
Higher Numbers of Family Meals and Social Eating Behavior Are Associated with Greater Self-Esteem among Adolescents: The EHDLA



Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Procedure
2.2. Measurements
2.2.1. Family Meals
2.2.2. Social Eating Behavior
2.2.3. Self-Esteem
2.2.4. Covariates
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leary, M.; Tangney, J. Handbook of Self and Identity, 2nd ed.; Guilford Press: New York, NY, USA, 2014; ISBN 978-1-4625-1537-0. [Google Scholar]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton Legacy Library, Princeton University Press: Princeton, NJ, USA, 2016; ISBN 978-1-4008-7613-6. [Google Scholar]
- Mann, M. Self-Esteem in a Broad-Spectrum Approach for Mental Health Promotion. Health Educ. Res. 2004, 19, 357–372. [Google Scholar] [CrossRef] [PubMed]
- Lerner, R.; Steinberg, L. Handbook of Adolescent Psychology, 1st ed.; Wiley: New York, NY, USA, 2009; ISBN 978-0-470-14920-1. [Google Scholar]
- Erikson, E.H. Identity: Youth and Crisis; Norton & Co.: Oxford; UK, 1968; ISBN 0-393-31144-9. [Google Scholar]
- Steinberg, L.; Morris, A.S. Adolescent Development. Annu. Rev. Psychol. 2001, 52, 83–110. [Google Scholar] [CrossRef] [PubMed]
- González Moreno, A.; Molero Jurado, M.D.M. Healthy Lifestyle in Adolescence: Associations with Stress, Self-Esteem and the Roles of School Violence. Healthcare 2023, 12, 63. [Google Scholar] [CrossRef] [PubMed]
- Fisberg, M.; Gioia, N.; Maximino, P. Transgenerational Transmission of Eating Habits. J. Pediatr. 2023, 100, S82–S87. [Google Scholar] [CrossRef] [PubMed]
- Higgs, S. Social Norms and Their Influence on Eating Behaviours. Appetite 2015, 86, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Absolom, S.; Roberts, A. Connecting with Others: The Meaning of Social Eating as an Everyday Occupation for Young People. J. Occup. Sci. 2011, 18, 339–346. [Google Scholar] [CrossRef]
- Krauss, S.; Orth, U.; Robins, R.W. Family Environment and Self-Esteem Development: A Longitudinal Study from Age 10 to 16. J. Personal. Soc. Psychol. 2020, 119, 457–478. [Google Scholar] [CrossRef] [PubMed]
- Keer, M.R.; Ballard, E.L. Are Family Meals as Good for Youth as We Think They Are? A Review of the Literature on Family Meals as They Pertain to Adolescent Risk Prevention. J. Youth Adolesc. 2013, 42, 943–963. [Google Scholar] [CrossRef]
- Harrison, M.E.; Norris, M.L.; Obeid, N.; Fu, M.; Weinstangel, H.; Sampson, M. Systematic Review of the Effects of Family Meal Frequency on Psychosocial Outcomes in Youth. Can. Fam. Physician 2015, 61, e96–e106. [Google Scholar]
- Neumark-Sztainer, D.; Story, M.; Ackard, D.; Moe, J.; Perry, C. The “Family Meal”: Views of Adolescents. J. Nutr. Educ. 2000, 32, 329–334. [Google Scholar] [CrossRef]
- Orth, U.; Robins, R.W.; Widaman, K.F. Life-Span Development of Self-Esteem and Its Effects on Important Life Outcomes. J. Pers. Soc. Psychol. 2012, 102, 1271–1288. [Google Scholar] [CrossRef] [PubMed]
- López-Gil, J.F. The Eating Healthy and Daily Life Activities (EHDLA) Study. Children 2022, 9, 370. [Google Scholar] [CrossRef] [PubMed]
- Neumark-Sztainer, D.; Larson, N.I.; Fulkerson, J.A.; Eisenberg, M.E.; Story, M. Family Meals and Adolescents: What Have We Learned from Project EAT (Eating Among Teens)? Public Health Nutr. 2010, 13, 1113–1121. [Google Scholar] [CrossRef]
- Larson, N.I.; Neumark-Sztainer, D.; Hannan, P.J.; Story, M. Family Meals during Adolescence Are Associated with Higher Diet Quality and Healthful Meal Patterns during Young Adulthood. J. Am. Diet. Assoc. 2007, 107, 1502–1510. [Google Scholar] [CrossRef] [PubMed]
- Martín-Albo, J.; Núñez, J.L.; Navarro, J.G.; Grijalvo, F. The Rosenberg Self-Esteem Scale: Translation and Validation in University Students. Span. J. Psychol. 2007, 10, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Currie, C.; Molcho, M.; Boyce, W.; Holstein, B.; Torsheim, T.; Richter, M. Researching Health Inequalities in Adolescents: The Development of the Health Behaviour in School-Aged Children (HBSC) Family Affluence Scale. Soc. Sci. Med. 2008, 66, 1429–1436. [Google Scholar] [CrossRef]
- de Onis, M. Development of a WHO Growth Reference for School-Aged Children and Adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Saint-Maurice, P.F.; Welk, G.J. Validity and Calibration of the Youth Activity Profile. PLoS ONE 2015, 10, e0143949. [Google Scholar] [CrossRef] [PubMed]
- Segura-Díaz, J.M.; Barranco-Ruiz, Y.; Saucedo-Araujo, R.G.; Aranda-Balboa, M.J.; Cadenas-Sanchez, C.; Migueles, J.H.; Saint-Maurice, P.F.; Ortega, F.B.; Welk, G.J.; Herrador-Colmenero, M.; et al. Feasibility and Reliability of the Spanish Version of the Youth Activity Profile Questionnaire (YAP-Spain) in Children and Adolescents. J. Sports Sci. 2021, 39, 801–807. [Google Scholar] [CrossRef]
- Maechler, M.; Rousseeuw, P.; Croux, C.; Todorov, V.; Ruckstuhl, A.; Salibian-Barrera, M.; Verbeke, T.; Koller, M.; Conceicao, E.L.; di Palma, M.A. Robustbase: Basic Robust Statistics. Available online: https://cran.r-project.org/web/packages/robustbase/index.html (accessed on 26 March 2024).
- Eckert, K.F.; Asbridge, M.; Campbell, L.A.; Stewart, S.; Bennett, M.; Loewen, O.K.; Veugelers, P.J.; Cahill, L.E. Meal Regularity Is Associated with Self-Esteem among Grade 5 Children. Am. J. Clin. Nutr. 2021, 113, 467–475. [Google Scholar] [CrossRef]
- Utter, J.; Larson, N.; Berge, J.M.; Eisenberg, M.E.; Fulkerson, J.A.; Neumark-Sztainer, D. Family Meals among Parents: Associations with Nutritional, Social and Emotional Wellbeing. Prev. Med. 2018, 113, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Fulkerson, J.A.; Strauss, J.; Neumark-Sztainer, D.; Story, M.; Boutelle, K. Correlates of Psychosocial Well-Being among Overweight Adolescents: The Role of the Family. J. Consult. Clin. Psychol. 2007, 75, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Fulkerson, J.A.; Story, M.; Mellin, A.; Leffert, N.; Neumark-Sztainer, D.; French, S.A. Family Dinner Meal Frequency and Adolescent Development: Relationships with Developmental Assets and High-Risk Behaviors. J. Adolesc. Health 2006, 39, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, M.E.; Olson, R.E.; Neumark-Sztainer, D.; Story, M.; Bearinger, L.H. Correlations Between Family Meals and Psychosocial Well-Being among Adolescents. Arch. Pediatr. Adolesc. Med. 2004, 158, 792. [Google Scholar] [CrossRef] [PubMed]
- Middleton, G.; Golley, R.K.; Patterson, K.A.; Coveney, J. The Family Meal Framework: A Grounded Theory Study Conceptualising the Work That Underpins the Family Meal. Appetite 2022, 175, 106071. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Blissett, J.; Higgs, S. Social Influences on Eating: Implications for Nutritional Interventions. Nutr. Res. Rev. 2013, 26, 166–176. [Google Scholar] [CrossRef]
- Harbec, M.-J.; Pagani, L.S. Associations between Early Family Meal Environment Quality and Later Well-Being in School-Age Children. J. Dev. Behav. Pediatr. 2018, 39, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Ikiz, F.E.; Cakar, F.S. Perceived Social Support and Self-Esteem in Adolescence. Procedia-Soc. Behav. Sci. 2010, 5, 2338–2342. [Google Scholar] [CrossRef]
- Felson, R.B.; Zielinski, M.A. Children’s Self-Esteem and Parental Support. J. Marriage Fam. 1989, 51, 727. [Google Scholar] [CrossRef]
- Huang, X.; Hu, N.; Yao, Z.; Peng, B. Family Functioning and Adolescent Depression: A Moderated Mediation Model of Self-Esteem and Peer Relationships. Front. Psychol. 2022, 13, 962147. [Google Scholar] [CrossRef]
- Ho, H.C.Y.; Mui, M.; Wan, A.; Yew, C.; Lam, T.H.; Chan, S.S.; Stewart, S.M. Family Meal Practices and Well-Being in Hong Kong: The Mediating Effect of Family Communication. J. Fam. Issues 2018, 39, 3835–3856. [Google Scholar] [CrossRef]
- Middleton, G.; Golley, R.; Patterson, K.; Le Moal, F.; Coveney, J. What Can Families Gain from the Family Meal? A Mixed-Papers Systematic Review. Appetite 2020, 153, 104725. [Google Scholar] [CrossRef] [PubMed]
- Szcześniak, M.; Bajkowska, I.; Czaprowska, A.; Sileńska, A. Adolescents’ Self-Esteem and Life Satisfaction: Communication with Peers as a Mediator. Int. J. Environ. Res. Public Health 2022, 19, 3777. [Google Scholar] [CrossRef] [PubMed]
- DuBois, D.L. Self-Esteem, Adolescence. In Encyclopedia of Primary Prevention and Health Promotion; Gullotta, T.P., Bloom, M., Kotch, J., Blakely, C., Bond, L., Adams, G., Browne, C., Klein, W., Ramos, J., Eds.; Springer: Boston, MA, USA, 2003; pp. 953–961. ISBN 978-1-4613-4961-7. [Google Scholar]
- Armstrong-Carter, E.; Telzer, E.H. Family Meals Buffer the Daily Emotional Risk Associated with Family Conflict. Dev. Psychol. 2020, 56, 2110–2120. [Google Scholar] [CrossRef] [PubMed]
- Cappellini, B.; Parsons, E. Sharing the Meal: Food Consumption and Family Identity. In Research in Consumer Behavior; Belk, R.W., Askegaard, S., Scott, L., Eds.; Emerald Group Publishing Limited: Bradford, UK, 2012; pp. 109–128. ISBN 978-1-78190-022-2. [Google Scholar]
- Masson, E.; Bubendorff, S.; Fraïssé, C. Toward New Forms of Meal Sharing? Collective Habits and Personal Diets. Appetite 2018, 123, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Martiny, S.E.; Rubin, M. Towards a Clearer Understanding of Social Identity Theory’s Self-Esteem Hypothesis. In Understanding Peace and Conflict through Social Identity Theory; McKeown, S., Haji, R., Ferguson, N., Eds.; Peace Psychology Book Series; Springer International Publishing: Cham, Switzerland; New York, NY, USA, 2016; pp. 19–32. ISBN 978-3-319-29867-2. [Google Scholar]
- Liu, J.; Thomas, J.M.; Higgs, S. The Relationship between Social Identity, Descriptive Social Norms and Eating Intentions and Behaviors. J. Exp. Soc. Psychol. 2019, 82, 217–230. [Google Scholar] [CrossRef]
- Klucharev, V.; Hytönen, K.; Rijpkema, M.; Smidts, A.; Fernández, G. Reinforcement Learning Signal Predicts Social Conformity. Neuron 2009, 61, 140–151. [Google Scholar] [CrossRef] [PubMed]
- Boothby, E.J.; Clark, M.S.; Bargh, J.A. Shared Experiences Are Amplified. Psychol. Sci. 2014, 25, 2209–2216. [Google Scholar] [CrossRef] [PubMed]
- Deci, E.L.; Sheinman, L.; Wheeler, L.; Hart, R. Rewards, Motivation, and Self-Esteem. Educ. Forum 1980, 44, 429–433. [Google Scholar] [CrossRef]
- Delormier, T.; Frohlich, K.L.; Potvin, L. Food and Eating as Social Practice—Understanding Eating Patterns as Social Phenomena and Implications for Public Health. Sociol. Health Illn. 2009, 31, 215–228. [Google Scholar] [CrossRef]
- Bijstra, J.O.; Jackson, S. Social Skills Training with Early Adolescents: Effects on Social Skills, Well-Being, Self-Esteem and Coping. Eur. J. Psychol. Educ. 1998, 13, 569–583. [Google Scholar] [CrossRef]
- Babakhani, N. The Effects of Social Skills Training on Self-Esteem and Aggression Male Adolescents. Procedia Soc. Behav. Sci. 2011, 30, 1565–1570. [Google Scholar] [CrossRef]
- Prior, A.-L.; Limbert, C. Adolescents’ Perceptions and Experiences of Family Meals. J. Child Health Care 2013, 17, 354–365. [Google Scholar] [CrossRef] [PubMed]
- Orth, U.; Robins, R.W. The Development of Self-Esteem. Curr. Dir. Psychol. Sci. 2014, 23, 381–387. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | Total * | |
|---|---|---|
| Age (years) | Median (IQR) | 14.0 (2.0) |
| Sex | Boys (%) | 310 (43.9) |
| Girls (%) | 396 (56.1) | |
| FAS-III (score) | Median (IQR) | 8.0 (3.0) |
| YAP-S physical activity (score) | Median (IQR) | 2.6 (0.9) |
| YAP-S sedentary behavior (score) | Median (IQR) | 2.6 (0.8) |
| Overall sleep duration (minutes) | Median (IQR) | 501.4 (71.8) |
| Body mass index (kg/m2) | Median (IQR) | 21.7 (6.0) |
| Body mass index (z-score) † | Median (IQR) | 0.0 (2.0) |
| Energy intake (kcal) | Median (IQR) | 2554.3 (1465.9) |
| Weekly family meals (number) | Median (IQR) | 14.0 (6.0) |
| Social eating behavior (score) ‡ | Median (IQR) | 10.0 (2.0) |
| Self-esteem (score) § | Median (IQR) | 26.0 (5.0) |
| Self-Esteem (Score) † | ||
|---|---|---|
| Predictor (continuous) | B (95% CI, p value) (unadjusted) | B (95% CI, p value) (adjusted ‡) |
| Family meals (per further meal) | 0.109 (0.045 to 0.173, p = 0.001) | 0.071 (0.008 to 0.133, p = 0.026) |
| Social eating behavior (per further point) | 0.270 (0.095 to 0.445, p = 0.003) | 0.259 (0.091 to 0.427, p = 0.003) |
| Predictor (categorical) | B (95% CI, p value) (unadjusted) | B (95% CI, p value) (adjusted ‡) |
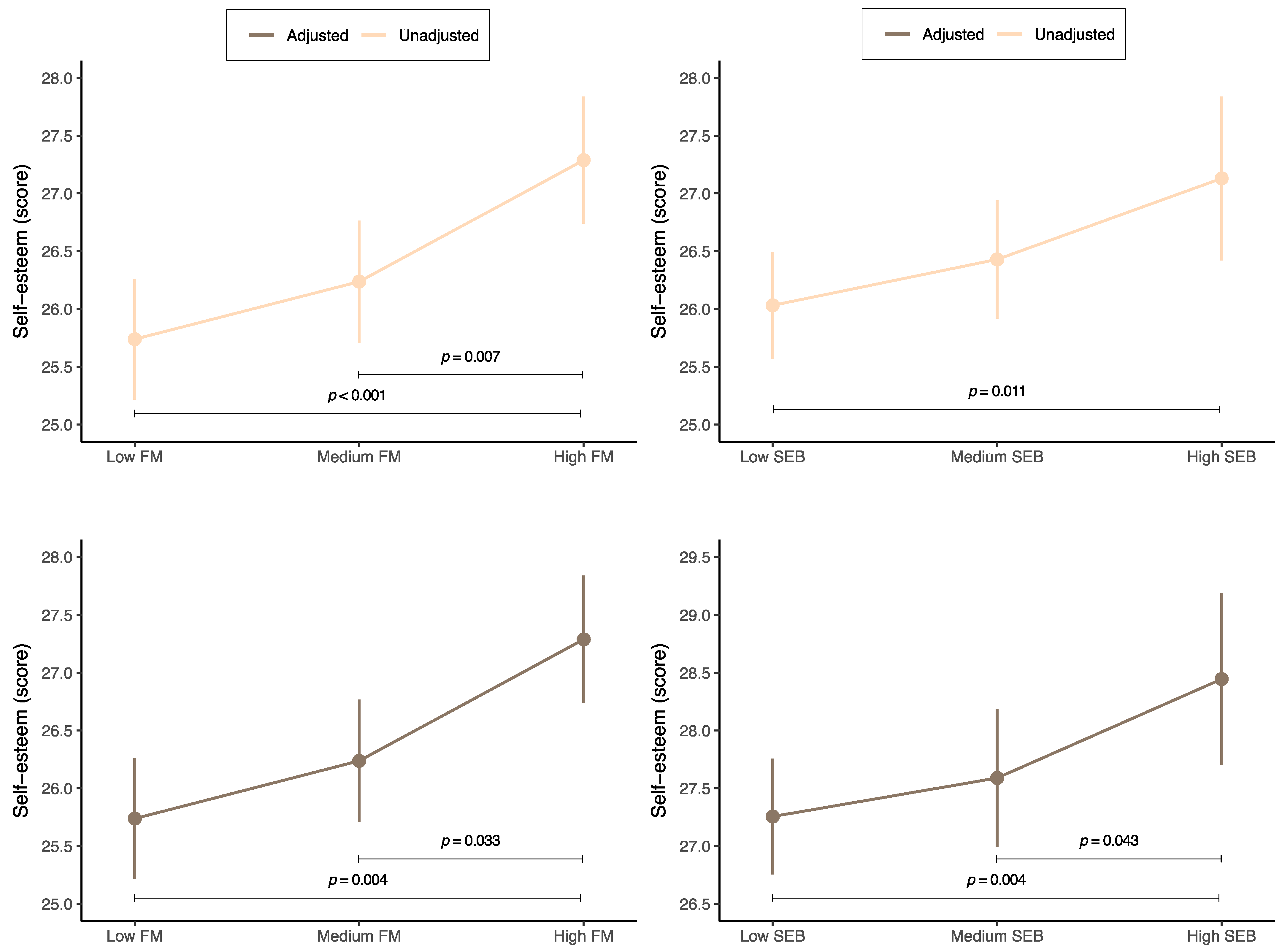
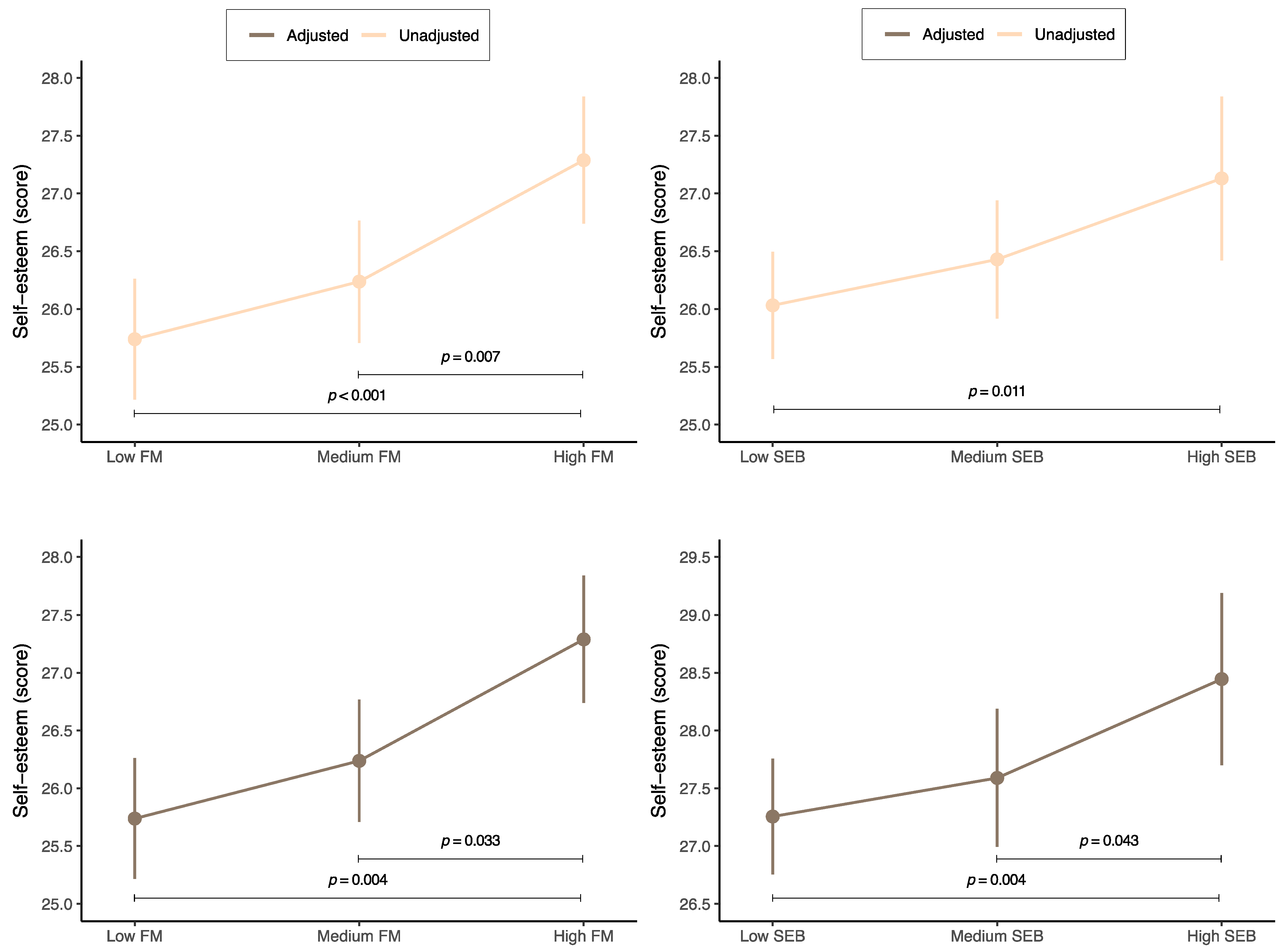
| Low number of family meals (0–11 weekly meals) | Reference | Reference |
| Medium number of family meals (12–15 weekly meals) | 0.499 (–0.244 to 1.242, p = 0.188) | 0.295 (–0.415 to 1.005, p = 0.415) |
| High number of family meals (16–21 weekly meals) | 1.550 (0.791 to 2.309, p < 0.001) | 1.100 (0.365 to 1.835, p = 0.004) |
| Low level of social eating behavior (3–8 points) | Reference | Reference |
| Medium level of social eating behavior (9–11 points) | 0.404 (–0.294 to 1.102, p = 0.258) | 0.336 (–0.328 to 1.000, p = 0.323) |
| High level of social eating behavior (12 points) | 1.120 (0.285 to 1.955, p = 0.009) | 1.190 (0.390 to 1.990, p = 0.004) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Gil, J.F.; Gutiérrez-Espinoza, H.; Manzano-Sánchez, D. Higher Numbers of Family Meals and Social Eating Behavior Are Associated with Greater Self-Esteem among Adolescents: The EHDLA. Nutrients 2024, 16, 1216. https://doi.org/10.3390/nu16081216
López-Gil JF, Gutiérrez-Espinoza H, Manzano-Sánchez D. Higher Numbers of Family Meals and Social Eating Behavior Are Associated with Greater Self-Esteem among Adolescents: The EHDLA. Nutrients. 2024; 16(8):1216. https://doi.org/10.3390/nu16081216
Chicago/Turabian StyleLópez-Gil, José Francisco, Héctor Gutiérrez-Espinoza, and David Manzano-Sánchez. 2024. "Higher Numbers of Family Meals and Social Eating Behavior Are Associated with Greater Self-Esteem among Adolescents: The EHDLA" Nutrients 16, no. 8: 1216. https://doi.org/10.3390/nu16081216
APA StyleLópez-Gil, J. F., Gutiérrez-Espinoza, H., & Manzano-Sánchez, D. (2024). Higher Numbers of Family Meals and Social Eating Behavior Are Associated with Greater Self-Esteem among Adolescents: The EHDLA. Nutrients, 16(8), 1216. https://doi.org/10.3390/nu16081216