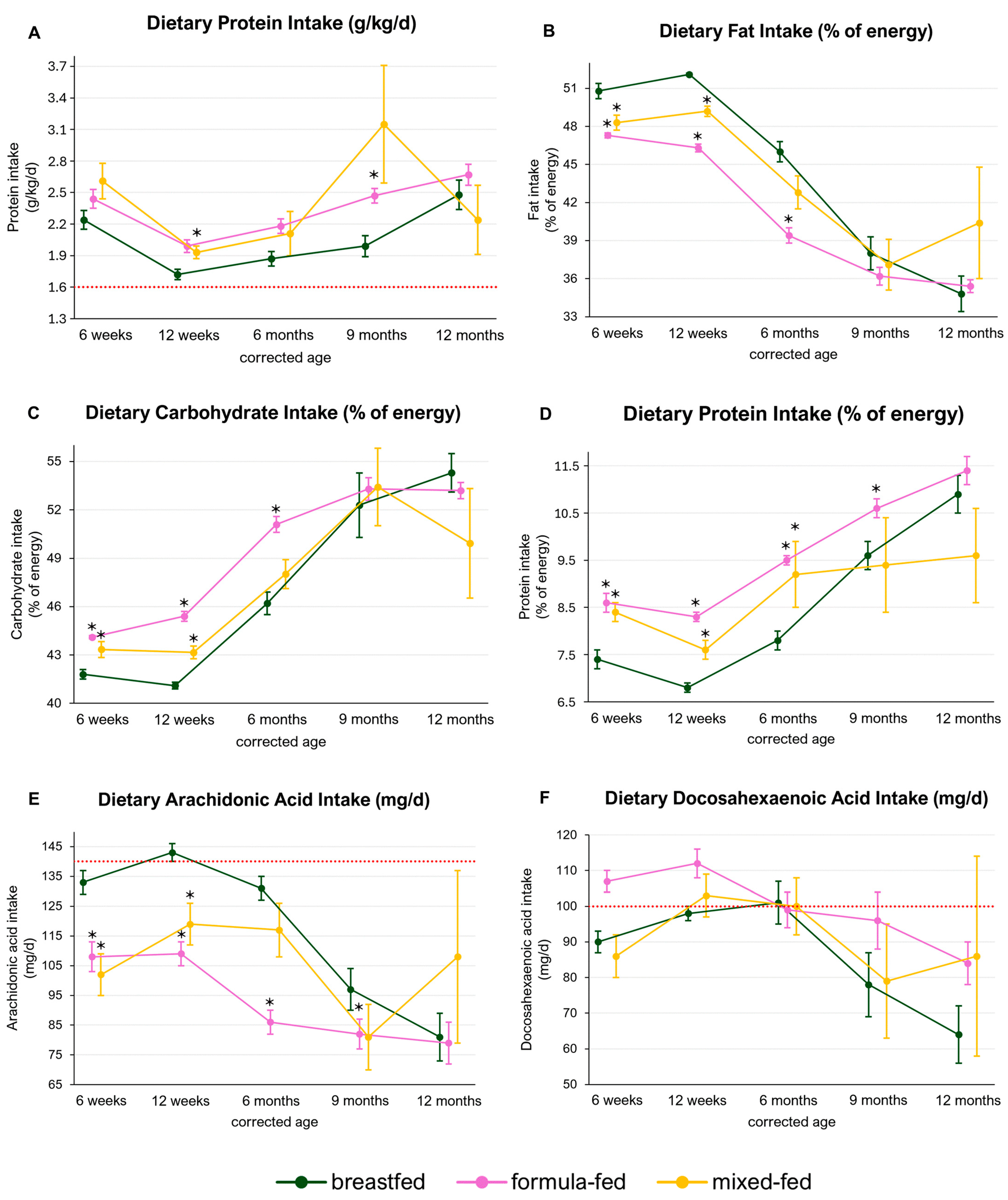
3.4. Macronutrient Intake in Breastfed, Formula-Fed and Mixed-Fed Infants
4. Discussion
4.1. Dietary Protein Intake
4.2. Dietary Fat Intake
Dietary PUFA Intake
4.3. Comorbidities
4.4. Type of Milk Feeding
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cusick, S.E.; Georgieff, M.K. The Role of Nutrition in Brain Development: The Golden Opportunity of the “First 1000 Days”. J. Pediatr. 2016, 175, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Mameli, C.; Mazzantini, S.; Zuccotti, G. Nutrition in the First 1000 Days: The Origin of Childhood Obesity. Int. J. Environ. Res. Public Health 2016, 13, 838. [Google Scholar] [CrossRef] [PubMed]
- Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Fidler Mis, N.; Hojsak, I.; Hulst, J.M.; Indrio, F.; Lapillonne, A.; et al. Complementary Feeding: A Position Paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Endrinikapoulos, A.; Afifah, D.N.; Mexitalia, M.; Andoyo, R.; Hatimah, I.; Nuryanto, N. Study of the importance of protein needs for catch-up growth in Indonesian stunted children: A narrative review. SAGE Open Med. 2023, 11, 20503121231165562. [Google Scholar] [CrossRef]
- Krebs, N.F.; Lozoff, B.; Georgieff, M.K. Neurodevelopment: The Impact of Nutrition and Inflammation During Infancy in Low-Resource Settings. Pediatrics 2017, 139, S50–S58. [Google Scholar] [CrossRef]
- Voortman, T.; Braun, K.V.E.; Kiefte-De Jong, J.C.; Jaddoe, V.W.V.; Franco, O.H.; Van Den Hooven, E.H. Protein intake in early childhood and body composition at the age of 6 years: The Generation R Study. Int. J. Obes. 2016, 40, 1018–1025. [Google Scholar] [CrossRef]
- Weber, M.; Grote, V.; Closa-Monasterolo, R.; Escribano, J.; Langhendries, J.-P.; Dain, E.; Giovannini, M.; Verduci, E.; Gruszfeld, D.; Socha, P.; et al. Lower protein content in infant formula reduces BMI and obesity risk at school age: Follow-up of a randomized trial. Am. J. Clin. Nutr. 2014, 99, 1041–1051. [Google Scholar] [CrossRef]
- Sambra, V.; Echeverria, F.; Valenzuela, A.; Chouinard-Watkins, R.; Valenzuela, R. Docosahexaenoic and Arachidonic Acids as Neuroprotective Nutrients throughout the Life Cycle. Nutrients 2021, 13, 986. [Google Scholar] [CrossRef]
- Gow, R.V.; Hibbeln, J.R. Omega-3 Fatty Acid and Nutrient Deficits in Adverse Neurodevelopment and Childhood Behaviors. Child. Adolesc. Psychiatr. Clin. N. Am. 2014, 23, 555–590. [Google Scholar] [CrossRef]
- Gupta, S.; Agarwal, R.; Aggarwal, K.C.; Chellani, H.; Duggal, A.; Arya, S.; Bhatia, S.; Sankar, M.J.; Sreenivas, V.; Jain, V.; et al. Complementary feeding at 4 versus 6 months of age for preterm infants born at less than 34 weeks of gestation: A randomised, open-label, multicentre trial. Lancet Glob. Health 2017, 5, e501–e511. [Google Scholar] [CrossRef]
- Marriott, L.D. Weaning preterm infants: A randomised controlled trial. Arch. Dis. Child.—Fetal Neonatal Ed. 2003, 88, F302–F307. [Google Scholar] [CrossRef] [PubMed]
- Haiden, N.; Thanhaeuser, M.; Eibensteiner, F.; Huber-Dangl, M.; Gsoellpointner, M.; Ristl, R.; Kroyer, B.; Brandstetter, S.; Kornsteiner-Krenn, M.; Binder, C.; et al. Randomized Controlled Trial of Two Timepoints for Introduction of Standardized Complementary Food in Preterm Infants. Nutrients 2022, 14, 697. [Google Scholar] [CrossRef] [PubMed]
- Gsoellpointner, M.; Eibensteiner, F.; Thanhaeuser, M.; Ristl, R.; Jilma, B.; Berger, A.; Haiden, N. Effects of early introduction of solid foods on nutrient intake in preterm infants during their 1st year of life: A secondary outcome analysis of a prospective, randomized intervention study. Front. Nutr. 2023, 10, 1124544. [Google Scholar] [CrossRef] [PubMed]
- Thanhaeuser, M.; Gsoellpointner, M.; Kornsteiner-Krenn, M.; Steyrl, D.; Brandstetter, S.; Jilma, B.; Berger, A.; Haiden, N. Introduction of Solid Foods in Preterm Infants and Its Impact on Growth in the First Year of Life—A Prospective Observational Study. Nutrients 2024, 16, 2077. [Google Scholar] [CrossRef] [PubMed]
- Dewey, K.G.; Beaton, G.; Fjeld, C.; Lönnerdal, B.; Reeds, P. Protein requirements of infants and children. Eur. J. Clin. Nutr. 1996, 50 (Suppl. 1), S119–S147; discussion S147–S150. [Google Scholar]
- Baldassarre, M.E.; Panza, R.; Cresi, F.; Salvatori, G.; Corvaglia, L.; Aceti, A.; Giannì, M.L.; Liotto, N.; Ilardi, L.; Laforgia, N.; et al. Complementary feeding in preterm infants: A position paper by Italian neonatal, paediatric and paediatric gastroenterology joint societies. Ital. J. Pediatr. 2022, 48, 143. [Google Scholar] [CrossRef]
- Deutsche Gesellschaft für Ernährung, Österreichische Gesellschaft für Ernährung. Referenzwerte für die Nährstoffzufuhr, 2nd ed.; 8th updated ed.; Neuer Umschau Buchverlag: Bonn, Germany, 2024. [Google Scholar]
- EFSA Panel on Dietetic Products, Nutrition, and Allergies (NDA). Scientific Opinion on Dietary Reference Values for fats, including saturated fatty acids, polyunsaturated fatty acids, monounsaturated fatty acids, trans fatty acids, and cholesterol. EFSA J. 2010, 8, 1461. [Google Scholar] [CrossRef]
- Koletzko, B.; Lien, E.; Agostoni, C.; Böhles, H.; Campoy, C.; Cetin, I.; Decsi, T.; Dudenhausen, J.W.; Dupont, C.; Forsyth, S.; et al. The roles of long-chain polyunsaturated fatty acids in pregnancy, lactation and infancy: Review of current knowledge and consensus recommendations. J. Perinat. Med. 2008, 36, 5–14. [Google Scholar] [CrossRef]
- Embleton, N.D.; Jennifer Moltu, S.; Lapillonne, A.; van den Akker, C.H.P.; Carnielli, V.; Fusch, C.; Gerasimidis, K.; van Goudoever, J.B.; Haiden, N.; Iacobelli, S.; et al. Enteral Nutrition in Preterm Infants (2022): A Position Paper from the ESPGHAN Committee on Nutrition and Invited Experts. J. Pediatr. Gastroenterol. Nutr. 2023, 76, 248–268. [Google Scholar] [CrossRef]
- Michaelsen, K.F.; Grummer-Strawn, L.; Bégin, F. Emerging issues in complementary feeding: Global aspects. Matern. Child. Nutr. 2017, 13, e12444. [Google Scholar] [CrossRef]
- Rolland-Cachera, M.F.; Maillot, M.; Deheeger, M.; Souberbielle, J.C.; Péneau, S.; Hercberg, S. Association of nutrition in early life with body fat and serum leptin at adult age. Int. J. Obes. 2013, 37, 1116–1122. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products, Nutrition, and Allergies (NDA). Scientific Opinion on nutrient requirements and dietary intakes of infants and young children in the European Union. EFSA J. 2013, 11, 3408. [Google Scholar] [CrossRef]
- Moltu, S.J.; Nordvik, T.; Rossholt, M.E.; Wendel, K.; Chawla, M.; Server, A.; Gunnarsdottir, G.; Pripp, A.H.; Domellöf, M.; Bratlie, M.; et al. Arachidonic and docosahexaenoic acid supplementation and brain maturation in preterm infants; a double blind RCT. Clin. Nutr. 2024, 43, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Gsoellpointner, M.; Thanhaeuser, M.; Eibensteiner, F.; Ristl, R.; Jilma, B.; Fuiko, R.; Brandstetter, S.; Berger, A.; Haiden, N. Polyunsaturated Fatty Acid Intake during Complementary Feeding and Neurodevelopmental Outcome in Very Low Birth Weight Infants. Nutrients 2023, 15, 3141. [Google Scholar] [CrossRef]
- Saini, R.K.; Keum, Y.S. Omega-3 and omega-6 polyunsaturated fatty acids: Dietary sources, metabolism, and significance—A review. Life Sci. 2018, 203, 255–267. [Google Scholar] [CrossRef]
- Smith, S.L.; Rouse, C.A. Docosahexaenoic acid and the preterm infant. Matern. Health Neonatol. Perinatol. 2017, 3, 22. [Google Scholar] [CrossRef]
- Simopoulos, A.P. The Importance of the Omega-6/Omega-3 Fatty Acid Ratio in Cardiovascular Disease and Other Chronic Diseases. Exp. Biol. Med. 2008, 233, 674–688. [Google Scholar] [CrossRef]
- Donahue, S.M.A.; Rifas-Shiman, S.L.; Gold, D.R.; Jouni, Z.E.; Gillman, M.W.; Oken, E. Prenatal fatty acid status and child adiposity at age 3 y: Results from a US pregnancy cohort. Am. J. Clin. Nutr. 2011, 93, 780–788. [Google Scholar] [CrossRef]
- Park, J.; Knafl, G.; Thoyre, S.; Brandon, D. Factors Associated with Feeding Progression in Extremely Preterm Infants. Nurs. Res. 2015, 64, 159–167. [Google Scholar] [CrossRef]
- Rocha, G.; Guimarães, H.; Pereira-da-Silva, L. The Role of Nutrition in the Prevention and Management of Bronchopulmonary Dysplasia: A Literature Review and Clinical Approach. Int. J. Environ. Res. Public Health 2021, 18, 6245. [Google Scholar] [CrossRef]
- Bott, L.; Béghin, L.; Devos, P.; Pierrat, V.; Matran, R.; Gottrand, F. Nutritional Status at 2 Years in Former Infants with Bronchopulmonary Dysplasia Influences Nutrition and Pulmonary Outcomes During Childhood. Pediatr. Res. 2006, 60, 340–344. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Wang, S.; Zhang, T.; Duan, S.; Wang, H. Neurodevelopmental outcomes in preterm or low birth weight infants with germinal matrix-intraventricular hemorrhage: A meta-analysis. Pediatr. Res. 2024, 95, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Liu, S.; Lu, M.; Huang, T.; Huang, L. Neurodevelopmental outcomes of preterm with necrotizing enterocolitis: A systematic review and meta-analysis. Eur. J. Pediatr. 2024, 183, 3147–3158. [Google Scholar] [CrossRef] [PubMed]
- Caroli, M.; Vania, A.; Tomaselli, M.A.; Scotese, I.; Tezza, G.; Verga, M.C.; Di Mauro, G.; Antignani, A.; Miniello, A.; Bergamini, M. Breastfed and Formula-Fed Infants: Need of a Different Complementary Feeding Model? Nutrients 2021, 13, 3756. [Google Scholar] [CrossRef]
- Pani, P.; Carletti, C.; Knowles, A.; Parpinel, M.; Concina, F.; Montico, M.; Cattaneo, A. Patterns of nutrients’ intake at six months in the northeast of Italy: A cohort study. BMC Pediatr. 2014, 14, 127. [Google Scholar] [CrossRef]
- Rozé, J.-C.; Darmaun, D.; Boquien, C.-Y.; Flamant, C.; Picaud, J.-C.; Savagner, C.; Claris, O.; Lapillonne, A.; Mitanchez, D.; Branger, B.; et al. The apparent breastfeeding paradox in very preterm infants: Relationship between breast feeding, early weight gain and neurodevelopment based on results from two cohorts, EPIPAGE and LIFT. BMJ Open 2012, 2, e000834. [Google Scholar] [CrossRef]
- Brenna, J.T.; Varamini, B.; Jensen, R.G.; Diersen-Schade, D.A.; Boettcher, J.A.; Arterburn, L.M. Docosahexaenoic and arachidonic acid concentrations in human breast milk worldwide. Am. J. Clin. Nutr. 2007, 85, 1457–1464. [Google Scholar] [CrossRef]
- European Commission. Commission Delegated Regulation (EU) 2016/127 of 25 September 2015 supplementing Regulation (EU) No 609/2013 of the European Parliament and of the Council as regards the specific compositional and information requirements for infant formula and follow-on formula and as regards requirements on information relating to infant and young child feeding. OJEC 2016, 59, 1–29. [Google Scholar]
- Aggett, P.J.; Agostoni, C.; Axelsson, I.; De Curtis, M.; Goulet, O.; Hernell, O.; Koletzko, B.; Lafeber, H.N.; Michaelsen, K.F.; Puntis, J.W.L.; et al. Feeding Preterm Infants After Hospital Discharge: A Commentary by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2006, 42, 596–603. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CA | Early Group n = 115 | Late Group n = 82 | Total |
|---|---|---|---|
| 6 weeks | 86 (74.8%) | 60 (73.2%) | 146 |
| 12 weeks | 106 (92.2%) | 64 (78.0%) | 170 |
| 6 months | 90 (78.2%) | 66 (80.5%) | 156 |
| 9 months | 63 (54.7%) | 51 (62.2%) | 114 |
| 12 months | 65 (56.0%) | 57 (69.5%) | 122 |
| Parameter | Early (n = 115) | Late (n = 82) | p-Value |
|---|---|---|---|
| Neonatal parameters | |||
| Male sex | 69 (60%) | 36 (44%) | 0.04 |
| Gestational age (weeks) | 27 + 1 (25 + 3–28 + 3) | 26 + 3 (24 + 6–28 + 2) | 0.33 |
| Birth weight (g) | 925 (718–1133) | 820 (650–1078) | 0.13 |
| Small for gestational age | 4 (3.5%) | 4 (4.9%) | 0.62 |
| Neonatal morbidities | |||
| Necrotizing enterocolitis ≥ grade II | 5 (4%) | 6 (7%) | 0.42 |
| Bronchopulmonary dysplasia | 14 (12%) | 23 (28%) | 0.01 |
| Intraventricular hemorrhage ≥ grade II | 17 (15%) | 12 (15%) | 0.74 |
| Periventricular leukomalacia | 0 (0%) | 1 (1%) | / |
| Nutrition | |||
| Introduction of solid foods (weeks CA) | 13.7 (12.6–15.4) | 19.4 (18.3–21.7) | <0.001 |
| Type of first solid food | |||
| Vegetables | 82 (71%) | 54 (66%) | 0.69 |
| Fruits | 17 (15%) | 14 (17%) | 0.82 |
| Milk and dairy products | 0 (0%) | 1 (1%) | / |
| Cereals (with gluten) | 1 (1%) | 1 (1%) | / |
| Cereals (without gluten) | 1 (1%) | 2 (2%) | / |
| Several | 11 (10%) | 7 (9%) | 0.99 |
| Type of milk feeding at 6 weeks CA | |||
| Breastfed | 28 (24%) | 34 (42%) | 0.01 |
| Formula fed | 66 (57%) | 31 (38%) | 0.01 |
| Mixed fed | 18 (16%) | 15 (18%) | 1.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gsoellpointner, M.; Thanhaeuser, M.; Kornsteiner-Krenn, M.; Eibensteiner, F.; Ristl, R.; Jilma, B.; Brandstetter, S.; Berger, A.; Haiden, N. Macronutrient Intake during Complementary Feeding in Very Low Birth Weight Infants Comparing Early and Late Introduction of Solid Foods: A Secondary Outcome Analysis. Nutrients 2024, 16, 3422. https://doi.org/10.3390/nu16193422
Gsoellpointner M, Thanhaeuser M, Kornsteiner-Krenn M, Eibensteiner F, Ristl R, Jilma B, Brandstetter S, Berger A, Haiden N. Macronutrient Intake during Complementary Feeding in Very Low Birth Weight Infants Comparing Early and Late Introduction of Solid Foods: A Secondary Outcome Analysis. Nutrients. 2024; 16(19):3422. https://doi.org/10.3390/nu16193422
Chicago/Turabian StyleGsoellpointner, Melanie, Margarita Thanhaeuser, Margit Kornsteiner-Krenn, Fabian Eibensteiner, Robin Ristl, Bernd Jilma, Sophia Brandstetter, Angelika Berger, and Nadja Haiden. 2024. "Macronutrient Intake during Complementary Feeding in Very Low Birth Weight Infants Comparing Early and Late Introduction of Solid Foods: A Secondary Outcome Analysis" Nutrients 16, no. 19: 3422. https://doi.org/10.3390/nu16193422