

Initiation of Enteral Feeding with Mother’s Own Milk or Donor Human Milk in Very Preterm Infants: Impact on Bronchopulmonary Dysplasia and Other Prematurity-Related Morbidities
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
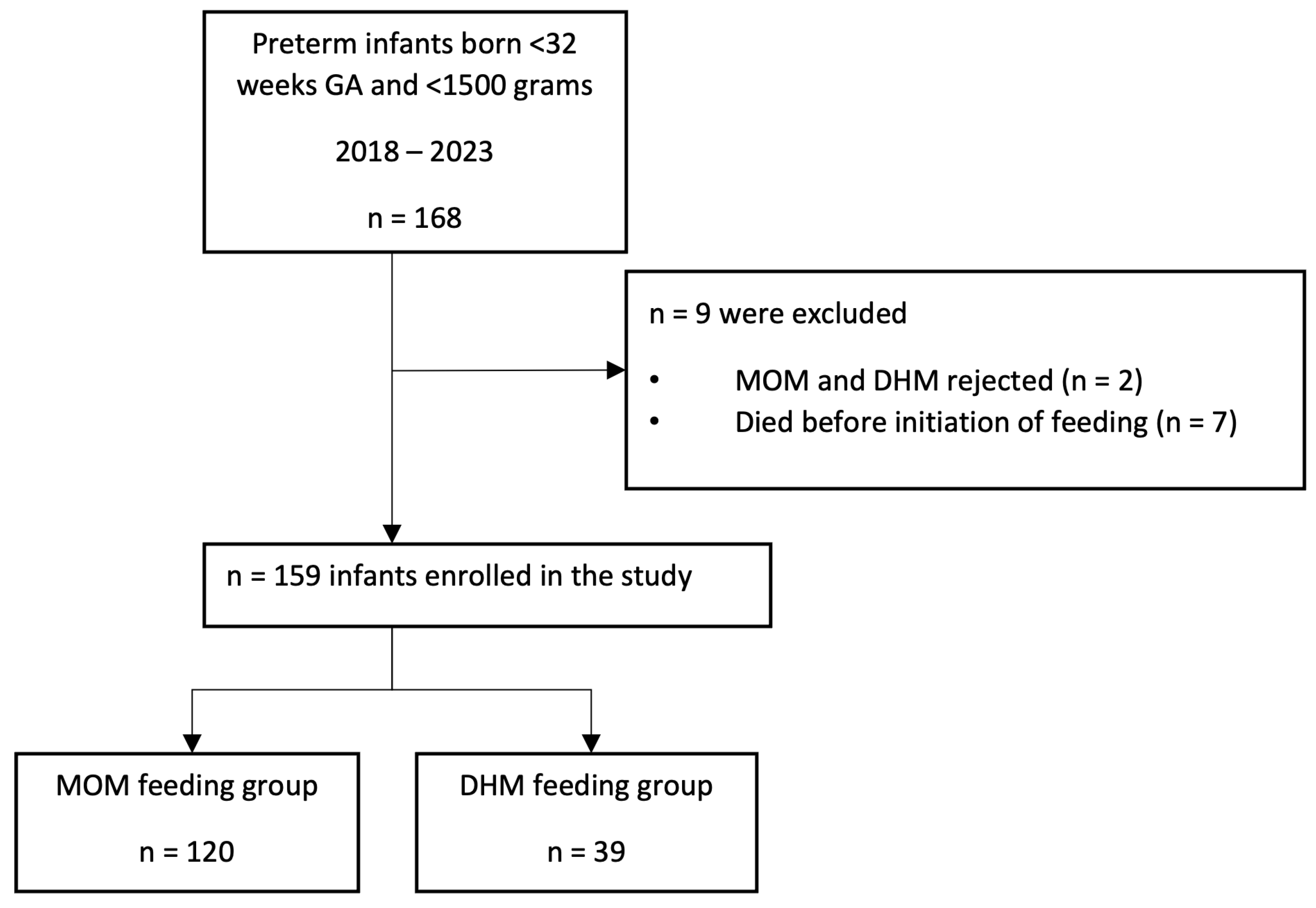
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BPD | Bronchopulmonary Dysplasia |
| MOM | Mother’s Own Milk |
| DHM | Donor Human Milk |
| GA | Gestational Age |
| PF | Preterm Formula |
| BW | Birth Weight |
| IMV | Invasive Mechanical Ventilation |
| SD | Standard Deviation |
| OR | Odds Ratio |
| CI | Confidence Interval |
References
- Ten, V.S. Mitochondrial dysfunction in alveolar and white matter developmental failure in premature infants. Pediatr. Res. 2017, 81, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Xuefei, Y.; Xinyi, Z.; Qing, C.; Dan, Z.; Ziyun, L.; Hejuan, Z.; Xindong, X.; Jianhua, F. Effects of Hyperoxia on Mitochondrial Homeostasis: Are Mitochondria the Hub for Bronchopulmonary Dysplasia? Front. Cell Dev. Biol. 2021, 9, 642717. [Google Scholar] [CrossRef] [PubMed]
- Sucasas Alonso, A.; Pértega Díaz, S.; Sáez Soto, R.; Ávila-Álvarez, A. Epidemiology and risk factors for bronchopulmonary dysplasia in prematures infants born at or less than 32 weeks of gestation. An. Pediatr. 2021, 96, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Rocha, G.; Guimarães, H.; Pereira-Da-silva, L. The role of nutrition in the prevention and management of bronchopulmonary dysplasia: A literature review and clinical approach. Int. J. Environ. Res. Public Health 2021, 18, 6245. [Google Scholar] [CrossRef] [PubMed]
- Thiess, T.; Lauer, T.; Woesler, A.; Neusius, J.; Stehle, S.; Zimmer, K.P.; Eckert, G.P.; Ehrhardt, H. Correlation of Early Nutritional Supply and Development of Bronchopulmonary Dysplasia in Preterm Infants <1000 g. Front. Pediatr. 2021, 9, 741365. [Google Scholar] [CrossRef]
- Fonseca, L.T.; Senna, D.C.; Silveira, R.C.; Procianoy, R.S. Association between Breast Milk and Bronchopulmonary Dysplasia: A Single Center Observational Study. Am. J. Perinatol. 2017, 34, 264–269. [Google Scholar] [CrossRef]
- Avila-Alvarez, A.; Zozaya, C.; Pértega-Diaz, S.; Sanchez-Luna, M.; Iriondo-Sanz, M.; Elorza, M.D.; García-Muñoz Rodrigo, F. Temporal trends in respiratory care and bronchopulmonary dysplasia in very preterm infants over a 10-year period in Spain. Arch. Dis. Child.-Fetal Neonatal Ed. 2021, 107, 143–149. [Google Scholar] [CrossRef]
- Huang, J.; Zhang, L.; Tang, J.; Shi, J.; Qu, Y.; Xiong, T.; Mu, D. Human milk as a protective factor for bronchopulmonary dysplasia: A systematic review and meta-analysis. Arch. Dis. Child.-Fetal Neonatal Ed. 2019, 104, F128–F136. [Google Scholar] [CrossRef]
- Villamor-Martínez, E.; Pierro, M.; Cavallaro, G.; Mosca, F.; Kramer, B.W.; Villamor, E. Donor human milk protects against bronchopulmonary dysplasia: A systematic review and meta-analysis. Nutrients 2018, 10, 238. [Google Scholar] [CrossRef]
- Spiegler, J.; Preuß, M.; Gebauer, C.; Bendiks, M.; Herting, E.; Göpel, W.; Berghäuser, M.A.; Böckenholt, K.; Bohnhorst, B.; Böttger, R.; et al. Does Breastmilk Influence the Development of Bronchopulmonary Dysplasia? J. Pediatr. 2016, 169, 76–80.e4. [Google Scholar] [CrossRef]
- Thébaud, B.; Goss, K.N.; Laughon, M.; Whitsett, J.A.; Abman, S.H.; Steinhorn, R.H.; Aschner, J.L.; Davis, P.G.; McGrath-Morrow, S.A.; Soll, R.F.; et al. Bronchopulmonary dysplasia. Nat. Rev. Dis. Prim. 2019, 5, 78. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Fuente, M.; Moreno, L.; Mitchell, J.A.; Reiss, I.K.; Lopez, P.; Elorza, D.; Duijts, L.; Avila-Alvarez, A.; Arruza, L.; Ramirez Orellana, M.; et al. Preventing bronchopulmonary dysplasia: New tools for an old challenge. Pediatr. Res. 2019, 85, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.L.; Johnson, T.J.; Robin, B.; Bigger, H.R.; Buchanan, A.; Christian, E.; Nandhan, V.; Shroff, A.; Schoeny, M.; Engstrom, J.L.; et al. Influence of own mother’s milk on bronchopulmonary dysplasia and costs. Arch. Dis. Child.-Fetal Neonatal Ed. 2017, 102, F256–F261. [Google Scholar] [CrossRef] [PubMed]
- Verd, S.; Porta, R.; Ginovart, G.; Avila-Alvarez, A.; García-Muñoz Rodrigo, F.; Izquierdo Renau, M.; Ventura, P.S. Human Milk Feeding Is Associated with Decreased Incidence of Moderate-Severe Bronchopulmonary Dysplasia in Extremely Preterm Infants. Children 2023, 10, 1267. [Google Scholar] [CrossRef]
- Verd, S.; Ginovart, G. Human milk is perhaps the single most under-rated strategy to prevent bronchopulmonary dysplasia. Arch. Dis. Child.-Fetal Neonatal Ed. 2018, 103, F599–F600. [Google Scholar] [CrossRef]
- Xu, Y.; Yu, Z.; Li, Q.; Zhou, J.; Yin, X.; Ma, Y.; Yin, Y.; Jiang, S.; Zhu, R.; Wu, Y.; et al. Dose-dependent effect of human milk on Bronchopulmonary dysplasia in very low birth weight infants. BMC Pediatr. 2020, 20, 522. [Google Scholar] [CrossRef]
- Gates, A.; Hair, A.B.; Salas, A.A.; Thompson, A.B.; Stansfield, B.K. Nutrient Composition of Donor Human Milk and Comparisons to Preterm Human Milk. J. Nutr. 2023, 153, 2622–2630. [Google Scholar] [CrossRef]
- Villamor-Martínez, E.; Pierro, M.; Cavallaro, G.; Mosca, F.; Villamor, E. Mother’s own milk and bronchopulmonary dysplasia: A systematic review and meta-analysis. Front. Pediatr. 2019, 7, 224. [Google Scholar] [CrossRef]
- Merino-Hernández, A.; Palacios-Bermejo, A.; Ramos-Navarro, C.; Caballero-Martín, S.; González-Pacheco, N.; Rodríguez-Corrales, E.; Sánchez-Gómez de Orgaz, M.C.; Sánchez-Luna, M. Effect of Donated Premature Milk in the Prevention of Bronchopulmonary Dysplasia. Nutrients 2024, 16, 859. [Google Scholar] [CrossRef]
- Bancalari, E.; Claure, N. Definitions and diagnostic criteria for bronchopulmonary dysplasia. Semin. Perinatol. 2006, 30, 164–170. [Google Scholar] [CrossRef]
- Gregory, K.E.; DeForge, C.E.; Natale, K.M.; Phillips, M.; Van Marter, L.J. Necrotizing enterocolitis in the premature infant: Neonatal nursing assessment, disease pathogenesis, and clinical presentation. Adv. Neonatal Care 2011, 11, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Volpe, J.J. Perinatal brain injury: From pathogenesis to neuroprotection. Ment. Retard. Dev. Disabil. Res. Rev. 2001, 7, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Castro Conde, J.R.; Echániz Urcelay, I.; Botet Mussons, F.; Pallás Alonso, C.R.; Narbona, E.; Sánchez Luna, M. Retinopathy of prematurity. Prevention, screening and treatment guidelines. An. Pediatr. 2009, 71, 514–523. [Google Scholar] [CrossRef]
- Arslanoglu, S.; Corpeleijn, W.; Moro, G.; Braegger, C.; Campoy, C.; Colomb, V.; Decsi, T.; Domellöf, M.; Fewtrell, M.; Hojsak, I.; et al. Donor human milk for preterm infants: Current evidence and research directions. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Eidelman, A.I.; Schanler, R.J. Breastfeeding and the use of human milk. Pediatrics 2012, 129, e827–e841. [Google Scholar] [CrossRef]
- Zhu, Y.; Chen, X.; Zhu, J.; Jiang, C.; Yu, Z.; Su, A. Effect of First Mother’s Own Milk Feeding Time on the Risk of Moderate and Severe Bronchopulmonary Dysplasia in Infants With Very Low Birth Weight. Front. Pediatr. 2022, 10, 887028. [Google Scholar] [CrossRef]
- Parker, L.A.; Koernere, R.; Fordham, K.; Bubshait, H.; Eugene, A.; Gefre, A.; Bendixen, M. Mother’s Own Milk Versus Donor Human Milk: What’s the Difference? Crit. Care Nurs. Clin. N. Am. 2024, 36, 119–133. [Google Scholar] [CrossRef]
- Chang, F.-Y.; Fang, L.-J.; Chang, C.-S.; Wu, T.-Z. The Effect of Processing Donor Milk on Its Nutrient and Energy Content. Breastfeed. Med. Off. J. Acad. Breastfeed. Med. 2020, 15, 576–582. [Google Scholar] [CrossRef]
- Young, B.E.; Borman, L.L.; Heinrich, R.; Long, J.; Pinney, S.; Westcott, J.; Krebs, N.F. Effect of Pooling Practices and Time Postpartum of Milk Donations on the Energy, Macronutrient, and Zinc Concentrations of Resultant Donor Human Milk Pools. J. Pediatr. 2019, 214, 54–59. [Google Scholar] [CrossRef]
- Johnson, T.J.; Patel, A.L.; Schoeny, M.E.; Meier, P.P. Cost Savings of Mother’s Own Milk for Very Low Birth Weight Infants in the Neonatal Intensive Care Unit. PharmacoEconomics-Open 2022, 6, 451–460. [Google Scholar] [CrossRef]
- Cartagena, D.; Penny, F.; McGrath, J.M.; Reyna, B.; Parker, L.A.; McInnis, J. Differences in Neonatal Outcomes Among Premature Infants Exposed to Mother’s Own Milk Versus Donor Human Milk. Adv. Neonatal Care Off. J. Natl. Assoc. Neonatal Nurses 2022, 22, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, A.; Voynow, J.; Chahin, N.; Williams, A.; Xu, J.; Chavez, D.; Carroll, L.; Hendricks-Muñoz, K.D. Greater and Earlier Exposure of Mother’s Own Milk Compared to Donor Human Milk Moderates Risk and Severity of Bronchopulmonary Dysplasia. Breastfeed. Med. Off. J. Acad. Breastfeed. Med. 2024; ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Quigley, M.; Embleton, N.D.; Meader, N.; McGuire, W. Donor human milk for preventing necrotising enterocolitis in very preterm or very low-birthweight infants. Cochrane Database Syst. Rev. 2024, 9, CD002971. [Google Scholar] [CrossRef] [PubMed]
- Schlesinger, E.; Hatiel, K.; Hod, N.; Shinwell, E.S. Longer skin-to-skin contact after birth enhances breastfeeding quality and duration: A cohort study. Acta Paediatr. 2024, 113, 2637–2642. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Total n = 159 | MOM n = 120 | DHM n = 39 | p-Value | |
|---|---|---|---|---|
| Gestational age (weeks) | 29.44 ± 2.34 | 29.18 ± 2.38 | 30.24 ± 2.04 | 0.013 |
| Sex (women) | 78 (49.10%) | 61 (50.80%) | 17 (43.60%) | 0.432 |
| Birth weight (g) | 1181.65 ± 349.76 | 1165.67 ± 345.06 | 1230.82 ± 364.01 | 0.314 |
| Birth weight percentile | 38.26 ± 24.65 | 40.38 ± 24.10 | 31.76 ± 25.90 | 0.059 |
| Birth weight < 10th percentile | 25 (16.40%) | 16 (14.0%) | 8 (23.70%) | 0.165 |
| Mother’s age | 38.61 ± 58.46 | 39.58 ± 67.27 | 35.61 ± 5.30 | 0.714 |
| Maternal hypertensive disorder | 35 (22.00%) | 26 (21.70%) | 9 (23.10%) | 0.853 |
| Chorioamnionitis | 26 (16.40%) | 21 (17.50%) | 5 (12.80%) | 0.492 |
| Antenatal steroids | 149 (93.70%) | 112 (93.30%) | 37 (94.90%) | 0.731 |
| Caesarean section | 94 (59.10%) | 64 (53.30%) | 30 (76.90%) | 0.009 |
| In vitro fertilization | 22 (13.80%) | 20 (16.70%) | 2 (5.10%) | 0.070 |
| Intubation in delivery room | 28 (17.60%) | 17 (14.20%) | 11 (28.20%) | 0.046 |
| Epinephrin in delivery room | 6 (3.80%) | 3 (2.50%) | 3 (7.70%) | 0.139 |
| Chest compressions in delivery room | 9 (5.70%) | 6 (5.00%) | 3 (7.70%) | 0.527 |
| Surfactant therapy | 68 (42.80%) | 52 (43.30%) | 16 (41.00%) | 0.813 |
| Caffeine | 145 (91.20%) | 110 (91.70%) | 35 (89.70%) | 0.713 |
| Inotropic therapy | 21 (13.30%) | 16 (13.30%) | 5 (13.20%) | 0.978 |
| Parenteral nutrition | 143 (90.50%) | 107 (89.20%) | 36 (94.70%) | 0.737 |
| Day when trophic feeding commenced | 1.86 ± 0.95 | 1.84 ± 0.87 | 1.92 ± 1.17 | 0.930 |
| Year | 0.358 | |||
| 2018 | 23 (14.50%) | 18 (15.00%) | 5 (12.80%) | |
| 2019 | 24 (15.10%) | 18 (15.00%) | 6 (15.40%) | |
| 2020 | 33 (20.80%) | 22 (18.30%) | 11 (28.20%) | |
| 2021 | 45 (28.30%) | 38 (31.70%) | 7 (17.90%) | |
| 2022 | 22 (13.80%) | 14 (11.70%) | 8 (20.50%) | |
| 2023 | 12 (7.50%) | 10 (8.30%) | 2 (5.10%) |
| Outcome Variables | Total n = 159 | MOM n = 120 | DHM n = 39 | p-Value |
|---|---|---|---|---|
| BPD | 39/157 (24.80%) | 33 (27.70%) | 6 (15.80%) | 0.138 |
| BPD moderate-to-severe | 16/154 (10.40%) | 15 (12.80%) | 1 (2.70%) | 0.064 |
| Steroids for BPD | 21/158 (13.30%) | 19 (15.80%) | 2 (5.30%) | 0.094 |
| MV | 55 (34.60%) | 44 (36.70%) | 11 (28.20%) | 0.515 |
| Duration of MV (hours) | 187.24 ± 269.50 | 210.37 ± 295.57 | 105.38 ± 118.91 | 0.218 |
| Duration of NIMV (hours) | 213.47 ± 205.54 | 229.90 ± 212.92 | 162.83 ± 173.88 | 0.085 |
| Duration of supplemental oxygen (hours) | 597.29 ± 722.64 | 704.26 ± 775.91 | 306.46 ± 445.18 | 0.007 |
| Oxygen at home | 12/155 (7.70%) | 10 (8.30%) | 2 (5.70%) | 0.463 |
| FiO2 at day 7 | 23.30 ± 8.39 | 23.38 ± 9.17 | 23.05 ± 5.45 | 0.833 |
| FiO2 at day 14 | 23.37 ± 7.79 | 23.90 ± 8.82 | 21.70 ± 2.13 | 0.135 |
| MV at day 14 | 10/153 (6.50%) | 8 (6.90%) | 2 (5.40%) | 0.548 |
| NIMV at day 28 | 11/156 (7.1%) | 9 (7.70%) | 2 (5.10%) | 0.450 |
| NEC | 10/158 (6.30%) | 8 (6.70%) | 2 (5.30%) | 0.553 |
| Surgical NEC | 6/158 (3.80%) | 5 (4.20%) | 1 (2.60%) | 0.555 |
| ROP > II | 6/151 (4.30%) | 4 (3.70%) | 2 (6.10%) | 0.557 |
| IVH > II | 9 (5.80%) | 8 (6.90%) | 1 (2.60%) | 0.288 |
| Periventricular leukomalacia | 3 (1.90%) | 3 (2.50%) | 0 (0.0%) | 0.435 |
| Nosocomial sepsis | 43 (27.00%) | 32 (26.70%) | 11 (28.20%) | 0.851 |
| Spontaneous intestinal perforation | 5 (3.20%) | 4 (3.30%) | 1 (2.60%) | 0.653 |
| Anemia requiring blood transfusion | 91 (57.20%) | 69 (57.50%) | 22 (56.40%) | 0.905 |
| PDA | 21 (13.40%) | 19 (16,00%) | 2 (5.30%) | 0.072 |
| Ibuprofen for PDA | 14 (8.90%) | 13 (10.80%) | 1 (2.60%) | 0.104 |
| Surgery for PDA | 7 (4.40%) | 5 (4.20%) | 2 (5.30%) | 0.535 |
| Days in the NICU | 27.74 ± 19.97 | 28.54 ± 21.09 | 25.21 ± 16.18 | 0.372 |
| Days until discharge | 58.35 ± 63.53 | 62.12 ± 70.88 | 45.45 ± 21.78 | 0.173 |
| Duration of parenteral nutrition (days) | 12.58 ± 7.96 | 12.52 ± 7.86 | 12.73 ± 8.34 | 0.892 |
| Death | 9 (5.70%) | 7 (5.80%) | 2 (5.10%) | 0.614 |
| BPD/death at 28 days of life | 50 (31.60%) | 42 (35.00%) | 8 (21.10%) | 0.107 |
| BPD/death at 36 weeks of life | 24 (15.2%) | 21 (17.50%) | 3 (7.90%) | 0.116 |
| p-Value | OR | CI 95% | |
|---|---|---|---|
| Gestational Age (weeks) | 0.037 | 1.23 | 1.01–1.50 |
| Born by C-section | 0.118 | 2.15 | 0.82–5.64 |
| Intubation in the DR | 0.044 | 2.69 | 1.02–7.05 |
| Birth weight percentile | 0.689 | 0.99 | 0.97–1.01 |
| In vitro fertilization | 0.142 | 0.31 | 0.06–1.48 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Avila-Alvarez, A.; Fernandez-Gonzalez, S.M.; Sucasas-Alonso, A.; Ansede, A.S. Initiation of Enteral Feeding with Mother’s Own Milk or Donor Human Milk in Very Preterm Infants: Impact on Bronchopulmonary Dysplasia and Other Prematurity-Related Morbidities. Nutrients 2025, 17, 508. https://doi.org/10.3390/nu17030508
Avila-Alvarez A, Fernandez-Gonzalez SM, Sucasas-Alonso A, Ansede AS. Initiation of Enteral Feeding with Mother’s Own Milk or Donor Human Milk in Very Preterm Infants: Impact on Bronchopulmonary Dysplasia and Other Prematurity-Related Morbidities. Nutrients. 2025; 17(3):508. https://doi.org/10.3390/nu17030508
Chicago/Turabian StyleAvila-Alvarez, Alejandro, Sara María Fernandez-Gonzalez, Andrea Sucasas-Alonso, and Alba Sanchez Ansede. 2025. "Initiation of Enteral Feeding with Mother’s Own Milk or Donor Human Milk in Very Preterm Infants: Impact on Bronchopulmonary Dysplasia and Other Prematurity-Related Morbidities" Nutrients 17, no. 3: 508. https://doi.org/10.3390/nu17030508
APA StyleAvila-Alvarez, A., Fernandez-Gonzalez, S. M., Sucasas-Alonso, A., & Ansede, A. S. (2025). Initiation of Enteral Feeding with Mother’s Own Milk or Donor Human Milk in Very Preterm Infants: Impact on Bronchopulmonary Dysplasia and Other Prematurity-Related Morbidities. Nutrients, 17(3), 508. https://doi.org/10.3390/nu17030508