
The Circulating Selenium Concentration Is Positively Related to the Lipid Accumulation Product: A Population-Based Cross-Sectional Study



Abstract
:1. Introduction
2. Materials and Methods
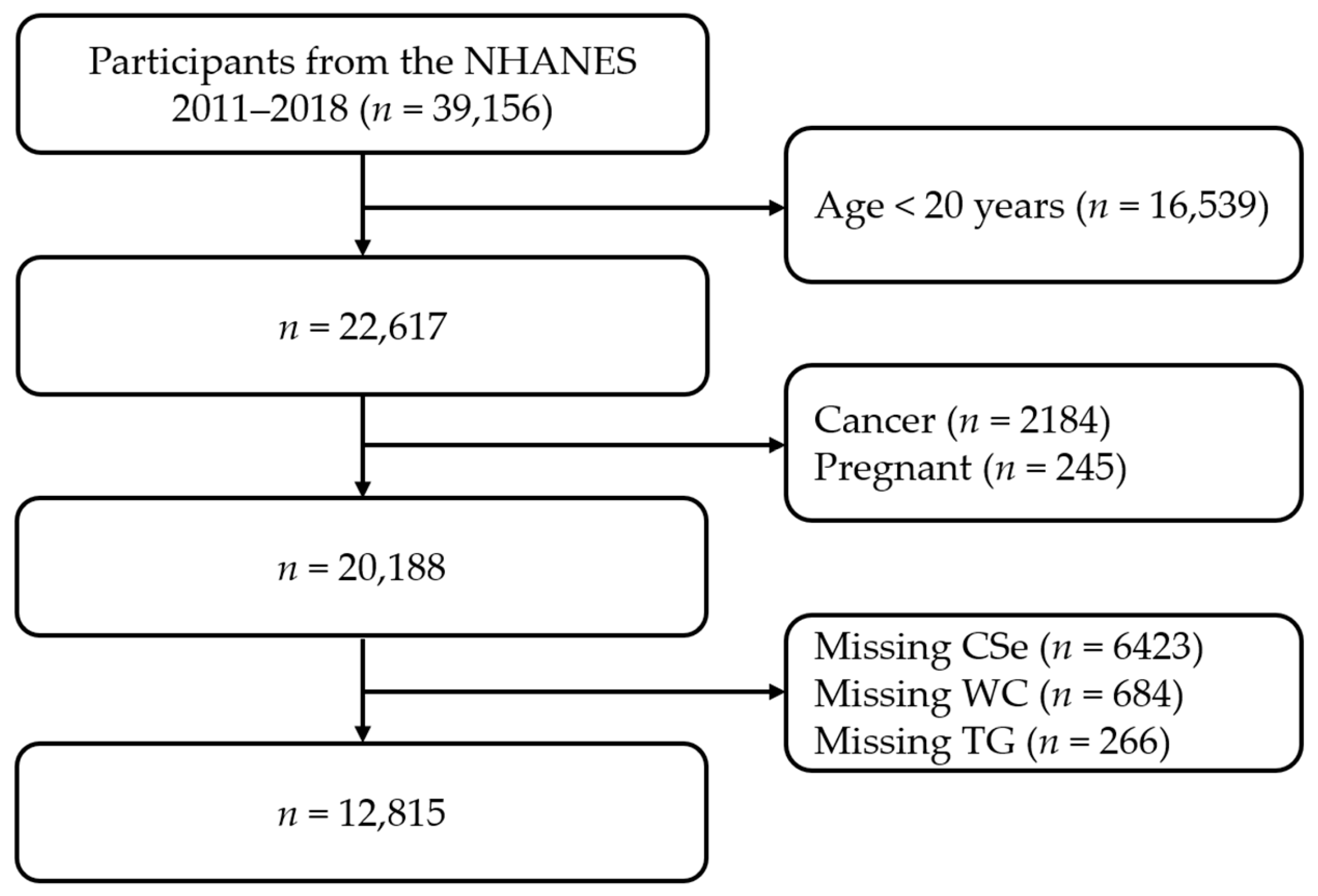
2.1. Study Population
2.2. Acquisition of Variables
2.3. Case Definition
2.4. Lipid Accumulation Product Index Calculation
2.5. Covariates Assessment
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Univariate Analysis
3.3. Multivariate Analysis
3.4. Dose–Response Analysis
3.5. Subgroup Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Friedrich, M.J. Global obesity epidemic worsening. JAMA 2017, 318, 603. [Google Scholar] [CrossRef]
- Visscher, T.L.; Heitmann, B.L.; Rissanen, A.; Lahti-Koski, M.; Lissner, L. A break in the obesity epidemic? Explained by biases or misinterpretation of the data? Int. J. Obes. 2015, 39, 189–198. [Google Scholar] [CrossRef]
- Willett, W.C.; Dietz, W.H.; Colditz, G.A. Guidelines for healthy weight. N. Engl. J. Med. 1999, 341, 427–434. [Google Scholar] [CrossRef]
- Dong, Q.; Sidra, S.; Gieger, C.; Wang-Sattler, R.; Rathmann, W.; Prehn, C.; Adamski, J.; Koenig, W.; Peters, A.; Grallert, H.; et al. Metabolic signatures elucidate the effect of body mass index on type 2 diabetes. Metabolites 2023, 13, 227. [Google Scholar] [CrossRef] [PubMed]
- Field, A.E.; Coakley, E.H.; Must, A.; Spadano, J.L.; Laird, N.; Dietz, W.H.; Rimm, E.; Colditz, G.A. Impact of overweight on the risk of developing common chronic diseases during a 10-year period. Arch. Intern. Med. 2001, 161, 1581–1586. [Google Scholar] [CrossRef] [PubMed]
- Iftikhar, R.; Snarski, P.; King, A.N.; Ghimire, J.; Ruiz, E.; Lau, F.; Savkovic, S.D. Epiploic adipose tissue (EPAT) in obese individuals promotes colonic tumorigenesis: A novel model for EPAT-dependent colorectal cancer progression. Cancers 2023, 15, 977. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.L.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef] [PubMed]
- Cruciani, S.; Delitala, A.P.; Cossu, M.L.; Ventura, C.; Maioli, M. Management of obesity and obesity-related disorders: From stem cells and epigenetics to its treatment. Int. J. Mol. Sci. 2023, 24, 2310. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Bautista, L.; Franzosi, M.G.; Commerford, P.; Lang, C.C.; Rumboldt, Z.; Onen, C.L.; Lisheng, L. Obesity and the risk of myocardial infarction in 27,000 participants from 52 countries: A case-control study. Lancet 2005, 366, 1640–1649. [Google Scholar] [CrossRef] [PubMed]
- Romero-Corral, A.; Montori, V.M.; Somers, V.K.; Korinek, J.; Thomas, R.J.; Allison, T.G.; Mookadam, F.; Lopez-Jimenez, F. Association of bodyweight with total mortality and with cardiovascular events in coronary artery disease: A systematic review of cohort studies. Lancet 2006, 368, 666–678. [Google Scholar] [CrossRef]
- Kahn, H.S. The “lipid accumulation product” performs better than the body mass index for recognizing cardiovascular risk: A population-based comparison. BMC Cardiovasc. Disord. 2005, 5, 26. [Google Scholar] [CrossRef]
- Kahn, H.S. The lipid accumulation product is better than BMI for identifying diabetes: A population-based comparison. Diabetes Care 2006, 29, 151–153. [Google Scholar] [CrossRef]
- Steinbrenner, H.; Speckmann, B.; Klotz, L.O. Selenoproteins: Antioxidant selenoenzymes and beyond. Arch. Biochem. Biophys. 2016, 595, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Tan, H.Y.; Li, S.; Xu, Y.; Guo, W.; Feng, Y. Supplementation of micronutrient selenium in metabolic diseases: Its role as an antioxidant. Oxid. Med. Cell Longev. 2017, 2017, 7478523. [Google Scholar] [CrossRef] [PubMed]
- Handy, D.E.; Joseph, J.; Loscalzo, J. Selenium, a micronutrient that modulates cardiovascular health via redox enzymology. Nutrients 2021, 13, 3238. [Google Scholar] [CrossRef]
- Chen, J.; Feng, T.; Wang, B.; He, R.; Xu, Y.; Gao, P.; Zhang, Z.H.; Zhang, L.; Fu, J.; Liu, Z.; et al. Enhancing organic selenium content and antioxidant activities of soy sauce using nano-selenium during soybean soaking. Front. Nutr. 2022, 9, 970206. [Google Scholar] [CrossRef]
- Liu, H.; Xu, H.; Huang, K. Selenium in the prevention of atherosclerosis and its underlying mechanisms. Metallomics 2017, 9, 21–37. [Google Scholar] [CrossRef] [PubMed]
- Rayman, M.P. Selenium and human health. Lancet 2012, 379, 1256–1268. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo, A.; Casas, C.; Herrero, E. Selenite-induced cell death in saccharomyces cerevisiae: Protective role of glutaredoxins. Microbiology 2010, 156, 2608–2620. [Google Scholar] [CrossRef]
- Mangiapane, E.; Pessione, A.; Pessione, E. Selenium and selenoproteins: An overview on different biological systems. Curr. Protein Pept. Sci. 2014, 15, 598–607. [Google Scholar] [CrossRef]
- Gao, X.; Shan, P.; Feng, T.; He, P.; Ran, J.; Fu, J.; Zhou, C. Enhancing selenium and key flavor compounds contents in soy sauce using selenium-enriched soybean. J. Food Compos. Anal. 2022, 106, 104299. [Google Scholar] [CrossRef]
- Shimada, B.K.; Watanabe, L.M.; Swanson, S.; Toh, P.; Seale, L.A. Selenium and selenoproteins in thermogenic adipocytes. Arch. Biochem. Biophys. 2022, 731, 109445. [Google Scholar] [CrossRef] [PubMed]
- Davanzo, G.G.; Castro, G.; Monteiro, L.B.; Castelucci, B.G.; Jaccomo, V.H.; da Silva, F.C.; Marques, A.M.; Francelin, C.; de Campos, B.B.; de Aguiar, C.F.; et al. Obesity increases blood-brain barrier permeability and aggravates the mouse model of multiple sclerosis. Mult. Scler. Relat. Disord. 2023, 72, 104605. [Google Scholar] [CrossRef] [PubMed]
- Sonnefeld, L.; Rohmann, N.; Geisler, C.; Laudes, M. Is human obesity an inflammatory disease of the hypothalamus? Eur. J. Endocrinol. 2023, 188, R37–R45. [Google Scholar] [CrossRef] [PubMed]
- He, Z.; Xu, H.; Li, C.; Yang, H.; Mao, Y. Intermittent fasting and immunomodulatory effects: A systematic review. Front. Nutr. 2023, 10, 1048230. [Google Scholar] [CrossRef] [PubMed]
- Fontenelle, L.C.; Cardoso de Araújo, D.S.; da Cunha Soares, T.; Clímaco Cruz, K.J.; Henriques, G.S.; Marreiro, D.D.N. Nutritional status of selenium in overweight and obesity: A systematic review and meta-analysis. Clin. Nutr. 2022, 41, 862–884. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.L.; Paulose-Ram, R.; Ogden, C.L. National health and nutrition examination survey: Analytic guidelines, 1999–2010. Vital Health Stat. 2 2013, 161, 1–24. [Google Scholar]
- American Heart Association. Blood Pressure Categories 2018. Available online: https://www.health.harvard.edu/heart-health/reading-the-new-blood-pressure-guidelines (accessed on 10 May 2023).
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef]
- Ding, N.; He, L.; Li, C.; Su, Y. Uric acid and blood pressure in NHANES dated from 2009 to 2018: A cross-sectional research. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 2568–2578. [Google Scholar] [CrossRef]
- Bao, W.; Liu, B.; Simonsen, D.W.; Lehmler, H.J. Association between exposure to pyrethroid insecticides and risk of all-cause and cause-specific mortality in the general U.S. adult population. JAMA Intern. Med. 2020, 180, 367–374. [Google Scholar] [CrossRef]
- Sun, H.; Wang, N.; Chen, C.; Nie, X.; Han, B.; Li, Q.; Zhu, C.; Chen, Y.; Xia, F.; Chen, Y.; et al. Cadmium exposure and its association with serum uric acid and hyperuricemia. Sci. Rep. 2017, 7, 550. [Google Scholar] [CrossRef]
- González-Domínguez, Á.; Millán-Martínez, M.; Domínguez-Riscart, J.; Mateos, R.M.; Lechuga-Sancho, A.M.; González-Domínguez, R. Altered metal homeostasis associates with inflammation, oxidative stress, impaired glucose metabolism, and dyslipidemia in the crosstalk between childhood obesity and insulin resistance. Antioxidants 2022, 11, 2439. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.W.; Chang, H.H.; Yang, K.C.; Kuo, C.S.; Lee, L.T.; Huang, K.C. High serum selenium levels are associated with increased risk for diabetes mellitus independent of central obesity and insulin resistance. BMJ Open Diabetes Res. Care 2016, 4, e000253. [Google Scholar] [CrossRef] [PubMed]
- Fatani, S.H.; Saleh, S.A.; Adly, H.M.; Abdulkhaliq, A.A. Trace element alterations in the hair of diabetic and obese women. Biol. Trace Elem. Res. 2016, 174, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Galan, P.; Viteri, F.E.; Bertrais, S.; Czernichow, S.; Faure, H.; Arnaud, J.; Ruffieux, D.; Chenal, S.; Arnault, N.; Favier, A.; et al. Serum concentrations of beta-carotene, vitamins C and E, zinc and selenium are influenced by sex, age, diet, smoking status, alcohol consumption and corpulence in a general French adult population. Eur. J. Clin. Nutr. 2005, 59, 1181–1190. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Ma, X.; Li, M.; Yan, S.; Zhao, H.; Pan, Y.; Wang, C.; Yao, Y.; Jin, L.; Li, B. Association between dietary mineral nutrient intake, body mass index, and waist circumference in U.S. adults using quantile regression analysis NHANES 2007–2014. PeerJ 2020, 8, e9127. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Xu, H.; Zhang, Y.; Chen, L.; Tian, C.; Huang, B.; Chen, Y.; Ma, L. Associations of dietary antioxidant micronutrients with the prevalence of obesity in adults. Front. Nutr. 2023, 10, 1098761. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wu, B.; Sun, G.; Gao, J.; Huang, T.; Liu, J.; Zhou, Q.; He, X.; Zhang, S.; Wang, C.Y.; et al. Dietary selenomethionine attenuates obesity by enhancing beiging process in white adipose tissue. J. Nutr. Biochem. 2023, 113, 109230. [Google Scholar] [CrossRef] [PubMed]
- Cavedon, E.; Manso, J.; Negro, I.; Censi, S.; Serra, R.; Busetto, L.; Vettor, R.; Plebani, M.; Pezzani, R.; Nacamulli, D.; et al. Selenium supplementation, body mass composition, and leptin levels in patients with obesity on a balanced mildly hypocaloric diet: A pilot study. Int. J. Endocrinol. 2020, 2020, 4802739. [Google Scholar] [CrossRef]
- Viegas-Crespo, A.M.; Pavão, M.L.; Paulo, O.; Santos, V.; Santos, M.C.; Nève, J. Trace element status (Se, Cu, Zn) and serum lipid profile in Portuguese subjects of San Miguel Island from Azores’archipelago. J. Trace Elem. Med. Biol. 2000, 14, 1–5. [Google Scholar] [CrossRef]
- Kafai, M.R.; Ganji, V. Sex, age, geographical location, smoking, and alcohol consumption influence serum selenium concentrations in the USA: Third National Health and Nutrition Examination Survey, 1988–1994. J. Trace Elem. Med. Biol. 2003, 17, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Schomburg, L. Selene, the goddess of the moon: Does she shine on men only? Eur. Heart J. 2007, 28, 2043–2044. [Google Scholar] [CrossRef] [PubMed]
- Alanne, M.; Kristiansson, K.; Auro, K.; Silander, K.; Kuulasmaa, K.; Peltonen, L.; Salomaa, V.; Perola, M. Variation in the selenoprotein S gene locus is associated with coronary heart disease and ischemic stroke in two independent Finnish cohorts. Hum. Genet 2007, 122, 355–365. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, I.; Daimon, T. A strong association between lipid accumulation product and diabetes mellitus in japanese women and men. J. Atheroscler. Thromb. 2014, 21, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Ali, J.; Haider, S.M.S.; Ali, S.M.; Haider, T.; Anwar, A.; Hashmi, A.A. Overall clinical features of type 2 diabetes mellitus with respect to gender. Cureus 2023, 15, e35771. [Google Scholar] [CrossRef] [PubMed]
- Swanson, C.A.; Longnecker, M.P.; Veillon, C.; Howe, M.; Levander, O.A.; Taylor, P.R.; McAdam, P.A.; Brown, C.C.; Stampfer, M.J.; Willett, W.C. Selenium intake, age, gender, and smoking in relation to indices of selenium status of adults residing in a seleniferous area. Am. J. Clin. Nutr. 1990, 52, 858–862. [Google Scholar] [CrossRef]
- Zhao, K.; Zhang, Y.; Sui, W. Association between blood selenium levels and stroke: A study based on the NHANES (2011–2018). Biol. Trace Elem. Res. 2023, 202, 25–33. [Google Scholar] [CrossRef]
- Okura, Y.; Urban, L.H.; Mahoney, D.W.; Jacobsen, S.J.; Rodeheffer, R.J. Agreement between self-report questionnaires and medical record data was substantial for diabetes, hypertension, myocardial infarction and stroke but not for heart failure. J. Clin. Epidemiol. 2004, 57, 1096–1103. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Total (n = 12,815) | Low (n = 4272) | Medium (n = 4271) | High (n = 4272) | p Value | |
|---|---|---|---|---|---|
| Age (years) | <0.001 | ||||
| Young | 5726 (48.46) | 2514 (61.80) | 1672 (44.04) | 1540 (39.46) | |
| Middle-aged | 3297 (28.78) | 855 (22.18) | 1129 (29.98) | 1313 (34.18) | |
| Old | 3792 (22.77) | 903 (16.03) | 1470 (25.98) | 1419 (26.36) | |
| Sex | <0.001 | ||||
| Males | 6379 (49.94) | 2057 (46.23) | 2065 (48.77) | 2257 (54.79) | |
| Females | 6436 (50.06) | 2215 (53.77) | 2206 (51.23) | 2015 (45.21) | |
| Race | <0.001 | ||||
| Mexican American | 1754 (9.18) | 390 (6.98) | 594 (9.25) | 770 (11.31) | |
| Other Hispanic | 1384 (6.89) | 381 (6.71) | 492 (7.18) | 511 (6.78) | |
| Non-Hispanic White | 4458 (63.42) | 1372 (61.53) | 1431 (62.83) | 1655 (65.87) | |
| Non-Hispanic Black | 2958 (11.18) | 1176 (13.81) | 1051 (11.77) | 731 (7.99) | |
| Others | 2261 (9.34) | 953 (10.97) | 703 (8.97) | 605 (8.06) | |
| Education | <0.001 | ||||
| <high school | 2775 (14.02) | 752 (11.45) | 956 (14.32) | 1067 (16.29) | |
| High school | 2887 (23.36) | 915 (21.19) | 934 (21.89) | 1038 (26.97) | |
| >high school | 7144 (62.59) | 2602 (67.33) | 2377 (63.76) | 2165 (56.71) | |
| Un | 9 (0.03) | 3 (0.02) | 4 (0.03) | 2 (0.03) | |
| FPRI | 0.027 | ||||
| <1 | 2542 (13.79) | 842 (14.19) | 799 (12.70) | 901 (14.45) | |
| 1–3 | 4901 (33.83) | 1540 (31.70) | 1631 (34.16) | 1730 (35.64) | |
| >3 | 4141 (44.86) | 1486 (46.23) | 1400 (45.21) | 1255 (43.15) | |
| Un | 1231 (7.52) | 404 (7.88) | 441 (7.93) | 386 (6.76) | |
| Marital status | <0.001 | ||||
| Married | 6403 (53.40) | 1874 (46.85) | 2221 (55.50) | 2308 (57.88) | |
| Never | 2645 (20.50) | 1274 (29.67) | 743 (17.40) | 628 (14.38) | |
| Others | 3761 (26.08) | 1122 (23.45) | 1304 (27.08) | 1335 (27.73) | |
| Un | 6 (0.02) | 2 (0.03) | 3 (0.02) | 1 (0.01) | |
| Current smoking status | 0.470 | ||||
| No | 10,317 (81.19) | 3407 (81.31) | 3499 (81.89) | 3411 (80.39) | |
| Yes | 2491 (18.79) | 861 (18.65) | 770 (18.09) | 860 (19.60) | |
| Un | 7 (0.02) | 4 (0.04) | 2 (0.02) | 1 (0.01) | |
| Alcohol consumption | <0.001 | ||||
| ≤3 drinks/day | 6400 (55.60) | 2272 (58.65) | 2144 (56.06) | 1984 (52.10) | |
| >3 drinks/day | 1855 (15.95) | 617 (16.03) | 555 (14.77) | 683 (17.03) | |
| Un | 4560 (28.45) | 1383 (25.32) | 1572 (29.17) | 1605 (30.88) | |
| BMI (kg/m2) | <0.001 | ||||
| <25 | 3678 (28.32) | 2686 (63.35) | 751 (17.05) | 241 (4.53) | |
| 25–30 | 4127 (32.76) | 1207 (29.05) | 1792 (44.63) | 1128 (25.06) | |
| ≥30 | 4979 (38.74) | 370 (7.60) | 1716 (38.32) | 2893 (70.41) | |
| Un | 31 (0.17) | 9 (0.153) | 12 (0.219) | 10 (0.135) | |
| Hypertension | <0.001 | ||||
| No | 6286 (53.87) | 2797 (70.84) | 1989 (52.53) | 1500 (38.25) | |
| Yes | 6529 (46.13) | 1475 (29.16) | 2282 (47.47) | 2772 (61.75) | |
| T2DM | <0.001 | ||||
| No | 10,433 (86.60) | 3966 (95.80) | 3505 (88.34) | 3023 (76.91) | |
| Yes | 2382 (13.40) | 306 (4.20) | 762 (11.62) | 1248 (23.07) | |
| Stroke | <0.001 | ||||
| No | 12,388 (97.66) | 4169 (98.44) | 4115 (97.55) | 4104 (96.99) | |
| Yes | 420 (2.28) | 100 (1.51) | 155 (2.44) | 165 (2.88) | |
| Un | 7 (0.06) | 3 (0.05) | 1 (0.01) | 3 (0.13) | |
| Coronary heart disease | <0.001 | ||||
| No | 12,362 (96.97) | 4180 (98.06) | 4122 (97.31) | 4060 (95.57) | |
| Yes | 412 (2.82) | 83 (1.83) | 137 (2.47) | 192 (4.16) | |
| Un | 41 (0.20) | 9 (0.11) | 12 (0.22) | 20 (0.28) | |
| Current taking of hypotensive drugs | <0.001 | ||||
| No | 8952 (74.02) | 3519 (86.16) | 2896 (73.41) | 2537 (62.53) | |
| Yes | 3262 (21.18) | 595 (10.15) | 1170 (21.84) | 1497 (31.53) | |
| Un | 601 (4.80) | 158 (3.69) | 205 (4.76) | 238 (5.95) | |
| Current injection of insulin | <0.001 | ||||
| No | 12,336 (97.45) | 4206 (98.64) | 4140 (98.14) | 3990 (95.59) | |
| Yes | 474 (2.51) | 65 (1.32) | 129 (1.82) | 280 (4.38) | |
| Un | 5 (0.04) | 1 (0.04) | 2 (0.04) | 2 (0.03) | |
| SBP (mmHg) | 119.33 (110.67, 130.00) | 114.00 (106.00, 124.67) | 120.00 (111.33, 130.00) | 123.33 (114.67, 134.00) | <0.001 |
| DBP (mmHg) | 71.33 (64.67, 78.00) | 68.67 (62.67, 75.33) | 72.00 (65.33, 78.00) | 74.00 (67.33, 80.67) | <0.001 |
| TC (mmol/L) | 4.89 (4.22, 5.59) | 4.55 (3.98, 5.20) | 4.94 (4.27, 5.61) | 5.17 (4.53, 5.87) | <0.001 |
| TG (mmol/L) | 1.33 (0.89, 2.00) | 0.79 (0.63, 1.01) | 1.30 (1.05, 1.60) | 2.36 (1.83, 3.25) | <0.001 |
| Glucose (mmol/L) | 5.11 (4.72, 5.61) | 4.88 (4.61, 5.27) | 5.11 (4.77, 5.55) | 5.38 (4.94, 6.16) | <0.001 |
| CSe (μmol/L) | 2.45 (2.27, 2.65) | 2.41 (2.24, 2.60) | 2.45 (2.27, 2.63) | 2.49 (2.30, 2.69) | <0.001 |
| β (95% CI) | p Value | |
|---|---|---|
| Age (years) | ||
| Young | Ref | |
| Middle-aged | 0.37 (0.31, 0.43) | <0.001 |
| Old | 0.39 (0.33, 0.45) | <0.001 |
| Sex | ||
| Males | Ref | |
| Females | −0.11 (−0.16, −0.07) | <0.001 |
| Race | ||
| Mexican American | Ref | |
| Other Hispanic | −0.20 (−0.28, −0.12) | <0.001 |
| Non-Hispanic White | −0.15 (−0.22, −0.09) | <0.001 |
| Non-Hispanic Black | −0.44 (−0.50, −0.39) | <0.001 |
| Others | −0.31 (−0.39, −0.24) | <0.001 |
| Education | ||
| <high school | Ref | |
| High school | −0.02 (−0.09, 0.04) | 0.487 |
| >high school | −0.17 (−0.22, −0.11) | <0.001 |
| Un | −0.01 (−0.45, 0.42) | 0.962 |
| FPRI | ||
| <1 | Ref | |
| 1–3 | 0.06 (−0.02, 0.13) | 0.133 |
| >3 | −0.02 (−0.06, 0.09) | 0.685 |
| Un | −0.04 (−0.13, 0.06) | 0.454 |
| Marital status | ||
| Married | Ref | |
| Never | −0.43 (−0.49, −0.36) | <0.001 |
| Others | −0.04 (−0.09, 0.01) | 0.099 |
| Un | −0.14 (−0.55, 0.27) | 0.511 |
| Current smoking status | ||
| No | Ref | |
| Yes | −0.00 (−0.06, 0.05) | 0.948 |
| Un | −0.18 (−0.95, 0.58) | 0.639 |
| Alcohol consumption | ||
| ≤3 drinks/day | Ref | |
| >3 drinks/day | 0.05 (−0.03, 0.13) | 0.200 |
| Un | 0.11 (0.06, 0.15) | <0.001 |
| BMI (kg/m2) | ||
| <25 | Ref | |
| 25–30 | 0.84 (0.80, 0.88) | <0.001 |
| ≥30 | 1.44 (1.40, 1.48) | <0.001 |
| Un | 0.89 (0.39, 1.39) | <0.001 |
| Hypertension | ||
| No | Ref | |
| Yes | 0.52 (0.47, 0.57) | <0.001 |
| T2DM | ||
| No | Ref | |
| Yes | 0.68 (0.61, 0.75) | <0.001 |
| Stroke | ||
| No | Ref | |
| Yes | 0.24 (0.12, 0.37) | <0.001 |
| Un | 0.20 (−0.78, 1.17) | 0.692 |
| Coronary heart disease | ||
| No | Ref | |
| Yes | 0.37 (0.22, 0.52) | <0.001 |
| Un | 0.22 (−0.06, 0.49) | 0.131 |
| TC (mmol/L) | ||
| <6.22 | Ref | |
| ≥6.22 | 0.50 (0.44, 0.56) | <0.001 |
| Glucose (mmol/L) | ||
| <6.1 | Ref | |
| 6.1–7.0 | 0.46 (0.39, 0.53) | <0.001 |
| ≥7.0 | 0.81 (0.72, 0.89) | <0.001 |
| SBP (mmHg) | ||
| <130 | Ref | |
| ≥130 | 0.37 (0.32, 0.41) | <0.001 |
| Un | 0.17 (0.10, 0.24) | <0.001 |
| DBP (mmHg) | ||
| <80 | Ref | |
| ≥80 | 0.37 (0.31, 0.42) | <0.001 |
| Un | 0.15 (0.08, 0.23) | <0.001 |
| Current taking of hypotensive drugs | ||
| No | Ref | |
| Yes | 0.53 (0.47, 0.59) | <0.001 |
| Un | 0.31 (0.23, 0.40) | <0.001 |
| Current injection of insulin | ||
| No | Ref | |
| Yes | 0.54 (0.40, 0.69) | <0.001 |
| Un | −0.10 (−1.22, 1.01) | 0.855 |
| Ln CSe (μmol/L) | 0.76 (0.56, 0.95) | <0.001 |
| Model A | p Value | Model B | p Value | Model C | p Value | |
|---|---|---|---|---|---|---|
| β (95% CI) | β (95% CI) | β (95% CI) | ||||
| Ln CSe (μmol/L) | 0.76 (0.56, 0.95) | <0.001 | 0.66 (0.47, 0.84) | <0.001 | 0.41 (0.28, 0.54) | <0.001 |
| Ln Cse quartiles | ||||||
| Quartile 1 (<0.81) | Ref | Ref | Ref | |||
| Quartile 2 (0.81–0.89) | 0.09 (0.02, 0.15) | 0.018 | 0.07 (0.00, 0.14) | 0.048 | 0.04 (−0.01, 0.10) | 0.119 |
| Quartile 3 (0.90–0.97) | 0.16 (0.10, 0.21) | <0.001 | 0.14 (0.08, 0.20) | <0.001 | 0.07 (0.02, 0.12) | 0.011 |
| Quartile 4 (≥0.98) | 0.29 (0.23, 0.36) | <0.001 | 0.26 (0.20, 0.32) | <0.001 | 0.16 (0.12, 0.21) | <0.001 |
| p for trend | <0.001 | <0.001 | <0.001 |
| Inflection Point of Ln CSe (μmol/L) | β (95% CI) | p Value |
|---|---|---|
| <1.10 | 0.45 (0.35, 0.55) | <0.001 |
| ≥1.10 | −0.13 (−0.48, 0.21) | 0.454 |
| p for log-likelihood ratio test | 0.003 |
| β (95% CI) | p Value | p for Interaction | |
|---|---|---|---|
| Age (years) | 0.032 | ||
| Young | 0.47 (0.33, 0.62) | <0.001 | |
| Middle-aged | 0.56 (0.26, 0.86) | 0.001 | |
| Old | 0.17 (−0.02, 0.36) | 0.092 | |
| Sex | <0.001 | ||
| Males | 0.64 (0.47, 0.80) | <0.001 | |
| Females | 0.20 (0.06, 0.34) | 0.011 | |
| Race | 0.589 | ||
| Mexican American | 0.30 (−0.03, 0.63) | 0.094 | |
| Other Hispanic | 0.31 (−0.00, 0.63) | 0.068 | |
| Non-Hispanic White | 0.40 (0.24, 0.57) | <0.001 | |
| Non-Hispanic Black | 0.41 (0.22, 0.61) | <0.001 | |
| Other | 0.57 (0.34, 0.79) | <0.001 | |
| Education | 0.981 | ||
| <high school | 0.42 (0.20, 0.65) | 0.001 | |
| High school | 0.41 (0.18, 0.64) | 0.002 | |
| >high school | 0.40 (0.25, 0.55) | <0.001 | |
| FPRI | 0.985 | ||
| <1 | 0.41 (0.20, 0.61) | 0.001 | |
| 1–3 | 0.38 (0.19, 0.58) | 0.001 | |
| >3 | 0.40 (0.20, 0.59) | 0.001 | |
| Marital status | 0.210 | ||
| Married | 0.33 (0.17, 0.50) | 0.001 | |
| Never | 0.60 (0.37, 0.83) | <0.001 | |
| Others | 0.41 (0.18, 0.64) | 0.002 | |
| Current smoking status | 0.037 | ||
| No | 0.37 (0.25, 0.50) | <0.001 | |
| Yes | 0.64 (0.37, 0.91) | <0.001 | |
| Alcohol consumption (drinks/day) | 0.092 | ||
| ≤3 | 0.37 (0.19, 0.56) | <0.001 | |
| >3 | 0.66 (0.36, 0.96) | <0.001 | |
| BMI (kg/m2) | 0.092 | ||
| <25 | 0.40 (0.18, 0.62) | 0.002 | |
| 25–30 | 0.26 (0.07, 0.44) | 0.013 | |
| ≥30 | 0.55 (0.35, 0.76) | <0.001 | |
| Hypertension | 0.067 | ||
| No | 0.51 (0.35, 0.66) | <0.001 | |
| Yes | 0.31 (0.14, 0.48) | 0.002 | |
| T2DM | 0.805 | ||
| No | 0.41 (0.28, 0.55) | <0.001 | |
| Yes | 0.38 (0.09, 0.66) | 0.017 | |
| Stroke | 0.033 | ||
| No | 0.43 (0.30, 0.57) | <0.001 | |
| Yes | −0.32 (−0.95, 0.31) | 0.329 | |
| Coronary heart disease | 0.943 | ||
| No | 0.40 (0.28, 0.53) | <0.001 | |
| Yes | 0.42 (−0.01, 0.85) | 0.066 | |
| TC (mmol/L) | 0.331 | ||
| <6.22 | 0.44 (0.31, 0.57) | <0.001 | |
| ≥6.22 | 0.22 (−0.21, 0.65) | 0.336 | |
| Glucose (mmol/L) | 0.051 | ||
| <6.1 | 0.41 (0.28, 0.55) | <0.001 | |
| 6.1–7.0 | 0.07 (−0.26, 0.41) | 0.678 | |
| ≥7.0 | 0.68 (0.31, 1.05) | 0.002 | |
| SBP (mmHg) | 0.903 | ||
| <130 | 0.41 (0.27, 0.55) | <0.001 | |
| ≥130 | 0.39 (0.10, 0.68) | 0.014 | |
| DBP (mmHg) | 0.076 | ||
| <80 | 0.46 (0.31, 0.61) | <0.001 | |
| ≥80 | 0.20 (−0.06, 0.46) | 0.139 | |
| Current taking of hypotensive drugs | 0.066 | ||
| No | 0.47 (0.32, 0.61) | <0.001 | |
| Yes | 0.22 (−0.01, 0.45) | 0.077 | |
| Current injection of insulin | 0.688 | ||
| No | 0.41 (0.28, 0.54) | <0.001 | |
| Yes | 0.29 (−0.31, 0.88) | 0.352 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, K.; Zhang, Y.; Sui, W. The Circulating Selenium Concentration Is Positively Related to the Lipid Accumulation Product: A Population-Based Cross-Sectional Study. Nutrients 2024, 16, 933. https://doi.org/10.3390/nu16070933
Zhao K, Zhang Y, Sui W. The Circulating Selenium Concentration Is Positively Related to the Lipid Accumulation Product: A Population-Based Cross-Sectional Study. Nutrients. 2024; 16(7):933. https://doi.org/10.3390/nu16070933
Chicago/Turabian StyleZhao, Kunsheng, Yun Zhang, and Wenhai Sui. 2024. "The Circulating Selenium Concentration Is Positively Related to the Lipid Accumulation Product: A Population-Based Cross-Sectional Study" Nutrients 16, no. 7: 933. https://doi.org/10.3390/nu16070933
APA StyleZhao, K., Zhang, Y., & Sui, W. (2024). The Circulating Selenium Concentration Is Positively Related to the Lipid Accumulation Product: A Population-Based Cross-Sectional Study. Nutrients, 16(7), 933. https://doi.org/10.3390/nu16070933