
Clinical Impact of Supplementation with Pasteurized Donor Human Milk by High-Temperature Short-Time Method versus Holder Method in Extremely Low Birth Weight Infants: A Multicentre Randomized Controlled Trial

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
2.1.1. Sample Size Calculation
2.1.2. Study Protocol
Feeding Protocol and Growth Monitoring
Processing of Study DHM Batches
Randomization and Blinding
2.1.3. Study Outcomes
2.1.4. Data Collection
2.2. Statistical Analyses
3. Results
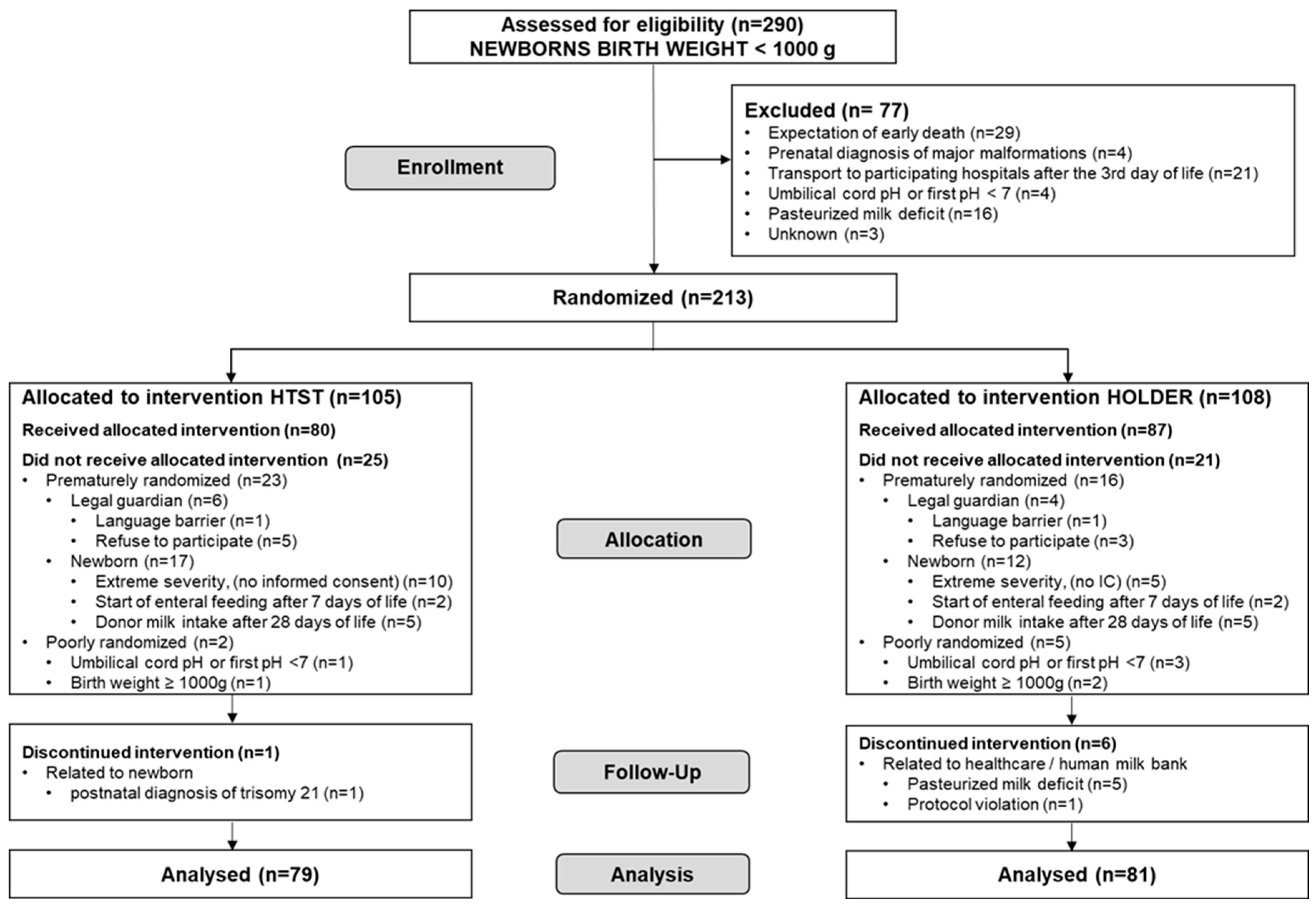
3.1. Study Population
3.2. Main Outcome
3.3. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Hornik, C.P.; Fort, P.; Clark, R.H.; Watt, K.; Benjamin, D.K.J.; Smith, P.B.; Manzoni, P.; Jacqz-Aigrain, E.; Kaguelidou, F.; Cohen-Wolkowiez, M. Early and late onset sepsis in very-low-birth-weight infants from a large group of neonatal intensive care units. Early Hum. Dev. 2012, 88 (Suppl. S2), S69–S74. [Google Scholar] [CrossRef] [PubMed]
- Coggins, S.A.; Glaser, K. Updates in Late-Onset Sepsis: Risk Assessment, Therapy, and Outcomes. Neoreviews 2022, 23, 738–755. [Google Scholar] [CrossRef]
- Razak, A.; Alhaidari, O.I.; Ahmed, J. Interventions for reducing late-onset sepsis in neonates: An umbrella review. J. Perinat. Med. 2023, 51, 403–422. [Google Scholar] [CrossRef] [PubMed]
- Stoll, B.J.; Hansen, N.I.; Adams-Chapman, I.; Fanaroff, A.A.; Hintz, S.R.; Vohr, B.; Higgins, R.D. Neurodevelopmental and growth impairment among extremely low-birth-weight infants with neonatal infection. JAMA 2004, 292, 2357–2365. [Google Scholar] [CrossRef]
- Johnson, T.J.; Patel, A.L.; Bigger, H.R.; Engstrom, J.L.; Meier, P.P. Economic benefits and costs of human milk feedings: A strategy to reduce the risk of prematurity-related morbidities in very-low-birth-weight infants. Adv. Nutr. 2014, 5, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Meier, P.P.; Engstrom, J.L.; Patel, A.L.; Jegier, B.J.; Bruns, N.E. Improving the use of human milk during and after the NICU stay. Clin. Perinatol. 2010, 37, 217–245. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.L.; Johnson, T.J.; Engstrom, J.L.; Fogg, L.F.; Jegier, B.J.; Bigger, H.R.; Meier, P.P. Impact of early human milk on sepsis and health-care costs in very low birth weight infants. J. Perinatol. 2013, 33, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Collado, M.C.; Cernada, M.; Neu, J.; Pérez-Martínez, G.; Gormaz, M.; Vento, M. Factors influencing gastrointestinal tract and microbiota immune interaction in preterm infants. Pediatr. Res. 2015, 77, 726–731. [Google Scholar] [CrossRef] [PubMed]
- Kan, B.; Razzaghian, H.R.; Lavoie, P.M. An Immunological Perspective on Neonatal Sepsis. Trends Mol. Med. 2016, 22, 290–302. [Google Scholar] [CrossRef]
- Lewis, E.D.; Richard, C.; Larsen, B.M.; Field, C.J. The Importance of Human Milk for Immunity in Preterm Infants. Clin. Perinatol. 2017, 44, 23–47. [Google Scholar] [CrossRef]
- Gregory, K.E.; Samuel, B.S.; Houghteling, P.; Shan, G.; Ausubel, F.M.; Sadreyev, R.I.; Walker, W.A. Influence of maternal breast milk ingestion on acquisition of the intestinal microbiome in preterm infants. Microbiome 2016, 4, 68. [Google Scholar] [CrossRef]
- Furman, L.; Taylor, G.; Minich, N.; Hack, M. The effect of maternal milk on neonatal morbidity of very low-birth-weight infants. Arch. Pediatr. Adolesc. Med. 2003, 157, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Schanler, R.J.; Shulman, R.J.; Lau, C. Feeding strategies for premature infants: Beneficial outcomes of feeding fortified human milk versus preterm formula. Pediatrics 1999, 103, 1150–1157. [Google Scholar] [CrossRef] [PubMed]
- Hylander, M.A.; Strobino, D.M.; Dhanireddy, R. Human milk feedings and infection among very low birth weight infants. Pediatrics 1998, 102, e38. [Google Scholar] [CrossRef]
- Miller, J.; Tonkin, E.; Damarell, R.A.; McPhee, A.J.; Suganuma, M.; Suganuma, H.; Middleton, P.F.; Makrides, M.; Collins, C.T. A Systematic Review and Meta-Analysis of Human Milk Feeding and Morbidity in Very Low Birth Weight Infants. Nutrients 2018, 10, 707. [Google Scholar] [CrossRef] [PubMed]
- Corpeleijn, W.E.; Kouwenhoven, S.M.P.; Paap, M.C.; van Vliet, I.; Scheerder, I.; Muizer, Y.; Helder, O.K.; van Goudoever, J.B.; Vermeulen, M.J. Intake of own mother’s milk during the first days of life is associated with decreased morbidity and mortality in very low birth weight infants during the first 60 days of life. Neonatology 2012, 102, 276–281. [Google Scholar] [CrossRef]
- WHO. WHO Recommendations for Care of the Preterm or Low-Birth-Weight Infant; World Health Organisation: Geneva, Switzerland, 2022; ISBN 9789240058262. [Google Scholar]
- AAP. Comittee on Nutrition; Section on Breastfeeding; Comittee on fetus and newbornborn Donor human milk for the high- risk infant: Preparation, safety, and usage options in the United States. Pediatrics 2017, 139, e20163440. [Google Scholar] [CrossRef]
- Arslanoglu, S.; Corpeleijn, W.; Moro, G.; Braegger, C.; Campoy, C.; Colomb, V.; Decsi, T.; Domellöf, M.; Fewtrell, M.; Hojsak, I.; et al. Donor human milk for preterm infants: Current evidence and research directions. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 535–542. [Google Scholar] [CrossRef]
- Meier, P.; Patel, A.; Esquerra-Zwiers, A. Donor Human Milk Update: Evidence, Mechanisms, and Priorities for Research and Practice. J. Pediatr. 2017, 180, 15–21. [Google Scholar] [CrossRef]
- Cossey, V.; Vanhole, C.; Eerdekens, A.; Rayyan, M.; Fieuws, S.; Schuermans, A. Pasteurization of mother’s own milk for preterm infants does not reduce the incidence of late-onset sepsis. Neonatology 2013, 103, 170–176. [Google Scholar] [CrossRef]
- Corpeleijn, W.E.; de Waard, M.; Christmann, V.; van Goudoever, J.B.; Jansen-van der Weide, M.C.; Kooi, E.M.W.; Koper, J.F.; Kouwenhoven, S.M.P.; Lafeber, H.N.; Mank, E.; et al. Effect of Donor Milk on Severe Infections and Mortality in Very Low-Birth-Weight Infants: The Early Nutrition Study Randomized Clinical Trial. JAMA Pediatr. 2016, 170, 654–661. [Google Scholar] [CrossRef] [PubMed]
- Peila, C.; Moro, G.; Bertino, E.; Cavallarin, L.; Giribaldi, M.; Giuliani, F.; Cresi, F.; Coscia, A. The Effect of Holder Pasteurization on Nutrients and Biologically-Active Components in Donor Human Milk: A Review. Nutrients 2016, 8, 477. [Google Scholar] [CrossRef] [PubMed]
- Moro, G.E.; Billeaud, C.; Rachel, B.; Calvo, J.; Cavallarin, L.; Christen, L.; Escuder-Vieco, D.; Gaya, A.; Lembo, D.; Wesolowska, A.; et al. Processing of Donor Human Milk: Update and Recommendations From the European Milk Bank Association (EMBA). Front. Pediatr. 2019, 7, 49. [Google Scholar] [CrossRef] [PubMed]
- Picaud, J.-C.; Buffin, R. Human Milk-Treatment and Quality of Banked Human Milk. Clin. Perinatol. 2017, 44, 95–119. [Google Scholar] [CrossRef] [PubMed]
- Czank, C.; Prime, D.K.; Hartmann, B.; Simmer, K.; Hartmann, P.E. Retention of the immunological proteins of pasteurized human milk in relation to pasteurizer design and practice. Pediatr. Res. 2009, 66, 374–379. [Google Scholar] [CrossRef] [PubMed]
- Baro, C.; Giribaldi, M.; Arslanoglu, S.; Giuffrida, M.G.; Dellavalle, G.; Conti, A.; Tonetto, P.; Biasini, A.; Coscia, A.; Fabris, C.; et al. Effect of two pasteurization methods on the protein content of human milk. Front. Biosci. 2011, 3, 818–829. [Google Scholar] [CrossRef]
- Wesolowska, A.; Sinkiewicz-Darol, E.; Barbarska, O.; Bernatowicz-Lojko, U.; Borszewska-Kornacka, M.K.; van Goudoever, J.B. Innovative Techniques of Processing Human Milk to Preserve Key Components. Nutrients 2019, 11, 1169. [Google Scholar] [CrossRef] [PubMed]
- Giribaldi, M.; Coscia, A.; Peila, C.; Antoniazzi, S.; Lamberti, C.; Ortoffi, M.; Moro, G.E.; Bertino, E.; Civera, T.; Cavallarin, L. Pasteurization of human milk by a benchtop High-Temperature Short-Time device. Innov. Food Sci. Emerg. Technol. 2016, 36, 228–233. [Google Scholar] [CrossRef]
- Dhar, J.; Fichtali, J.; Skura, B.; Nakai, S.; Davidson, A. Pasteurization Efficiency of a HTST System for Human Milk. J. Food Sci. 1996, 61, 569–573. [Google Scholar] [CrossRef]
- Escuder-Vieco, D.; Espinosa-Martos, I.; Rodríguez, J.M.; Corzo, N.; Montilla, A.; Siegfried, P.; Pallás-Alonso, C.R.; Fernández, L. High-Temperature Short-Time Pasteurization System for Donor Milk in a Human Milk Bank Setting. Front. Microbiol. 2018, 9, 926. [Google Scholar] [CrossRef]
- Escuder-Vieco, D.; Espinosa-Martos, I.; Rodríguez, J.M.; Fernández, L.; Pallás-Alonso, C.R. Effect of HTST and Holder Pasteurization on the Concentration of Immunoglobulins, Growth Factors, and Hormones in Donor Human Milk. Front. Immunol. 2018, 9, 2222. [Google Scholar] [CrossRef] [PubMed]
- Escuder-Vieco, D.; Rodríguez, J.M.; Espinosa-Martos, I.; Corzo, N.; Montilla, A.; García-Serrano, A.; Calvo, M.V.; Fontecha, J.; Serrano, J.; Fernández, L.; et al. High-Temperature Short-Time and Holder Pasteurization of Donor Milk: Impact on Milk Composition. Life 2021, 11, 114. [Google Scholar] [CrossRef] [PubMed]
- Gastmeier, P.; Geffers, C.; Schwab, F.; Fitzner, J.; Obladen, M.; Rüden, H. Development of a surveillance system for nosocomial infections: The component for neonatal intensive care units in Germany. J. Hosp. Infect. 2004, 57, 126–131. [Google Scholar] [CrossRef]
- Madrid-Aguilar, M.; López-Herrera, M.C.; Pérez-López, J.; Escudero-Argaluza, J.; Santesteban-Otazu, E.; Piening, B.; Villate-Navarro, J.I.; Pijoán-Zubizarreta, J.I. Implementation of NeoKissEs in Spain: A validated surveillance system for nosocomial sepsis in very low birth weight infants. An. Pediatr. 2019, 91, 3–12. [Google Scholar] [CrossRef]
- Fenton, T.R.; Sauve, R.S. Using the LMS method to calculate z-scores for the Fenton preterm infant growth chart. Eur. J. Clin. Nutr. 2007, 61, 1380–1385. [Google Scholar] [CrossRef]
- Fenton, T.R.; Kim, J.H. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013, 13, 59. [Google Scholar] [CrossRef]
- El Rafei, R.; Maier, R.F.; Jarreau, P.H.; Norman, M.; Barros, H.; Van Reempts, P.; Van Heijst, A.; Pedersen, P.; Cuttini, M.; Johnson, S.; et al. Postnatal growth restriction and neurodevelopment at 5 years of age: A European extremely preterm birth cohort study. Arch. Dis. Child. Fetal Neonatal Ed. 2023, 108, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Gounaris, A.K.; Sokou, R.; Gounari, E.A.; Panagiotounakou, P.; Grivea, I.N. Extrauterine Growth Restriction and Optimal Growth of Very Preterm Neonates: State of the Art. Nutrients 2023, 15, 3231. [Google Scholar] [CrossRef]
- Patel, A.L.; Engstrom, J.L.; Meier, P.P.; Kimura, R.E. Accuracy of methods for calculating postnatal growth velocity for extremely low birth weight infants. Pediatrics 2005, 116, 1466–1473. [Google Scholar] [CrossRef]
- Saiman, L. Risk factors for hospital-acquired infections in the neonatal intensive care unit. Semin. Perinatol. 2002, 26, 315–321. [Google Scholar] [CrossRef]
- Fleiss, N.; Tarun, S.; Polin, R.A. Infection prevention for extremely low birth weight infants in the NICU. Semin. Fetal Neonatal Med. 2022, 27, 101345. [Google Scholar] [CrossRef] [PubMed]
- Furuya, E.Y.; Dick, A.; Perencevich, E.N.; Pogorzelska, M.; Goldmann, D.; Stone, P.W. Central line bundle implementation in US intensive care units and impact on bloodstream infections. PLoS ONE 2011, 6, e15452. [Google Scholar] [CrossRef] [PubMed]
- Bowen, J.; Callander, I.; Richards, R.; Lindrea, K. Decreasing infection in neonatal intensive care units through quality improvement. Arch. Dis. Childhood. Fetal Neonatal Ed. 2017, 102, F51–F57. [Google Scholar] [CrossRef] [PubMed]
- Schulman, J.; Stricof, R.L.; Stevens, T.P.; Holzman, I.R.; Shields, E.P.; Angert, R.M.; Wasserman-Hoff, R.S.; Nafday, S.M.; Saiman, L. Development of a statewide collaborative to decrease NICU central line-associated bloodstream infections. J. Perinatol. 2009, 29, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Cetinbas, M.; Thai, J.; Filatava, E.; Gregory, K.E.; Sadreyev, R.I. Long-term dysbiosis and fluctuations of gut microbiome in antibiotic treated preterm infants. iScience 2023, 26, 107995. [Google Scholar] [CrossRef] [PubMed]
- Ting, J.Y.; Roberts, A. Association of early life antibiotics and health outcomes: Evidence from clinical studies. Semin. Perinatol. 2020, 44, 151322. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M.A.; Goodrich, J.K.; Maxan, M.-E.; Freedberg, D.E.; Abrams, J.A.; Poole, A.C.; Sutter, J.L.; Welter, D.; Ley, R.E.; Bell, J.T.; et al. Proton pump inhibitors alter the composition of the gut microbiota. Gut 2016, 65, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Terrin, G.; Passariello, A.; De Curtis, M.; Manguso, F.; Salvia, G.; Lega, L.; Messina, F.; Paludetto, R.; Canani, R.B. Ranitidine is associated with infections, necrotizing enterocolitis, and fatal outcome in newborns. Pediatrics 2012, 129, e40–e45. [Google Scholar] [CrossRef] [PubMed]
- Cotten, C.M. Adverse consequences of neonatal antibiotic exposure. Curr. Opin. Pediatr. 2016, 28, 141–149. [Google Scholar] [CrossRef]
- Esaiassen, E.; Fjalstad, J.W.; Juvet, L.K.; van den Anker, J.N.; Klingenberg, C. Antibiotic exposure in neonates and early adverse outcomes: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2017, 72, 1858–1870. [Google Scholar] [CrossRef]
- Pomar, L.; Favre, G.; de Labrusse, C.; Contier, A.; Boulvain, M.; Baud, D. Impact of the first wave of the COVID-19 pandemic on birth rates in Europe: A time series analysis in 24 countries. Hum. Reprod. 2022, 37, 2921–2931. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Moon, S.; Cho, K.-D.; Oh, M.-J.; Hong, S.J.; Cho, G.J. Changes in preterm birth and birthweight during the SARS-CoV-2 pandemic: A nationwide study in South Korea. Sci. Rep. 2022, 12, 16288. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| HTST Group (N = 79) | Holder Group (N = 81) | p-Values | |
|---|---|---|---|
| N (%) | N (%) | ||
| Sex (Male) | 35 (43.2) | 34 (43) | 0.98 |
| Multiple pregnancy (≥2) | 26 (32.9) | 27 (33.3) | 0.95 |
| Pregnancy (well-controlled) | 72 (91.2) | 74 (91.4) | 0.96 |
| Country of origin Spain | 47 (61.8) | 49 (62.8) | 0.90 |
| Antenatal corticosteroids (≥1 full course) | 62 (78.5) | 65 (80.3) | 0.78 |
| Low weight for gestational age (p < 10) | 24 (30) | 22 (27) | 0.65 |
| Median (IQR) | Median (IQR) | ||
| Gestational age (weeks) | 26 (25; 27) | 27 (25; 28) | 0.93 |
| Birth weight (grams) | 820 (650; 917) | 817 (660; 900) | 0.95 |
| Fenton z score for birth weight | −0.36 (−1.4; +0.2) | −0.6 (−1.3; +0.1) | 0.75 |
| Apgar score 5 min | 8 (6; 9) | 8 (6; 9) | 0.62 |
| CRIB I score | 6 (3; 9) | 6 (2; 9) | 0.93 |
| HTST Group (N = 79) | Holder Group (N = 81) | p Value | |
|---|---|---|---|
| No. episodes of confirmed catheter-associated sepsis/1000 catheter days | 17.5 | 18.7 | 0.78 |
| N (%) | N (%) | ||
| Mortality | 4 (5.1) | 4 (4.9) | 0.97 |
| NEC requiring surgery | 5 (6.3) | 2 (2.5) | 0.23 |
| NEC Bell grade ≥II or confirmed sepsis | 36 (45.6) | 39 (48.2) | 0.74 |
| Spontaneous intestinal perforation | 0 (0) | 2 (2.5) | 0.16 |
| Oxygen requirement at 36 weeks PMA age | 21 (26) | 22 (28.2) | 0.82 |
| ROP of prematurity ≥III grade | 10 (13.5) | 8 (10.3) | 0.53 |
| ROP requiring treatment | 10 (14.5) | 13(18) | 0.54 |
| Type of feeding at discharge | 0.11 | ||
| Exclusively breastfeeding | 35 (44) | 21 (26) | |
| Any amount of BF | 16 (20) | 22 (27) | |
| Exclusive formula | 25 (32) | 34 (42) | |
| Moderate EUGR birth—36 weeks PMA age (weight gain < 12.5 g/k/g/d) | 31 (39) | 36 (44) | 0.50 |
| Moderate EUGR birth—36 weeks PMA age (weight for age Fenton’s delta z-score < −1) | 46 (58) | 49 (60) | 0.77 |
| Median (IQR) | Median (IQR) | ||
| Nº of episodes of digestive intolerance/patient | 1 (0; 3) | 1 (0; 3) | 0.79 |
| Hospital stay (days) | 85 (74; 105) | 79 (69; 107) | 0.95 |
| Weight gain birth—36 wk PMA age (g/kg/day) | 12.8 (11.6; 14.8) | 12.7 (11.2; 14.1) | 0.33 |
| Fenton’s delta zscore for weight from birth to 36 weeks PMA age | −1.3 (−1.7; −0.8) | −1.4 (−1.9; −0.8) | 0.27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Lara, N.R.; Escuder-Vieco, D.; Cabrera-Lafuente, M.; Keller, K.; De Diego-Poncela, C.; Jiménez-González, C.; Núñez-Ramos, R.; Flores-Antón, B.; Escribano-Palomino, E.; Alonso-Díaz, C.; et al. Clinical Impact of Supplementation with Pasteurized Donor Human Milk by High-Temperature Short-Time Method versus Holder Method in Extremely Low Birth Weight Infants: A Multicentre Randomized Controlled Trial. Nutrients 2024, 16, 1090. https://doi.org/10.3390/nu16071090
García-Lara NR, Escuder-Vieco D, Cabrera-Lafuente M, Keller K, De Diego-Poncela C, Jiménez-González C, Núñez-Ramos R, Flores-Antón B, Escribano-Palomino E, Alonso-Díaz C, et al. Clinical Impact of Supplementation with Pasteurized Donor Human Milk by High-Temperature Short-Time Method versus Holder Method in Extremely Low Birth Weight Infants: A Multicentre Randomized Controlled Trial. Nutrients. 2024; 16(7):1090. https://doi.org/10.3390/nu16071090
Chicago/Turabian StyleGarcía-Lara, Nadia Raquel, Diana Escuder-Vieco, Marta Cabrera-Lafuente, Kristin Keller, Cristina De Diego-Poncela, Concepción Jiménez-González, Raquel Núñez-Ramos, Beatriz Flores-Antón, Esperanza Escribano-Palomino, Clara Alonso-Díaz, and et al. 2024. "Clinical Impact of Supplementation with Pasteurized Donor Human Milk by High-Temperature Short-Time Method versus Holder Method in Extremely Low Birth Weight Infants: A Multicentre Randomized Controlled Trial" Nutrients 16, no. 7: 1090. https://doi.org/10.3390/nu16071090
APA StyleGarcía-Lara, N. R., Escuder-Vieco, D., Cabrera-Lafuente, M., Keller, K., De Diego-Poncela, C., Jiménez-González, C., Núñez-Ramos, R., Flores-Antón, B., Escribano-Palomino, E., Alonso-Díaz, C., Vázquez-Román, S., Ureta-Velasco, N., Cruz-Bértolo, J. D. L., & Pallás-Alonso, C. R. (2024). Clinical Impact of Supplementation with Pasteurized Donor Human Milk by High-Temperature Short-Time Method versus Holder Method in Extremely Low Birth Weight Infants: A Multicentre Randomized Controlled Trial. Nutrients, 16(7), 1090. https://doi.org/10.3390/nu16071090