
Association between Urinary Sodium Excretion and Body Fat in School-Aged Children: Insights from the ARIA Study

 , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
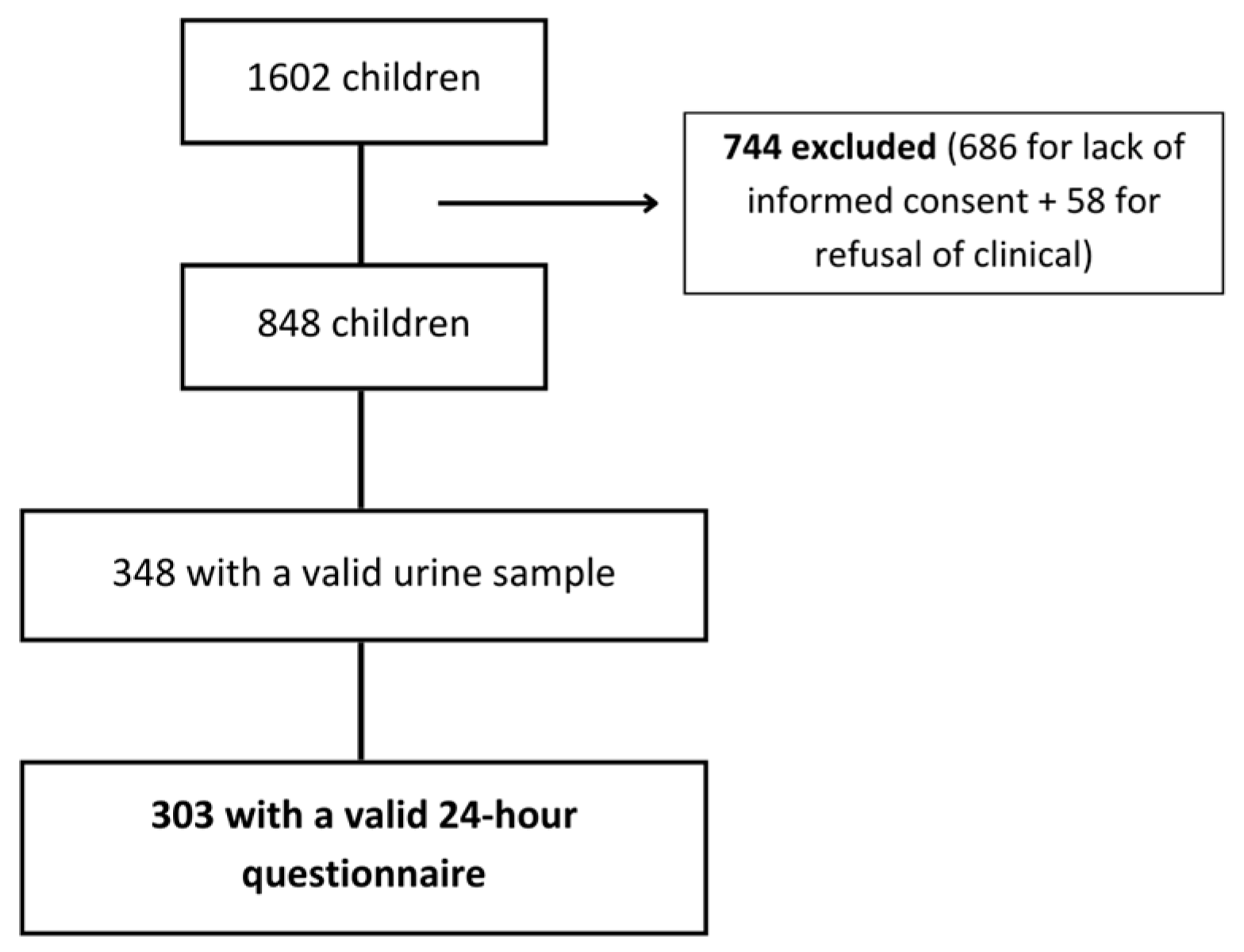
2.2. Participants and Study Design
2.3. Participant Assessment
2.3.1. Total Energy Intake Assessment
2.3.2. 24 h Urine Collection
2.3.3. Anthropometric Measurements and Body Fat Mass Percentage
2.3.4. Other Covariates
2.3.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hassapidou, M.; Vlassopoulos, A.; Kalliostra, M.; Govers, E.; Mulrooney, H.; Ells, L.; Salas, X.R.; Muscogiuri, G.; Darleska, T.H.; Busetto, L.; et al. Euroapean Association for the Study of Obesity Position Statement on Medical Nutrition Therapy for the Management of Overweight and Obesity in Adults Developed in Collaboration with the European Federation of the Associations of Dietitians. Obes. Facts 2023, 16, 11–28. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.D.; Fu, E.; Kobayashi, M.A. Prevention and Management of Childhood Obesity and Its Psychological and Health Comorbidities. Annu. Rev. Clin. Psychol. 2020, 16, 351–378. [Google Scholar] [CrossRef] [PubMed]
- Wójcik, M.; Kozioł-Kozakowska, A. Obesity, Sodium Homeostasis, and Arterial Hypertension in Children and Adolescents. Nutrients 2021, 13, 4032. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Li, J.; Macgregor, G.A. Effect of longer term modest salt reduction on blood pressure: Cochrane systematic review and meta-analysis of randomised trials. BMJ 2013, 346, f1325. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; MacGregor, G.A. Salt reduction lowers cardiovascular risk: Meta-analysis of outcome trials. Lancet 2011, 378, 380–382. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.A.; Kraak, V.I.; Allender, S.; Atkins, V.J.; Baker, P.I.; Bogard, J.R.; Brinsden, H.; Calvillo, A.; De Schutter, O.; Devarajan, R.; et al. The Global Syndemic of Obesity, Undernutrition, and Climate Change: The Lancet Commission report. Lancet 2019, 393, 791–846. [Google Scholar] [CrossRef] [PubMed]
- Puma, A.; Pecoraro, L.; Salvottini, C.; Carbonare, L.D.; Piacentini, G.; Pietrobelli, A. Parental Perceptions and Concerns Related to the Consequences of Pediatric Obesity: Feeling or Real Problem? Endocr. Metab. Immune Disord. Drug Targets 2023, 23, 1380–1391. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; MacGregor, G.A. A comprehensive review on salt and health and current experience of worldwide salt reduction programmes. J. Human. Hypertens. 2009, 23, 363–384. [Google Scholar] [CrossRef] [PubMed]
- Rito, A.; Mendes, S.; Figueira, I.; Faria, M.d.C.; Carvalho, R.; Santos, T.; Cardoso, S.; Feliciano, E.; Silvério, R.; Sancho, T.S. Childhood Obesity Surveillance Initiative: COSI Portugal 2022. 2023. Available online: https://repositorio.insa.pt/handle/10400.18/8630 (accessed on 10 April 2024).
- Golpour-Hamedani, S.; Rafie, N.; Pourmasoumi, M.; Morteza Safavi, S.; Mohammadifard, N. Sodium and potassium intakes and adiposity among Iranian pre-adolescents and adolescents: A cross-sectional study. Nutr. J. 2022, 21, 23. [Google Scholar] [CrossRef]
- Rahman, M.J.; Parvez, S.M.; Rahman, M.; He, F.J.; Cunningham, S.A.; Narayan, K.M.V.; Abedin, J.; Naser, A.M. Urinary Sodium Excretion and Obesity Markers among Bangladeshi Adult Population: Pooled Data from Three Cohort Studies. Nutrients 2022, 14, 3000. [Google Scholar] [CrossRef]
- Grimes, C.A.; Riddell, L.J.; Campbell, K.J.; Nowson, C.A. Dietary salt intake, sugar-sweetened beverage consumption, and obesity risk. Pediatrics 2013, 131, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Liu, W.; Bi, S.; Zhou, L.; Li, L. Association between minerals intake and childhood obesity: A cross-sectional study of the NHANES database in 2007-2014. PLoS ONE 2023, 18, e0295765. [Google Scholar] [CrossRef]
- He, F.J.; Marrero, N.M.; MacGregor, G.A. Salt intake is related to soft drink consumption in children and adolescents: A link to obesity? Hypertension 2008, 51, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; He, F.J.; MacGregor, G.A. High salt intake: Independent risk factor for obesity? Hypertension 2015, 66, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Pollock, N.K.; Kotak, I.; Gutin, B.; Wang, X.; Bhagatwala, J.; Parikh, S.; Harshfield, G.A.; Dong, Y. Dietary sodium, adiposity, and inflammation in healthy adolescents. Pediatrics 2014, 133, e635–e642. [Google Scholar] [CrossRef]
- Murakami, K.; Livingstone, M.B.; Sasaki, S.; Uenishi, K. Ability of self-reported estimates of dietary sodium, potassium and protein to detect an association with general and abdominal obesity: Comparison with the estimates derived from 24 h urinary excretion. Br. J. Nutr. 2015, 113, 1308–1318. [Google Scholar] [CrossRef]
- Libuda, L.; Kersting, M.; Alexy, U. Consumption of dietary salt measured by urinary sodium excretion and its association with body weight status in healthy children and adolescents. Public Health Nutr. 2012, 15, 433–441. [Google Scholar] [CrossRef]
- Yoon, Y.S.; Oh, S.W. Sodium density and obesity; the Korea National Health and Nutrition Examination Survey 2007-2010. Eur. J. Clin. Nutr. 2013, 67, 141–146. [Google Scholar] [CrossRef]
- Ellison, R.C.; Sosenko, J.M.; Harper, G.P.; Gibbons, L.; Pratter, F.E.; Miettinen, O.S. Obesity, sodium intake, and blood pressure in adolescents. Hypertension 1980, 2 Pt 2, 78–82. [Google Scholar] [CrossRef]
- Larsen, S.C.; Ängquist, L.; Sørensen, T.I.; Heitmann, B.L. 24h urinary sodium excretion and subsequent change in weight, waist circumference and body composition. PLoS ONE 2013, 8, e69689. [Google Scholar] [CrossRef]
- Lahti-Koski, M.; Gill, T. Defining childhood obesity. In Obesity in Childhood and Adolescence; Karger Publishers: Basel, Switzerland, 2004; Volume 9, pp. 1–19. [Google Scholar]
- Gray, D.S.; Fujioka, K. Use of relative weight and Body Mass Index for the determination of adiposity. J. Clin. Epidemiol. 1991, 44, 545–550. [Google Scholar] [CrossRef]
- Wells, J.C. Commentary: The paradox of body mass index in obesity assessment: Not a good index of adiposity, but not a bad index of cardio-metabolic risk. Int. J. Epidemiol. 2014, 43, 672–674. [Google Scholar] [CrossRef]
- Javed, A.; Jumean, M.; Murad, M.H.; Okorodudu, D.; Kumar, S.; Somers, V.K.; Sochor, O.; Lopez-Jimenez, F. Diagnostic performance of body mass index to identify obesity as defined by body adiposity in children and adolescents: A systematic review and meta-analysis. Pediatr. Obes. 2015, 10, 234–244. [Google Scholar] [CrossRef]
- Zeng, Q.; Dong, S.Y.; Sun, X.N.; Xie, J.; Cui, Y. Percent body fat is a better predictor of cardiovascular risk factors than body mass index. Braz. J. Med. Biol. Res. 2012, 45, 591–600. [Google Scholar] [CrossRef] [PubMed]
- Romero-Corral, A.; Somers, V.K.; Sierra-Johnson, J.; Thomas, R.J.; Collazo-Clavell, M.L.; Korinek, J.; Allison, T.G.; Batsis, J.A.; Sert-Kuniyoshi, F.H.; Lopez-Jimenez, F. Accuracy of body mass index in diagnosing obesity in the adult general population. Int. J. Obes. 2008, 32, 959–966. [Google Scholar] [CrossRef]
- Oliosa, P.R.; Zaniqueli, D.; Alvim, R.O.; Barbosa, M.C.R.; Mill, J.G. Body fat percentage is better than indicators of weight status to identify children and adolescents with unfavorable lipid profile. J. Pediatr. 2019, 95, 112–118. [Google Scholar] [CrossRef]
- Fang, K.; He, Y.; Fang, Y.; Lian, Y. Relationship of Sodium Intake with Overweight/Obesity among Chinese Children and Adolescents: Data from the CNNHS 2010-2012. Int. J. Environ. Res. Public Health 2021, 18, 4551. [Google Scholar] [CrossRef]
- Zhao, L.; Ogden, C.L.; Yang, Q.; Jackson, S.L.; Loria, C.M.; Galuska, D.A.; Wiltz, J.L.; Merritt, R.; Cogswell, M.E. Association of Usual Sodium Intake with Obesity Among US Children and Adolescents, NHANES 2009–2016. Obesity 2021, 29, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Mendes, F.C.; Paciência, I.; Cavaleiro Rufo, J.; Farraia, M.; Silva, D.; Padrão, P.; Delgado, L.; Garcia-Larsen, V.; Moreira, A.; Moreira, P. Higher diversity of vegetable consumption is associated with less airway inflammation and prevalence of asthma in school-aged children. Pediatr. Allergy Immunol. 2021, 32, 925–936. [Google Scholar] [CrossRef]
- Walker, J.L.; Ardouin, S.; Burrows, T. The validity of dietary assessment methods to accurately measure energy intake in children and adolescents who are overweight or obese: A systematic review. Eur. J. Clin. Nutr. 2018, 72, 185–197. [Google Scholar] [CrossRef]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake:basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1119–1130. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, A.M.; Willett, W.C. Trends in 24-h urinary sodium excretion in the United States, 1957-2003: A systematic review. Am. J. Clin. Nutr. 2010, 92, 1172–1180. [Google Scholar] [CrossRef] [PubMed]
- Preuss, H.G.; Clouatre, D.L. Sodium, Chloride, and Potassium. In Present Knowledge in Nutrition; International Life Sciences Institute: Washington, DC, USA, 2012; pp. 475–492. [Google Scholar] [CrossRef]
- Remer, T.; Neubert, A.; Maser-Gluth, C. Anthropometry-based reference values for 24-h urinary creatinine excretion during growth and their use in endocrine and nutritional research. Am. J. Clin. Nutr. 2002, 75, 561–569. [Google Scholar] [CrossRef]
- Chen, S.L.; Dahl, C.; Meyer, H.E.; Madar, A.A. Estimation of Salt Intake Assessed by 24-Hour Urinary Sodium Excretion among Somali Adults in Oslo, Norway. Nutrients 2018, 10, 900. [Google Scholar] [CrossRef] [PubMed]
- de Castro Mendes, F.; Paciência, I.; Rufo, J.C.; Farraia, M.; Silva, D.; Padrão, P.; Delgado, L.; Garcia-Larsen, V.; Moreira, A.; Moreira, P. Increasing Vegetable Diversity Consumption Impacts the Sympathetic Nervous System Activity in School-Aged Children. Nutrients 2021, 13, 1456. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, H.D.; Cole, T.J.; Fry, T.; Jebb, S.A.; Prentice, A.M. Body fat reference curves for children. Int. J. Obes. 2006, 30, 598–602. [Google Scholar] [CrossRef] [PubMed]
- Moreira, P.; Santos, S.; Padrão, P.; Cordeiro, T.; Bessa, M.; Valente, H.; Barros, R.; Teixeira, V.; Mitchell, V.; Lopes, C.; et al. Food patterns according to sociodemographics, physical activity, sleeping and obesity in Portuguese children. Int. J. Environ. Res. Public Health 2010, 7, 1121–1138. [Google Scholar] [CrossRef] [PubMed]
- Elsenburg, L.K.; Rieckmann, A.; Nguyen, T.L.; Bengtsson, J.; Andersen, A.N.; Taylor-Robinson, D.; Lange, T.; Rod, N.H. Mediation of the parental education gradient in early adult mortality by childhood adversity: A population-based cohort study of more than 1 million children. Lancet Public Health 2022, 7, e146–e155. [Google Scholar] [CrossRef]
- Yi, S.S.; Kansagra, S.M. Associations of Sodium Intake with Obesity, Body Mass Index, Waist Circumference, and Weight. Am. J. Prev. Med. 2014, 46, e53–e55. [Google Scholar] [CrossRef]
- Yoo, B.M.; Kim, M.; Kang, M.J. Association between childhood obesity and familial salt intake: Analysis of data from Korean National Health and Nutrition Examination Survey, 2014–2017. Endocr. J. 2021, 68, 1127–1134. [Google Scholar] [CrossRef]
- Lee, S.K.; Kim, M.K. Relationship of sodium intake with obesity among Korean children and adolescents: Korea National Health and Nutrition Examination Survey. Br. J. Nutr. 2016, 115, 834–841. [Google Scholar] [CrossRef] [PubMed]
- Fonseca-Alaniz, M.H.; Brito, L.C.; Borges-Silva, C.N.; Takada, J.; Andreotti, S.; Lima, F.B. High dietary sodium intake increases white adipose tissue mass and plasma leptin in rats. Obesity 2007, 15, 2200–2208. [Google Scholar] [CrossRef] [PubMed]
- Fonseca-Alaniz, M.H.; Takada, J.; Andreotti, S.; de Campos, T.B.; Campaña, A.B.; Borges-Silva, C.N.; Lima, F.B. High sodium intake enhances insulin-stimulated glucose uptake in rat epididymal adipose tissue. Obesity 2008, 16, 1186–1192. [Google Scholar] [CrossRef] [PubMed]
- Shore, A.C.; Markandu, N.D.; Sagnella, G.A.; Singer, D.R.; Forsling, M.L.; Buckley, M.G.; Sugden, A.L.; MacGregor, G.A. Endocrine and renal response to water loading and water restriction in normal man. Clin. Sci. 1988, 75, 171–177. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Markandu, N.D.; Sagnella, G.A.; de Wardener, H.E.; MacGregor, G.A. Plasma sodium: Ignored and underestimated. Hypertension 2005, 45, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Nowell, A.; Torres, S.J.; Hall, S.J.; Keske, M.A.; Torpy, D.J.; Parker, L.; Betik, A.C.; Turner, A.I. Is high salt intake inducing obesity via production of cortisol? A novel working hypothesis and pilot study. Eur. J. Nutr. 2024. [Google Scholar] [CrossRef]
- Wellens, R.I.; Roche, A.F.; Khamis, H.J.; Jackson, A.S.; Pollock, M.L.; Siervogel, R.M. Relationships between the Body Mass Index and body composition. Obes. Res. 1996, 4, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Strain, G.W.; Zumoff, B. The relationship of weight-height indices of obesity to body fat content. J. Am. Coll. Nutr. 1992, 11, 715–718. [Google Scholar] [CrossRef]
- Segal, K.R.; Dunaif, A.; Gutin, B.; Albu, J.; Nyman, A.; Pi-Sunyer, F.X. Body composition, not body weight, is related to cardiovascular disease risk factors and sex hormone levels in men. J. Clin. Investig. 1987, 80, 1050–1055. [Google Scholar] [CrossRef]
- Romero-Corral, A.; Somers, V.K.; Sierra-Johnson, J.; Korenfeld, Y.; Boarin, S.; Korinek, J.; Jensen, M.D.; Parati, G.; Lopez-Jimenez, F. Normal weight obesity: A risk factor for cardiometabolic dysregulation and cardiovascular mortality. Eur. Heart J. 2010, 31, 737–746. [Google Scholar] [CrossRef]
- Garn, S.M.; LaVelle, M.; Rosenberg, K.R.; Hawthorne, V.M. Maturational timing as a factor in female fatness and obesity. Am. J. Clin. Nutr. 1986, 43, 879–883. [Google Scholar] [CrossRef] [PubMed]
- Norgan, N.G. Relative sitting height and the interpretation of the body mass index. Ann. Hum. Biol. 1994, 21, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M.; Shepherd, J.A.; Looker, A.C.; Graubard, B.I.; Borrud, L.G.; Ogden, C.L.; Harris, T.B.; Everhart, J.E.; Schenker, N. Comparisons of percentage body fat, body mass index, waist circumference, and waist-stature ratio in adults. Am. J. Clin. Nutr. 2009, 89, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Turck, D.; Castenmiller, J.; de Henauw, S.; Hirsch-Ernst, K.I.; Kearney, J.; Knutsen, H.K.; Maciuk, A.; Mangelsdorf, I.; McArdle, H.J.; Pelaez, C.; et al. Dietary reference values for sodium. EFSA J. 2019, 17, e05778. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.; Castro Mendes, F.; Padrão, P.; Delgado, L.; Barros, R.; Rufo, J.C.; Silva, D.; Moreira, A.; Moreira, P. Does the Mediterranean Dietary Pattern Promote Lower Sodium Urinary Excretion in Children? Children 2023, 10, 1478. [Google Scholar] [CrossRef] [PubMed]
- Martin-Calvo, N.; Moreno-Galarraga, L.; Martinez-Gonzalez, M.A. Association between Body Mass Index, Waist-to-Height Ratio and Adiposity in Children: A Systematic Review and Meta-Analysis. Nutrients 2016, 8, 512. [Google Scholar] [CrossRef] [PubMed]
- Mei, Z.; Grummer-Strawn, L.M.; Pietrobelli, A.; Goulding, A.; Goran, M.I.; Dietz, W.H. Validity of body mass index compared with other body-composition screening indexes for the assessment of body fatness in children and adolescents. Am. J. Clin. Nutr. 2002, 75, 978–985. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; Dorosty, A.R.; Emmett, P.M. Identification of the obese child: Adequacy of the body mass index for clinical practice and epidemiology. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1623–1627. [Google Scholar] [CrossRef] [PubMed]
- Eisenmann, J.C.; Heelan, K.A.; Welk, G.J. Assessing body composition among 3- to 8-year-old children: Anthropometry, BIA, and DXA. Obes. Res. 2004, 12, 1633–1640. [Google Scholar] [CrossRef]
- Sung, R.Y.; Lau, P.; Yu, C.W.; Lam, P.K.; Nelson, E.A. Measurement of body fat using leg to leg bioimpedance. Arch. Dis. Child. 2001, 85, 263–267. [Google Scholar] [CrossRef]
- Hosking, J.; Metcalf, B.S.; Jeffery, A.N.; Voss, L.D.; Wilkin, T.J. Validation of foot-to-foot bioelectrical impedance analysis with dual-energy X-ray absorptiometry in the assessment of body composition in young children: The EarlyBird cohort. Br. J. Nutr. 2006, 96, 1163–1168. [Google Scholar] [CrossRef]
- Pietrobelli, A.; Rubiano, F.; St-Onge, M.P.; Heymsfield, S.B. New bioimpedance analysis system: Improved phenotyping with whole-body analysis. Eur. J. Clin. Nutr. 2004, 58, 1479–1484. [Google Scholar] [CrossRef]
- Parker, L.; Reilly, J.J.; Slater, C.; Wells, J.C.; Pitsiladis, Y. Validity of six field and laboratory methods for measurement of body composition in boys. Obes. Res. 2003, 11, 852–858. [Google Scholar] [CrossRef]
- Tyrrell, V.J.; Richards, G.; Hofman, P.; Gillies, G.F.; Robinson, E.; Cutfield, W.S. Foot-to-foot bioelectrical impedance analysis: A valuable tool for the measurement of body composition in children. Int. J. Obes. Relat. Metab. Disord. 2001, 25, 273–278. [Google Scholar] [CrossRef]
- Jebb, S.A.; Cole, T.J.; Doman, D.; Murgatroyd, P.R.; Prentice, A.M. Evaluation of the novel Tanita body-fat analyser to measure body composition by comparison with a four-compartment model. Br. J. Nutr. 2000, 83, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Wright, C.M.; Emmett, P.M.; Ness, A.R.; Reilly, J.J.; Sherriff, A. Tracking of obesity and body fatness through mid-childhood. Arch. Dis. Child. 2010, 95, 612–617. [Google Scholar] [CrossRef] [PubMed]
- Goldfield, G.S.; Cloutier, P.; Mallory, R.; Prud’homme, D.; Parker, T.; Doucet, E. Validity of foot-to-foot bioelectrical impedance analysis in overweight and obese children and parents. J. Sports Med. Phys. Fit. 2006, 46, 447–453. [Google Scholar]
- Brambilla, P.; Bedogni, G.; Moreno, L.A.; Goran, M.I.; Gutin, B.; Fox, K.R.; Peters, D.M.; Barbeau, P.; De Simone, M.; Pietrobelli, A. Crossvalidation of anthropometry against magnetic resonance imaging for the assessment of visceral and subcutaneous adipose tissue in children. Int. J. Obes. 2006, 30, 23–30. [Google Scholar] [CrossRef]
- Savva, S.C.; Tornaritis, M.; Savva, M.E.; Kourides, Y.; Panagi, A.; Silikiotou, N.; Georgiou, C.; Kafatos, A. Waist circumference and waist-to-height ratio are better predictors of cardiovascular disease risk factors in children than body mass index. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1453–1458. [Google Scholar] [CrossRef]
- Kelishadi, R.; Gheiratmand, R.; Ardalan, G.; Adeli, K.; Mehdi Gouya, M.; Mohammad Razaghi, E.; Majdzadeh, R.; Delavari, A.; Shariatinejad, K.; Motaghian, M.; et al. Association of anthropometric indices with cardiovascular disease risk factors among children and adolescents: CASPIAN Study. Int. J. Cardiol. 2007, 117, 340–348. [Google Scholar] [CrossRef]
- Foster, E.; Bradley, J. Methodological considerations and future insights for 24-hour dietary recall assessment in children. Nutr. Res. 2018, 51, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef] [PubMed]
- Ortega, R.M.; Pérez-Rodrigo, C.; López-Sobaler, A.M. Dietary assessment methods: Dietary records. Nutr. Hosp. 2015, 31 (Suppl. S3), 38–45. [Google Scholar] [CrossRef]


{kind=link}
| Total, n = 303 (100%) | Non-Overweight/Non-Obese (p < 85th) | Overweight/Obese (p ≥ 85th) | p-Value | %BF (p < 85th) | %BF (p ≥ 85th) | p-Value | |
|---|---|---|---|---|---|---|---|
| Age (years), median (25th–75th) | 8 (8–9) | 8 (8–9) | 8 (8–9) | 0.911 | 8 (8–9) | 8 (8–9) | 0.153 |
| Sex, n (%) | |||||||
| Female | 141 (46.50%) | 110 (47.60%) | 31 (43.10%) | 0.498 | 103 (49.30%) | 36 (40.00%) | 0.140 |
| Male | 162 (53.50%) | 121 (54.20%) | 41 (56.90%) | 106 (50.70%) | 54 (60.00%) | ||
| Total Energy Intake (kcal), Median (25th–75th) | 2178.67 (1890.28–2510.45) | 2173.15 (1864.01–2519.32) | 2222.42 (1943.68–2491.09) | 0.518 | 2175.19 (1873.54–2519.66) | 2199.22 (1901.25–2507.39) | 0.829 |
| 24 h Urinary Sodium Excretion (mg), Median (25th–75th) | 2507.00 (1909.00–3151.00) | 2392.00 (1886.00–3059.00) | 2725.50 (2087.25–3680.00) | 0.016 * | 2300.00 (1863.00–3024.50) | 2760.00 (2236.75–3622.50) | 0.001 * |
| 24 h Urinary Potassium Excretion (mg), Median (25th–75th) | 1681.30 (1368.50–2111.40) | 1642.20 (1290.30–2072.30) | 1915.90 (1485.80–2189.60) | 0.020 * | 1642.20 (1290.30–2052.75) | 1720.40 (1466.25–2189.60) | 0.057 |
| Ratio Na/K | 2.52 (1.99–3.29) | 2.51 (2.00–3.26) | 2.60 (1.91–3.38) | 0.928 | 2.46 (1.98–3.21) | 2.66 (2.00–3.54) | 0.111 |
| Physical Activity, n (%) | |||||||
| <2 times/week | 131 (47.00%) | 100 (47.20%) | 31 (46.30%) | 0.985 | 85 (45.00%) | 44 (51.20%) | 0.622 |
| 2–3 times/week | 108 (38.70%) | 82 (38.70%) | 26 (38.80%) | 76 (40.20%) | 30 (34.90%) | ||
| ≥4 times/week | 40 (14.30%) | 30 (14.20%) | 10 (14.90%) | 28 (14.80%) | 12 (14.00%) | ||
| Parental education, n (%) | |||||||
| <9 years | 103 (37.30%) | 71 (33.80%) | 32 (48.50%) | 0.054 | 64 (34.00%) | 36 (42.90%) | 0.336 |
| 10–12 years | 71 (25.70%) | 54 (25.70%) | 17 (25.80%) | 49 (26.10%) | 21 (25.00%) | ||
| ≥12 years | 102 (37.00%) | 85 (40.50%) | 12 (25.80%) | 75 (39.90%) | 27 (32.10%) | ||
| Excreted Sodium (>2507 mg), Crude Model, OR (95% CI) | p-Value | Excreted Sodium (>2507 mg), Adjusted Model, aOR (95% CI) | p-Value | |
|---|---|---|---|---|
| Overweight/obese (p ≥ 85th) | 2.04 (1.18–3.50) | 0.010 * | 1.56 (0.82–2.96) | 0.172 |
| %BF (p ≥ 85th) | 2.62 (1.56–4.38) | <0.001 * | 2.89 (1.58–5.30) | <0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soares, A.P.; Rodrigues, M.; Padrão, P.; Gonçalves, C.; Moreira, A.; Moreira, P. Association between Urinary Sodium Excretion and Body Fat in School-Aged Children: Insights from the ARIA Study. Nutrients 2024, 16, 1197. https://doi.org/10.3390/nu16081197
Soares AP, Rodrigues M, Padrão P, Gonçalves C, Moreira A, Moreira P. Association between Urinary Sodium Excretion and Body Fat in School-Aged Children: Insights from the ARIA Study. Nutrients. 2024; 16(8):1197. https://doi.org/10.3390/nu16081197
Chicago/Turabian StyleSoares, Ana Patrícia, Mónica Rodrigues, Patrícia Padrão, Carla Gonçalves, André Moreira, and Pedro Moreira. 2024. "Association between Urinary Sodium Excretion and Body Fat in School-Aged Children: Insights from the ARIA Study" Nutrients 16, no. 8: 1197. https://doi.org/10.3390/nu16081197
APA StyleSoares, A. P., Rodrigues, M., Padrão, P., Gonçalves, C., Moreira, A., & Moreira, P. (2024). Association between Urinary Sodium Excretion and Body Fat in School-Aged Children: Insights from the ARIA Study. Nutrients, 16(8), 1197. https://doi.org/10.3390/nu16081197