
The Effect of a Program to Improve Adherence to the Mediterranean Diet on Cardiometabolic Parameters in 7034 Spanish Workers

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
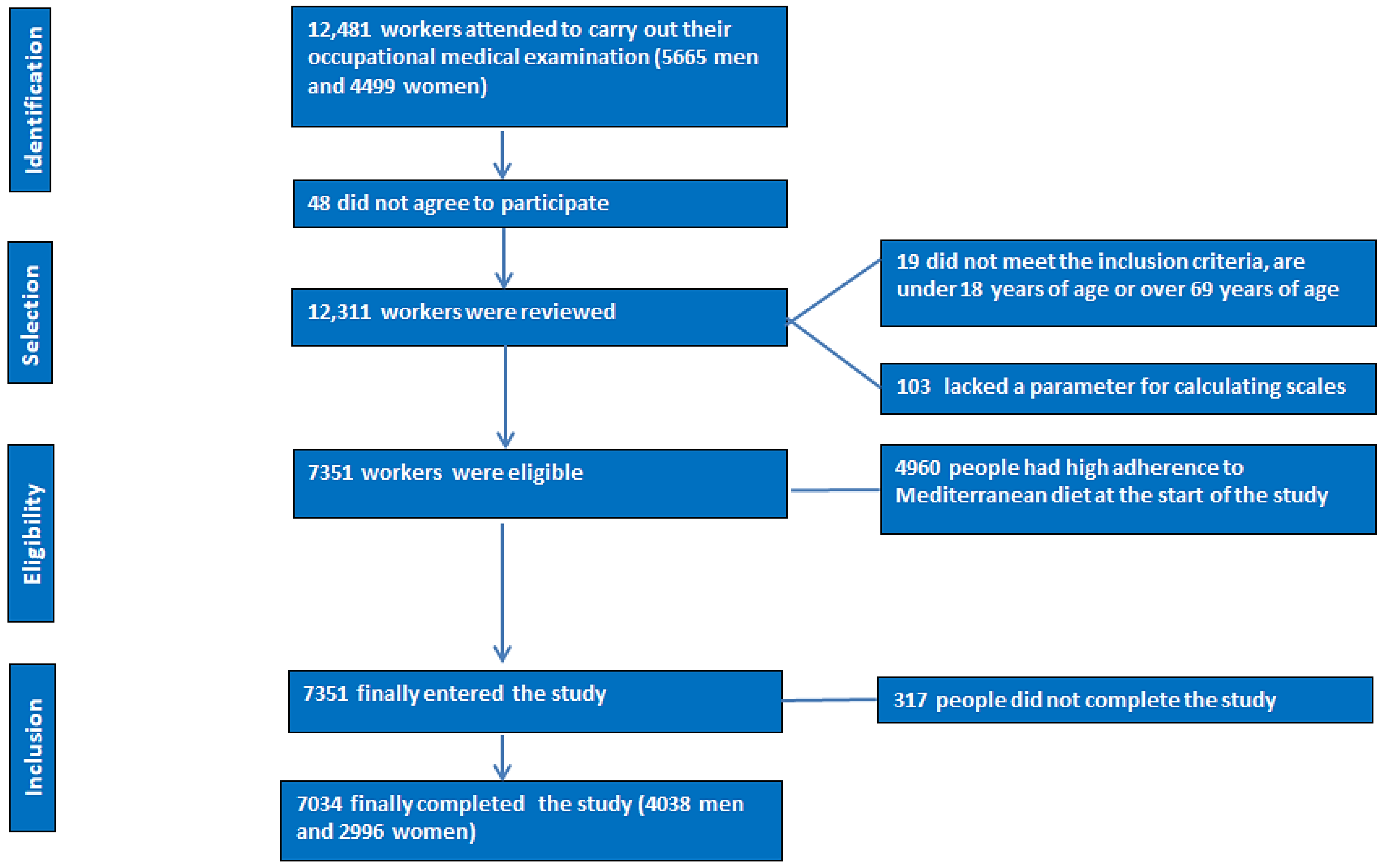
2.1. Participants
- -
- Being between 18 and 69 years of age;
- -
- Belonging to one of the companies included in this study;
- -
- Agreeing to participate in this study;
- -
- Presenting low adherence to the Mediterranean diet at the beginning of this study.
2.2. Determination of Variables
- -
- Anamnesis. A comprehensive clinical history in which data on sociodemographic variables such as age, sex, and adherence to the Mediterranean diet were collected.
- -
- Anthropometric and clinical determinations. These included height, weight, waist and hip circumference, and systolic and diastolic blood pressure.
- -
- Analytical determinations. The lipid profile and glycaemia were determined.
2.2.1. Anthropometric Determinations
2.2.2. Clinical Determinations
2.2.3. Analytical Determinations
2.2.4. Risk Scales
2.3. Statistical Analysis
3. Results
4. Discussion
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chew, N.W.S.; Ng, C.H.; Tan, D.J.H.; Kong, G.; Lin, C.; Chin, Y.H.; Lim, W.H.; Huang, D.Q.; Quek, J.; Fu, C.E.; et al. The global burden of metabolic disease: Data from 2000 to 2019. Cell Metab. 2023, 35, 414–428.e3. [Google Scholar] [CrossRef]
- Osborn, B.; Haemer, M.A. Dietary Patterns and Their Association with Cardiometabolic Biomarkers and Outcomes among Hispanic Adults: A Cross-Sectional Study from the National Health and Nutrition Examination Survey (2013–2018). Nutrients 2023, 15, 4641. [Google Scholar] [CrossRef]
- World Health Organization. Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 27 January 2024).
- Yusuf, S.; Joseph, P.; Rangarajan, S.; Islam, S.; Mente, A.; Hystad, P.; Brauer, M.; Kutty, V.R.; Gupta, R.; Wielgosz, A.; et al. Modifiable risk factors, cardiovascular disease, and mortality in 155 722 individuals from 21 high-income, middle-income, and low-income countries (PURE): A prospective cohort study. Lancet 2020, 395, 795–808, Erratum in: Lancet 2020, 395, 784. [Google Scholar] [CrossRef]
- Vicente-Herrero, M.T.; Ramírez-Iñiguez de la Torre, M.V.; López González, A.A. Cardiometabolic risk level estimated in workers with overweight/obesity. Lifestyle and sociodemographic variables. Acad. J. Health Sci. 2022, 37, 134–141. [Google Scholar] [CrossRef]
- GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Yi, Y.; An, J. Sex Differences in Risk Factors for Metabolic Syndrome in the Korean Population. Int. J. Environ. Res. Public Health 2020, 17, 9513. [Google Scholar] [CrossRef]
- Kuma, A.; Kato, A. Lifestyle-Related Risk Factors for the Incidence and Progression of Chronic Kidney Disease in the Healthy Young and Middle-Aged Population. Nutrients 2022, 14, 3787. [Google Scholar] [CrossRef]
- Chong, B.; Kong, G.; Shankar, K.; Chew, H.S.J.; Lin, C.; Goh, R.; Chin, Y.H.; Tan, D.J.H.; Chan, K.E.; Lim, W.H.; et al. The global syndemic of metabolic diseases in the young adult population: A consortium of trends and projections from the Global Burden of Disease 2000–2019. Metabolism 2023, 141, 155402. [Google Scholar] [CrossRef]
- World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks. Available online: https://apps.who.int/iris/bitstream/handle/10665/44203/9789241563871_eng.pdf (accessed on 28 January 2024).
- Moffat, K.; Mercer, S.W. Challenges of managing people with multimorbidity in today’s healthcare systems. BMC Fam. Pract. 2015, 16, 129. [Google Scholar] [CrossRef]
- Beaglehole, R.; Epping-Jordan, J.; Patel, V.; Chopra, M.; Ebrahim, S.; Kidd, M.; Haines, A. Improving the prevention and management of chronic disease in low-income and middle-income countries: A priority for primary health care. Lancet 2008, 372, 940–949. [Google Scholar] [CrossRef]
- Drozdz, D.; Alvarez-Pitti, J.; Wójcik, M.; Borghi, C.; Gabbianelli, R.; Mazur, A.; Herceg-Čavrak, V.; Lopez-Valcarcel, B.G.; Brzeziński, M.; Lurbe, E.; et al. Obesity and Cardiometabolic Risk Factors: From Childhood to Adulthood. Nutrients 2021, 13, 4176. [Google Scholar] [CrossRef]
- Calcaterra, V.; Cena, H.; Magenes, V.C.; Vincenti, A.; Comola, G.; Beretta, A.; Di Napoli, I.; Zuccotti, G. Sugar-Sweetened Beverages and Metabolic Risk in Children and Adolescents with Obesity: A Narrative Review. Nutrients 2023, 15, 702. [Google Scholar] [CrossRef]
- Stol, D.M.; Over, E.A.B.; Badenbroek, I.F.; Hollander, M.; Nielen, M.M.J.; Kraaijenhagen, R.A.; Schellevis, F.G.; de Wit, N.J.; de Wit, G.A. Cost-effectiveness of a stepwise cardiometabolic disease prevention program: Results of a randomized controlled trial in primary care. BMC Med. 2021, 19, 57. [Google Scholar] [CrossRef]
- Fernández-de-Bobadilla, J.; López-de-Sá, E. Economic and Social Burden of Coronary Heart Disease. Rev. Esp. Cardiol. Supl. 2013, 13, 42–47. [Google Scholar] [CrossRef]
- Ferrara, P. Assessing the Economic Burden of Disease in Migrants: The Diabetes Case in Northern Italy. Int. J. Environ. Res. Public Health 2020, 17, 2250. [Google Scholar] [CrossRef]
- Liu, J.; Liu, M.; Chai, Z.; Li, C.; Wang, Y.; Shen, M.; Zhuang, G.; Zhang, L. Projected rapid growth in diabetes disease burden and economic burden in China: A spatio-temporal study from 2020 to 2030. Lancet Reg. Health West Pac. 2023, 33, 100700. [Google Scholar] [CrossRef]
- Luengo-Fernandez, R.; Walli-Attaei, M.; Gray, A.; Torbica, A.; Maggioni, A.P.; Huculeci, R.; Bairami, F.; Aboyans, V.; Timmis, A.D.; Vardas, P.; et al. Economic burden of cardiovascular diseases in the European Union: A population-based cost study. Eur. Heart J. 2023, 44, 4752–4767. [Google Scholar] [CrossRef]
- Chen, P.; Zhang, M.; Zhang, Y.; Su, X.; Chen, J.; Xu, B.; Tao, J.; Wang, Z.; Ma, A.; Li, H. Economic Burden of Myocardial Infarction Combined with Dyslipidemia. Front. Public Health 2021, 9, 648172. [Google Scholar] [CrossRef]
- Cai, S.; Huang, F.; Wang, R.; Wu, M.; Liu, M.; Peng, Y.; Cao, G.; Li, Y.; Liu, S.; Lu, J.; et al. Habitual physical activity improves outcomes among patients with myocardial infarction. Front. Cardiovasc. Med. 2023, 10, 1174466. [Google Scholar] [CrossRef]
- Shi, L.; Fonseca, V.; Childs, B. Economic burden of diabetes-related hypoglycemia on patients, payors, and employers. J. Diabetes Complicat. 2021, 35, 107916. [Google Scholar] [CrossRef]
- Chaput, J.P.; Janssen, I.; Lang, J.J.; Sampasa-Kanyinga, H. Economic burden of excessive sedentary behaviour in Canada. Can. J. Public Health 2023, 114, 165–174. [Google Scholar] [CrossRef]
- Gupta, C.C.; Vincent, G.E.; Coates, A.M.; Khalesi, S.; Irwin, C.; Dorrian, J.; Ferguson, S.A. A Time to Rest, a Time to Dine: Sleep, Time-Restricted Eating, and Cardiometabolic Health. Nutrients 2022, 14, 420. [Google Scholar] [CrossRef]
- Lyzwinski, L.N.; Elgendi, M.; Menon, C. Conversational Agents and Avatars for Cardiometabolic Risk Factors and Lifestyle-Related Behaviors: Scoping Review. JMIR Mhealth Uhealth 2023, 11, e39649. [Google Scholar] [CrossRef]
- Aguas-Ayesa, M.; Yárnoz-Esquiroz, P.; Olazarán, L.; Perdomo, C.M.; García-Goñi, M.; Andrada, P.; Escalada, J.; Silva, C.; Marcos, A.; Frühbeck, G. Evaluation of Dietary and Alcohol Drinking Patterns in Patients with Excess Body Weight in a Spanish Cohort: Impact on Cardiometabolic Risk Factors. Nutrients 2023, 15, 4824. [Google Scholar] [CrossRef]
- Kitano, N.; Kai, Y.; Jindo, T.; Fujii, Y.; Tsunoda, K.; Arao, T. Association of domain-specific physical activity and sedentary behavior with cardiometabolic health among office workers. Scand. J. Med. Sci. Sports 2022, 32, 1224–1235. [Google Scholar] [CrossRef]
- Sang, C.J., 3rd; Song, X.; de Visser, R.S.F.; Krallman, R.; Montgomery, D.; Pai, C.W.; Kline-Rogers, E.; DuRussel-Weston, J.; Eagle, K.A.; Jackson, E.A. Lifestyle Behaviors and Cardiometabolic Health in Middle-School Children. Child. Obes. 2022, 18, 361–368. [Google Scholar] [CrossRef]
- Lancellotti, P. Focus on cardiometabolic risk factors. Acta Cardiol. 2023, 78, 515–518. [Google Scholar] [CrossRef]
- Ganguli, D.; Das, N.; Saha, I.; Sanapala, K.R.; Chaudhuri, D.; Ghosh, S.; Dey, S. Association between inflammatory markers and cardiovascular risk factors in women from Kolkata, W.B., India. Arq. Bras. Cardiol. 2011, 96, 38–46, (In English, In Portuguese, In Spanish). [Google Scholar] [CrossRef]
- Lowe, G.D.; Pepys, M.B. C-reactive protein and cardiovascular disease: Weighing the evidence. Curr. Atheroscler. Rep. 2006, 8, 421–428. [Google Scholar] [CrossRef]
- Bermudez, E.A.; Rifai, N.; Buring, J.; Manson, J.E.; Ridker, P.M. Interrelationships among circulating interleukin-6, C-reactive protein, and traditional cardiovascular risk factors in women. Arter. Arterioscler. Thromb. Vasc. Biol. 2002, 22, 1668–1673. [Google Scholar] [CrossRef]
- Ramírez Alvarado, M.M.; Sánchez Roitz, C. Relación entre los niveles séricos de la proteína C reactiva y medidas antropométricas; una revisión sistemática de los estudios realizados en Suramérica [Relation of serum levels of C-reactive protein to anthropometric meaurements; a sustematic review of studies in South America]. Nutr. Hosp. 2012, 27, 971–977. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Yoshida, T.; Kaneshi, T.; Shimabukuro, T.; Sunagawa, M.; Ohta, T. Serum C-reactive protein and its relation to cardiovascular risk factors and adipocytokines in Japanese children. J. Clin. Endocrinol. Metab. 2006, 91, 2133–2137. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.H.; He, Y.; Xu, W.D.; Zhao, Z.X.; Liu, M.; Luo, X.; He, C.S.; Chen, J. Carotid intima-media thickness in patients with hyperuricemia: A systematic review and meta-analysis. Aging Clin. Exp. Res. 2021, 33, 2967–2977. [Google Scholar] [CrossRef] [PubMed]
- Ma, M.; Wang, L.; Huang, W.; Zhong, X.; Li, L.; Wang, H.; Peng, B.; Mao, M. Meta-analysis of the correlation between serum uric acid level and carotid intima-media thickness. PLoS ONE 2021, 16, e0246416. [Google Scholar] [CrossRef] [PubMed]
- Martos, R.; Valle, M.; Morales, R.; Cañete, R.; Gavilan, M.I.; Sánchez-Margalet, V. Hyperhomocysteinemia correlates with insulin resistance and low-grade systemic inflammation in obese prepubertal children. Metabolism 2006, 55, 72–77. [Google Scholar] [CrossRef]
- De Pergola, G.; Pannacciulli, N.; Zamboni, M.; Minenna, A.; Brocco, G.; Sciaraffia, M.; Giorgino, R. Homocysteine plasma levels are independently associated with insulin resistance in normal weight, overweight and obese pre-menopausal women. Diabetes Nutr. Metab. 2001, 14, 253–258. [Google Scholar]
- Dipietro, L.; Zhang, Y.; Mavredes, M.; Simmens, S.J.; Whiteley, J.A.; Hayman, L.L.; Faro, J.; Malin, S.K.; Winston, G.; Napolitano, M.A. Physical Activity and Cardiometabolic Risk Factor Clustering in Young Adults with Obesity. Med. Sci. Sports Exerc. 2020, 52, 1050–1056. [Google Scholar] [CrossRef]
- The Lancet Child Adolescent Health. Metabolism and risk. Lancet Child. Adolesc. Health 2022, 6, 137. [Google Scholar] [CrossRef]
- Singleton, C.M.H.; Brar, S.; Robertson, N.; DiTommaso, L.; Fuchs, G.J., 3rd; Schadler, A.; Radulescu, A.; Attia, S.L. Cardiometabolic risk factors in South American children: A systematic review and meta-analysis. PLoS ONE 2023, 18, e0293865. [Google Scholar] [CrossRef]
- Nicolucci, A.; Maffeis, C. The adolescent with obesity: What perspectives for treatment? Ital. J. Pediatr. 2022, 48, 9. [Google Scholar] [CrossRef]
- Celada Roldana, C.; López Díez, J.; Cerezuela, M.A.; Rider, F.; Tárraga Marcos, A.; Tárraga López, P.J.; López González, A.A.; Ramírez Manent, J.I. Cardiovascular effects of a nutritional educational intervention in diabetic patients with poor control. Acad. J. Health Sci. 2023, 38, 57–65. [Google Scholar] [CrossRef]
- Laffond, A.; Rivera-Picón, C.; Rodríguez-Muñoz, P.M.; Juárez-Vela, R.; Ruiz de Viñaspre-Hernández, R.; Navas-Echazarreta, N.; Sánchez-González, J.L. Mediterranean Diet for Primary and Secondary Prevention of Cardiovascular Disease and Mortality: An Updated Systematic Review. Nutrients 2023, 15, 3356. [Google Scholar] [CrossRef]
- Delgado-Lista, J.; Alcala-Diaz, J.F.; Torres-Peña, J.D.; Quintana-Navarro, G.M.; Fuentes, F.; Garcia-Rios, A.; Ortiz-Morales, A.M.; Gonzalez-Requero, A.I.; Perez-Caballero, A.I.; Lopez-Miranda, J.; et al. Long-term secondary prevention of cardiovascular disease with a Mediterranean diet and a low-fat diet (CORDIOPREV): A randomised controlled trial. Lancet 2022, 399, 1876–1885. [Google Scholar] [CrossRef] [PubMed]
- Ramirez Manent, J.I.; Belmonte Lomas, S.; Tárraga Marcos, L.; López González, A.A.; Gordito Soler, M.; Tárraga López, P.J. Analysis of the efficacy of the main dietary patterns in reducing cardiovascular risk. Acad. J. Health Sci. 2023, 38, 153–170. [Google Scholar] [CrossRef]
- Stewart, A.; Marfell-Jones, M.; Olds, T.; Ridder, H. International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry–ISAK: Lower Hutt, New Zealand, 2011. [Google Scholar]
- Physical status: The use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ. Tech. Rep. Ser. 1995, 854, 1–452. [Google Scholar]
- NHLBI Obesity Education Initiative. The Practical Guide to the Identification, Evaluation and Treatment of Overweight and Obesity in Adults; NIH: Bethesda, MD, USA, 2000.
- Sastre-Alzamora, T.; Tomás-Gil, P.; Paublini, H.; Pallarés, L.; Ramírez-Manent, J.I.; López-González, A.A. Relationship between different scales of overweight and obesity and heart age values in 139634 spanish workers. Acad. J. Health Sci. 2023, 38, 137–144. [Google Scholar] [CrossRef]
- Allain, C.C.; Poon, L.S.; Chan, C.S.; Richmond, W.; Fu, P.C. Enzymatic determination of total serum cholesterol. Clin. Chem. 1974, 20, 470–475. [Google Scholar] [CrossRef] [PubMed]
- Roeschlau, P.; Bernt, E.; Gruber, W. Enzymatic determination of total cholesterol in serum. Z. Klin. Chem. Klin. Biochem. 1974, 12, 226. [Google Scholar]
- Mestre Font, M.; Busquets-Cortés, C.; Ramírez-Manent, J.I.; Tomás-Gil, P.; Paublini, H.; López-González, Á.A. Influence of Sociodemographic Variables and Healthy Habits on the Values of Insulin Resistance Indicators in 386,924 Spanish Workers. Nutrients 2023, 15, 5122. [Google Scholar] [CrossRef]
- Han, Y.; Zhou, Z.; Zhang, Y.; Zhao, G.; Xu, B. The Association of Surrogates of Insulin Resistance with Hyperuricemia among Middle-Aged and Older Individuals: A Population-Based Nationwide Cohort Study. Nutrients 2023, 15, 3139. [Google Scholar] [CrossRef]
- Seo, M.W.; Cho, W.; Kim, J.Y. The single point insulin sensitivity estimator (SPISE) index as a predictor of metabolic syndrome in Korean adults. Obes. Res. Clin. Pract. 2023, 17, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Shao, Q.; Li, J.; Wu, Y.; Liu, X.; Wang, N.; Jiang, Y.; Zhao, Q.; Zhao, G. Enhanced Predictive Value of Lipid Accumulation Product for Identifying Metabolic Syndrome in the General Population of China. Nutrients 2023, 15, 3168. [Google Scholar] [CrossRef] [PubMed]
- Jian, J.Z.; Tzeng, I.S.; Hsieh, C.F.; Huang, H.L.; Chen, C.L.; Liu, K.L. Validation of the Framingham General Cardiovascular Risk Score and Pooled Cohort Equations in a Community-Based Population: A Prospective Cohort Study Analysis 2006–2017. Acta Cardiol Sin. 2023, 39, 879–887. [Google Scholar] [CrossRef] [PubMed]
- Andersen, C.; Sloan, A.; Dupree, L.; Walker, B. Younger Relative Metabolic Age Is Associated with a More Favorable Body Composition and Plant-based Dietary Pattern (P21-038-19). Curr. Dev. Nutr. 2019, 1, 3130978. [Google Scholar] [CrossRef]
- Ramírez-Manent, J.I.; Tomás-Gil, P.; Coll Villalonga, J.L.; Marti-Lliteras, P.; López-González, A.A.; Paublini, H. Association between atherogenic dyslipidemia and lipid triad with cardiovascular risk scales in 418.343 Spanish workers. Acad. J. Health Sci. 2024, 39, 9–15. [Google Scholar] [CrossRef]
- López González, Á.A.; Rivero Ledo, Y.I.; Vicente Herrero, M.T.; Gil Llinás, M.; Tomás Salvá, M.; Riutord Fe, B. Índices aterogénicos en trabajadores de diferentes sectores laborales del área Mediterránea Española [Atherogenic indices in workers of different occupational sectors of the Spanish Mediterranean area]. Clin. Investig. Arterioscler. 2015, 27, 118–128. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Manent, J.I.; Jover, A.M.; Martinez, C.S.; Tomás-Gil, P.; Martí-Lliteras, P.; López-González, Á.A. Waist Circumference Is an Essential Factor in Predicting Insulin Resistance and Early Detection of Metabolic Syndrome in Adults. Nutrients 2023, 15, 257. [Google Scholar] [CrossRef] [PubMed]
- Riutord-Sbert, P.; Riutord-Fe, B.; Riutord-Fe, N.; Arroyo-Bote, S.; López González, A.A.; Ramírez-Manent, J.I. Influence of physical activity and mediterranean diet on the values of different scales of overweight and obesity. Acad. J. Health Sci. 2022, 37, 21–28. [Google Scholar] [CrossRef]
- Estilo de Vida Saludable. Available online: https://estilosdevidasaludable.sanidad.gob.es/ (accessed on 7 February 2024).
- Lugones-Sanchez, C.; Recio-Rodriguez, J.I.; Agudo-Conde, C.; Repiso-Gento, I.G.; Adalia, E.; Ramirez-Manent, J.I.; Sanchez-Calavera, M.A.; Rodriguez-Sanchez, E.; Gomez-Marcos, M.A.; Garcia-Ortiz, L.; et al. Long-term Effectiveness of a Smartphone App Combined with a Smart Band on Weight Loss, Physical Activity, and Caloric Intake in a Population With Overweight and Obesity (Evident 3 Study): Randomized Controlled Trial. J. Med. Internet Res. 2022, 24, e30416. [Google Scholar] [CrossRef]
- Wang, Y.; Min, J.; Khuri, J.; Xue, H.; Xie, B.; Kaminsky, L.A.; Cheskin, L.J. Effectiveness of Mobile Health Interventions on Diabetes and Obesity Treatment and Management: Systematic Review of Systematic Reviews. JMIR Mhealth Uhealth 2020, 8, e15400. [Google Scholar] [CrossRef]
- Burke, L.E.; Sereika, S.M.; Bizhanova, Z.; Parmanto, B.; Kariuki, J.; Cheng, J.; Beatrice, B.; Cedillo, M.; Pulantara, I.W.; Conroy, M.B.; et al. The Effect of Tailored, Daily, Smartphone Feedback to Lifestyle Self-Monitoring on Weight Loss at 12 Months: The SMARTER Randomized Clinical Trial. J. Med. Internet Res. 2022, 24, e38243. [Google Scholar] [CrossRef]
- Spring, B.; Pellegrini, C.; McFadden, H.G.; Pfammatter, A.F.; Stump, T.K.; Siddique, J.; King, A.C.; Hedeker, D. Multicomponent mHealth Intervention for Large, Sustained Change in Multiple Diet and Activity Risk Behaviors: The Make Better Choices 2 Randomized Controlled Trial. J. Med. Internet Res. 2018, 20, e10528. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística (Spain). Available online: https://www.ine.es/ss/Satellite?L=es_ES&c=INESeccion_C&cid=1259944484459&p=1254735110672&pagename=ProductosYServcios%2FPYSLayout¶m1=PYSDetalleFichaIndicador¶m3=1259937499084#:~:text=Las%20cifras%20definitivas%20de%20la,3%20a%C3%B1os%20para%20los%20hombres (accessed on 12 February 2024).
- Modesti, P.A.; Jarraya, F.; Mascherini, G.; Perticone, F. Cardiometabolic risk prevention strategies: The importance of sharing experiences between Mediterranean countries. Intern. Emerg. Med. 2020, 15, 543–548. [Google Scholar] [CrossRef]
- Weihe, P.; Weihrauch-Blüher, S. Metabolic Syndrome in Children and Adolescents: Diagnostic Criteria, Therapeutic Options and Perspectives. Curr. Obes. Rep. 2019, 8, 472–479. [Google Scholar] [CrossRef]
- Lopez Lucas, M.J.; Barja, S.; Villarroel Del Pino, L.; Arnaiz, P.; Mardones, F. Riesgo cardiometabólico en niños con obesidad grave [Cardiometabolic risk in children with severe obesity]. Nutr. Hosp. 2022, 39, 290–297. (In Spanish) [Google Scholar] [CrossRef]
- Noubiap, J.J.; Nansseu, J.R.; Lontchi-Yimagou, E.; Nkeck, J.R.; Nyaga, U.F.; Ngouo, A.T.; Tounouga, D.N.; Tianyi, F.L.; Foka, A.J.; Bigna, J.J.; et al. Global, regional, and country estimates of metabolic syndrome burden in children and adolescents in 2020: A systematic review and modelling analysis. Lancet Child Adolesc Health 2022, 6, 158–170. [Google Scholar] [CrossRef]
- Badimon, L.; Chagas, P.; Chiva-Blanch, G. Diet and Cardiovascular Disease: Effects of Foods and Nutrients in Classical and Emerging Cardiovascular Risk Factors. Curr. Med. Chem. 2019, 26, 3639–3651. [Google Scholar] [CrossRef]
- Diab, A.; Dastmalchi, L.N.; Gulati, M.; Michos, E.D. A Heart-Healthy Diet for Cardiovascular Disease Prevention: Where Are We Now? Vasc. Health Risk Manag. 2023, 19, 237–253. [Google Scholar] [CrossRef]
- Celada Roldana, C.; López Díez, J.; Rider, F.; Tárraga Marcos, A.; Tárraga Marcos, M.L.; Tárraga López, P.J.; Ramírez Gallegos, I.; Marina Arroyo, M.; Ramírez Manent, J.I.; López González, A.A. Impact of adherence to the Mediterranean diet on health-related quality of life in poorly controlled diabetics. Acad. J. Health Sci. 2024, 39, 103–112. [Google Scholar] [CrossRef]
- Calvo-Malvar, M.; Benítez-Estévez, A.J.; Sánchez-Castro, J.; Leis, R.; Gude, F. Effects of a Community-Based Behavioral Intervention with a Traditional Atlantic Diet on Cardiometabolic Risk Markers: A Cluster Randomized Controlled Trial (“The GALIAT Study”). Nutrients 2021, 13, 1211. [Google Scholar] [CrossRef]
- López-González, L.; Becerra-Tomás, N.; Babio, N.; Martínez-González, M.Á.; Nishi, S.K.; Corella, D.; Goday, A.; Romaguera, D.; Vioque, J.; Alonso-Gómez, M.; et al. One-year changes in fruit and vegetable variety intake and cardiometabolic risk factors changes in a middle-aged Mediterranean population at high cardiovascular risk. Eur. J. Clin. Nutr. 2022, 76, 1393–1402. [Google Scholar] [CrossRef]
- Filippou, C.; Tatakis, F.; Polyzos, D.; Manta, E.; Thomopoulos, C.; Nihoyannopoulos, P.; Tousoulis, D.; Tsioufis, K. Overview of salt restriction in the Dietary Approaches to Stop Hypertension (DASH) and the Mediterranean diet for blood pressure reduction. Rev. Cardiovasc. Med. 2022, 23, 36. [Google Scholar] [CrossRef]
- Filippou, C.; Thomopoulos, C.; Konstantinidis, D.; Siafi, E.; Tatakis, F.; Manta, E.; Drogkaris, S.; Polyzos, D.; Kyriazopoulos, K.; Grigoriou, K.; et al. DASH vs. Mediterranean diet on a salt restriction background in adults with high normal blood pressure or grade 1 hypertension: A randomized controlled trial. Clin. Nutr. 2023, 42, 1807–1816. [Google Scholar] [CrossRef]
- Jennings, A.; Berendsen, A.M.; de Groot, L.C.P.G.M.; Feskens, E.J.M.; Brzozowska, A.; Sicinska, E.; Pietruszka, B.; Meunier, N.; Caumon, E.; Cassidy, A.; et al. Mediterranean-Style Diet Improves Systolic Blood Pressure and Arterial Stiffness in Older Adults. Hypertension 2019, 73, 578–586. [Google Scholar] [CrossRef]
- Antoniazzi, L.; Arroyo-Olivares, R.; Bittencourt, M.S.; Tada, M.T.; Lima, I.; Jannes, C.E.; Krieger, J.E.; Pereira, A.C.; Quintana-Navarro, G.; Santos, R.D.; et al. Adherence to a Mediterranean diet, dyslipidemia and inflammation in familial hypercholesterolemia. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2014–2022. [Google Scholar] [CrossRef]
- Meslier, V.; Laiola, M.; Roager, H.M.; De Filippis, F.; Roume, H.; Quinquis, B.; Giacco, R.; Mennella, I.; Ferracane, R.; Ercolini, D.; et al. Mediterranean diet intervention in overweight and obese subjects lowers plasma cholesterol and causes changes in the gut microbiome and metabolome independently of energy intake. Gut 2020, 69, 1258–1268. [Google Scholar] [CrossRef]
- Ivan, C.R.; Messina, A.; Cibelli, G.; Messina, G.; Polito, R.; Losavio, F.; Torre, E.; Monda, V.; Monda, M.; Defeudis, G.; et al. Italian Ketogenic Mediterranean Diet in Overweight and Obese Patients with Prediabetes or Type 2 Diabetes. Nutrients 2022, 14, 4361. [Google Scholar] [CrossRef]
- Gioxari, A.; Grammatikopoulou, M.G.; Katsarou, C.; Panagiotakos, D.B.; Toutouza, M.; Kavouras, S.A.; Sidossis, L.S.; Maraki, M.I. A Modified Mediterranean Diet Improves Fasting and Postprandial Glucoregulation in Adults with Overweight and Obesity: A Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 15347. [Google Scholar] [CrossRef]
- Di Rosa, C.; Lattanzi, G.; Spiezia, C.; Imperia, E.; Piccirilli, S.; Beato, I.; Gaspa, G.; Micheli, V.; De Joannon, F.; Khazrai, Y.M.; et al. Mediterranean Diet versus Very Low-Calorie Ketogenic Diet: Effects of Reaching 5% Body Weight Loss on Body Composition in Subjects with Overweight and with Obesity-A Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 13040. [Google Scholar] [CrossRef]
- López-Gil, J.F.; García-Hermoso, A.; Sotos-Prieto, M.; Cavero-Redondo, I.; Martínez-Vizcaíno, V.; Kales, S.N. Mediterranean Diet-Based Interventions to Improve Anthropometric and Obesity Indicators in Children and Adolescents: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. Adv. Nutr. 2023, 14, 858–869. [Google Scholar] [CrossRef]
- Dayi, T.; Ozgoren, M. Effects of the Mediterranean diet on the components of metabolic syndrome. J. Prev. Med. Hyg. 2022, 63 (Suppl. 3), E56–E64. [Google Scholar] [CrossRef]
- Rubín-García, M.; Vitelli-Storelli, F.; Toledo, E.; Castro-Barquero, S.; Tresserra-Rimbau, A.; Martínez-González, M.Á.; Salas-Salvadó, J.; Corella, D.; Hernáez, Á.; Martín-Sánchez, V.; et al. Polyphenol intake and cardiovascular risk in the PREDIMED-Plus trial. A Comp. Differ. Risk Equ. Rev. Esp. Cardiol. Engl. Ed. 2022, 75, 401–411, (In English, In Spanish). [Google Scholar] [CrossRef]
- Vásquez-Alvarez, S.; Bustamante-Villagomez, S.K.; Vazquez-Marroquin, G.; Porchia, L.M.; Pérez-Fuentes, R.; Torres-Rasgado, E.; Herrera-Fomperosa, O.; Montes-Arana, I.; Gonzalez-Mejia, M.E. Metabolic Age, an Index Based on Basal Metabolic Rate, Can Predict Individuals That are High Risk of Developing Metabolic Syndrome. High. Blood Press. Cardiovasc. Prev. 2021, 28, 263–270. [Google Scholar] [CrossRef]
- Elguezabal-Rodelo, R.; Ochoa-Précoma, R.; Vazquez-Marroquin, G.; Porchia, L.M.; Montes-Arana, I.; Torres-Rasgado, E.; Méndez-Fernández, E.; Pérez-Fuentes, R.; Gonzalez-Mejia, M.E. Metabolic age correlates better than chronological age with waist-to-height ratio, a cardiovascular risk index. Med. Clin. 2021, 157, 409–417, (In English, In Spanish). [Google Scholar] [CrossRef]
- Vidal-Ostos, F.; Ramos-Lopez, O.; Blaak, E.E.; Astrup, A.; Martinez, J.A. The triglyceride-glucose index as an adiposity marker and a predictor of fat loss induced by a low-calorie diet. Eur. J. Clin. Investig. 2022, 52, e13674. [Google Scholar] [CrossRef]
- Rohner, M.; Heiz, R.; Feldhaus, S.; Bornstein, S.R. Hepatic-Metabolite-Based Intermittent Fasting Enables a Sustained Reduction in Insulin Resistance in Type 2 Diabetes and Metabolic Syndrome. Horm. Metab. Res. 2021, 53, 529–540. [Google Scholar] [CrossRef]
- Gomes, J.M.G.; Costa, J.D.A.; Alfenas, R.C.G. Effect of increased calcium consumption from fat-free milk in an energy-restricted diet on the metabolic syndrome and cardiometabolic outcomes in adults with type 2 diabetes mellitus: A randomised cross-over clinical trial. Br. J. Nutr. 2018, 119, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Amini, M.R.; Shahinfar, H.; Babaei, N.; Davarzani, S.; Ebaditabar, M.; Djafarian, K.; Clark, C.C.T.; Shab-Bidar, S. Association of Dietary Patterns with Visceral Adiposity, Lipid Accumulation Product, and Triglyceride-Glucose Index in Iranian Adults. Clin. Nutr. Res. 2020, 9, 145–156. [Google Scholar] [CrossRef]
- Mazidi, M.; Gao, H.K.; Kengne, A.P. Lipid accumulation product and visceral adiposity index are associated with dietary patterns in adult Americans. Medicine 2018, 97, e0322. [Google Scholar] [CrossRef]
- Shahavandi, M.; Djafari, F.; Shahinfar, H.; Davarzani, S.; Babaei, N.; Ebaditabar, M.; Djafarian, K.; Clark, C.C.T.; Shab-Bidar, S. The association of plant-based dietary patterns with visceral adiposity, lipid accumulation product, and triglyceride-glucose index in Iranian adults. Complement. Ther. Med. 2020, 53, 102531. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Salas-Salvadó, J.; Estruch, R.; Corella, D.; Fitó, M.; Ros, E.; PREDIMED Investigators. Benefits of the Mediterranean Diet: Insights from the PREDIMED Study. Prog. Cardiovasc. Dis. 2015, 58, 50–60. [Google Scholar] [CrossRef]
- Guasch-Ferré, M.; Hu, F.B.; Martínez-González, M.A.; Fitó, M.; Bulló, M.; Estruch, R.; Ros, E.; Corella, D.; Recondo, J.; Salas-Salvadó, J.; et al. Olive oil intake and risk of cardiovascular disease and mortality in the PREDIMED Study. BMC Med. 2014, 12, 78. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; Gea, A.; Ruiz-Canela, M. The Mediterranean Diet and Cardiovascular Health. Circ. Res. 2019, 124, 779–798. [Google Scholar] [CrossRef]
- Gallardo-Alfaro, L.; Bibiloni, M.D.M.; Mascaró, C.M.; Montemayor, S.; Ruiz-Canela, M.; Salas-Salvadó, J.; Corella, D.; Fitó, M.; Romaguera, D.; Tur, J.A.; et al. Leisure-Time Physical Activity, Sedentary Behaviour and Diet Quality are Associated with Metabolic Syndrome Severity: The PREDIMED-Plus Study. Nutrients 2020, 12, 1013. [Google Scholar] [CrossRef]
- Glenn, A.J.; Hernández-Alonso, P.; Kendall, C.W.C.; Martínez-González, M.Á.; Corella, D.; Fitó, M.; Martínez, J.A.; Alonso-Gómez, Á.M.; Wärnberg, J.; Salas-Salvadó, J.; et al. Longitudinal changes in adherence to the portfolio and DASH dietary patterns and cardiometabolic risk factors in the PREDIMED-Plus study. Clin. Nutr. 2021, 40, 2825–2836. [Google Scholar] [CrossRef]
- Nabhani, Z.; Clark, C.C.T.; Goudarzi, N.; Hariri Far, A.; Razmpoosh, E. The effect of synbiotic supplementation on atherogenic indices, hs-CRP, and malondialdehyde, as major CVD-related parameters, in women with gestational diabetes mellitus: A secondary data-analysis of a randomized double-blind, placebo-controlled study. Diabetol. Metab. Syndr. 2022, 14, 87. [Google Scholar] [CrossRef]
- Mahdavi-Roshan, M.; Salari, A.; Vakilpour, A.; Savar Rakhsh, A.; Ghorbani, Z. Rice bran oil could favorably ameliorate atherogenicity and insulin resistance indices among men with coronary artery disease: Post hoc analysis of a randomized controlled trial. Lipids Health Dis. 2021, 20, 153. [Google Scholar] [CrossRef]
- Ramírez-Manent, J.I.; Tomás-Gil, P.; Martí-Lliteras, P.; Coll Villalonga, J.L.; Martínez-Almoyna Rifá, E.; López-González, Á.A. Dietary Intervention on Overweight and Obesity after Confinement by COVID-19. Nutrients 2023, 15, 912. [Google Scholar] [CrossRef]
- Wade, A.T.; Davis, C.R.; Dyer, K.A.; Hodgson, J.M.; Woodman, R.J.; Murphy, K.J. A Mediterranean diet supplemented with dairy foods improves markers of cardiovascular risk: Results from the MedDairy randomized controlled trial. Am. J. Clin. Nutr. 2018, 108, 1166–1182. [Google Scholar] [CrossRef]
- Godos, J.; Zappalà, G.; Bernardini, S.; Giambini, I.; Bes-Rastrollo, M.; Martinez-Gonzalez, M. Adherence to the Mediterranean diet is inversely associated with metabolic syndrome occurrence: A meta-analysis of observational studies. Int. J. Food Sci. Nutr. 2017, 68, 138–148. [Google Scholar] [CrossRef]
- Phillips, C.M.; Harrington, J.M.; Perry, I.J. Relationship between dietary quality, determined by DASH score, and cardiometabolic health biomarkers: A cross-sectional analysis in adults. Clin. Nutr. 2019, 38, 1620–1628. [Google Scholar] [CrossRef]
- Liu, Y.S.; Wu, Q.J.; Xia, Y.; Zhang, J.Y.; Jiang, Y.T.; Chang, Q.; Zhao, Y.H. Carbohydrate intake and risk of metabolic syndrome: A dose-response meta-analysis of observational studies. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 1288–1298. [Google Scholar] [CrossRef]
- Campos-Nonato, I.; Hernandez, L.; Barquera, S. Effect of a High-Protein Diet versus Standard-Protein Diet on Weight Loss and Biomarkers of Metabolic Syndrome: A Randomized Clinical Trial. Obes. Facts. 2017, 10, 238–251. [Google Scholar] [CrossRef]
- Ramezani-Jolfaie, N.; Mohammadi, M.; Salehi-Abargouei, A. The effect of healthy Nordic diet on cardio-metabolic markers: A systematic review and meta-analysis of randomized controlled clinical trials. Eur. J. Nutr. 2019, 58, 2159–2174. [Google Scholar] [CrossRef]
- Thomas, M.S.; Calle, M.; Fernandez, M.L. Healthy plant-based diets improve dyslipidemias, insulin resistance, and inflammation in metabolic syndrome. A narrative review. Adv. Nutr. 2023, 14, 44–54. [Google Scholar] [CrossRef]
- Castro-Barquero, S.; Ruiz-León, A.M.; Sierra-Pérez, M.; Estruch, R.; Casas, R. Dietary Strategies for Metabolic Syndrome: A Comprehensive Review. Nutrients 2020, 12, 2983. [Google Scholar] [CrossRef]
- Finicelli, M.; Di Salle, A.; Galderisi, U.; Peluso, G. The Mediterranean Diet: An Update of the Clinical Trials. Nutrients 2022, 14, 2956. [Google Scholar] [CrossRef]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Murray, C.J.L.; et al. Food in the Anthropocene: The EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492, Erratum in: Lancet 2019, 393, 530. Erratum in: Lancet 2019, 393, 2590. Erratum in: Lancet 2020, 395, 338. Erratum in: Lancet 2020, 396, e56. [Google Scholar] [CrossRef]
- Afshin, A.; Babalola, D.; Mclean, M.; Yu, Z.; Ma, W.; Chen, C.Y.; Arabi, M.; Mozaffarian, D. Information Technology and Lifestyle: A Systematic Evaluation of Internet and Mobile Interventions for Improving Diet, Physical Activity, Obesity, Tobacco, and Alcohol Use. J. Am. Heart Assoc. 2016, 5, e003058. [Google Scholar] [CrossRef]
- Lavikainen, P.; Mattila, E.; Absetz, P.; Harjumaa, M.; Lindström, J.; Järvelä-Reijonen, E.; Aittola, K.; Männikkö, R.; Tilles-Tirkkonen, T.; Martikainen, J.; et al. Digitally Supported Lifestyle Intervention to Prevent Type 2 Diabetes Through Healthy Habits: Secondary Analysis of Long-Term User Engagement Trajectories in a Randomized Controlled Trial. J. Med. Internet Res. 2022, 24, e31530. [Google Scholar] [CrossRef]
- Hincapié Tabares, M.; Pérez Carrillo, V.; Donado Gómez, J.H. Causes of patient loss during clinical trials: A meta-epidemiological study. Salud Barranquilla 2019, 35, 57–71. Available online: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0120-55522019000100057&lng=en&nrm=iso. (accessed on 10 March 2024). ISSN 0120-5552. [CrossRef]
- LaValley, G.; Storer, A.; Szalai, H.; Farah, M.; Pack, Q.R. A Motivational Telephone Intervention to Reduce Early Dropouts in Cardiac Rehabilitation: A Feasibility Pilot Study. J. Cardiopulm. Rehabil. Prev. 2019, 39, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Marciniak, T.A.; Cherepanov, V.; Golukhova, E.; Kim, M.H.; Serebruany, V. Drug Discontinuation and Follow-up Rates in Oral Antithrombotic Trials. JAMA Intern. Med. 2016, 176, 257–259. [Google Scholar] [CrossRef]


{kind=link}
| Formula | Cut-Off | |
|---|---|---|
| BMI | Weight/Height2 | >30 kg/m2 obesity |
| WtHR | Waist/Height | >0.50 |
| WtHipR | Waist/Hip | 0.8 women; 0.95 men |
| TyG index | LN (triglycerides × glycaemia/2) | >8.5 |
| METS-IR | LN (2 × glycaemia + triglycerides) × BMI/LN(HDL-c) | >50 |
| SPISE | (=600 × HDL0.185/triglycerides0.2 × BMI1.338) | 6.14 |
| LAP | (waist (cm)-65) × triglyc (mMol) men; (waist (cm)-58) × triglyc (mMol) women | no cut-off |
| Atherogenic dyslipidaemia | high triglycerides + low HDL-c | |
| Lipid triad | Atherogenic dyslipidaemia + high LDL-c | |
| AI total cholesterol/HDL-c | Total cholesterol/HDL-c | >7 women; >9 men |
| AI LDL-c/HDL-c | LDL-c/HDL-c | >3 |
| AI triglycerides/HDL-c | Triglycerides/HDL-c | >3 |
| Men Pre (n = 4038) | Men Post (n = 4038) | Women Pre (n = 2996) | Women Post (n = 2996) | |||
|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | p-Value | Mean (SD) | Mean (SD) | p-Value | |
| Age | 47.1 (8.0) | 47.6 (8.1) | <0.001 | 45.4 (8.3) | 46.0 (8.3) | <0.001 |
| Weight | 87.1 (13.1) | 84.4 (13.0) | <0.001 | 78.2 (14.1) | 72.2 (12.2) | <0.001 |
| Waist | 100.8 (9.1) | 98.3 (9.6) | <0.001 | 104.3 (9.8) | 98.7 (11.1) | <0.001 |
| Hip | 109.6 (9.4) | 107.2 (9.7) | <0.001 | 114.8 (9.6) | 110.8 (10.3) | <0.001 |
| SBP | 138.2 (19.0) | 136.5 (18.8) | <0.001 | 130.2 (18.3) | 127.3 (18.0) | <0.001 |
| DBP | 83.5 (11.7) | 82.5 (11.8) | <0.001 | 80.1 (11.4) | 78.1 (11.1) | <0.001 |
| Total cholesterol | 206.4 (38.9) | 205.0 (39.4) | <0.001 | 204.8 (36.5) | 200.7 (35.6) | <0.001 |
| HDL-c | 49.3 (10.9) | 50.2 (10.8) | <0.001 | 57.5 (12.1) | 58.6 (12.3) | <0.001 |
| LDL-c | 128.4 (33.6) | 126.7 (34.1) | <0.001 | 126.1 (32.4) | 122.3 (31.4) | <0.001 |
| Triglycerides | 144.0 (95.7) | 138.6 (90.9) | <0.001 | 105.7 (57.7) | 99.3 (57.9) | <0.001 |
| Glycaemia | 97.1 (24.3) | 95.7 (23.4) | <0.001 | 93.2 (22.6) | 91.6 (19.5) | <0.001 |
| Men Pre (n = 4038) | Men Post (n = 4038) | Women Pre (n = 2996) | Women Post (n = 2996) | |||||
|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Difference | p-Value | Mean (SD) | Mean (SD) | Difference | p-Value | |
| Metabolic age | 14.4 (1.1) | 13.9 (1.7) | −3.9 | <0.001 | 12.9 (1.6) | 11.7 (2.1) | −9.0 | <0.001 |
| BMI | 28.9 (3.8) | 28.1 (3.8) | −2.8 | <0.001 | 29.8 (4.9) | 27.7 (4.4) | −7.0 | <0.001 |
| WtHR | 0.58 (0.05) | 0.57 (0.06) | −1.7 | <0.001 | 0.64 (0.07) | 0.61 (0.07) | −4.7 | <0.001 |
| WtHipR | 0.92 (0.06) | 0.91 (0.06) | −1.1 | 0.017 | 0.91 (0.07) | 0.89 (0.07) | −2.2 | <0.001 |
| % body fat | 34.6 (5.7) | 32.5 (6.5) | −6.1 | <0.001 | 44.6 (4.2) | 41.3 (5.1) | −7.4 | <0.001 |
| % visceral fat | 16.6 (5.4) | 15.0 (5.7) | −9.6 | <0.001 | 11.1 (4.0) | 9.6 (3.7) | −13.5 | <0.001 |
| ALLY heart age | 9.0 (8.6) | 8.5 (8.7) | −5.6 | <0.001 | 6.5 (10.1) | 4.9 (10.5) | −24.6 | <0.001 |
| Framingham relative risk | 1.7 (0.9) | 1.6 (0.9) | −5.9 | 0.028 | 1.4 (0.8) | 1.3 (0.8) | −7.1 | <0.001 |
| TyG index | 8.7 (0.6) | 8.6 (0.6) | −1.1 | <0.001 | 8.4 (0.5) | 8.3 (0.5) | −1.2 | <0.001 |
| METS-IR | 45.9 (8.2) | 44.2 (8.2) | −3.7 | <0.001 | 44.3 (9.2) | 40.6 (8.2) | −8.4 | <0.001 |
| SPISE | 5.4 (1.2) | 5.7 (1.3) | 5.6 | <0.001 | 5.7 (1.4) | 6.4 (1.5) | 12.3 | <0.001 |
| LAP | 58.9 (45.0) | 53.4 (42.3) | −9.3 | <0.001 | 49.3 (39.0) | 46.1 (38.0) | −6.5 | <0.001 |
| AI total cholesterol/HDL-c | 4.3 (1.1) | 4.2 (1.0) | −2.3 | 0.031 | 3.7 (0.9) | 3.5 (0.9) | −5.4 | <0.001 |
| AI LDL-c/HDL-c | 2.7 (0.8) | 2.6 (0.8) | −3.7 | 0.027 | 2.3 (0.7) | 2.2 (0.7) | −4.3 | <0.001 |
| AI triglycerides/HDL-c | 3.2 (2.5) | 3.0 (2.4) | −6.3 | <0.001 | 2.0 (1.5) | 1.8 (1.5) | −10.0 | <0.001 |
| Metabolic syndrome nº factors | 1.9 (1.2) | 1.7 (1.2) | −10.5 | <0.001 | 2.8 (1.0) | 2.5 (1.1) | −10.7 | <0.001 |
| Men Pre (n = 4038) | Men Post (n = 4038) | Women Pre (n = 2996) | Women Post (n = 2996) | |||||
|---|---|---|---|---|---|---|---|---|
| % | % | Difference | p-Value | % | % | Difference | p-Value | |
| Metabolic age ≥ 12 years | 68.2 | 53.3 | −21.8 | <0.001 | 16.02 | 9.8 | −38.5 | <0.001 |
| Hypertension | 47.9 | 43.5 | −9.2 | <0.001 | 30.7 | 24.6 | −19.9 | <0.001 |
| High Total cholesterol | 53.3 | 51.5 | −3.4 | <0.001 | 52.6 | 48.1 | −8.6 | <0.001 |
| High LDL-c | 46.5 | 44.5 | −4.3 | <0.001 | 42.7 | 37.6 | −11.9 | <0.001 |
| High Triglycerides | 34.3 | 31.5 | −8.2 | <0.001 | 16.2 | 13.2 | −18.5 | <0.001 |
| Glycaemia > 125 mg/dL | 7.8 | 7.3 | −6.4 | <0.001 | 5.0 | 3.6 | −28.0 | <0.001 |
| BMI obesity | 31.7 | 24.5 | −22.7 | <0.001 | 39.4 | 21.5 | −45.4 | <0.001 |
| High WtHR | 96.8 | 91.0 | −6.0 | <0.001 | 99.2 | 95.2 | −4.0 | <0.001 |
| High WtHipR | 96.8 | 92.3 | −4.6 | <0.001 | 95.9 | 91.7 | −4.4 | <0.001 |
| Very high % body fat | 100.0 | 87.3 | −12.7 | <0.001 | 100.0 | 82.9 | −17.1 | <0.001 |
| High ALLY heart age | 18.2 | 15.7 | −13.7 | <0.001 | 7.4 | 6.1 | −17.6 | <0.001 |
| Framingham relative risk | 30.9 | 28.7 | −7.1 | <0.001 | 9.6 | 8.9 | −7.3 | <0.001 |
| High TyG index | 39.1 | 35.7 | −8.7 | <0.001 | 24.2 | 19.6 | −19.0 | <0.001 |
| High METS-IR | 26.8 | 21.1 | −21.3 | <0.001 | 21.6 | 11.9 | −44.9 | <0.001 |
| High SPISE | 83.7 | 75.7 | −9.6 | <0.001 | 76.1 | 56.0 | −26.4 | <0.001 |
| High AI total cholesterol/HDL-c | 23.3 | 21.7 | −6.9 | <0.001 | 15.2 | 12.4 | −18.4 | <0.001 |
| High AI LDL-c/HDL-c | 32.7 | 31.6 | −3.4 | <0.001 | 16.3 | 12.7 | −22.1 | <0.001 |
| High AI triglycerides/HDL-c | 39.5 | 35.8 | −9.4 | <0.001 | 14.7 | 11.7 | −20.4 | <0.001 |
| Atherogenic dyslipidaemia | 10.1 | 8.3 | −17.8 | <0.001 | 12.7 | 9.7 | −23.6 | <0.001 |
| Lipid triad | 7.5 | 6.3 | −16.0 | <0.001 | 8.1 | 6.3 | −22.2 | <0.001 |
| Metabolic syndrome NCEP ATPIII | 27.5 | 22.5 | −18.2 | <0.001 | 23.7 | 20.5 | −13.5 | <0.001 |
| Metabolic syndrome IDF | 38.9 | 32.0 | −17.7 | <0.001 | 27.7 | 23.3 | −15.9 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramírez Gallegos, I.; Marina Arroyo, M.; López-González, Á.A.; Vicente-Herrero, M.T.; Vallejos, D.; Sastre-Alzamora, T.; Ramírez-Manent, J.I. The Effect of a Program to Improve Adherence to the Mediterranean Diet on Cardiometabolic Parameters in 7034 Spanish Workers. Nutrients 2024, 16, 1082. https://doi.org/10.3390/nu16071082
Ramírez Gallegos I, Marina Arroyo M, López-González ÁA, Vicente-Herrero MT, Vallejos D, Sastre-Alzamora T, Ramírez-Manent JI. The Effect of a Program to Improve Adherence to the Mediterranean Diet on Cardiometabolic Parameters in 7034 Spanish Workers. Nutrients. 2024; 16(7):1082. https://doi.org/10.3390/nu16071082
Chicago/Turabian StyleRamírez Gallegos, Ignacio, Marta Marina Arroyo, Ángel Arturo López-González, Maria Teófila Vicente-Herrero, Daniela Vallejos, Tomás Sastre-Alzamora, and José Ignacio Ramírez-Manent. 2024. "The Effect of a Program to Improve Adherence to the Mediterranean Diet on Cardiometabolic Parameters in 7034 Spanish Workers" Nutrients 16, no. 7: 1082. https://doi.org/10.3390/nu16071082
APA StyleRamírez Gallegos, I., Marina Arroyo, M., López-González, Á. A., Vicente-Herrero, M. T., Vallejos, D., Sastre-Alzamora, T., & Ramírez-Manent, J. I. (2024). The Effect of a Program to Improve Adherence to the Mediterranean Diet on Cardiometabolic Parameters in 7034 Spanish Workers. Nutrients, 16(7), 1082. https://doi.org/10.3390/nu16071082