
Home Meal Replacement Fortified with Eggshell Powder and Vitamin D Prevents Bone Loss in Postmenopausal Women: A Randomized, Double-Blind, Controlled Study
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
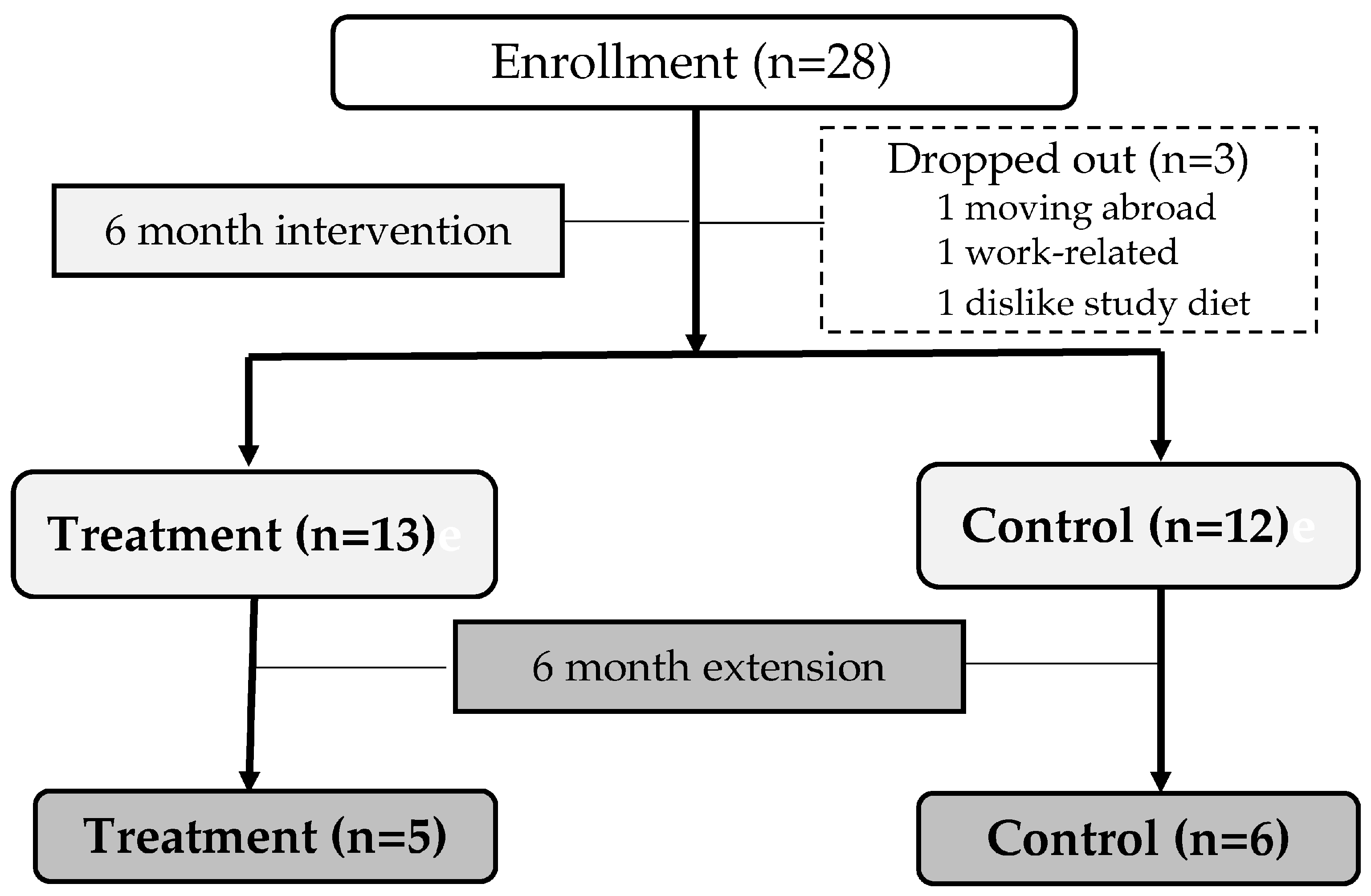
2.1. Study Design
2.2. Participants
2.3. Anthropometry, Biochemical Analysis, Bone Mineral Density Measurement, and Assessment of Dietary Intake
2.4. Dietary Carotenoid and Serum Carotenoid Analysis
2.5. Lifestyle Habits Evaluation
2.6. Statistical Analysis
3. Results
3.1. Similar Baseline Characteristics of Control and Treatment Groups
3.2. Calcium, Vitamin D, and Carotenoid Contents in Study Diets
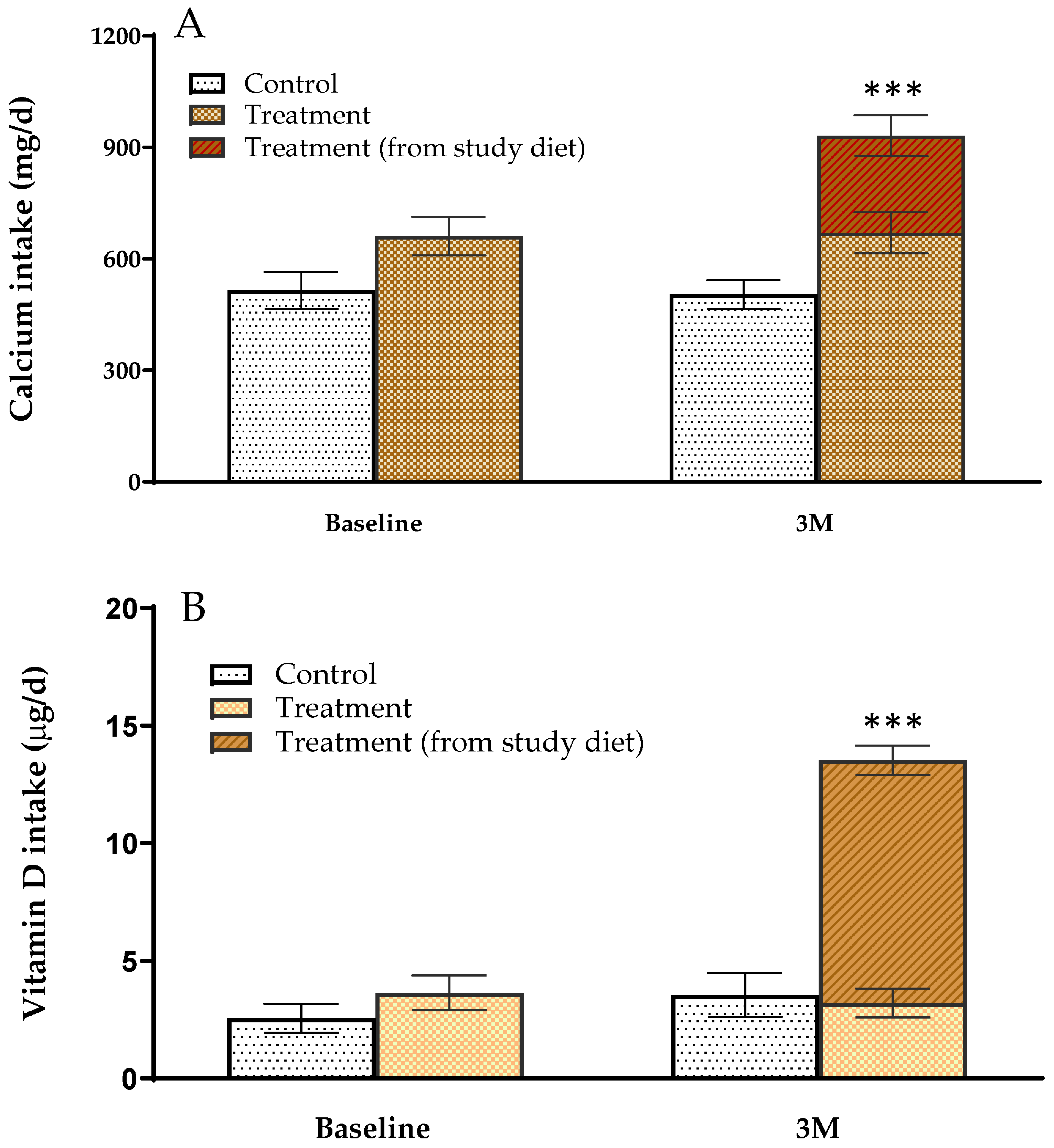
3.3. Calcium and Vitamin D Intake of Study Participants
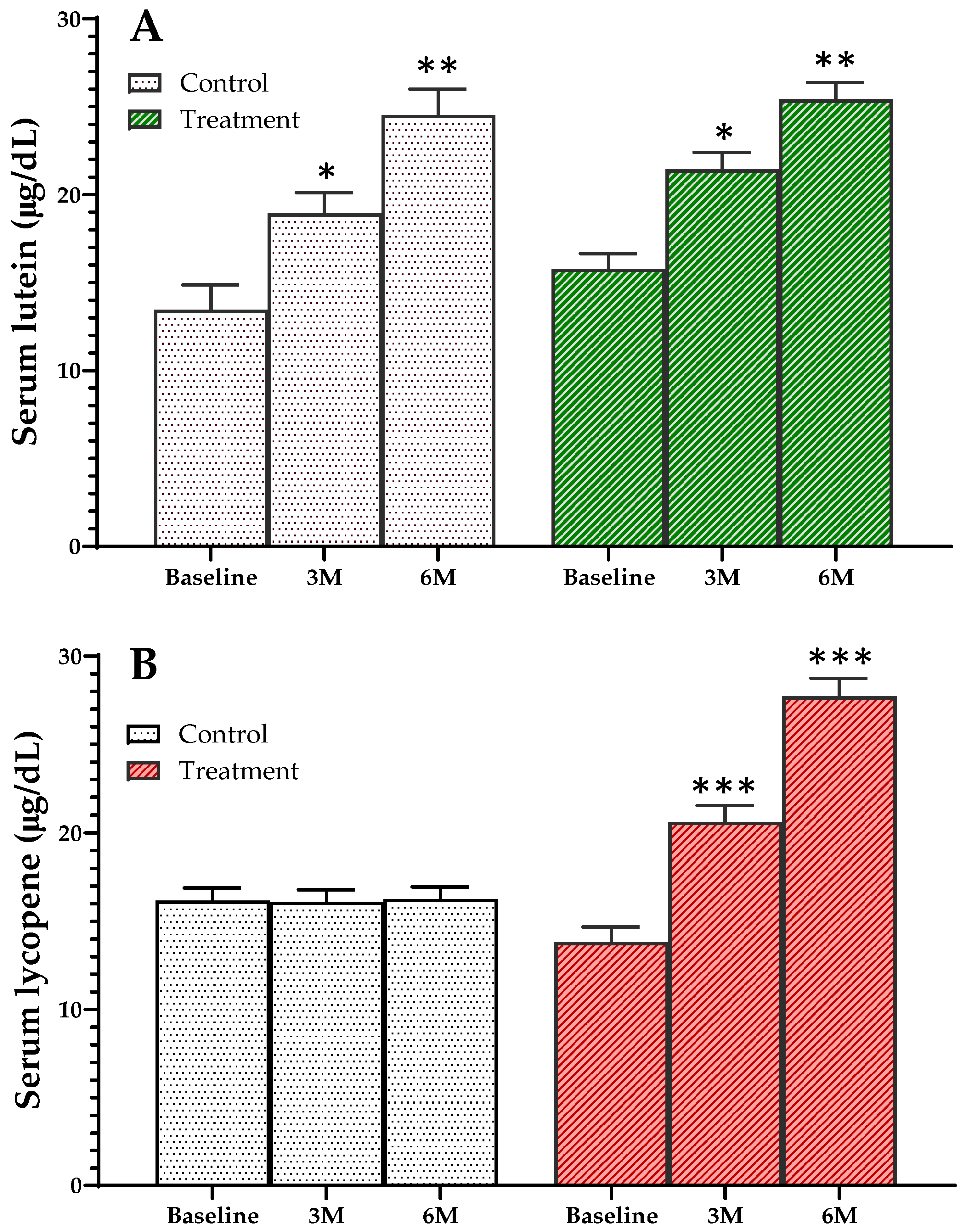
3.4. Changes in Serum Carotenoid Concentrations of Study Participants
3.5. Changes in Bone Mineral Density and Bone Markers of Study Participants
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holvik, K.; Ellingsen, C.L.; Solbakken, S.M.; Finnes, T.E.; Talsnes, O.; Grimnes, G.; Tell, G.S.; Sogaard, A.J.; Meyer, H.E. Cause-specific excess mortality after hip fracture: The Norwegian Epidemiologic Osteoporosis Studies (NOREPOS). BMC Geriatr. 2023, 23, 201. [Google Scholar] [CrossRef]
- Weaver, C.M.; Alexander, D.D.; Boushey, C.J.; Dawson-Hughes, B.; Lappe, J.M.; LeBoff, M.S.; Liu, S.; Looker, A.C.; Wallace, T.C.; Wang, D.D. Calcium plus vitamin D supplementation and risk of fractures: An updated meta-analysis from the National Osteoporosis Foundation. Osteoporos. Int. 2016, 27, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Kung, A.W.; Lee, K.K.; Ho, A.Y.; Tang, G.; Luk, K.D. Ten-year risk of osteoporotic fractures in postmenopausal Chinese women according to clinical risk factors and BMD T-scores: A prospective study. J. Bone Miner. Res. 2007, 22, 1080–1087. [Google Scholar] [CrossRef] [PubMed]
- Cano, A.; Chedraui, P.; Goulis, D.G.; Lopes, P.; Mishra, G.; Mueck, A.; Senturk, L.M.; Simoncini, T.; Stevenson, J.C.; Stute, P.; et al. Calcium in the prevention of postmenopausal osteoporosis: EMAS clinical guide. Maturitas 2018, 107, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Manoj, P.; Derwin, R.; George, S. What is the impact of daily oral supplementation of vitamin D3 (cholecalciferol) plus calcium on the incidence of hip fracture in older people? A systematic review and meta-analysis. Int. J. Older People Nurs. 2023, 18, e12492. [Google Scholar] [CrossRef]
- Force, U.S.P.S.T.; Grossman, D.C.; Curry, S.J.; Owens, D.K.; Barry, M.J.; Caughey, A.B.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W., Jr.; Kemper, A.R.; et al. Vitamin D, Calcium, or Combined Supplementation for the Primary Prevention of Fractures in Community-Dwelling Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2018, 319, 1592–1599. [Google Scholar] [CrossRef]
- Uusi-Rasi, K.; Karkkainen, M.U.; Lamberg-Allardt, C.J. Calcium intake in health maintenance—A systematic review. Food Nutr. Res. 2013, 57, 21082. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; Wang, Z.; Zhang, J.; Du, W.; Su, C.; Jiang, H.; Jia, X.; Ouyang, Y.; Wang, Y.; Li, L.; et al. Dietary calcium intake and food sources among Chinese adults in CNTCS. PLoS ONE 2018, 13, e0205045. [Google Scholar] [CrossRef] [PubMed]
- Raj, J.P.; Venkatachalam, S.; Shekoba, M.; Norris, J.J.; Amaravati, R.S. Dietary calcium intake and physical activity levels among people living in Karnataka, India—An observational hospital-based study. J. Family Med. Prim. Care 2018, 7, 1411–1416. [Google Scholar] [CrossRef]
- Ohta, H.; Uenishi, K.; Shiraki, M. Recent nutritional trends of calcium and vitamin D in East Asia. Osteoporos. Sarcopenia 2016, 2, 208–213. [Google Scholar] [CrossRef]
- Kogure, M.; Tsuchiya, N.; Narita, A.; Hirata, T.; Nakaya, N.; Nakamura, T.; Hozawa, A.; Hayakawa, T.; Okuda, N.; Miyagawa, N.; et al. Relationship Between Calcium Intake and Impaired Activities of Daily Living in a Japanese Population: NIPPON DATA90. J. Epidemiol. 2021, 31, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Joo, N.S.; Dawson-Hughes, B.; Kim, Y.S.; Oh, K.; Yeum, K.J. Impact of calcium and vitamin D insufficiencies on serum parathyroid hormone and bone mineral density: Analysis of the fourth and fifth Korea National Health and Nutrition Examination Survey (KNHANES IV-3, 2009 and KNHANES V-1, 2010). J. Bone Miner. Res. 2013, 28, 764–770. [Google Scholar] [CrossRef] [PubMed]
- Platonova, K.; Kitamura, K.; Watanabe, Y.; Takachi, R.; Saito, T.; Kabasawa, K.; Takahashi, A.; Kobayashi, R.; Oshiki, R.; Solovev, A.; et al. Dietary calcium and vitamin K are associated with osteoporotic fracture risk in middle-aged and elderly Japanese women, but not men: The Murakami Cohort Study. Br. J. Nutr. 2021, 125, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Storhaug, C.L.; Fosse, S.K.; Fadnes, L.T. Country, regional, and global estimates for lactose malabsorption in adults: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2017, 2, 738–746. [Google Scholar] [CrossRef] [PubMed]
- Anguita-Ruiz, A.; Aguilera, C.M.; Gil, A. Genetics of Lactose Intolerance: An Updated Review and Online Interactive World Maps of Phenotype and Genotype Frequencies. Nutrients 2020, 12, 2689. [Google Scholar] [CrossRef] [PubMed]
- Maoka, T. Carotenoids as natural functional pigments. J. Nat. Med. 2020, 74, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Yeum, K.J.; Booth, S.L.; Sadowski, J.A.; Liu, C.; Tang, G.; Krinsky, N.I.; Russell, R.M. Human plasma carotenoid response to the ingestion of controlled diets high in fruits and vegetables. Am. J. Clin. Nutr. 1996, 64, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Milani, A.; Basirnejad, M.; Shahbazi, S.; Bolhassani, A. Carotenoids: Biochemistry, pharmacology and treatment. Br. J. Pharmacol. 2017, 174, 1290–1324. [Google Scholar] [CrossRef] [PubMed]
- Semeghini, M.S.; Scalize, P.H.; Coelho, M.C.; Fernandes, R.R.; Pitol, D.L.; Tavares, M.S.; de Sousa, L.G.; Coppi, A.A.; Siessere, S.; Bombonato-Prado, K.F. Lycopene prevents bone loss in ovariectomized rats and increases the number of osteocytes and osteoblasts. J. Anat. 2022, 241, 729–740. [Google Scholar] [CrossRef]
- Fina, B.L.; Brun, L.R.; Rigalli, A. Increase of calcium and reduction of lactose concentration in milk by treatment with kefir grains and eggshell. Int. J. Food Sci. Nutr. 2016, 67, 133–140. [Google Scholar] [CrossRef]
- Waheed, M.; Butt, M.S.; Shehzad, A.; Adzahan, N.M.; Shabbir, M.A.; Suleria, H.A.R.; Aadil, R.M. Eggshell calcium: A cheap alternative to expensive supplements. Trends Food Sci. Technol. 2019, 91, 219–230. [Google Scholar] [CrossRef]
- Schaafsma, A.; Pakan, I.; Hofstede, G.J.; Muskiet, F.A.; Van Der Veer, E.; De Vries, P.J. Mineral, amino acid, and hormonal composition of chicken eggshell powder and the evaluation of its use in human nutrition. Poult. Sci. 2000, 79, 1833–1838. [Google Scholar] [CrossRef] [PubMed]
- Schaafsma, A.; van Doormaal, J.J.; Muskiet, F.A.; Hofstede, G.J.; Pakan, I.; van der Veer, E. Positive effects of a chicken eggshell powder-enriched vitamin-mineral supplement on femoral neck bone mineral density in healthy late post-menopausal Dutch women. Br. J. Nutr. 2002, 87, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Ji, Y.; Han, J. Sustainable Home Meal Replacement (HMR) Consumption in Korea: Exploring Service Strategies Using a Modified Importance-Performance Analysis. Foods 2022, 11, 889. [Google Scholar] [CrossRef] [PubMed]
- Bae, M.A.; Park, S.H.; Cheng, S.; Chang, K.J. Comparison of consumption behaviors and development needs for the home meal replacement among Chinese college students studying abroad in Korea, Chinese college students in China, and Korean college students in Korea. Nutr. Res. Pract. 2021, 15, 747–760. [Google Scholar] [CrossRef]
- Folch, J.; Lees, M.; Sloane Stanley, G. A simple method for the isolation and purification of total lipids from animal tissues. J. Biol Chem. 1957, 226, 497–509. [Google Scholar] [CrossRef] [PubMed]
- Ju, J.-H.; Cho, S.-Y.; Song, H.-Y.; Ju, S.; Yoon, Y.-H.; Yeum, K.-J. Growth and carotenoid contents of intercropped vegetables in building-integrated urban agriculture. J. Food Qual. 2021, 2021, 1159567. [Google Scholar] [CrossRef]
- Shlisky, J.; Mandlik, R.; Askari, S.; Abrams, S.; Belizan, J.M.; Bourassa, M.W.; Cormick, G.; Driller-Colangelo, A.; Gomes, F.; Khadilkar, A.; et al. Calcium deficiency worldwide: Prevalence of inadequate intakes and associated health outcomes. Ann. N. Y. Acad. Sci. 2022, 1512, 10–28. [Google Scholar] [CrossRef] [PubMed]
- Kumssa, D.B.; Joy, E.J.; Ander, E.L.; Watts, M.J.; Young, S.D.; Walker, S.; Broadley, M.R. Dietary calcium and zinc deficiency risks are decreasing but remain prevalent. Sci. Rep. 2015, 5, 10974. [Google Scholar] [CrossRef]
- Balk, E.M.; Adam, G.P.; Langberg, V.N.; Earley, A.; Clark, P.; Ebeling, P.R.; Mithal, A.; Rizzoli, R.; Zerbini, C.A.F.; Pierroz, D.D.; et al. Global dietary calcium intake among adults: A systematic review. Osteoporos. Int. 2017, 28, 3315–3324. [Google Scholar] [CrossRef]
- Kim, J.; Ha, J.; Jeong, C.; Lee, J.; Lim, Y.; Jo, K.; Kim, M.K.; Kwon, H.S.; Song, K.H.; Baek, K.H. Bone mineral density and lipid profiles in older adults: A nationwide cross-sectional study. Osteoporos. Int. 2023, 34, 119–128. [Google Scholar] [CrossRef]
- Zheng, M.; Wan, Y.; Liu, G.; Gao, Y.; Pan, X.; You, W.; Yuan, D.; Shen, J.; Lu, J.; Wang, X.; et al. Differences in the prevalence and risk factors of osteoporosis in chinese urban and rural regions: A cross-sectional study. BMC Musculoskelet. Disord. 2023, 24, 46. [Google Scholar] [CrossRef] [PubMed]
- Wallace, T.C.; Bailey, R.L.; Lappe, J.; O’Brien, K.O.; Wang, D.D.; Sahni, S.; Weaver, C.M. Dairy intake and bone health across the lifespan: A systematic review and expert narrative. Crit. Rev. Food Sci. Nutr. 2021, 61, 3661–3707. [Google Scholar] [CrossRef] [PubMed]
- Rizzoli, R. Dairy products and bone health. Aging Clin. Exp. Res. 2022, 34, 9–24. [Google Scholar] [CrossRef]
- Cormick, G.; Betran, A.P.; Metz, F.; Palacios, C.; Beltran-Velazquez, F.; Garcia-Casal, M.L.N.; Pena-Rosas, J.P.; Hofmeyr, G.J.; Belizan, J.M. Regulatory and Policy-Related Aspects of Calcium Fortification of Foods. Implications for Implementing National Strategies of Calcium Fortification. Nutrients 2020, 12, 1022. [Google Scholar] [CrossRef] [PubMed]
- Cormick, G.; Betran, A.P.; Romero, I.B.; Cormick, M.S.; Belizan, J.M.; Bardach, A.; Ciapponi, A. Effect of Calcium Fortified Foods on Health Outcomes: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 316. [Google Scholar] [CrossRef]
- Norton, C.; Hettiarachchi, M.; Cooke, R.; Kozior, M.; Kontro, H.; Daniel, R.; Jakeman, P. Effect of 24-Week, Late-Evening Ingestion of a Calcium-Fortified, Milk-Based Protein Matrix on Biomarkers of Bone Metabolism and Site-Specific Bone Mineral Density in Postmenopausal Women with Osteopenia. Nutrients 2022, 14, 3486. [Google Scholar] [CrossRef]
- Morato-Martinez, M.; Lopez-Plaza, B.; Santurino, C.; Palma-Milla, S.; Gomez-Candela, C. A Dairy Product to Reconstitute Enriched with Bioactive Nutrients Stops Bone Loss in High-Risk Menopausal Women without Pharmacological Treatment. Nutrients 2020, 12, 2203. [Google Scholar] [CrossRef]
- Friling, M.; Haber, A.; Furman-Assaf, S.; Israel, D.; Harari, G.; Evans, M.; Crowley, D.C.; Ouwehand, A.C.; Ivanir, E. Bioavailability of calcium in an enriched postbiotic system compared to calcium citrate in healthy postmenopausal females; A randomized, double-blind, comparator-controlled, crossover study. Front. Nutr. 2023, 10, 1073622. [Google Scholar] [CrossRef]
- Kim, K.M.; Choi, H.S.; Choi, M.J.; Chung, H.Y. Calcium and Vitamin D Supplementations: 2015 Position Statement of the Korean Society for Bone and Mineral Research. J. Bone Metab. 2015, 22, 143–149. [Google Scholar] [CrossRef]
- Bu, S.Y.; Choi, M.J.; Choi, D.S.; Jung, Y.M.; Jang, I.S.; Yang, N.; Kim, K.; Park, C.Y. Perspectives on the systematic review for the 2020 Dietary Reference Intakes for Koreans for calcium. Nutr. Res. Pract 2022, 16, S89–S112. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.; Hu, J.; Kong, X.; Zhu, Z. Association between Dietary Calcium Intake and Bone Mineral Density in Older Adults. Ecol. Food Nutr. 2020, 62, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Bailey, R.L.; Zou, P.; Wallace, T.C.; McCabe, G.P.; Craig, B.A.; Jun, S.; Cauley, J.A.; Weaver, C.M. Calcium Supplement Use Is Associated with Less Bone Mineral Density Loss, But Does Not Lessen the Risk of Bone Fracture Across the Menopause Transition: Data From the Study of Women’s Health Across the Nation. JBMR Plus 2020, 4, e10246. [Google Scholar] [CrossRef] [PubMed]
- Bristow, S.M.; Horne, A.M.; Gamble, G.D.; Mihov, B.; Stewart, A.; Reid, I.R. Dietary Calcium Intake and Bone Loss Over 6 Years in Osteopenic Postmenopausal Women. J. Clin. Endocrinol. Metab. 2019, 104, 3576–3584. [Google Scholar] [CrossRef] [PubMed]
- Aloia, J.F.; Chen, D.G.; Yeh, J.K.; Chen, H. Serum vitamin D metabolites and intestinal calcium absorption efficiency in women. Am. J. Clin. Nutr. 2010, 92, 835–840. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.G.; Zeng, X.T.; Wang, J.; Liu, L. Association Between Calcium or Vitamin D Supplementation and Fracture Incidence in Community-Dwelling Older Adults: A Systematic Review and Meta-analysis. JAMA 2017, 318, 2466–2482. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Kurahashi, N.; Ishihara, J.; Inoue, M.; Tsugane, S.; Japan Public Health Centre-Based Prospective Study Group. Calcium intake and the 10-year incidence of self-reported vertebral fractures in women and men: The Japan Public Health Centre-based Prospective Study. Br. J. Nutr. 2009, 101, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Warensjo Lemming, E.; Byberg, L.; Hoijer, J.; Larsson, S.C.; Wolk, A.; Michaelsson, K. Combinations of dietary calcium intake and mediterranean-style diet on risk of hip fracture: A longitudinal cohort study of 82,000 women and men. Clin. Nutr. 2021, 40, 4161–4170. [Google Scholar] [CrossRef] [PubMed]
- Marini, H.; Minutoli, L.; Polito, F.; Bitto, A.; Altavilla, D.; Atteritano, M.; Gaudio, A.; Mazzaferro, S.; Frisina, A.; Frisina, N.; et al. OPG and sRANKL serum concentrations in osteopenic, postmenopausal women after 2-year genistein administration. J. Bone Miner. Res. 2008, 23, 715–720. [Google Scholar] [CrossRef]
- Liu, C.; Wong, P.Y.; Tong, X.; Chow, S.K.; Hung, V.W.; Cheung, W.H.; Qin, L.; Law, S.W.; Wong, R.M.Y. Muscle plays a more superior role than fat in bone homeostasis: A cross-sectional study of old Asian people. Front. Endocrinol. 2022, 13, 990442. [Google Scholar] [CrossRef]
- Chen, M.; Zhang, Y.; Zhang, L.; Wang, L.; Guo, Q.; Zhou, H.; Wang, W.; He, Y.; Xia, S.; Shao, L. The Effect of Education Intervention on Osteoporotic Fracture and Bone Mineral Density in Elderly Women with Osteoporosis: A Randomized Controlled Trial. Altern. Ther. Health Med. 2022, 28, 89–95. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 25) | Treatment (n = 13) | Control (n = 12) | p-Value |
|---|---|---|---|---|
| General characteristics | ||||
| Age (years) | 55.7 (3.4) | 56.0 (2.7) | 55.3 (4.1) | 0.611 |
| Body weight (kg) | 60.1 (8.1) | 59.8 (8.9) | 60.8 (7.5) | 0.852 |
| Height (cm) | 158.0 (4.8) | 158.3 (4.4) | 157.6 (5.3) | 0.574 |
| BMI (kg/m2) | 24.1 (3.1) | 23.8 (3.0) | 24.5 (3.4) | 0.810 |
| Waist circumference (cm) | 82.7 (7.7) | 82.8 (8.0) | 82.5 (7.8) | 0.979 |
| Clinical characteristics | ||||
| SBP (mmHg) | 120.6 (10.2) | 119.9 (10.7) | 121.3 (10.0) | 0.810 |
| DBP (mmHg) | 76.1 (9.6) | 76.6 (8.7) | 75.5 (10.6) | 0.769 |
| FBS (mg/dl) | 96.0 (11.7) | 93.7 (11.0) | 98.6 (12.5) | 0.270 |
| Total cholesterol (mg/dl) | 241.2 (38.2) | 236.0 (32.9) | 190.5 (28.9) | 0.002 |
| Triglyceride (mg/dl) | 113.8 (51.4) | 108.2 (51.3) | 120.0 (53.1) | 0.728 |
| HDL (mg/dl) | 63.9 (16.9) | 68.5 (18.9) | 58.8 (13.5) | 0.137 |
| LDL (mg/dl) | 127.5 (35.8) | 145.8 (36.3) | 107.8 (23.5) | 0.010 |
| Dietary intake | ||||
| Calorie intake (kcal/day) | 2165.7 (716.7) | 2376.2 (748.8) | 1972.7 (657.7) | 0.082 |
| Carbohydrate (g/d) | 357.1 (122.5) | 402.6 (117.0) | 315.4 (116.6) | >0.999 |
| Protein (g/d) | 77.1 (27.4) | 86.8 (32.0) | 68.1 (19.7) | >0.999 |
| Fat (g/d) | 47.6 (18.9) | 47.7 (22.0) | 47.5 (16.4) | >0.999 |
| Calcium intake (mg/d) | 585.1 (24.2) | 661.5 (307.0) | 515.1 (142.6) | >0.999 |
| Vitamin D intake (μg/d) | 3.079 (2.5) | 3.650 (2.6) | 2.554 (2.4) | >0.999 |
| Serum calcium, vitamin D and parathyroid hormone | ||||
| Calcium (mg/dL) | 9.4 (0.4) | 9.5 (0.3) | 9.4 (0.5) | 0.503 |
| PTH (pg/mL) | 36.0 (20.9) | 41.5 (24.6) | 30.0 (14.9) | 0.205 |
| 25(OH)D (ng/mL) | 25.1 (10.5) | 25.8 (13.1) | 24.2 (7.3) | 0.894 |
| Bone turnover markers | ||||
| Serum osteocalcin (ng/mL) | 24.2 (8.2) | 22.6 (7.4) | 26.0 (8.7) | 0.247 |
| Urine NTx (mMBCE/mM Cr) | 55.1 (24.1) | 53.7 (26.8) | 56.7 (21.9) | 0.538 |
| Bone Mineral Density (BMD) | ||||
| Lumbar BMD (g/cm2) | 1.086 (0.152) | 1.077 (0.148) | 1.096 (0.163) | 0.728 |
| Femur neck BMD (g/cm2) | 0.859 (0.142) | 0.838 (0.117) | 0.881 (0.168) | 0.611 |
| Total hip BMD (g/cm2) | 0.930 (0.135) | 0.910 (0.104) | 0.951 (0.165) | 0.810 |
| Lifestyle | ||||
| Exercise/day (min) | 60.9 (6.8) | 65.8 (11.8) | 55.0 (5.0) | 0.872 |
| Smoking, Yes (n) | 25 | 0 | 0 | |
| Alcohol drinking, Yes (n) | 8 | 4 | 4 | 0.072 # |
| Regular exercise, Yes (n) | 22 | 12 | 10 | <0.001 # |
| Variables | Treatment | Control |
|---|---|---|
| Calcium and vitamin D content | ||
| Curry (200 g/serv.) | ||
| Calcium (mg/serv.) | 740.1 (23.4) | 101.4 (18.9) |
| Vitamin D (µg/serv.) | 16.10 (0.62) | ND |
| Black bean sauce (200 g/serv.) | ||
| Calcium (mg/serv.) | 600.9 (13.5) | 130.1 (6.08) |
| Vitamin D (µg/serv.) | 29.95 (1.80) | ND |
| Sweet pumpkin porridge (285 g/serv.) | ||
| Calcium (mg/serv.) | 580.7 (75.41) | 85.5 (1.21) |
| Vitamin D (µg/serv.) | 26.27 (0.70) | ND |
| Average | ||
| Calcium (mg/serv.) | 609.4 (33.2) | 129.2 (6.54) |
| Vitamin D (µg/serv.) | 24.10 (0.66) | ND |
| Carotenoid content | ||
| Curry (200 g/serv.) | ||
| Lycopene (mg/serv.) | 6.608 (0.049) | ND |
| Sweet pumpkin porridge (285 g/serv.) | ||
| Lutein (mg/serv.) | 6.809 (0.056) | 7.008 (0.044) |
| β-carotene (mg/serv.) | 6.211 (0.032) | 6.514 (0.086) |
| Variables | Treatment (n = 13) | Control (n = 12) | 95% CI | p-Value |
|---|---|---|---|---|
| ΔPTH (pg/mL) | −3.9 (18.4) | 5.8 (7.3) | −2.534~22.016 | 0.093 |
| Δ25(OH)D (ng/mL) | −1.9 (9.5) | −3.6 (6.7) | −8.736~5.051 | 0.574 |
| ΔOsteocalcin (ng/mL) | 1.9 (5.7) | 0.5 (6.1) | −6.347~3.400 | 0.650 |
| ΔNTx (mMBCE/mM Cr) | −6.8 (17.3) | −3.2 (13.9) | −9.399~16.758 | 0.769 |
| ΔUrine calcium/Creatinine | 0.003 (0.088) | −0.016 (0.076) | −0.087~0.049 | 0.769 |
| ΔLumbar BMD (g/cm2) | −0.013 (0.022) | −0.024 (0.037) | −0.121~0.139 | 0.320 |
| ΔFemur neck BMD (g/cm2) | −0.004 (0.018) | −0.023 (0.021) | −0.035~−0.002 | 0.035 |
| ΔTotal hip BMD (g/cm2) | −0.005 (0.015) | −0.001 (0.015) | −0.062~0.155 | 0.406 |
| Mean Values at 12 m/Δ | Treatment (n = 5) | Control (n = 6) | p-Value |
|---|---|---|---|
| PTH (pg/mL)/ΔPTH | 51.8 (11.9)/12.0 (19.2) | 41.8 (22.1)/15.3 (14.2) | 0.537/0.792 |
| 25(OH)D (ng/mL)/Δ25(OH)D | 24.9 (3.6)/−6.9 (18.0) | 17.8 (4.2)/−2.6 (5.4) | 0.017/0.537 |
| Osteocalcin (ng/mL)/ΔOsteocalcin | 21.3 (9.1)/1.2 (7.9) | 28.1 (9.3)/0.5 (7.0) | 0.177/1.000 |
| NTx (mMBCE/mM Cr)/ΔNTx | 62.0 (25.2)/14.2 (19.1) | 72.8 (16.8)/5.7 (16.7) | 0.537/0.329 |
| Urine calcium/Creatinine/ΔCa/Cr | 0.190 (0.064)/−0.008 (0.119) | 0.132 (0.039)/−0.003 (0.072) | 0.247/0.931 |
| Lumbar BMD/ΔL-BMD (g/cm2) | 1.071 (0.099)/−0.010 (0.028) | 1.120 (0.196)/−0.035 (0.032) | 0.931/0.247 |
| Femur neck BMD/ΔFemur neck BMD | 0.832 (0.137)/−0.007 (0.019) | 0.887 (0.186)/−0.033 (0.020) | 0.792/0.052 |
| Total hip BMD/ΔTotal hip BMD | 0.908 (0.128)/0.007 (0.021) | 0.982 (0.194)/−0.020 (0.028) | 0.931/0.329 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Joo, N.-S.; Shin, S.-H.; Kim, K.-N.; Lee, S.-H.; Jung, S.; Yeum, K.-J. Home Meal Replacement Fortified with Eggshell Powder and Vitamin D Prevents Bone Loss in Postmenopausal Women: A Randomized, Double-Blind, Controlled Study. Nutrients 2024, 16, 1152. https://doi.org/10.3390/nu16081152
Joo N-S, Shin S-H, Kim K-N, Lee S-H, Jung S, Yeum K-J. Home Meal Replacement Fortified with Eggshell Powder and Vitamin D Prevents Bone Loss in Postmenopausal Women: A Randomized, Double-Blind, Controlled Study. Nutrients. 2024; 16(8):1152. https://doi.org/10.3390/nu16081152
Chicago/Turabian StyleJoo, Nam-Seok, So-Hui Shin, Kyu-Nam Kim, Seok-Hoon Lee, Susie Jung, and Kyung-Jin Yeum. 2024. "Home Meal Replacement Fortified with Eggshell Powder and Vitamin D Prevents Bone Loss in Postmenopausal Women: A Randomized, Double-Blind, Controlled Study" Nutrients 16, no. 8: 1152. https://doi.org/10.3390/nu16081152