Abstract
Background: Head Start, a federally funded preschool for low-income families, offers a unique space for interventionists to equitably reach parents and children, and promote healthful behavior for chronic disease prevention. However, determinants of implementation in this context remain understudied, hindering opportunities for improvement. We aim to identify organization-level factors affecting implementation of an obesity prevention program, as relayed by implementation partners at Head Start. Methods: Communities for Healthy Living (CHL), designed and implemented with Greater Boston Head Start (n = 16 programs across n = 2 agencies), is a cluster-randomized obesity prevention trial offering enhanced nutrition support, media campaign, and a parenting program. The current study draws on two years (2017-19) of data collected from Head Start implementation partners. Pre-implementation, staff completed anonymous surveys: implementation readiness (n = 119), staff training evaluation (n = 166), and facilitator training evaluation (n = 22); response frequencies were tabulated. Mid-implementation, staff and leadership participated in focus groups (n = 3 groups with n = 16 participants) and interviews (n = 9); transcripts were analyzed using a deductive-inductive hybrid approach, grounded in the Consolidated Framework for Implementation Research. Results: Most staff strongly agreed or agreed they understood their role (98.8%), planned on recruiting parents (98.2%), and reported commitment to implementation (92.5%); however, fewer identified CHL as a priority (69.7%) and were confident in their ability to coordinate efforts (84.9%), handle challenges (77.3%), and receive support (83.2%). Thematic analysis yielded implementation facilitators, including mission alignment, partner engagement in design, allocation of intervention-specific resources, and expressed leadership support. Barriers included strains imposed on staff workflow, a lack of shared responsibility, and challenges in coordinating CHL activities amidst competing Head Start programs. Conclusions: Responsive efforts to address deliverer-identified barriers to implementation may include reducing intervention impact on preexisting workflow, as well as clearly distinguishing intervention activities from preexisting Head Start programs.
1. Introduction
Chronic disease is the leading cause of morbidity and mortality in the United States (U.S.) [1]. Disparities in chronic disease risk—by socioeconomic status [2], race and ethnicity [3]—emerge early [3,4] and persist across the lifespan [5,6] as a result of inequitable structural barriers to social, economic, and environmental opportunity [7,8], alongside heightened stress levels and reduced access to healthcare [9]. Interventions targeting modifiable behavioral risk factors early in life [10] are urgently necessary [11,12,13]—especially those which authentically engage and serve health disparity populations most affected by chronic disease burden [3].
One promising setting for such behavior change intervention efforts—including obesity prevention interventions—is that of early care and education (ECE) [14,15,16,17]. Not only do ECEs reach over 60% of children age 3–5 years in the U.S. [18], but they also offer a longitudinal connection with parents and the larger family system. Consequently, an abundance of ECE-based health promotion and behavior change interventions have emerged in the past fifteen years [14,19].
Although parent-engaged approaches to child health behavior change are considered the “gold standard” [20], few ECE studies have directly, effectively, and sustainably engaged parents as agents of change in child health behavior. This is attributed to notable challenges engaging parents of young children, including but not limited to a lack of parent and ECE staff time, competing work and caregiving responsibilities, and a lack of childcare outside school hours [21,22]. Instead, most ECE-based interventions have focused on teacher and child behavior intervention [23]. Fewer still have used a community-engaged participatory (CBPR) [24] approach to for intervention design and delivery [25,26,27].
In response, our academic research team partnered with parents, staff, and the leadership of Greater Boston Head Start—a federally funded school readiness program for young children (aged three to five years) of low-income households disproportionately affected by chronic disease [28]. Together, we adapted and implemented Communities for Healthy Living (CHL), a multi-component intervention to support parental empowerment and healthy parenting behaviors among low-income families across 16 programs (adaptation: 2016–2017, implementation: 2017–2020) [29], involving enhanced nutrition support, a media campaign, and a 10-week, opt-in parenting program.
Previously published findings suggested that parents who enrolled in CHL’s parenting program (vs. not) demonstrated significant increases in parental empowerment [30,31]; further, both parenting program participants [32] and facilitators [33] reported high program acceptability and appropriateness. While those exposed to lower-intensity CHL intervention components (e.g., enhanced nutrition support and media campaign) reported higher odds of children meeting three health behavior recommendations (i.e., sugar-sweetened beverage intake, water intake, and screen time), intervention exposure was not associated with clinically significant changes in child weight status.
Mixed results like these are common [34,35], despite mounting evidence supporting the promise of ECE-based interventions for early childhood health promotion intervention [36]. Further, those studies which do observe evidence of effectiveness often find that changes are not sustained long-term [37]. Contextual implementation determinants which are potentially driving these inconsistent and poorly maintained results remain understudied—particularly among CBPR interventions targeting parent behavior in low-resource ECE contexts [23,38]. Specifically, as noted in a recent scoping review of determinants underlying implementation of ECE-based interventions, there are limited data from evaluations grounded in theory, models, or frameworks, and from interventions designed to serve low-income or minorized populations specifically [23]. These research gaps not only prevent the advancement of intervention revision efforts, but they also impede progress in closing striking disparities in chronic disease risk and outcomes [3].
The current multimethod study aimed to fill this knowledge gap by summarizing contextual determinants (i.e., factors driving the success or failure of implementing an intervention) experienced and reported by Head Start leaders, staff, and parent facilitators over two years of intervention implementation (2017–2019).
2. Materials and Methods
2.1. Study Design
The current study describes findings from pre-implementation surveys and mid-implementation-interviews with Head Start staff, leadership, and facilitators (parents and staff) involved in the CHL intervention implementation (2017–2019). The CHL intervention is a program-level cluster-randomized pediatric obesity prevention intervention designed in partnership with Head Start (2016–2019) to support parental empowerment and healthy parenting behaviors among low-income families. Details on CHL protocol [29,39] (e.g., theoretical framing, participatory methods, intervention components) and impact evaluation findings [30] have been previously reported.
2.2. Intervention Development
Aligned with a CBPR [24] approach, CHL intervention design, implementation, and evaluation were driven by community-researcher co-leadership. For the first year, Head Start convened two Community Advisory Boards (CABs) of parents and staff, who met regularly to adapt study materials from a 2009 upstate New York pilot study [40] to fit the Greater Boston context. Key changes included extending the parenting program (PConnect) to 20 h over 10 weeks and adding nutrition support for Head Start staff. Media resources were expanded from posters to include brochures, social media, and online platforms. Ultimately, the adapted intervention involved three components: enhanced nutrition support, a media campaign, and a 10-week opt-in parenting program (PConnect), which have been described previously [29]. The revised program and evaluation surveys were then pilot tested in spring 2017 before the randomized trial in fall 2017.
Prior to intervention implementation, the study manager, with oversight from the study statistician, randomly assigned Head Start programs to one of three intervention start times. Over the next three years, the adapted intervention was implemented across 16 programs, via stepped wedge design [41], with the support of Head Start staff and leadership. Aligning with CBPR principles, financial resources were shared through subcontracts; an intervention coordinator was hired by Head Start partners to support translating research plans into implementation efforts. Primary study outcomes included child weight status and body mass index z-score. Secondary outcomes included child health behaviors (i.e., dietary intake, physical activity, screen use, and sleep), parenting practices across the same domains, and parent empowerment.
2.3. Theoretical Framework and Intervention Components
Grounded in empowerment theories [42] and the Family Ecological Model [43], the CHL intervention’s theory of change [29] (Figure 1) posited that increases in parental empowerment (i.e., the process by which parents realize control and take action for child health) [42,44,45,46] and healthy weight-related parenting practices (i.e., behaviors to shape child health) [47] would be associated with positive changes in child health behaviors and weight status [46]. Intervention components described above directly align with this theory of change.
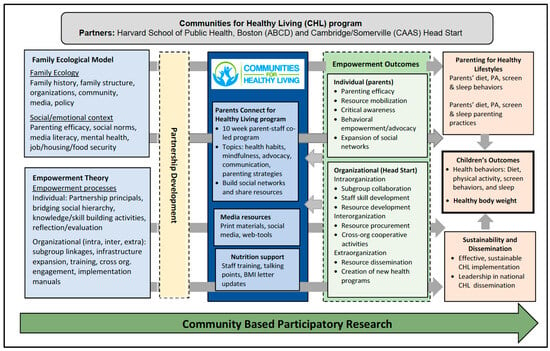
Figure 1.
The Communities for Healthy Living intervention theory of change.
Briefly, the enhanced nutrition support involved implementing standardized procedures for height and weight measurements of children and counseling for parents, developing a technical manual for anthropometric measurement and questionnaire administration, creating visual aids to facilitate questionnaire administration, delivering ongoing staff training, and revising child health screening reports. The media campaign involved redesigning brochures and flyers, sharing community-specific information and resources through online platforms, and creating a novel online neighborhood resource map. Finally, a 10-week parenting program was designed to cover content areas critical to child health (e.g., parenting practices, parent and child health behaviors, mindfulness, advocacy, and communication), as well as support skill development in social networking and resource sharing.
2.4. Data Collection
Data collection procedures were previously described in detail [39] and the data collection timeline is summarized in Figure 2. Briefly, data were collected through surveys, interviews, and focus groups between September 2017 and June 2019, in alignment with fall (September–December) and spring (April–June) semesters at Head Start.
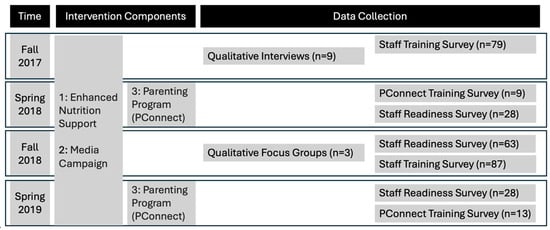
Figure 2.
Overview of Community for Healthy Living intervention components and data collection timeline.
Specifically, three anonymous surveys were administered to eligible Head Start staff and PConnect facilitators; these surveys included the Staff Training Survey, the PConnect Training Survey, and the Staff Readiness Survey. The Staff Training Survey (n = 5 items) was administered via paper to Head Start staff in fall 2018 and 2019 at the end of CHL intervention training offered before intervention initiation; survey items were developed to measure clarity and complexity of staff role in the CHL intervention and self-efficacy using CHL intervention resources. Second, the PConnect Training Survey (n = 32 items) was administered in Spring 2018 and 2019 via paper at the end of the three-day training for PConnect facilitators (Head Start parents and staff) covering PConnect program content and facilitation skills; items were developed to measure training effectiveness, training quality, and the quality of PConnect program materials. Third, via convenience sampling, all Head Start staff at participating intervention sites were invited via email broadcast and in-person staff meetings to complete the Staff Readiness Survey (n = 29 items adapted from the validated Organizational Readiness for Implementing Change (ORIC) measure [48]) via paper or Research Electronic Data Capture (REDCap); this survey was administered biannually in 2018 and 2019 and survey items were developed to measure staff readiness to implement the intervention, staff use of CHL materials, as well as perceived quality and usefulness of CHL materials.
Via purposive sampling, key Head Start staff and leadership involved in the implementation of CHL were selected and invited to participate in qualitative interviews (n = 9 staff) in fall 2019 and focus groups (n = 2 with n = 2 leaders and n = 14 staff) in fall 2018. Participants included Head Start program directors, supervisors and family engagement managers, Head Start nutritionists, Head Start health service team members, and CHL coordinators. Interviews and focus groups lasted between 30 min and one hour. Interviews were conducted via phone, and focus groups were conducted in person at Head Start administrative offices. All interviews and focus groups were audio recorded, and transcribed by an offsite company (Landmark Associates, Inc., Phoenix, AZ, USA).
2.5. Ethics
All surveys, interviews, and focus groups were conducted by trained research staff. Before survey completion, all participants reviewed information about the study and marked a checkbox as indication of consent. Before interview or focus group completion, participants received a key information sheet, reviewed information about the study verbally, and provided verbal consent. Study protocols were approved by the ethics review boards at Harvard University and Boston College. The trial protocol was registered at ClinicalTrials.gov (NCT03334669).
2.6. Conceptual Framework
Given the lag in translating behavior change research into practice in the context of ECEs [23], we grounded our evaluation in the Consolidated Framework for Implementation Research 2.0 (CFIR). CFIR represents one of the most widely published implementation science determinant frameworks, programing attention around innovation recipients (e.g., parents) and determinants of equitable implementation [49]. Specifically, we focused on three CFIR domains (e.g., levels), including that of the individual (e.g., Head Start staff and leadership), the innovation (e.g., the CHL intervention), and the inner setting (e.g., Head Start sites).
2.7. Analysis
We applied a convergent, mixed-methods approach, wherein quantitative and qualitative data were collected and analyzed independently and subsequently integrated via joint display [50]. (CG and Survey responses were downloaded from REDCap; frequency (n, %) and mean scores were tabulated in R 4.2.2 (R Core Team, 2022). Simultaneously, qualitative data were analyzed by two trained qualitative researchers AAT) via thematic analysis. Specifically, the primary coder (CG) used a deductive approach to capture implementation determinants through a preliminary coding structure informed by the CFIR. Both coders then reviewed the initial codebook and used inductive (open and axial coding) methods to independently code the same two transcripts. The coders then met over video conference to review and revise the codebook, as well as reconcile coding differences through comparison and discussion. After applying the revised codebook to independently code another two transcripts and revise the first two, they then met again to compare and reconcile differences; at this point, coding was deemed consistent (though comparison and discussion) and no further changes to the codebook were required. The revised codebook was then used to independently code the remaining transcripts, and a final set of themes were collaboratively generated through excerpt review and discussion over video conference. A total of n = 12 transcripts were coded for analysis, including n = 9 staff interviews and n = 3 focus groups (with a total of n = 16 participants; range: 2–10 participants). All analyses were conducted in Dedoose (version 9.0.17, Los Angeles, CA, USA).
3. Results
3.1. Sample Characteristics
Briefly, most survey respondents identified as female (61.3% of staff and 100% of PConnect facilitators, Table 1). Approximately one in three staff respondents and one in four PConnect facilitators identified as Hispanic (33.6%), one in five (19.3%) as non-Hispanic (NH) Black, and one in five as NH Asian; among PConnect facilitators, fewer identified as Hispanic (27.3%) and more as NH Black (31.8%). Similar frequencies of staff and facilitators had earned an undergraduate or graduate degree (49.6% of staff and 40.9% of facilitators). A majority of staff had been at Head Start for 10 years or more (50.5%) while most facilitators had been there less than 4 (72.6%).

Table 1.
Demographic characteristics of survey respondents (n = 144 Head Start staff and parents, Massachusetts, 2017–2019).
3.1.1. Theme 1 (CFIR’s Mission Alignment): CHL Intervention Activities Align with the Head Start Mission
“With [Head Start’s] mission [to support] families, I think [CHL] gives you one more way to connect with families.”—Head Start leadership
Head Start staff and leadership described nutritional health not only as an important community need, but as a prerequisite for Head Start’s mission of promoting school readiness (e.g., “If you don’t take care of the basic needs of children and families… [it] doesn’t matter what you teach them—it’s not gonna sustain.”). This same synergy was also reflected in survey responses, with 93.2% of staff agreeing that the CHL intervention addresses an important need for the community and 94.9% agreeing that the CHL intervention will be effective in improving family and child health (Table 2 and Table S1). Beyond school readiness and health outcomes alone, Head Start staff viewed CHL’s activities as an additional platform for connecting with parents, which is central to Head Start’s mission to engage family systems in child development (“It’s everybody’s business when it comes to parent engagement and recruitment, helping families”). This agreement was also reflected in survey responses, through which 95.5% of PConnect facilitators agreed that PConnect would help them connect with parents.
Table 2.
Joint display used to compare and integrate findings from of qualitative interviews and surveys.
3.1.2. Theme 2 (CFIR’s Engaging): Participation in the Design Process Results in High-Quality Materials
“I feel like the resource map was a really great… tool that I could share with those specific staff members. It helped [staff] support their families.”—Head Start Staff
Interview responses suggest that engaging with the Head Start leadership, staff, and parents was critical for improving the quality, appropriateness, and acceptability of materials. Head Start staff consistently reported that participatory methods resulted in the development of better materials, including staff talking points, brochures, and online neighborhood resource maps (e.g., “Any changes that we suggested were done. In the meeting we all talked about it. Then the next meeting, we will see what they work on and results.”). Further, Head Start staff appreciated the receptivity of the research team to changes (e.g., “You guys have been very receptive in listening to everything”). This appreciation was also reflected in the survey responses, with 66.7% of Head Start staff strongly agreeing they would use the Healthy Habits brochures as a resource. However, mid-implementation, reports of material utilization were more varied, with 33.3% reporting they consistently use the Staff Talking Points, 66.7% Healthy Habits brochures, and 50.7% using the Neighborhood Resource Map (Table S2). Despite this variable uptake, most Head Start staff rated the staff talking points, healthy habits brochures, and posters as useful.
3.1.3. Theme 3 (CFIR’s Available Resources): Allocation of CHL-Specific Resources Is Necessary for Success
“We are running by a shoestring budget… you definitely need some funding.”—Head Start Staff
Head Start staff and leadership reflected on the importance of allocating intervention-specific resources and staff to alleviate Head Start employee burden. Further, they described the challenges associated with long-term intervention planning in the context of short-term funding cycles (e.g., “We’ve been having that support from the [university] people and then once they’re no longer involved… I’m thinking money is the future of the grant. I’m thinking about it a lot.”). Specifically, leadership applauded the positive impact that hiring a CHL-specific coordinator posed on staff implementation burden (e.g., “[The CHL intervention coordinator] is extremely helpful. She’s there. She’s around. She kind of takes the burden off people”).
3.1.4. Theme 4 (CFIR’s Relative Priority): Demonstrated Support from Leadership Is Necessary for Staff Buy-In and Prioritization
“If you don’t have the support from the director, it doesn’t work.”—Head Start Staff
Many Head Start staff and leadership noted the need for greater program visibility and involvement among management. Achieving this would not only ensure that staff felt support for their implementation efforts, but it would also help to facilitate greater parent engagement with the program (e.g., “If the program director has an understanding of what’s happening… that could be included in the calendar, if she was better aware of what was going on with CHL”). This lack of CHL intervention visibility was also reflected in survey responses, with only 28.6% of staff strongly agreeing that they were confident they would be supported in CHL implementation and 19.3% strongly agreeing CHL is a priority at their program. Beyond prioritization alone, Head Start staff viewed leadership and management involvement as critical for building and maintaining accountability structures; for example, staff reported that lack of authority over others limited staff ability to coordinate CHL intervention activities with other staff, calling for management and leadership to step in (e.g., “I’m not an authority—I’m not anyone’s boss, so it’s hard to make—have any authority to tell people they need to be doing things”). Lack of alignment between CHL intervention activities and staff responsibilities further hindered CHL intervention activity coordination (e.g., “My supervisor might say that it has, potentially, taken away from other things… because [CHL] wasn’t technically my job description.”).
3.1.5. Theme 5 (CFIR’s Deliverer Opportunity): CHL Strains Workflow but Offers Benefits
“I feel like [the CHL intervention] needs to be something that is added in to our responsibilities, I guess.”—Head Start Staff
Head Start staff perceived CHL intervention tasks as additional burdens beyond that required of their already high responsibilities and expectations; this directly contrasted the intervention designers’ intention of integration. In response, staff called for the need to formally align CHL intervention activities with staff responsibilities or formally add CHL intervention activities to job descriptions and expectations. This same sentiment was also reflected in survey responses, with one-in-four surveyed staff (22.7%) strongly agreeing that the CHL intervention fits within their current job responsibilities and 32.8% strongly agreeing that they want to implement the CHL intervention. Still, despite the time commitment it involved, staff did report benefits of supporting the CHL intervention implementation; for example, 77.3% of PConnect facilitators surveyed agreed the experience of facilitating would help them professionally.
3.1.6. Theme 6 (CFIR’s Teaming): Lack of Shared Responsibility Amidst Frequent Turnover Hindered CHL Implementation
“We’ve lost a few staff over the last couple of years… if you don’t have someone who has seen it through who can be a mentor to other people, it can be tough.”—Head Start Staff
Overall, Head Start staff described the lack of shared responsibility as a barrier to implementation. This was attributed to two key factors: lack of staff engagement and turnover, especially early in the intervention, among leadership and champions involved in intervention development. Regarding staff engagement, staff and leadership described lack of cohesion as a barrier to CHL intervention implementation (e.g., “I think it needs to be more cohesive with staff being included”); in response, staff and leadership described the need for authentically and actively engaging as many staff as possible in design and implementation (e.g., “Incorporating staff, I think, needs to be on the front burner”). Regarding turnover, staff described inconsistent training for off-cycle hires and a lack of long-term involvement with the CHL intervention as barriers to implementation. For example, pervasive lack of training and experience with the CHL intervention resulted in implementation burden falling almost entirely on a few key staff members (e.g., “[When a team member does not] necessarily feel empowered to do [an activity] … I think it falls on my shoulders, or it doesn’t happen”). This lack of teaming was also reflected in survey responses. While nearly all staff (92.5%) reported they were committed to implementing CHL, the degree of commitment varied, with only 30.3% strongly agreeing versus 62.2% agreeing they were committed. A few more staff strongly agreed they wanted to implement CHL (32.8% versus 59.7% agreed), indicating a potential disconnect between desire to support and capacity to do so.
3.1.7. Theme 7 (CFIR’s Compatibility): Challenges Coordinating Competing Programs
“We have classes, consults, parent meetings, different workshops so the parents want to do everything, but they can’t… that could be affecting attendance.”—Head Start Staff
Head Start staff reported that scheduling CHL was often a challenge amidst the rich array of other programs offered at Head Start—not only in terms of allocating staffing to cover simultaneous programming, but also finding space and directing parents to the appropriate programs (e.g., “I feel like…trying to schedule [CHL] around other programs… that’s the only real problem with the CHL grant.”). Even in cases where parents were interested in multiple programs, staff noted they would have to choose one, ultimately hindering attendance across all competing programs, not just the CHL intervention. Further, the wide array of frequently changing options made it hard for staff to keep up to date, leaving both staff and parents overwhelmed with information (e.g., “They would be confused because we have so many meetings.”). Without distinguishing CHL as a unique and important program with specific goals, staff were unable to distinguish and elevate it in the context of other ongoing programs. This was reflected in the survey data as well, with 21.0% strongly agreeing they could help coordinate efforts.
4. Discussion
While most prior studies targeting obesity prevention in early childhood have focused on child-programed approaches [51], the CHL intervention partnered with ECE leadership, staff, and parents to address larger family ecologies through parent behavior change [43]. This study is among the first to explore implementation partner perspectives on contextual determinants to parent-programed obesity prevention intervention implementation in the context of Head Start, despite burgeoning evidence supporting the promise of intervention research in this context [23]. Aligning with recent literature on contextual determinants of ECE intervention sustainability [51], findings synthesized through our multimethod approach suggest facilitators to intervention implementation include mission alignment, authentic engagement, resource co-investment [52], and leadership buy-in as facilitators to intervention implementation. On the other hand, partners also noted several key barriers to implementation, including misaligned expectations, siloed responsibility, and challenges coordinating competing programs [53].
From these findings and prior literature, several key practice recommendations were generated. First, mission and expectations between the intervention and partner organizations must be aligned. Further, these must be communicated clearly, consistently, and repeatedly over the intervention life course for partner staff and leadership to justify intervention prioritization and distinction amidst competing programs offering clearer alignment. For example, materials disseminated in the context of Head Start must directly and clearly support school readiness [54]. This may also support program visibility and buy-in amongst leadership [55], which could facilitate management of staff expectations and shared responsibilities [56] related to intervention activities.
Second, following a CBPR approach [57], all stages of intervention design and implementation should be iteratively revised [58] in partnership with engaged Head Start leadership and staff. Not only does iterative engagement process foster partner buy-in, but it also ensures that materials fit the unique needs of the community, thereby optimizing intervention implementation and, ultimately, effectiveness [24].
Third, in line with CBPR principles, intervention designers should invest in and share resources for long-term intervention sustainment [59,60]. In particular, Head Start staff and leadership applauded investment in personnel for intervention coordination. However, anticipation of coordinator loss at grant’s end was considered detrimental for long-term intervention sustainment [61]. Intervention efforts in ECEs require efficient methods for assessing, establishing, and maintaining clear priorities to ensure appropriate allocation of limited funding, strict scrutiny of external resources, and clarity about staff roles, responsibilities, and the interconnections across program components. In cases where long-term intervention-specific staffing is untenable, train-the-trainer models [62] may be appropriate.
Beyond hiring additional staff, interventionists must also intentionally work with ECE leadership to align intervention engagement opportunities [63] with current staff expectations and workflows. Achieving this will not only ensure that staff could get more involved, but also that they are able to access the concrete support necessary for success. To further support responsibility sharing and prevent tasks from falling on a select few, interventionists must simultaneously work with ECE leadership to build supervisory structures for intervention tasks in support of implementation oversight and authority [64]. This is particularly important in the context of ECE, where money is stretched thin and turnover rates are high [65,66]. Beyond supporting intervention sustainability alone, these findings suggest that public investment in professional development opportunities, behavioral health initiatives, and mentorship services is critical for supporting staff retention and maintaining a stable ECE workforce [67].
Further, applying a policy, systems, and environment approach—which reshapes the contexts in which children grow—may provide a sustainable model for promoting healthful behavior change while reducing ECE staff burden [13,68,69,70,71]. Examples of such interventions include connecting families with existing social and economic resources (e.g., nutrition assistance programs, legal services, job training programs), increasing healthy food options at ECEs and across neighboring retailers, providing transportation and childcare supports for parents to attend programs like PConnect, and build strategic partnerships with universities to support participatory grant writing and program development [70].
Several key limitations should be noted. First, data were collected before the Coronavirus disease 2019 (COVID-19) pandemic, which may limit generalizability today; that said, Head Start operations have largely returned to pre-COVID-19 conditions and ECE-based interventions continue to grow. Second, these data were collected in Northeastern US; other contexts may present distinct facilitators and barriers, based on state-level policies [66]. That said, Head Start is a federal program, which offers some generalizability and scalability of findings from the current study. Third, recall and social desirability bias may have been introduced, given that self-report surveys were administered in the context of the workplace; to limit this, surveys remained anonymous, and sample sociodemographic characteristics were not collected for those who completed the interviews, to help protect participant identities. Finally, it is possible that those who completed the interviews or surveys were systematically different from the larger Head Start staff population (thereby introducing selection bias); however, this is unlikely given that we collected data from a range of participants, exemplified by the range of years at Head Start and roles represented, for example.
This study also offers notable strengths. First, this study leverages multi-year data from a large sample of staff from n = 16 Head Start programs across two agencies, offering a larger sample size than most comparable studies. Second, this study reports on an important context for health interventions [67], with Head Start being the largest federally funded early childhood education program in the US, serving nearly one million children every year. Third, findings were generated at the intersection of both qualitative and quantitative data from diverse stakeholders (Head Start leadership, staff, and facilitators), who are underrepresented in the literature. This multimethod approach elucidated a richer understanding of their experiences implementing the intervention than would be possible through one data source alone.
5. Conclusions
In conclusion, our findings suggest that CBPR obesity prevention intervention facilitators in the context of ECEs include mission alignment, partner engagement in design, allocation of intervention-specific resources, and expressed leadership support. Barriers included strains imposed on staff workflow, a lack of shared responsibility, and challenges in coordinating CHL activities amidst competing Head Start programs. In response, interventionist designers should align activities with current ECE workflows, define mission alignment while distinguishing the unique value added by intervention activities, and allocate intervention-specific resources to ensure program continuity long-term.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/nu17061063/s1, Table S1. Head Start staff and parent facilitator survey responses on implementation readiness and training experiences (Massachusetts, 2017–2019); Table S2. Head Start staff survey responses on CHL material utilization (n = 75, Massachusetts, 2017–2019); Table S3. Facilitator Training Survey (n = 22 Head Start staff and parent facilitators).
Author Contributions
Conceptualization, C.M.G., A.A.-T. and K.K.D.; Data curation, C.M.G.; Formal analysis, C.M.G. and A.A.-T.; Funding acquisition, K.K.D.; Investigation, C.M.G. and A.A.-T.; Methodology, C.M.G. and K.K.D.; Project administration, K.K.D.; Resources, A.A.-T.; Software, C.M.G.; Supervision, K.K.D.; Writing—original draft, C.M.G.; Writing—review and editing, A.A.-T., N.G. and K.K.D. All authors have read and agreed to the published version of the manuscript.
Funding
This work was conducted with support from the National Institute of Diabetes and Digestive and Kidney Diseases (R01DK108200) from the National Institutes of Health (NIH). No funding agency participated in the study design, data collection, data analysis, writing of the manuscript, or decision to submit the manuscript for publication.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of Harvard University and Boston College (#20.005.01; 19 June 2019). Trial protocol was registered at ClinicalTrials.gov (NCT03334669).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available from the corresponding author upon request due to ethical restrictions.
Acknowledgments
We would like to thank the Head Start staff and parents who contributed their time, energy, and reflections to make this study possible. Copyrighted material was not included; copyrighted surveys/instruments/tools were not used. The authors declare no potential conflicts of interest with respect to the research, authorship, or publication of this article. No copyrighted material, surveys, instruments, or tools were used in the research described in this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CAB | Community Advisory Board |
| CBPR | Community-Based Participatory Research |
| CFIR | Consolidated Framework for Implementation Research |
| CHL | Communities for Healthy Living |
| ECE | Early care and education |
References
- Raghupathi, W.; Raghupathi, V. An Empirical Study of Chronic Diseases in the United States: A Visual Analytics Approach. Int. J. Environ. Res. Public Health 2018, 15, 431. [Google Scholar] [CrossRef] [PubMed]
- Braveman, P.A.; Cubbin, C.; Egerter, S.; Williams, D.R.; Pamuk, E. Socioeconomic Disparities in Health in the United States: What the Patterns Tell Us. Am. J. Public Health 2010, 100, S186–S196. [Google Scholar] [CrossRef] [PubMed]
- Isong, I.A.; Rao, S.R.; Bind, M.-A.; Avendaño, M.; Kawachi, I.; Richmond, T.K. Racial and Ethnic Disparities in Early Childhood Obesity. Pediatrics 2018, 141, e20170865. [Google Scholar] [CrossRef] [PubMed]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of obesity among adults and youth: United States, 2015–2016. NCHS Data Brief 2017, 188, 1–8. [Google Scholar]
- Hertzman, C.; Boyce, T. How experience gets under the skin to create gradients in developmental health. Annu. Rev. Public Health 2010, 31, 329–347. [Google Scholar] [CrossRef]
- Halfon, N.; Larson, K.; Lu, M.; Tullis, E.; Russ, S. Lifecourse Health Development: Past, Present and Future. Matern. Child. Health J. 2014, 18, 344–365. [Google Scholar] [CrossRef]
- Seligman, H.K.; Schillinger, D. Hunger and Socioeconomic Disparities in Chronic Disease. N. Engl. J. Med. 2010, 363, 6–9. [Google Scholar] [CrossRef]
- Bagby, S.P.; Martin, D.; Chung, S.T.; Rajapakse, N. From the Outside In: Biological Mechanisms Linking Social and Environmental Exposures to Chronic Disease and to Health Disparities. Am. J. Public Health 2019, 109, S56–S63. [Google Scholar] [CrossRef]
- Price, J.H.; Khubchandani, J.; McKinney, M.; Braun, R. Racial/Ethnic Disparities in Chronic Diseases of Youths and Access to Health Care in the United States. Biomed. Res. Int. 2013, 2013, 787616. [Google Scholar] [CrossRef]
- Monasta, L.; Batty, G.D.; Cattaneo, A.; Lutje, V.; Ronfani, L.; Van Lenthe, F.J.; Brug, J. Early-life determinants of overweight and obesity: A review of systematic reviews. Obes. Rev. 2010, 11, 695–708. [Google Scholar] [CrossRef]
- Gortmaker, S.L.; Swinburn, B.A.; Levy, D.; Carter, R.; Mabry, P.L.; Finegood, D.T.; Huang, T.; Marsh, T.; Moodie, M.L. Changing the future of obesity: Science, policy, and action. Lancet 2011, 378, 838–847. [Google Scholar] [CrossRef] [PubMed]
- Davison, K.K.; Birch, L.L. Childhood overweight: A contextual model and recommendations for future research. Obes. Rev. 2001, 2, 159–171. [Google Scholar] [CrossRef] [PubMed]
- Kracht, C.L.; Burkart, S.; Flanagan, E.W.; Melnick, E.; Luecking, C.; Neshteruk, C. Policy, system, and environmental interventions addressing obesity and diet-related outcomes in early childhood education settings: A systematic review. Obes. Rev. 2023, 24, e13547. [Google Scholar] [CrossRef] [PubMed]
- Ward, D.S.; Welker, E.; Choate, A.; Henderson, K.E.; Lott, M.; Tovar, A.; Wilson, A.; Sallis, J.F. Strength of obesity prevention interventions in early care and education settings: A systematic review. Prev. Med. 2017, 95, S37–S52. [Google Scholar] [CrossRef]
- Jones-Taylor, M. Early Care and Education Settings Are Vital for Childhood Obesity Prevention. Child. Obes. 2015, 11, 489–490. [Google Scholar] [CrossRef]
- Dattilo, A.M.; Birch, L.; Krebs, N.F.; Lake, A.; Taveras, E.M.; Saavedra, J.M. Need for Early Interventions in the Prevention of Pediatric Overweight: A Review and Upcoming Directions. J. Obes. 2012, 2012, e123023. [Google Scholar] [CrossRef]
- Buscemi, J.; Kanwischer, K.; Becker, A.B.; Ward, D.S.; Fitzgibbon, M.L.; on behalf of the Society of Behavioral Medicine Health Policy Committee. Society of Behavioral Medicine position statement: Early care and education (ECE) policies can impact obesity prevention among preschool-aged children. Transl. Behav. Med. 2015, 5, 122–125. [Google Scholar] [CrossRef]
- COE—Enrollment Rates of Young Children. Available online: https://nces.ed.gov/programs/coe/indicator/cfa/enrollment-of-young-children (accessed on 11 January 2024).
- Larson, N.; Ward, D.S.; Neelon, S.B.; Story, M. What Role Can Child-Care Settings Play in Obesity Prevention? A Review of the Evidence and Call for Research Efforts. J. Am. Diet. Assoc. 2011, 111, 1343–1362. [Google Scholar] [CrossRef]
- Perdew, M.; Liu, S.; Naylor, P.-J. Family-based nutrition interventions for obesity prevention among school-aged children: A systematic review. Transl. Behav. Med. 2021, 11, 709–723. [Google Scholar] [CrossRef]
- Kelleher, E.; Davoren, M.P.; Harrington, J.M.; Shiely, F.; Perry, I.J.; McHugh, S.M. Barriers and facilitators to initial and continued attendance at community-based lifestyle programmes among families of overweight and obese children: A systematic review. Obes. Rev. 2017, 18, 183–194. [Google Scholar] [CrossRef]
- Schmied, E.A.; Madanat, H.; Chuang, E.; Moody, J.; Ibarra, L.; Cervantes, G.; Strong, D.; Boutelle, K.; Ayala, G.X. Factors predicting parent engagement in a family-based childhood obesity prevention and control program. BMC Public Health 2023, 23, 457. [Google Scholar] [CrossRef] [PubMed]
- Asada, Y.; Lin, S.; Siegel, L.; Kong, A. Facilitators and Barriers to Implementation and Sustainability of Nutrition and Physical Activity Interventions in Early Childcare Settings: A Systematic Review. Prev. Sci. 2023, 24, 64–83. [Google Scholar] [CrossRef] [PubMed]
- Wallerstein, N.; Duran, B. Community-based participatory research contributions to intervention research: The intersection of science and practice to improve health equity. Am. J. Public Health 2010, 100 (Suppl. S1), S40–S46. [Google Scholar] [CrossRef]
- Calancie, L.; Nappi, D.; Appel, J.; Hennessy, E.; Korn, A.R.; Mitchell, J.; Patrick, A.; Werner, K.; Economos, C.D. Implementing and Evaluating a Stakeholder-Driven Community Diffusion–Informed Early Childhood Intervention to Prevent Obesity, Cuyahoga County, Ohio, 2018–2020. Prev. Chronic Dis. 2022, 19, E03. [Google Scholar] [CrossRef]
- Slining, M.; Wills, S.; Fair, M.; Stephenson, J.; Knobel, S.; Pearson, M.; Prostko, T.; Smyers, J.; Timberlake, J.; Negrete, M. LiveWell in early childhood: Results from a two-year pilot intervention to improve nutrition and physical activity policies, systems and environments among early childhood education programs in South Carolina. BMC Public Health 2021, 21, 919. [Google Scholar] [CrossRef]
- Farewell, C.V.; Puma, J.E.; Powers, J.; Belansky, E.S. Assess, Identify, Make it Happen (AIM) for Preschools: A Tool to Decrease Early Childhood Obesity. Health Promot. Pract. 2018, 19, 935–945. [Google Scholar] [CrossRef]
- Imoisili, O.; Dooyema, C.; Kompaniyets, L.; Lundeen, E.A.; Park, S.; Goodman, A.B.; Blanck, H.M. Prevalence of Overweight and Obesity Among Children Enrolled in Head Start, 2012–2018. Am. J. Health Promot. 2021, 35, 334–343. [Google Scholar] [CrossRef]
- Beckerman, J.P.; Aftosmes-Tobio, A.; Kitos, N.; Jurkowski, J.M.; Lansburg, K.; Kazik, C.; Gavarkovs, A.; Vigilante, A.; Kalyoncu, B.; Figueroa, R.; et al. Communities for healthy living (CHL)—A family-centered childhood obesity prevention program integrated into Head Start services: Study protocol for a pragmatic cluster randomized trial. Contemp. Clin. Trials 2019, 78, 34–45. [Google Scholar] [CrossRef]
- Gago, C.; Aftosmes-Tobio, A.; Beckerman-Hsu, J.P.; Oddleifson, C.; Garcia, E.A.; Lansburg, K.; Figueroa, R.; Yu, X.; Kitos, N.; Torrico, M.; et al. Evaluation of a cluster-randomized controlled trial: Communities for Healthy Living, family-centered obesity prevention program for Head Start parents and children. Int. J. Behav. Nutr. Phys. Act. 2023, 20, 4. [Google Scholar] [CrossRef]
- Grafft, N.M.; Gago, C.; Garcia, E.; Aftosmes-Tobio, A.; Jurkowski, J.M.; Blaine, R.E.D.; Davison, K.K. Parent Experiences of Empowerment: Understanding the Role of Parent Empowerment in Child Health Promotion. Fam. Commun. Health 2024, 47, 261–274. [Google Scholar] [CrossRef]
- Grafft, N.; Aftosmes-Tobio, A.; Gago, C.; Lansburg, K.; Beckerman-Hsu, J.; Trefry, B.; Kumanyika, S.; Davison, K. Adaptation and implementation outcomes of a parenting program for low-income, ethnically diverse families delivered virtually versus in-person. Transl. Behav. Med. 2022, 12, 1065–1075. [Google Scholar] [CrossRef] [PubMed]
- Beckerman-Hsu, J.P.; Gago, C.; Aftosmes-Tobio, A.; Jurkowski, J.M.; Lansburg, K.; Leonard, J.; Torrico, M.; Haneuse, S.; Subramanian, S.V.; Kenney, E.L.; et al. Acceptability and appropriateness of a novel parent-staff co-leadership model for childhood obesity prevention in Head Start: A qualitative interview study. BMC Public Health 2021, 21, 201. [Google Scholar] [CrossRef] [PubMed]
- Sisson, S.B.; Krampe, M.; Anundson, K.; Castle, S. Obesity prevention and obesogenic behavior interventions in child care: A systematic review. Prev. Med. 2016, 87, 57–69. [Google Scholar] [CrossRef] [PubMed]
- Luybli, M.; Schmillen, H.; Sotos-Prieto, M. School-Based Interventions in Low Socioeconomic Settings to Reduce Obesity Outcomes among Preschoolers: A Scoping Review. Nutrients 2019, 11, 1518. [Google Scholar] [CrossRef]
- Scott-Sheldon, L.A.; Hedges, L.V.; Cyr, C.; Young-Hyman, D.; Khan, L.K.; Magnus, M.; King, H.; Arteaga, S.; Cawley, J.; Economos, C.D.; et al. Childhood Obesity Evidence Base Project: A Systematic Review and Meta-Analysis of a New Taxonomy of Intervention Components to Improve Weight Status in Children 2–5 Years of Age, 2005–2019. Child. Obes. 2020, 16, S2–S21. [Google Scholar] [CrossRef]
- Yavuz, H.M.; van Ijzendoorn, M.H.; Mesman, J.; van der Veek, S. Interventions aimed at reducing obesity in early childhood: A meta-analysis of programs that involve parents. J. Child Psychol. Psychiatry 2015, 56, 677–692. [Google Scholar] [CrossRef]
- Matwiejczyk, L.; Mehta, K.; Scott, J.; Tonkin, E.; Coveney, J. Characteristics of Effective Interventions Promoting Healthy Eating for Pre-Schoolers in Childcare Settings: An Umbrella Review. Nutrients 2018, 10, 293. [Google Scholar] [CrossRef]
- Beckerman-Hsu, J.P.; Aftosmes-Tobio, A.; Gavarkovs, A.; Kitos, N.; Figueroa, R.; Kalyoncu, Z.B.; Lansburg, K.; Yu, X.; Kazik, C.; Vigilante, A.; et al. Communities for Healthy Living (CHL) A Community-based Intervention to Prevent Obesity in Low-Income Preschool Children: Process Evaluation Protocol. Trials 2020, 21, 674. [Google Scholar] [CrossRef]
- Davison, K.K.; Jurkowski, J.M.; Li, K.; Kranz, S.; Lawson, H.A. A childhood obesity intervention developed by families for families: Results from a pilot study. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 3. [Google Scholar] [CrossRef]
- The Stepped Wedge Cluster Randomised Trial: Rationale, Design, Analysis, and Reporting|The BMJ. Available online: https://www.bmj.com/content/350/bmj.h391.abstract (accessed on 20 January 2025).
- Zimmerman, M.A. Psychological empowerment: Issues and illustrations. Am. J. Commun. Psychol. 1995, 23, 581–599. [Google Scholar] [CrossRef]
- Davison, K.K.; Jurkowski, J.M.; Lawson, H.A. Reframing family-centred obesity prevention using the Family Ecological Model. Public Health Nutr. 2013, 16, 1861–1869. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, R.; Gago, C.M.; Beckerman-Hsu, J.; Aftosmes-Tobio, A.; Yu, X.; Davison, K.K.; Jurkowski, J.J. Development and Validation of a Parental Health-Related Empowerment Scale with Low Income Parents. Int. J. Environ. Res. Public Health 2020, 17, 8645. [Google Scholar] [CrossRef] [PubMed]
- Jurkowski, J.M.; Lawson, H.A.; Green Mills, L.L.; Wilner, P.G.I.; Davison, K.K. The Empowerment of Low-Income Parents Engaged in a Childhood Obesity Intervention. Fam. Commun. Health 2014, 37, 104. [Google Scholar] [CrossRef]
- Gago, C.M.; Jurkowski, J.; Beckerman-Hsu, J.P.; Aftosmes-Tobio, A.; Figueroa, R.; Oddleifson, C.; Mattei, J.; Kenney, E.L.; Haneuse, S.; Davison, K.K. Exploring a theory of change: Are increases in parental empowerment associated with healthier weight-related parenting practices? Soc. Sci. Med. 2022, 296, 114761. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, R.; Saltzman, J.A.; Aftosmes-Tobio, A.; Davison, K.K. The Obesity Parenting Intervention Scale: Factorial Validity and Invariance Among Head Start Parents. Am. J. Prev. Med. 2019, 57, 844–852. [Google Scholar] [CrossRef]
- Damschroder, L.J.; Reardon, C.M.; Opra Widerquist, M.A.; Lowery, J. Conceptualizing outcomes for use with the Consolidated Framework for Implementation Research (CFIR): The CFIR Outcomes Addendum. Implement. Sci. 2022, 17, 7. [Google Scholar] [CrossRef]
- Meissner, H.; Creswell, J.; Klassen, A.C.; Plano, V.; Smith, K.C. Best Practices for Mixed Methods Research in the Health Sciences. Bethesda Natl. Inst. Health 2011, 2013, 541–545. [Google Scholar]
- Flynn, A.C.; Suleiman, F.; Windsor-Aubrey, H.; Wolfe, I.; O’Keeffe, M.; Poston, L.; Dalrymple, K.V. Preventing and treating childhood overweight and obesity in children up to 5 years old: A systematic review by intervention setting. Matern. Child Nutr. 2022, 18, e13354. [Google Scholar] [CrossRef]
- Imad, N.; Hall, A.; Nathan, N.; Shoesmith, A.; Pearson, N.; Lum, M.; Grady, A.; Nolan, E.; Yoong, S. A cross-sectional study assessing barriers and facilitators to the sustainability of physical activity and nutrition interventions in early childhood education and care settings. Int. J. Behav. Nutr. Phys. Act. 2025, 22, 2. [Google Scholar] [CrossRef]
- Byrd-Williams, C.; Dooley, E.E.; Sharma, S.V.; Chuang, R.-J.; Butte, N.; Hoelscher, D.M. Best Practices and Barriers to Obesity Prevention in Head Start: Differences Between Director and Teacher Perceptions. Prev. Chronic Dis. 2017, 14, E139. [Google Scholar] [CrossRef]
- Hoard, L.; Supplee, L. Results from the “I Am Moving, I Am Learning” Stage 1 Survey. 2007. Available online: https://acf.gov/sites/default/files/documents/opre/stage1_survey.pdf (accessed on 11 November 2024).
- Williams, N.J.; Wolk, C.B.; Becker-Haimes, E.M.; Beidas, R.S. Testing a theory of strategic implementation leadership, implementation climate, and clinicians’ use of evidence-based practice: A 5-year panel analysis. Implement. Sci. 2020, 15, 10. [Google Scholar] [CrossRef]
- Bergström, H.; Haggård, U.; Norman, Å.; Sundblom, E.; Schäfer Elinder, L.; Nyberg, G. Factors influencing the implementation of a school-based parental support programme to promote health-related behaviours—Interviews with teachers and parents. BMC Public Health 2015, 15, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Israel, B.A.; Schulz, A.J.; Parker, E.A.; Becker, A.B. Review of Community-Based Research: Assessing Partnership Approaches to Improve Public Health. Annu. Rev. Public Health 1998, 19, 173–202. [Google Scholar] [CrossRef] [PubMed]
- Researcher Readiness for Participating in Community-Engaged Dissemination and Implementation Research: A Conceptual Framework of Core Competencies|Translational Behavioral Medicine|Oxford Academic. Available online: https://academic.oup.com/tbm/article-abstract/7/3/393/4644888?redirectedFrom=fulltext (accessed on 16 January 2025).
- Brush, B.L.; Mentz, G.; Jensen, M.; Jacobs, B.; Saylor, K.M.; Rowe, Z.; Israel, B.A.; Lachance, L. Success in Long-Standing Community-Based Participatory Research (CBPR) Partnerships: A Scoping Literature Review. Health Educ. Behav. 2020, 47, 556–568. [Google Scholar] [CrossRef] [PubMed]
- Fathi, L.I.; Walker, J.; Dix, C.F.; Cartwright, J.R.; Joubert, S.; Carmichael, K.A.; Huang, Y.S.; Littlewood, R.; Truby, H. Applying the Integrated Sustainability Framework to explore the long-term sustainability of nutrition education programmes in schools: A systematic review. Public Health Nutr. 2023, 26, 2165–2179. [Google Scholar] [CrossRef]
- Burton, W.; Twiddy, M.; Sahota, P.; Brown, J.; Bryant, M. Participant engagement with a UK community-based preschool childhood obesity prevention programme: A focused ethnography study. BMC Public Health 2019, 19, 1074. [Google Scholar] [CrossRef]
- Successes and Challenges Using a Train-the-Trainer Approach: Educating Children About Nutrition and Physical Activity in After-School Programs. Ingenta Connect. Available online: https://www.ingentaconnect.com/content/aafcs/jfcs/2016/00000108/00000001/art00012 (accessed on 6 February 2025).
- Ward, S.; Chow, A.F.; Humbert, M.L.; Bélanger, M.; Muhajarine, N.; Vatanparast, H.; Leis, A. Promoting physical activity, healthy eating and gross motor skills development among preschoolers attending childcare centers: Process evaluation of the Healthy Start-Départ Santé intervention using the RE-AIM framework. Eval. Program. Plan. 2018, 68, 90–98. [Google Scholar] [CrossRef]
- Stokke, K.; Olsen, N.R.; Espehaug, B.; Nortvedt, M.W. Evidence based practice beliefs and implementation among nurses: A cross-sectional study. BMC Nurs. 2014, 13, 8. [Google Scholar] [CrossRef]
- Examining Barriers to Sustained Implementation of School-Wide Prevention Practices—Mary, G. Turri, Sterett H. Mercer, Kent McIntosh, Rhonda N. T. Nese, M. Kathleen Strickland-Cohen, Robert Hoselton. 2016. Available online: https://journals.sagepub.com/doi/10.1177/1534508416634624 (accessed on 16 January 2025).
- Whitebook, M.; Phillips, D.; Howes, C. Worthy Work, STILL Unlivable Wages: The Early Childhood Workforce 25 Years after the National Child Care Staffing Study. 2014. Available online: https://cscce.berkeley.edu/wp-content/uploads/publications/ReportFINAL.pdf (accessed on 11 November 2024).
- Swindle, T.; Johnson, S.L.; Davenport, K.; Whiteside-Mansell, L.; Thirunavukarasu, T.; Sadasavin, G.; Curran, G.M. A Mixed-Methods Exploration of Barriers and Facilitators to Evidence-Based Practices for Obesity Prevention in Head Start. J. Nutr. Educ. Behav. 2019, 51, 1067–1079.e1. [Google Scholar] [CrossRef]
- Hughes, C.C.; Gooze, R.A.; Finkelstein, D.M.; Whitaker, R.C. Barriers to Obesity Prevention in Head Start. Health Aff. 2010, 29, 454–462. [Google Scholar] [CrossRef]
- Olstad, D.L.; Ancilotto, R.; Teychenne, M.; Minaker, L.M.; Taber, D.R.; Raine, K.D.; Nykiforuk, C.I.J.; Ball, K. Can Targeted Policies Reduce Obesity and Improve Obesity-Related Behaviours in Socioeconomically Disadvantaged Populations? A Systematic Review. Obes. Rev. 2017, 18, 791–807. [Google Scholar] [CrossRef] [PubMed]
- Story, M.; Kaphingst, K.M.; Robinson-O’Brien, R.; Glanz, K. Creating Healthy Food and Eating Environments: Policy and Environmental Approaches. Annu. Rev. Public Health 2008, 29, 253–272. [Google Scholar] [CrossRef] [PubMed]
- Kumanyika, S. Getting to Equity in Obesity Prevention: A New Framework. NAM Perspectives. 2017. Available online: https://nam.edu/wp-content/uploads/2017/01/Getting-to-Equity-in-Obesity-Prevention-A-New-Framework.pdf (accessed on 11 March 2025).
- Neshteruk, C.; Burkart, S.; Flanagan, E.W.; Melnick, E.; Luecking, C.; Kracht, C.L. Policy, Systems, and Environmental Interventions Addressing Physical Activity in Early Childhood Education Settings: A Systematic Review. Prev. Med. 2023, 173, 107606. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).