
The Role of Lifestyle Intervention in Female Fertility: A Modifiable Factor for Preconception Health
 ,
,  and
and {kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Body Weight Management and Improvement of Fertility: Lifestyle Interventions
2.1. Diet and Improvement of Fertility
2.1.1. Pre-Treatment Dietary Patterns and Assisted Reproductive Technology (ART) Outcomes
2.1.2. Preconception Care Intervention Through Diet Normalization: In Vivo Animal Models
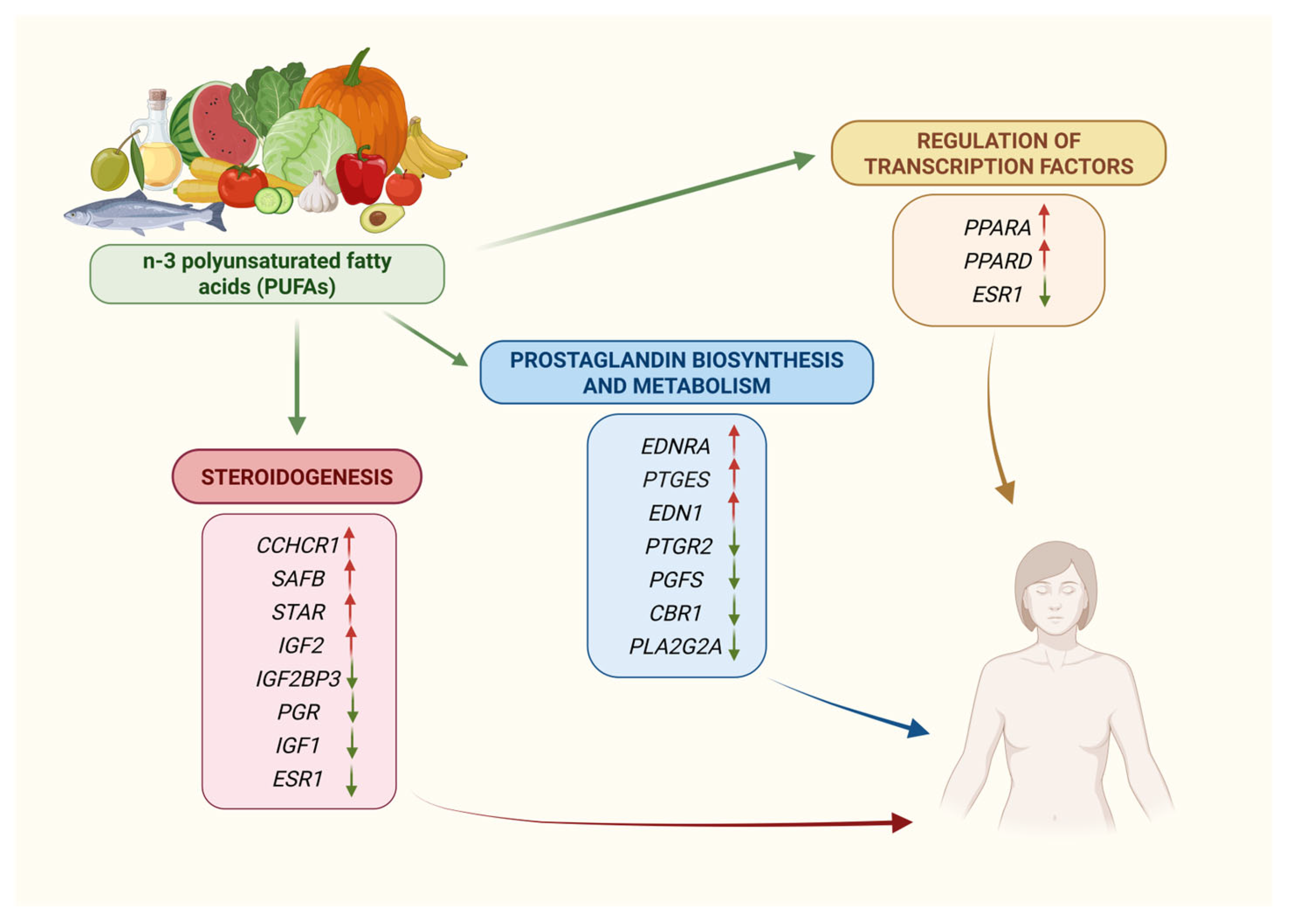
2.2. Diet and Modulation of Gene Expression: The Effect of n-3 Polyunsaturated Fatty Acids (PUFAs) on the Endometrium
Impact of n-3 Polyunsaturated Fatty Acid Supplementation on Endometrial Gene Expression
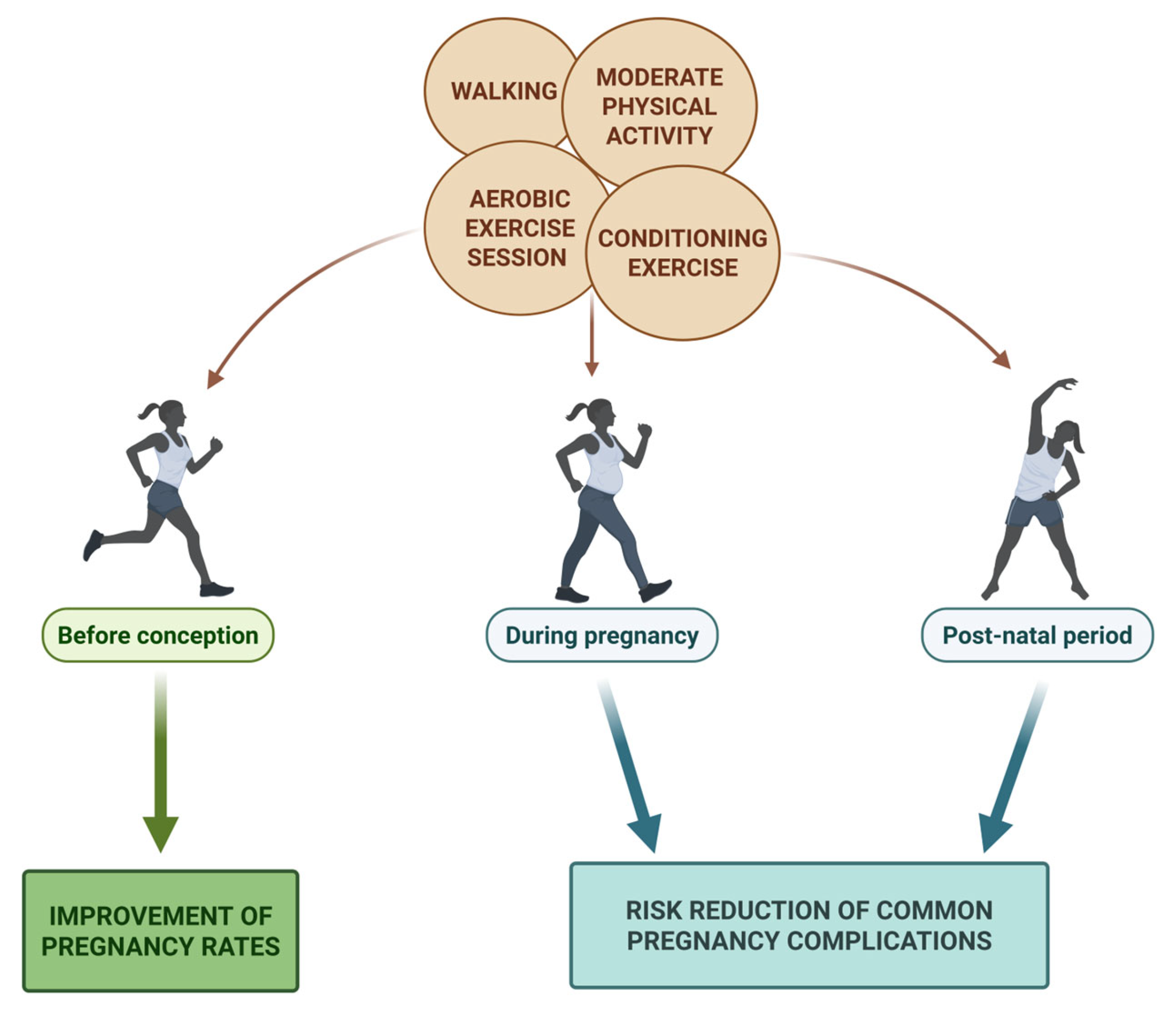
2.3. Physical Activity
3. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pisarska, M.D.; Chan, J.L.; Lawrenson, K.; Gonzalez, T.L.; Wang, E.T. Genetics and Epigenetics of Infertility and Treatments on Outcomes. J. Clin. Endocrinol. Metab. 2019, 104, 1871–1886. [Google Scholar] [CrossRef] [PubMed]
- Vander Borght, M.; Wyns, C. Fertility and infertility: Definition and epidemiology. Clin. Biochem. 2018, 62, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Konstantinidou, F.; Budani, M.C.; Sarra, A.; Stuppia, L.; Tiboni, G.M.; Gatta, V. Impact of Cigarette Smoking on the Expression of Oxidative Stress-Related Genes in Cumulus Cells Retrieved from Healthy Women Undergoing IVF. Int. J. Mol. Sci. 2021, 22, 13147. [Google Scholar] [CrossRef] [PubMed]
- Konstantinidou, F.; Stuppia, L.; Gatta, V. Looking Inside the World of Granulosa Cells: The Noxious Effects of Cigarette Smoke. Biomedicines 2020, 8, 309. [Google Scholar] [CrossRef]
- Sharma, R.; Biedenharn, K.R.; Fedor, J.M.; Agarwal, A. Lifestyle factors and reproductive health: Taking control of your fertility. Reprod. Biol. Endocrinol. 2013, 11, 66. [Google Scholar] [CrossRef]
- Monteiro, J.; Bicho, M.; Valente, A. The Contribution of Precision Nutrition Intervention in Subfertile Couples. Nutrients 2025, 17, 103. [Google Scholar] [CrossRef]
- Østensen, M. Preconception Counseling. Rheum. Dis. Clin. N. Am. 2017, 43, 189–199. [Google Scholar] [CrossRef]
- Chavarro, J.E.; Rich-Edwards, J.W.; Rosner, B.A.; Willett, W.C. Diet and lifestyle in the prevention of ovulatory disorder infertility. Obstet. Gynecol. 2007, 110, 1050–1058. [Google Scholar] [CrossRef]
- Della Torre, S.; Benedusi, V.; Fontana, R.; Maggi, A. Energy metabolism and fertility: A balance preserved for female health. Nat. Rev. Endocrinol. 2014, 10, 13–23. [Google Scholar] [CrossRef]
- Mircea, C.N.; Lujan, M.E.; Pierson, R.A. Metabolic fuel and clinical implications for female reproduction. J. Obstet. Gynaecol. Can. 2007, 29, 887–902. [Google Scholar] [CrossRef]
- Olive, D.L. Exercise and fertility: An update. Curr. Opin. Obstet. Gynecol. 2010, 22, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Harrison, C.L.; Brown, W.J.; Hayman, M.; Moran, L.J.; Redman, L.M. The Role of Physical Activity in Preconception, Pregnancy and Postpartum Health. Semin. Reprod. Med. 2016, 34, 28–37. [Google Scholar]
- Torkel, S.; Moran, L.; Wang, R.; Villani, A.; Mantzioris, E.; Norman, R.J.; Cowan, S. Barriers and enablers to a healthy lifestyle in people with infertility: A qualitative descriptive study. Reprod. Biol. Endocrinol. 2025, 23, 52. [Google Scholar] [CrossRef] [PubMed]
- Gonnella, F.; Konstantinidou, F.; Donato, M.; Gatta, D.M.P.; Peserico, A.; Barboni, B.; Stuppia, L.; Nothnick, W.B.; Gatta, V. The Molecular Link between Obesity and the Endometrial Environment: A Starting Point for Female Infertility. Int. J. Mol. Sci. 2024, 25, 6855. [Google Scholar] [CrossRef]
- Di Berardino, C.; Barceviciute, U.; Camerano Spelta Rapini, C.; Peserico, A.; Capacchietti, G.; Bernabò, N.; Russo, V.; Gatta, V.; Konstantinidou, F.; Donato, M.; et al. High-fat diet-negative impact on female fertility: From mechanisms to protective actions of antioxidant matrices. Front. Nutr. 2024, 11, 1415455. [Google Scholar] [CrossRef]
- Alesi, S.; Villani, A.; Mantzioris, E.; Takele, W.W.; Cowan, S.; Moran, L.J.; Mousa, A. Anti-Inflammatory Diets in Fertility: An Evidence Review. Nutrients 2022, 14, 3914. [Google Scholar] [CrossRef]
- Muffone, A.R.M.C.; de Oliveira Lübke, P.D.P.; Rabito, E.I. Mediterranean diet and infertility: A systematic review with meta-analysis of cohort studies. Nutr. Rev. 2023, 81, 775–789. [Google Scholar] [CrossRef]
- Twigt, J.M.; Bolhuis, M.E.; Steegers, E.A.; Hammiche, F.; van Inzen, W.G.; Laven, J.S.; Steegers-Theunissen, R.P. The preconception diet is associated with the chance of ongoing pregnancy in women undergoing IVF/ICSI treatment. Hum. Reprod. 2012, 27, 2526–2531. [Google Scholar] [CrossRef]
- Baroutis, D.; Kalampokas, T.; Katsianou, E.; Psarris, A.; Daskalakis, G.; Panoulis, K.; Eleftheriades, M. The Role of the Mediterranean Diet in Assisted Reproduction: A Literature Review. Nutrients 2024, 16, 2807. [Google Scholar] [CrossRef]
- Wathes, D.C.; Abayasekara, D.R.; Aitken, R.J. Polyunsaturated fatty acids in male and female reproduction. Biol. Reprod. 2007, 77, 190–201. [Google Scholar] [CrossRef]
- Lopes, C.N.; Cooke, R.F.; Reis, M.M.; Peres, R.F.; Vasconcelos, J.L. Strategic supplementation of calcium salts of polyunsaturated fatty acids to enhance reproductive performance of Bos indicus beef cows. J. Anim. Sci. 2011, 89, 3116–3124. [Google Scholar] [CrossRef] [PubMed]
- Childs, S.; Carter, F.; Lynch, C.O.; Sreenan, J.M.; Lonergan, P.; Hennessy, A.A.; Kenny, D.A. Embryo yield and quality following dietary supplementation of beef heifers with n-3 polyunsaturated fatty acids (PUFA). Theriogenology 2008, 70, 992–1003. [Google Scholar] [CrossRef]
- Darwich, A.S.; Neuhoff, S.; Jamei, M.; Rostami-Hodjegan, A. Interplay of metabolism and transport in determining oral drug absorption and gut wall metabolism: A simulation assessment using the “Advanced Dissolution, Absorption, Metabolism (ADAM)” model. Curr. Drug Metab. 2010, 11, 716–729. [Google Scholar] [CrossRef]
- Practice Committee of the American Society for Reproductive Medicine. Obesity and reproduction: A committee opinion. Fertil. Steril. 2021, 116, 1266–1285. [Google Scholar] [CrossRef]
- Fowler, J.R.; Jenkins, S.M.; Jack, B.W. Preconception Counseling. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2025. [Google Scholar]
- Vitek, W.S.; Hoeger, K.M. Worth the wait? Preconception weight reduction in women and men with obesity and infertility: A narrative review. Fertil. Steril. 2022, 118, 447–455. [Google Scholar] [CrossRef]
- Wing, R.R.; Phelan, S. Long-term weight loss maintenance. Am. J. Clin. Nutr. 2005, 82, 222S–225S. [Google Scholar] [CrossRef]
- Jiskoot, G.; Timman, R.; Beerthuizen, A.; Dietz de Loos, A.; Busschbach, J.; Laven, J. Weight Reduction Through a Cognitive Behavioral Therapy Lifestyle Intervention in PCOS: The Primary Outcome of a Randomized Controlled Trial. Obesity 2020, 28, 2134–2141. [Google Scholar] [CrossRef]
- Gaskins, A.J.; Nassan, F.L.; Chiu, Y.H.; Arvizu, M.; Williams, P.L.; Keller, M.G.; Souter, I.; Hauser, R.; Chavarro, J.E.; EARTH Study Team. Dietary patterns and outcomes of assisted reproduction. Am. J. Obstet. Gynecol. 2019, 220, 567.e1–567.e18. [Google Scholar] [CrossRef]
- Karayiannis, D.; Kontogianni, M.D.; Mendorou, C.; Mastrominas, M.; Yiannakouris, N. Adherence to the Mediterranean diet and IVF success rate among non-obese women attempting fertility. Hum. Reprod. 2018, 33, 494–502. [Google Scholar] [CrossRef]
- Vujkovic, M.; de Vries, J.H.; Lindemans, J.; Macklon, N.S.; van der Spek, P.J.; Steegers, E.A.; Steegers-Theunissen, R.P. The preconception Mediterranean dietary pattern in couples undergoing in vitro fertilization/intracytoplasmic sperm injection treatment increases the chance of pregnancy. Fertil. Steril. 2010, 94, 2096–2101. [Google Scholar] [CrossRef]
- Herforth, A.; Arimond, M.; Álvarez-Sánchez, C.; Coates, J.; Christianson, K.; Muehlhoff, E. A Global Review of Food-Based Dietary Guidelines. Adv. Nutr. 2019, 10, 590–605. [Google Scholar] [CrossRef] [PubMed]
- Smits, A.; Marei, W.F.A.; De Neubourg, D.; Leroy, J.L.M.R. Diet normalization or caloric restriction as a preconception care strategy to improve metabolic health and oocyte quality in obese outbred mice. Reprod. Biol. Endocrinol. 2021, 19, 166. [Google Scholar] [CrossRef] [PubMed]
- Catandi, G.D.; Fresa, K.J.; Cheng, M.H.; Whitcomb, L.A.; Broeckling, C.D.; Chen, T.W.; Chicco, A.J.; Carnevale, E.M. Follicular metabolic alterations are associated with obesity in mares and can be mitigated by dietary supplementation. Sci. Rep. 2024, 14, 7571. [Google Scholar] [CrossRef] [PubMed]
- Smits, A.; Marei, W.F.A.; Moorkens, K.; Bols, P.E.J.; De Neubourg, D.; Leroy, J.L.M.R. Obese outbred mice only partially benefit from diet normalization or calorie restriction as preconception care interventions to improve metabolic health and oocyte quality. Hum. Reprod. 2022, 37, 2867–2884. [Google Scholar] [CrossRef]
- Oh, S.; Kim, E.; Shoda, J. Editorial: Lifestyle modification strategies as first line of chronic disease management. Front. Physiol. 2023, 14, 1204581. [Google Scholar] [CrossRef]
- Weiss, G.; Goldsmith, L.T.; Taylor, R.N.; Bellet, D.; Taylor, H.S. Inflammation in reproductive disorders. Reprod. Sci. 2009, 16, 216–229. [Google Scholar] [CrossRef]
- Skoracka, K.; Ratajczak, A.E.; Rychter, A.M.; Dobrowolska, A.; Krela-Kaźmierczak, I. Female Fertility and the Nutritional Approach: The Most Essential Aspects. Adv. Nutr. 2021, 12, 2372–2386. [Google Scholar] [CrossRef]
- Winter, H.G.; Rolnik, D.L.; Mol, B.W.J.; Torkel, S.; Alesi, S.; Mousa, A.; Habibi, N.; Silva, T.R.; Oi Cheung, T.; Thien Tay, C.; et al. Can Dietary Patterns Impact Fertility Outcomes? A Systematic Review and Meta-Analysis. Nutrients 2023, 15, 2589. [Google Scholar] [CrossRef]
- Kohil, A.; Chouliaras, S.; Alabduljabbar, S.; Lakshmanan, A.P.; Ahmed, S.H.; Awwad, J.; Terranegra, A. Female infertility and diet, is there a role for a personalized nutritional approach in assisted reproductive technologies? A Narrative Review. Front. Nutr. 2022, 9, 927972. [Google Scholar] [CrossRef]
- Schipper, M.C.; Jaddoe, V.W.; Bekkers, E.L.; Mulders, A.G.; Gaillard, R. Dietary intake of polyunsaturated fatty acids, their food sources and fertility in females and males: A preconception prospective population-based cohort study. Am. J. Clin. Nutr. 2025, 121, 1354–1364. [Google Scholar] [CrossRef]
- Duttaroy, A.K.; Basak, S. Maternal Fatty Acid Metabolism in Pregnancy and Its Consequences in the Feto-Placental Development. Front. Physiol. 2022, 12, 787848. [Google Scholar] [CrossRef] [PubMed]
- Coyne, G.S.; Kenny, D.A.; Childs, S.; Sreenan, J.M.; Waters, S.M. Dietary n-3 polyunsaturated fatty acids alter the expression of genes involved in prostaglandin biosynthesis in the bovine uterus. Theriogenology 2008, 70, 772–782. [Google Scholar] [CrossRef] [PubMed]
- Coyne, G.S.; Kenny, D.A.; Waters, S.M. Effect of dietary n-3 polyunsaturated fatty acid supplementation on bovine uterine endometrial and hepatic gene expression of the insulin-like growth factor system. Theriogenology 2011, 75, 500–512. [Google Scholar] [CrossRef]
- Waters, S.M.; Coyne, G.S.; Kenny, D.A.; MacHugh, D.E.; Morris, D.G. Dietary n-3 polyunsaturated fatty acid supplementation alters the expression of genes involved in the control of fertility in the bovine uterine endometrium. Physiol. Genom. 2012, 44, 878–888. [Google Scholar] [CrossRef]
- Waters, S.M.; Coyne, G.S.; Kenny, D.A.; Morris, D.G. Effect of dietary n-3 polyunsaturated fatty acids on transcription factor regulation in the bovine endometrium. Mol. Biol. Rep. 2014, 41, 2745–2755. [Google Scholar] [CrossRef]
- Gokuldas, P.P.; Singh, S.K.; Tamuli, M.K.; Naskar, S.; Vashi, Y.; Thomas, R.; Barman, K.; Pegu, S.R.; Chethan, S.G.; Agarwal, S.K. Dietary supplementation of n-3 polyunsaturated fatty acid alters endometrial expression of genes involved in prostaglandin biosynthetic pathway in breeding sows (Sus scrofa). Theriogenology 2018, 110, 201–208. [Google Scholar] [CrossRef]
- WHO Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020.
- Committee on Obstetric Practice. Physical Activity and Exercise During Pregnancy and the Postpartum Period: ACOG Committee Opinion, Number 804. Obstet. Gynecol. 2020, 135, 178–188. [Google Scholar] [CrossRef]
- Dağ, Z.Ö.; Dilbaz, B. Impact of obesity on infertility in women. J. Turk. Ger. Gynecol. Assoc. 2015, 16, 111–117. [Google Scholar]
- Shashwathi, G.; Rao, B.K.; Bailey, A.; Kumar, P.; Ramachandra, P. “If by exercising I can conceive; I would like to exercise”. Exploring knowledge, perception, and practices about exercise among women with infertility: A qualitative study. Braz. J. Phys. Ther. 2025, 29, 101186. [Google Scholar] [CrossRef]
- Joseph, D.N.; Whirledge, S. Stress and the HPA Axis: Balancing Homeostasis and Fertility. Int. J. Mol. Sci. 2017, 18, 2224. [Google Scholar] [CrossRef]
- Brinson, A.K.; da Silva, S.G.; Hesketh, K.R.; Evenson, K.R. Impact of Physical Activity and Sedentary Behavior on Spontaneous Female and Male Fertility: A Systematic Review. J. Phys. Act. Health 2023, 20, 600–615. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 762: Prepregnancy Counseling. Obstet. Gynecol. 2019, 133, 78–89. [Google Scholar] [CrossRef] [PubMed]
- Mutsaerts, M.A.; van Oers, A.M.; Groen, H.; Burggraaff, J.M.; Kuchenbecker, W.K.; Perquin, D.A.; Koks, C.A.; van Golde, R.; Kaaijk, E.M.; Schierbeek, J.M.; et al. Randomized Trial of a Lifestyle Program in Obese Infertile Women. N. Engl. J. Med. 2018, 378, 2546. [Google Scholar]
- Norman, R.J.; Mol, B.W.J. Successful weight loss interventions before in vitro fertilization: Fat chance? Fertil. Steril. 2018, 110, 581–586. [Google Scholar] [CrossRef]
- Espinós, J.J.; Polo, A.; Sánchez-Hernández, J.; Bordas, R.; Pares, P.; Martínez, O.; Calaf, J. Weight decrease improves live birth rates in obese women undergoing IVF: A pilot study. Reprod. Biomed. Online 2017, 35, 417–424. [Google Scholar] [CrossRef]
- Nasrekani, A.Z.; Fathi, M. Efficacy of 12 weeks aerobic training on body composition, aerobic power and some women-hormones in polycystic ovary syndrome infertile women. Iran. J. Obstet. Gynecol. Infertil. 2016, 19, 1–10. [Google Scholar]
- Du, M.C.; Ouyang, Y.Q.; Nie, X.F.; Huang, Y.; Redding, S.R. Effects of physical exercise during pregnancy on maternal and infant outcomes in overweight and obese pregnant women: A meta-analysis. Birth 2019, 46, 211–221. [Google Scholar] [CrossRef]
- Choi, J.; Fukuoka, Y.; Lee, J.H. The effects of physical activity and physical activity plus diet interventions on body weight in overweight or obese women who are pregnant or in postpartum: A systematic review and meta-analysis of randomized controlled trials. Prev. Med. 2013, 56, 351–364. [Google Scholar] [CrossRef]
- Oteng-Ntim, E.; Varma, R.; Croker, H.; Poston, L.; Doyle, P. Lifestyle interventions for overweight and obese pregnant women to improve pregnancy outcome: Systematic review and meta-analysis. BMC Med. 2012, 10, 47. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Gitsi, E.; Livadas, S.; Argyrakopoulou, G. Nutritional and exercise interventions to improve conception in women suffering from obesity and distinct nosological entities. Front. Endocrinol. 2024, 15, 1426542. [Google Scholar] [CrossRef] [PubMed]
- Mena, G.P.; Mielke, G.I.; Brown, W.J. The effect of physical activity on reproductive health outcomes in young women: A systematic review and meta-analysis. Hum. Reprod. Update 2019, 25, 541–563. [Google Scholar] [CrossRef] [PubMed]
- Best, D.; Avenell, A.; Bhattacharya, S. How effective are weight-loss interventions for improving fertility in women and men who are overweight or obese? A systematic review and meta-analysis of the evidence. Hum. Reprod. Update 2017, 23, 681–705. [Google Scholar] [CrossRef]
- Sõritsa, D.; Mäestu, E.; Nuut, M.; Mäestu, J.; Migueles, J.H.; Läänelaid, S.; Ehrenberg, A.; Sekavin, A.; Sõritsa, A.; Salumets, A.; et al. Maternal physical activity and sedentary behaviour before and during in vitro fertilization treatment: A longitudinal study exploring the associations with controlled ovarian stimulation and pregnancy outcomes. J. Assist. Reprod. Genet. 2020, 37, 1869–1881. [Google Scholar] [CrossRef]
- Rao, M.; Zeng, Z.; Tang, L. Maternal physical activity before IVF/ICSI cycles improves clinical pregnancy rate and live birth rate: A systematic review and meta-analysis. Reprod. Biol. Endocrinol. 2018, 16, 11. [Google Scholar] [CrossRef]
- Redman, L.M. Physical activity and its effects on reproduction. Reprod. Biomed. Online. 2006, 12, 579–586. [Google Scholar] [CrossRef]
- Yusuf, S.; Anand, S. Body-mass index, abdominal adiposity, and cardiovascular risk. Lancet 2011, 378, 226–227. [Google Scholar] [CrossRef]
- Palomba, S.; Falbo, A.; Russo, T.; Orio, F.; Tolino, A.; Zullo, F. Systemic and local effects of metformin administration in patients with polycystic ovary syndrome (PCOS): Relationship to the ovulatory response. Hum. Reprod. 2010, 25, 1005–1013. [Google Scholar] [CrossRef]
- Wang, W.; Yang, F.; Bai, Y.; Lu, Y.; Mao, X. Association between domain-specific physical activity and mental health status after embryo transfer in IVF-ET-assisted pregnancy patients. Sci. Rep. 2024, 14, 4928. [Google Scholar] [CrossRef]
- Hunter, E.; Avenell, A.; Maheshwari, A.; Stadler, G.; Best, D. The effectiveness of weight-loss lifestyle interventions for improving fertility in women and men with overweight or obesity and infertility: A systematic review update of evidence from randomized controlled trials. Obes. Rev. 2021, 22, 13325. [Google Scholar] [CrossRef]
- Haase, C.L.; Varbo, A.; Laursen, P.N.; Schnecke, V.; Balen, A.H. Association between body mass index, weight loss and the chance of pregnancy in women with polycystic ovary syndrome and overweight or obesity: A retrospective cohort study in the UK. Hum. Reprod. 2023, 38, 471–481. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donato, M.; Capalbo, A.; Morizio, E.; Fratini, R.M.; Pilenzi, L.; D’Antonio, F.; Stuppia, L.; Vitacolonna, E.; Gatta, V.; Konstantinidou, F. The Role of Lifestyle Intervention in Female Fertility: A Modifiable Factor for Preconception Health. Nutrients 2025, 17, 2101. https://doi.org/10.3390/nu17132101
Donato M, Capalbo A, Morizio E, Fratini RM, Pilenzi L, D’Antonio F, Stuppia L, Vitacolonna E, Gatta V, Konstantinidou F. The Role of Lifestyle Intervention in Female Fertility: A Modifiable Factor for Preconception Health. Nutrients. 2025; 17(13):2101. https://doi.org/10.3390/nu17132101
Chicago/Turabian StyleDonato, Marisa, Antonio Capalbo, Elisena Morizio, Rosa Maria Fratini, Lucrezia Pilenzi, Francesco D’Antonio, Liborio Stuppia, Ester Vitacolonna, Valentina Gatta, and Fani Konstantinidou. 2025. "The Role of Lifestyle Intervention in Female Fertility: A Modifiable Factor for Preconception Health" Nutrients 17, no. 13: 2101. https://doi.org/10.3390/nu17132101
APA StyleDonato, M., Capalbo, A., Morizio, E., Fratini, R. M., Pilenzi, L., D’Antonio, F., Stuppia, L., Vitacolonna, E., Gatta, V., & Konstantinidou, F. (2025). The Role of Lifestyle Intervention in Female Fertility: A Modifiable Factor for Preconception Health. Nutrients, 17(13), 2101. https://doi.org/10.3390/nu17132101